Back to Journals » Journal of Healthcare Leadership » Volume 17
Leadership Challenges in a Resource-Constrained Health Care System in South Africa’s North West Province Case Study
Received 8 August 2025
Accepted for publication 8 November 2025
Published 9 December 2025 Volume 2025:17 Pages 831—842
DOI https://doi.org/10.2147/JHL.S553227
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Magome Masike,1,* Ozayr Mahomed2,*
1Health Professional Council of South Africa, Pretoria, South Africa; Discipline of Public Health Medicine, University of Kwazulu-Natal, Durban, South Africa; 2Department of Public Health Medicine, University of KwaZulu-Natal, Durban, South Africa
*These authors contributed equally to this work
Correspondence: Magome Masike, Public Health Medicine, University of KwaZulu-Natal, Private Bag X54001, Durban, 4000, South Africa, Tel +27115120194, Email [email protected]
Purpose: This study aimed to identify and explore the leadership challenges impeding the delivery of quality healthcare services in two district municipalities of the North West Province, South Africa.
Patients and Methods: A qualitative phenomenological design was used. Purposive sampling selected senior healthcare managers from the Bojanala Platinum District (BPD) and the Ngaka Modiri Molema District (NMMD). Data collection involved six focus group discussions (FGDs) with 6– 10 participants each and eight individual in-depth interviews (IDIs). Data analysis employed thematic and narrative analysis methods. Ethical approval was granted, and informed consent was obtained from participants.
Results: Participants identified five key themes: (1) Limited leadership empowerment, characterised by excessive centralisation of decision-making, causing delays and reduced local managerial autonomy; (2) Ineffective performance management due to poor implementation and underuse of the Performance Management and Development System (PMDS); (3) Weak policy execution, linked to inconsistent governance structures and poor oversight mechanisms; (4) Resource allocation and stewardship, including financial constraints and supply chain issues, leading to chronic shortages of essential medicines and poor equipment maintenance; and (5) Inadequate primary healthcare infrastructure and governance, resulting in diminished patient confidence, facility bypassing, and compromised service quality.
Conclusion: These findings, among the first to qualitatively examine leadership challenges within South Africa’s district health system, highlight how centralised decision-making, weak performance management, and resource constraints specifically impede service delivery in the North West Province. By offering context-specific insights and practical strategies for decentralisation, governance strengthening, and resource optimisation, this study provides locally relevant evidence to inform health system reform in similar low- and middle-income settings.
Keywords: healthcare leadership, governance, primary healthcare, performance management, resource management, policy implementation, South Africa
Introduction
Healthcare systems worldwide are increasingly recognised as complex adaptive systems that require leaders capable of navigating uncertainty, aligning diverse stakeholders, and sustaining high-quality service delivery despite resource constraints. In low- and middle-income countries (LMICs), where financial and human resources are often limited, effective leadership at all levels of the system is essential for improving population health outcomes. South Africa, classified as an “emerging and developing” nation by the United Nations and the International Monetary Fund,1 allocates a substantial portion of its budget to healthcare compared to peer nations, yet fails to achieve commensurate health outcomes.2 South Africa faces significant challenges in attaining favourable health outcomes due to a complex interplay of factors that include, amongst others, a quadruple burden of diseases, an HIV/TB epidemic, high child mortality and maternal mortality, high levels of non-communicable diseases, and high levels of violence and injuries.3 These challenges are compounded by a growing population, driven partly by immigration,4 which strains healthcare resources and exacerbates disparities in human resource distribution, particularly between urban and rural areas.4
In the North West Province, healthcare expenditure averaged 29.38% of the provincial budget (approximately R25.96 billion) from 2020/21 to 2023/24,5 supporting a population of 6.3% to 6.9% of South Africa’s total.6 However, health outcomes remain suboptimal. Malnutrition rates in the province averaged 16.83% over this period, slightly below the national average of 17.5%.5 Maternal mortality rates in the province consistently exceeded national figures, rising from 125/100,000 in 2019 to 188.5/100,000 in 2021, before declining to 116.8/100,000 in 2022.7 Similarly, the under-5 mortality rate (U5MR) in the Northwest was 55,7% in 2022, compared to a national estimate of 40, reflecting persistent challenges.8
Leadership in healthcare has been extensively studied, and various modern frameworks provide insights into how leaders can manage complexity. Transformational leadership focuses on vision-driven change and empowering staff; complexity leadership highlights adaptability and emergence within dynamic, non-linear systems; and systems leadership emphasises collaboration and alignment across multiple levels of interconnected health networks.9–13 These approaches are becoming increasingly important in healthcare management research in high-income settings, yet their use in LMIC district health systems remains insufficiently examined. In South Africa, where historical centralisation and bureaucratic inertia still exist, district-level managers often lack the leadership autonomy and support structures necessary to carry out responsive, locally adapted strategies. Poor fiscal management, unequal resource distribution, and limited capacity within the health workforce weaken service delivery, especially in rural areas.
This theoretical gap is especially significant considering South Africa’s National Health Insurance (NHI) reform. NHI aims to overhaul financing and governance structures to achieve universal health coverage and fair access to healthcare. While it shows promise, this transition presents extraordinary leadership challenges: district managers must navigate changing accountability systems, manage limited resources under new purchasing mechanisms, and uphold service quality amid systemic restructuring. Understanding how leaders experience and handle these pressures in real time is vital for strengthening the country’s health system and ensuring the success of NHI.
This qualitative study investigates the leadership challenges that impede quality healthcare delivery in two districts of North West Province: Bojanala Platinum District (BPD) and Ngaka Modiri Molema District (NMMD). By analysing these challenges, the study seeks to inform targeted interventions and policy reforms to enhance healthcare leadership, optimise resource allocation, and improve health outcomes for these communities. By providing context-specific, empirically grounded insights, the study broadens and applies established leadership theories (transformational, complexity, and systems leadership) within a resource-constrained and decentralising health system, offering actionable recommendations to influence both policy and practice amid South Africa’s ongoing health sector reforms.
Methods
This study employed a hermeneutic (interpretive) phenomenological design to explore the lived experiences of leadership among senior healthcare managers in the North West Province, South Africa. This approach was chosen to go beyond mere description and to interpret how participants understand the complex leadership challenges they face within a dynamic health system.
This qualitative phenomenological study was conducted among healthcare managers working for the NW province’s Department of Health in the BPD and NMMD municipalities. Focus group discussions, as an extended form of the interview method14, are employed for their versatility and strength, as they are both descriptive and interpretive, whereas the in-depth interviews are solely interpretive.
The target population for this study includes deliberately selected employees of the NW Department of Health assigned to roles such as Head of Department, Deputy Director General, hospital Chief Executive Officers, Chief Directors, Directors, Clinical Managers, and other senior management service staff (SMS) at regional hospitals, district hospitals, and community health centres. A total of 68 employees volunteered to participate in the research.
Purposive sampling was utilised to select participants from the public health sector based on their contextual knowledge and capacity to address the research questions. Data were collected through six focus group discussions (6–10 participants each) and eight in-depth interviews.
FGDs were used as an extended form of interview to stimulate discussion and surface collective system-level leadership perspectives, while IDIs allowed participants to reflect on personal experiences and sensitive organisational dynamics that might not emerge in groups. Focus group discussions lasted approximately two hours per session. These group interviews aimed to elicit the participants’ collective views on how management exercised leadership within the components of the health system, motivated the workforce, prioritised issues, implemented national policies, communicated the vision, and empowered leaders at the local level.
The focus group discussions took place between October and November 2022. A detailed schedule for each FGD was created through a thorough process that included a literature review on healthcare leadership challenges, piloting of the focus group questions, refining them based on feedback, and ensuring alignment with the study’s research objectives before conducting each focus group.
Key questions asked during the FGDs included how management exercised leadership in the components of the health system, motivating the workforce, prioritisation, implementation of national policies, communication of the vision, and empowerment of leaders at the local level.
Each of the eight individual interviews concentrated on the challenges faced in healthcare leadership and the obstacles to achieving quality healthcare services. These interviews also focused on high-ranking leaders such as clinical managers, chief executive officers of district hospitals, and managers of community health centres, to explore the implementation of policies at the organisational level, the oversight by local governance structures, and the health outcomes within the district.
Reflexivity and Bracketing
The lead researcher had previously served as a Member of the Executive Council (MEC) for Health in the province and therefore kept a reflective journal and engaged in memo writing throughout the research process. These reflexivity practices were used to identify and bracket personal assumptions, document positionality, and minimise potential bias, thereby enhancing the confirmability and trustworthiness of the findings.
Standard questions were employed to break down the research question and examine the feedback. Microsoft’s Excel spreadsheet application was utilised for organising, cleaning, and analysing the data. The researcher interrogated the data, generating initial codes, searching for themes, reviewing the themes, and defining and naming them from the in-depth interviews, focus group discussions, and allocated open codes,15 whilst the individual in-depth analysis involved “narrative analysis”,16 which mapped each participant’s views, to enable the researcher to understand how each personal experience contributed to the overall narrative.
Data were analysed inductively following Braun and Clarke’s six-phase thematic analysis (familiarisation, coding, theme development, review, definition, reporting). Initial open codes were generated across transcripts, clustered into categories, and iteratively refined into overarching themes. Narrative analysis complemented thematic analysis to preserve the personal meaning and lived experience conveyed by participants.
To preserve the lived-experience perspective, narrative analysis complemented the thematic process by illustrating how individual accounts constructed the collective story. The lead researcher kept analytic memos and reflexive journals to record decisions, assumptions, and emerging insights. Peer debriefing with a second qualitative researcher was carried out to review coding consistency, challenge theme definitions, and improve the credibility of the findings. Microsoft Excel was used to organise and track codes, categories, and theme iterations.
Credibility was strengthened by including participants from various seniority levels and facility types, as well as by triangulating focus group and interview data. Transferability was facilitated through purposive sampling across two of the four provincial districts, which helped capture variation in leadership contexts.
Ethical approval was granted by the University of KwaZulu-Natal Biomedical Research Ethics Committee (BREC), with protocol reference number BREC 690/18. The Department of Health in the North West Province granted gatekeeper permission. Participants were informed of the study’s aims, and written informed consent was obtained. Participants were also advised that their direct quotes might be used anonymously in publications, where applicable. The researchers used all data solely for the purpose of the study. This research adhered to the principles of the Declaration of Helsinki.
Results
Sociodemographic Characteristics of Participants
Sixty managers took part in the focus group discussion, and eight participants were interviewed. Fifty per cent of the participants (36) were between 11 and 12 (middle management), while almost 40% (27) were junior management. Fifty-three per cent (36) of managers had only a bachelor’s degree, whereas 7% (5) held postgraduate qualifications. There were more females (53%) than males (47%) participation. The majority (46%) were aged between 46 and 55 years, with a further 38% between 36 and 45 years. Seventy-five per cent (51) had been employed in their positions for more than five years. Fifty-three per cent of participants were from the NMMD municipality (see Table 1).
 |
Table 1 Sociodemographic Profile of Study Participants |
Results – Focus Group Discussions and Individual Interviews
Focus group discussions (FGDs) and in-depth interviews (IDIs) with purposively selected public health workers revealed gaps in leadership, governance, and operational practices. The findings are organised into five key themes: (1) limited leadership empowerment, (2) ineffective performance management, (3) weak policy implementation, (4) resource allocation and stewardship, and (5) inadequate primary healthcare (PHC) infrastructure and governance (see Table 2).
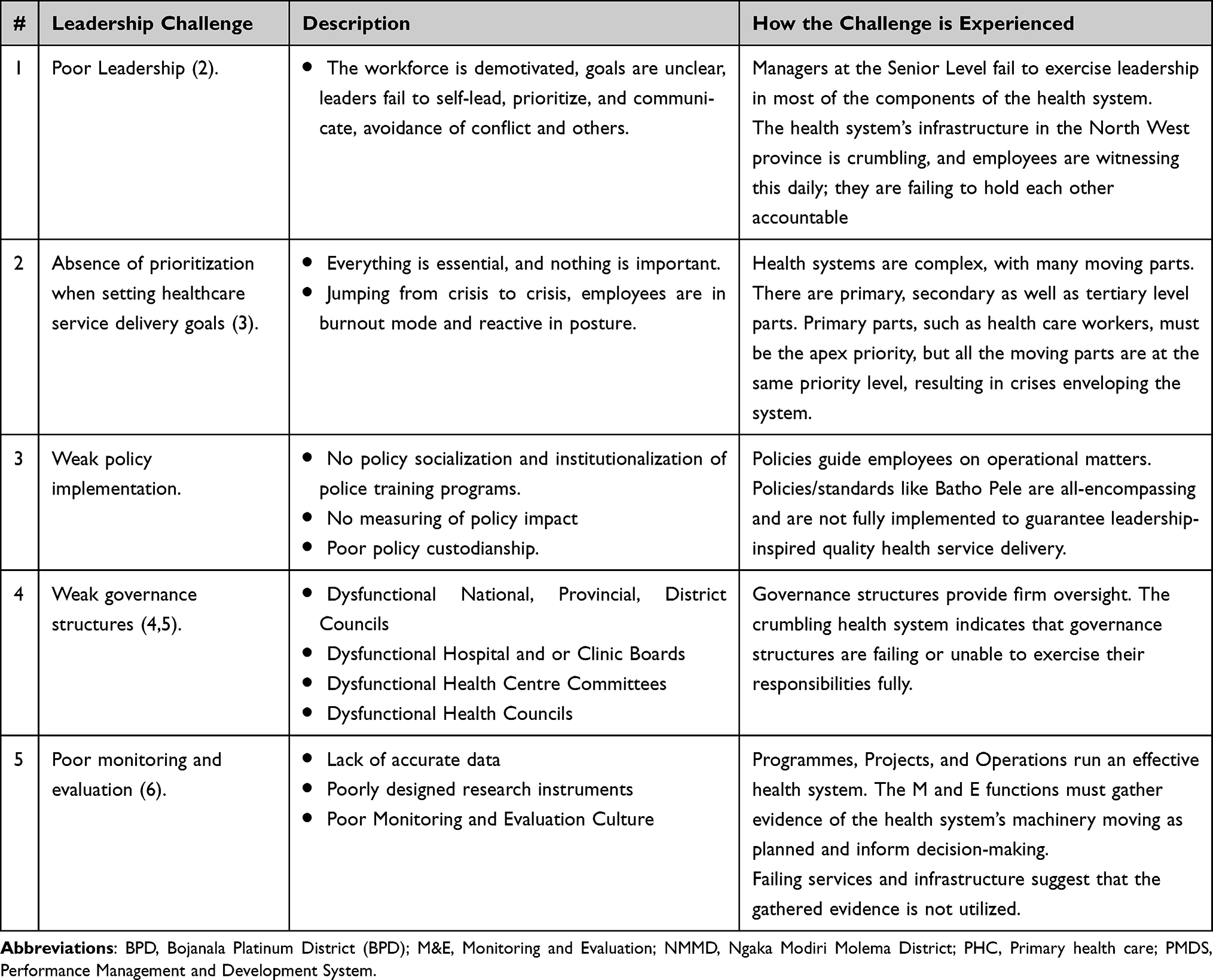 |
Table 2 Healthcare Leadership Challenges in NMMD and BPD Municipalities NW |
Limited Leadership Empowerment
Participants highlighted a lack of decision-making autonomy among local managers, who often deferred to the Head Office of the Provincial Department of Health, even for locally manageable issues.
One participant observed,
Some of our local managers lack confidence and are unable or afraid to make decisions. This behaviour makes them poor leaders who must constantly check with the Provincial Head Office for matters that should be decided locally. The start of the COVID-19 pandemic began without any guidance from the Head Office, leading to confusion at the local level. We were left to manage on our own.
This dependence on centralised directives caused delays and confusion, especially during the initial stages of the pandemic.
Furthermore, participants expressed a gap between theoretical knowledge and practical application, with one stating, “Most managers understand the theory but lack the practical ability to implement it.” This disparity between theory and practice emphasises the need to develop hands-on experience and improve practical skills to effectively apply management principles.
Ineffective Performance Management
The Performance Management and Development System (PMDS) was seen as poorly implemented, which hindered operational efficiency and the quality of healthcare. Participants recognised the PMDS’s aim to evaluate and enhance performance through quarterly and yearly reviews but observed its limited effectiveness.
The PMDS process is a quarterly and annual assessment of public servants’ work that leads to the promotion of deserving workers.
One participant explained,
The PMDS impacts operational plans, but workers need to feel appreciated and well-rewarded to deliver quality care.
Participants also emphasised that training alone was insufficient, stating,We have learned the expensive way that training alone does not solve all our service quality delivery problems. Providing quality healthcare services requires more resources than is normally understood. The cost of poor-quality healthcare services to people’s lives is immeasurable. A conducive environment where employees adopt good attitudes towards their work will improve service delivery level quality against the set goals and priorities.
Weak Policy Implementation
Participants reported inconsistent policy implementation, which hindered operational efficiency. Health policies intended to ease pressure on healthcare professionals were often delayed or not enacted. One participant remarked, “Health policies are not implemented due to slow processes or complete inaction.”
Governance structures, such as clinic committees and hospital boards, were described as non-existent or dysfunctional, with one participant noting, “Clinic committees rarely meet, and hospital boards are active but inconsistent, leading to poor oversight and limited community input.” This weak policy implementation reflects systemic governance challenges that hinder effective leadership.
Resource Allocation and Stewardship
Resource constraints, worsened by austerity measures and inadequate financial oversight, remained a persistent problem. Participants reported that the Northwest Department of Health’s (NWDoH) shrinking budget limited workforce expansion, leading to union disputes. One participant stated,
The decreasing budget prevents hiring more workers, causing union problems.
Another participant noted,The economy is not growing, unemployment, and unequal access to decent health facilities could fuel discomfort and discontentment in poor communities.
In addition,The COVID-19 pandemic constrained resource management to the maximum. As for oxygen machines and protective personal equipment (PPE), the administration allocated a sufficient budget only to what they viewed as most important from the 2020/2021 financial year.
Supply chain inefficiencies exacerbated issues, with ongoing drug shortages, especially for hypertension and diabetes medicines, recognised as an annual problem.
A participant explained, Drug shortages worsen by the financial year’s end due to exhausted funds.
Some drugs are always available because their usage is low. Medications for conditions such as hypertension, diabetes, and other chronic conditions are mostly out of stock. Managers in charge of Community Health Centres assert that the new drug supply management system is not yet helpful because even if they make timely inputs on the low level of some drugs, they are still not delivered
.Furthermore, poor maintenance of healthcare technology, such as broken equipment, hampers service delivery. One participant noted, “Equipment could work if maintenance contracts were in place, but delays, like waiting for a patient’s X-ray, frustrate professionals.” These findings highlight a critical need for better resource allocation and supply chain management.
Primary Healthcare: Governance and Service Delivery Inputs
Participants expressed concerns about the state of PHC facilities, which lacked essential resources such as medicines and functional equipment. This led to reduced patient confidence, with one participant stating, “Patients bypass PHC facilities, lacking confidence in free services perceived as poor quality.”
Our patients do not have to pay, but they access other levels of care without referrals from the primary care level. They lack confidence in the current primary health care system because, in most cases, it is under-resourced to the extent that it lacks medicines and critical equipment is broken
.Our patients do not seem confident in free services. The perception is that the service is free and poor, meant for the poor.
Weak governance structures further worsened these issues, with irregular hospital board meetings and ineffective monitoring and evaluation (M&E) practices. One participant noted, “Regional governance weaknesses prevent localised M&E, and discussed actions are rarely implemented.” Additionally, a lack of prioritisation in goal-setting was clear, with one participant describing the system as “jumping from crisis to crisis,” leading to workforce burnout and reactive management.
Table 2 offers a summary of the key challenges and impacts emphasised by participants.
Discussion
This study identified deficiencies in leadership, governance, and operational practices that hinder the delivery of quality healthcare services within two district municipalities in the North West (NW) province, South Africa. The weaknesses identified—such as limited leadership empowerment, ineffective performance management, weak policy implementation, resource allocation and stewardship, and inadequate PHC infrastructure—highlight systemic barriers to effective leadership in the North West Province’s public health sector.
While the five themes identified in this study, namely leadership empowerment, performance management, policy implementation, resource stewardship, and infrastructure and governance, are well documented internationally, our findings provide context-specific insights by illustrating how these challenges manifest within South Africa’s decentralising district health system during the early implementation of National Health Insurance (NHI). The North West Province presents a distinctive leadership environment characterised by long-standing centralisation, fiscal constraints, corruption, nepotism, and uneven managerial autonomy. Capturing the lived experiences of senior leaders operating at multiple levels (provincial, district, and facility) offers timely evidence on how these systemic pressures are navigated in practice. While confirmatory at the theoretical level, these findings promote practice by informing decentralisation strategies, performance management reform, and governance strengthening in South Africa and other low- and middle-income settings undergoing similar health financing and structural transitions.
Transformational leadership emphasises empowerment, vision, and the ability to mobilise staff; however, participants described constrained autonomy and limited authority to implement change. Complexity leadership stresses adaptability and emergent problem-solving in dynamic systems; nevertheless, entrenched bureaucratic structures and rigid fiscal controls often restrict such responsiveness.17 Systems leadership requires alignment across stakeholders and levels of care; yet, fragmented governance and inconsistent policy implementation hinder this integration.18 These tensions suggest that while global leadership models are conceptually relevant, they necessitate contextual adaptation to hierarchical, resource-limited settings undergoing health reform, such as South Africa’s NHI transition.
In Scandinavian systems, such as those in Sweden, distributed governance and protected time for leadership development allow managers to act autonomously while remaining accountable.1 Uganda and Rwanda have effectively used performance-based financing and decentralised accountability to support adaptive leadership within limited budgets.10 South Africa’s context differs due to its highly centralised legacy and ongoing NHI policy transition, indicating that such approaches need careful contextual adaptation, including enhanced fiscal oversight and leadership capacity building aligned with decentralisation. Despite widespread recognition of these leadership gaps, several factors sustain them: entrenched bureaucratic culture limits adaptive responses; performance management remains compliance-driven rather than developmental; and leadership programmes have not been integrated into district-level career pathways.
These findings also have direct implications for the quality of care provided to communities. Ineffective decentralisation and weak managerial empowerment contribute to delayed decision-making, poor responsiveness to local health needs, and low staff morale, undermining service reliability and continuity. Compliance-driven rather than developmental performance management discourages innovation and accountability. Inadequate policy implementation and fragmented governance worsen supply shortages and service gaps, while inefficient resource allocation reduces the availability of essential medicines, equipment, and skilled staff. Collectively, these factors drive facility bypassing, diminish patient confidence, and compromise service quality, which have been repeatedly documented in South Africa and other low- and middle-income countries. Our findings within this broader health systems context highlight that strengthening district-level leadership is crucial for improving service quality and achieving the goals of the National Health Insurance.
Against this backdrop of entrenched centralisation, evolving financing reforms, and the need to adapt established leadership models to a resource-limited, hierarchical context, the lived experiences shared by district and facility managers illustrate how these systemic pressures unfold in practice. The following sections present and interpret the five themes that arose from the analysis.
Limited Leadership Empowerment
This study found that dysfunction in governance structures within the healthcare system negatively impacts service delivery promises as outlined by the Department of Health’s Patients’ Rights Charter. Governance deficiencies arise from over-centralisation, where district managers defer decision-making authority to provincial headquarters, reflecting insufficient leadership competencies such as accountability, decisiveness, and motivation.3 This over-centralisation, combined with ineffective bureaucracy, leads to delays in local decision-making, resulting in healthcare system inefficiencies and deteriorating infrastructure. This finding aligns with international literature, which emphasises that empowered local leadership is vital for adaptive and resilient health systems capable of responding swiftly to crises.4
Significant disparities exist in financial and administrative delegations between provinces, with the NW province notably restricting district manager autonomy when compared to provinces like the Western Cape (WC).19 The extent of these disparities becomes clear when comparing financial delegations: for example, the NW province permits delegations of up to R200,000, whereas the Western Cape (WC) allows delegations of up to R500,000. Additional disparities include the inability of district managers in the NW to fully adjudicate and finalise supply chain management matters or to make human resources appointment decisions at the district level.
Contemporary theory in healthcare leadership indicates that current leadership practices should be characterised by (a) the ability to lead with care, (b) sharing the vision, (c) engaging the team, (d) influencing outcomes, (e) evaluating information, (f) connecting the service, (g) developing capability, and (h) holding others to account, as taught by the National Health Service in the United Kingdom5 through their Healthcare Leadership Model. A cited report by the Institute of Medicine20 emphasises that leadership is vital for achieving goals related to quality care and patient safety. This report states that leadership is expected from individuals at all levels of organisation for quality of care to be achieved.
The Healthcare Leadership Model is designed to develop better leaders who adopt transformative practices. Other studies argue that leadership must be both inclusive and adaptive to respond to the rapidly changing healthcare landscape.5
A study reviewing and synthesising existing literature to provide a comprehensive understanding of healthcare leadership concludes that leadership development programmes are essential for the ongoing development of healthcare capabilities.21
Ineffective Performance Management
Participants highlighted that the implementation of the Performance Management and Development System (PMDS) within the studied municipalities was found deficient, leading to employee dissatisfaction and decreased motivation. These findings align with a qualitative study in Namibia’s Kavango East Region, where poor PMDS implementation was attributed to inadequate training, poor system design, and lack of management involvement.6 Similarly, a study in Dr. Kenneth Kaunda District, North West Province, reported nurses’ concerns about PMDS objectivity and transparency, reflecting systemic leadership failure.7 These findings suggest that performance management systems require strong leadership support, including training and motivational strategies, to foster a culture of accountability and engagement.
Weak Policy Implementation
The study identified inconsistent policy implementation, with clinic committees and hospital boards meeting irregularly, leading to poor oversight and operational inefficiencies. This mirrors findings from a review of literature citing studies in Kenya that highlighted a policy implementation gap despite the Abuja Declaration’s mandate for increased health sector funding.22 The Kenyan study emphasised leadership’s critical role in ensuring policy execution, a sentiment echoed in this study’s findings of slow or absent policy implementation.8 The North West Province’s challenges suggest a need for leadership that enhances policy custodianship and accountability, alongside metrics to evaluate implementation effectiveness beyond mere procedural adoption.
Resource Allocation and Stewardship
The NW province faces significant resource constraints, worsened by poor financial oversight and supply chain inefficiencies. Financial limitations and supply chain issues have become major barriers to effective healthcare delivery. Participants noted ongoing shortages of essential medicines for chronic conditions such as hypertension and diabetes, worsened by fiscal austerity and ineffective procurement processes. This aligns with other research indicating that Resource Allocation and Stewardship, combined with budgetary limitations, heavily influence chronic disease management and healthcare outcomes.23,24 Poor maintenance of vital healthcare equipment weakens service delivery, indicating inadequate contractual arrangements and oversight mechanisms.
Primary Health Care Governance and Service Delivery Inputs
The study found that under-resourced PHC facilities and weak governance structures reduced patient confidence and lowered service quality. Participants noted that patients bypassed PHC facilities due to perceived poor quality, worsened by inconsistent governance and weak monitoring and evaluation (M&E). A cross-sectional study conducted in Ntungamo District, Uganda, found that the way a Monitoring and Evaluation (M&E) programme is implemented in the healthcare sector significantly affects the quality of healthcare service delivery. The study also found that, although M&E should not be considered the only factor supporting the success of an intervention, it does have a moderate impact on healthcare service quality in Uganda.25 A comparative study in Uganda and Rwanda assessing the quality of M&E systems using (i) policy; (ii) quality of indicators, data, and methodology; (iii) organisation; (iv) capacity; (v) participation of non-governmental actors; and (vi) M&E outputs concluded that the health sector M&E systems in both Rwanda and Uganda are somewhat fragmented, with some elements being weak and others strong.26 This contrasts with the M&E practices of the North West Province’s Health Department, which are viewed as poorly executed.
Absence of Prioritization in Goal Setting
The lack of prioritisation in healthcare goal setting has resulted in reactive management and workforce burnout, with participants describing a system where “everything is important, and nothing is important.” Comparative studies on priority setting in the health sector were carried out in Sweden and Norway. Norway has a long history of open priority setting in healthcare at the national level, whereas this, like in the NWP is lacking at municipal health and care levels. Although there is recognition of the importance of priority setting, scepticism and distrust exist between municipalities and the central government. This scepticism and suspicion can be addressed through stakeholder engagement and transparent decision-making to ensure effective healthcare leadership.27 In Sweden, priority setting is employed to achieve fair and efficient allocation of limited resources, adopting what is regarded as a “sophisticated approach.” A study assessing Swedish physicians’ perspectives on (I) the impact of scarce resources on patient care; (II) clinical decision-making; and (III) the ethical framework and national guidelines for healthcare by the National Board of Health and Welfare concluded, among other things, that priority setting is a potential pathway to fair and transparent decision-making in clinical settings, with particular emphasis on the ethical platform.28 NW province’s healthcare system lacks structured prioritisation processes, emphasising the need for interventions aimed at establishing transparent, inclusive, and evidence-based priority-setting mechanisms grounded in an ethical platform. This can be facilitated through healthcare leadership practices advocated by the NHS Leadership Model.
Limitations
The study’s focus on two district municipalities and a sample consisting of senior management personnel may restrict the generalisability of the findings. Furthermore, potential social desirability bias arising from the researcher’s position necessitates careful interpretation of results. However, the use of purposive sampling and triangulation through FGDs and IDIs improves the credibility of the findings within the studied context. While this qualitative approach offers detailed contextual insights, future research could supplement it with quantitative methods to assess the prevalence and significance of the identified leadership challenges and examine their associations with health system performance indicators.
Conclusion
The findings emphasise systemic leadership challenges that weaken the North West Province’s health system, particularly in terms of the quality of care. While confirming globally recognised leadership gaps, this study provides practical, context-specific insights into how entrenched centralisation, financial constraints, and NHI policy changes influence district-level leadership. It expands on transformational, complexity, and systems leadership models by demonstrating how they need to be adapted to hierarchical, resource-constrained environments. Practically, the findings recommend devolving decision-making authority with clear financial accountability, adopting a developmental rather than merely compliance-based performance management approach, and institutionalising ongoing leadership development for the district.
Acknowledgments
We are grateful to the Northwest Department of Health for allowing us to conduct the study, the CEOS and managers of both districts for their participation, and my research assistant, Keitumetse Masike, for her patience.
Disclosure
The author(s) declare no conflicts of interest in this work.
References
1. Barros Leal Farias D. Which countries are ‘developing’? Comparing how international organizations and treaties divide the world. Political Geograph Open Res. 2022;1:100001. doi:10.1016/j.jpgor.2022.100001
2. Malakoane B, Heunis JC, Chikobvu P, et al. Public health system challenges in the Free State, South Africa: a situation appraisal to inform health system strengthening. BMC Health Serv Res. 2020;20(1):58. doi:10.1186/s12913-019-4862-y
3. Achoki T, Sartorius B, Watkins D, et al. Health trends, inequalities and opportunities in South Africa’s provinces, 1990-2019: findings from the global burden of disease 2019 study. J Epidemiol Community Health. 2022;76:471–481.20220119. doi:10.1136/jech-2021-217480
4. Manji K, Perera S, Hanefeld J, et al. An analysis of migration and implications for health in government policy of South Africa. Int J Equity Health. 2023;22(1):
5. North West Department of Health. Annual Report for 2023/24 Financial year Vote 3: Department of Health. Mahikeng: North West Department of Health; 2024.
6. Statistics South Africa. Statistical Release P0302 Mid-year Population Estimates, 2024. Pretoria: Statistics South Africa; 2024.
7. National Perinatal Morbidity and Mortality Committee. Saving babies 2020 ‐ 2022. triennial report of the national perinatal morbidity and mortality committee. 2022. Pretoria: National Department of Health.
8. Ndlovu N, Gray A, Mkhabela B, et al. Health and related indicator. In: Padarath A, Moeti TL, editors. South African Health Review 2022. Durban: Health Systems Trust; 2022.
9. Al-Rjoub S, Alsharawneh A, Alhawajreh MJ, Othman EH. Exploring the impact of transformational and transactional style of leadership on nursing care performance and patients outcomes. J Healthcare Leadership. 2024;16:557–568. doi:10.2147/JHL.S496266
10. Dzokoto MK, Mensah BT, Agbenu IA, Gatheru PM, Kwashie MD, Boateng KA. Leadership, management style and influence on healthcare worker’s job satisfaction and productivity: a scoping review, international journal of community medicine and public health. 2024. doi:10.18203/2394-6040.ijcmph20241859
11. Olatoye FO, Elufioye OA, Okoye CC, Nwanko EE, Oladapo JO. Leadership styles and their impact on healthcare management effectiveness: a review. International Journal of Science and Research Archive. 2024. doi:10.30574/ijsra.2024.11.1.0271
12. Restivo V, Minutolo G, Battaglini A, et al. Leadership effectiveness in healthcare setting: a systematic review and meta-analysis of cross-sectional and before-after studies, international of environment research and public health. 2022. doi:10.3390/ijerph191710995
13. Kaehne A, Feather J, Chambers N, et al. (2022): Rapid review on system leadership in healthcare: system leadership: what do we know and what do we need to find out? Edge Hill University, Available from: https://research.edgehill.ac.uk/ws/portalfiles/portal/49690310.
14. Gubdumogula M. The importance of focus groups in qualitative research, the international journal of humanities and social studies, Available from: https://hal.univ-lorraine.fr/hal-03126126/document.
15. Habibullah KM, Hamza M. Conceptual framework in the reflexive bracketing techniques in qualitative methodology, researchgate, Available from: https://www.researchgate.net/publication/373546586.
16. Kiger M, Varpio L. Thematic analysis in qualitative data: AMEE guide No. 131, medical teacher. 2020. doi:10.1080/0142159X.2020.1755030
17. McLeod S. Narrative analysis in qualitative research, researchgate, Available from: https://www.researchgate.net/publication/381926283.
18. Away F, Simamora B, Nadeak S, et al. Decentralization, centralization and quality of organizational performance of human resources. Acad Strategic Management J. 2021;20:1–12.
19. Jennings BM, Disch J, Senn L. Chapter 20. leadership, patient safety and quality: an evidence-based hand for nurses. 2008;2.
20. Sikalgar FR, Bangera D, Kumar MP, Bhuvaneshwari Paul Y, Muralidharan S. A review of leadership theories in healthcare. J Pharm Bioallied Sci. 2025;27. doi:10.4103/jpbs.jpbs_1907_24
21. Kumar RDC, Khiljee N. Leadership in healthcare. Anaesth Intensive Care Med. 2016;17(1):63–65. doi:10.1016/j.mpaic.2015.10.012
22. Rasa J. Developing effective health leaders: the critical elements for success. J Hospital Management Health Policy. 2020;2020.
23. Nahabwe J, Basheka BC, Mucunguzi A. Monitoring and evaluation of the quality of healthcare service delivery in Ntungamo District, Uganda, African journal of governance and public leadership, Available from: https://ajogpl.kab.ac.ug/index.php/1/article/view/86/.
24. Holvoet N, Inberg L. Taking Stock of monitoring and evaluation systems in the health sector: findings from rwanda and uganda, health policy and planning. Health Policy Plan. 2014;29(4):506–516. doi:10.1093/heapol/czt038
25. Torjusen ML, Feiring E, Barra M, Vollestad NK, Solberg CT. Priority setting in Norwegian municipal and health care services: a thematic analysis of public consultation documents, Scandinavian University Press. 2024;2025. doi:10.18261/tfo.10.2.9
26. Drees C, Krevers B, Ekerstad N, et al. (2021): Clinical priority setting and decision-making in sweden: a cross-sectional survey among physicians, international journal for health policy management, Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC98008196/6.
27. World Health Organisation. (2022): Global competency and outcomes framework for universal health coverage, Geneva:WHO, Available from: https://www.who.int/publications/i/item/9789240034686.
28. National Health System Academy. Healthcare leadership model, ACT academy, Available from: https://cms.bps.org.uk/sites/default/files/2022-07/.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.