Back to Journals » Open Access Journal of Contraception » Volume 10
“When you least expect, this happens, it’s already growing”: Problematizing the definition of unmet need for family planning
Authors Khalil I ![]() , Richardson EZL
, Richardson EZL ![]()
Received 23 August 2018
Accepted for publication 16 January 2019
Published 29 May 2019 Volume 2019:10 Pages 7—18
DOI https://doi.org/10.2147/OAJC.S184909
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Igal Wolman
Ielaf Khalil,1,2 Emma ZL Richardson1,2
1Centre for Ethical, Social and Cultural Risk, Li Ka Shing Knowledge Institute of St. Michael’s Hospital, Toronto, Ontario, Canada; 2Department of Health Research Methods, Evidence, and Impact, McMaster University, Hamilton, Ontario, Canada
Background: Unmet need is an important indicator to understand baselines and set goals for family planning interventions. Women may not fall neatly in categories of met or unmet need for family planning as defined by the demographic and health surveys (DHS). We explore women’s experiences of unmet need for family planning and provide empirical examples of how the static, binary DHS definitions of met and unmet need for family planning may be problematic.
Methods: Based on Social Cognitive Theory, we conducted elicitation interviews with 16 married young women between the ages of 20 and 24 in Chimaltenango, Guatemala to explore barriers to accessing and using family planning. Half the participants (n=8) were using a modern method of family planning and half (n=8) were not. The current analysis focuses on data that was coded as ambiguous or unclear for unmet need status.
Results: We identified framings of ambiguity from the women’s narratives that are silenced by the dominant binary of met and unmet need. We show inconsistencies between women’s lived experiences of unmet need and how their experiences would likely be represented in DHS questionnaires: 1) successful use of natural methods; 2) the complexity of “wantedness”; 3) conceptualizing met or unmet need as a trajectory; and 4) laughter obscuring clear response.
Conclusion: Family planning status is a complex trajectory that the DHS may not accurately capture. As a way to reflect the diversity of women’s family planning experiences, we suggest modifying the DHS classifications to incorporate latent met and unmet need as sub-classifications.
Keywords: contraception, pregnancy intention, qualitative research methods, Latin America and the Caribbean
Introduction
Family planning refers to the use of modern contraceptives to limit or space pregnancies. A woman’s ability to space and limit her pregnancies has direct consequences for her health and wellbeing.1 The objective of family planning interventions is to meet the demand for contraception and decrease unmet need.2 Investing in family planning has been deemed critical for achieving progress on the five themes of the sustainable development goals (SDGs), agreed upon in 2015.3,4 It has been suggested that universal access to family planning could make all the SDGs achievable.3 Yet approximately 225 million women worldwide still have unmet need for family planning, primarily in developing countries.1
Unmet need for family planning is a key family planning impact indicator5 and has been used as a central measure for monitoring family planning programs for decades.2 It is defined as the number of currently married women who do not want more children but are not using any form of family planning (unmet need for limiting) or who want to postpone their next birth for 2 years but are not using any form of family planning (unmet need for spacing).6 This indicator is calculated through intricate analysis of 15 different responses from the demographic and health surveys (DHS). The flowchart illustrating the classification based on DHS questionnaire responses is presented in Figure 1.7 The calculation was revised in 2012 to be more consistently applied over time and across countries.7
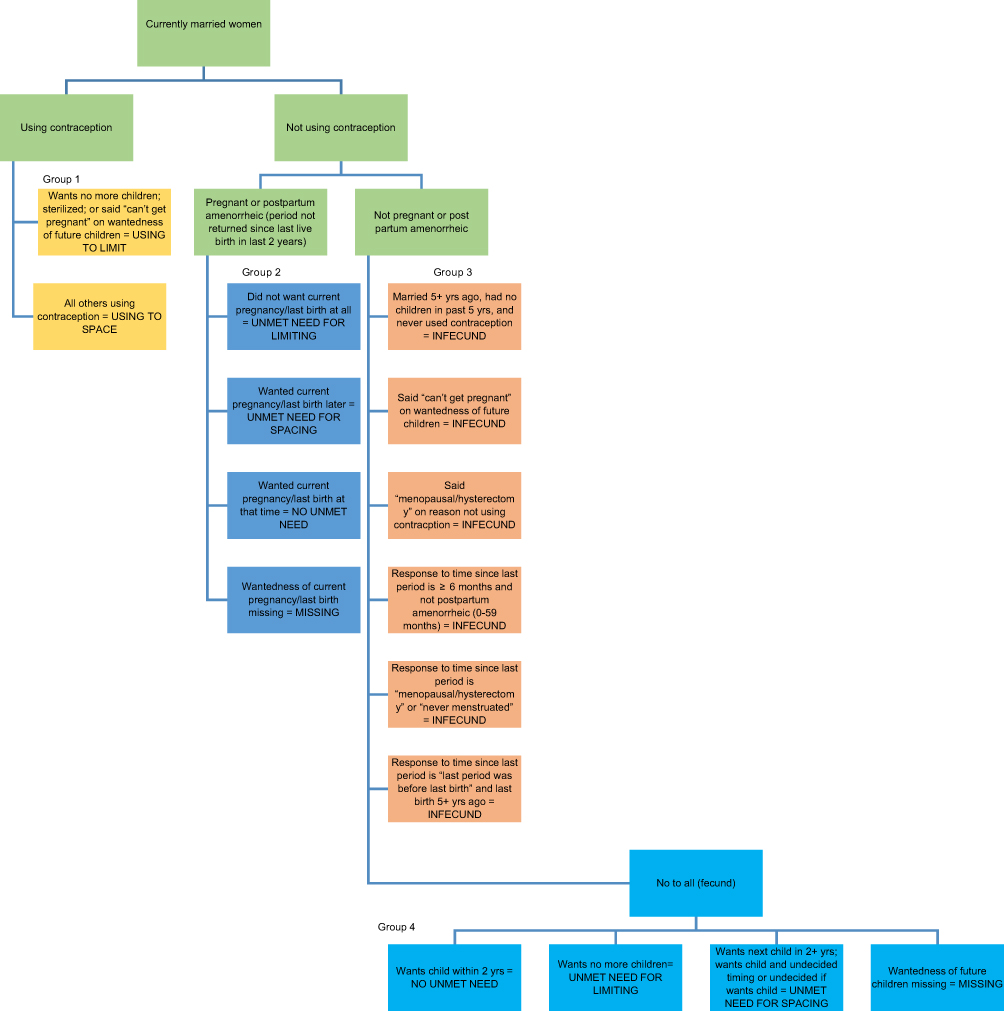 | Figure 1 Flowchart illustrating classification of unmet need based on DHS questionnaire responses.; Reprinted with permission from Bradley, Sarah E.K., Trevor N. Croft, Joy D. Fishel, and Charles F. Westoff. 2012. Revising Unmet Need for Family Planning. DHS Analytical Studies No. 25. Calverton, Maryland, USA: ICF International.7 |
The objective of this paper is to explore indigenous women’s experiences of family planning in rural Guatemala and examine how they fit within the definitions of met or unmet need for family planning as defined by the DHS. Exploring unmet need for family planning in Guatemala is important, as contraceptive use is low overall, but particularly among the marginalized group of indigenous, rural women.8
Material and methods
This data was collected as part of broader research examining access to family planning in highland Guatemala.9 According to Social Cognitive Theory, 16 elicitation interviews were carried out by the first author with married women aged 20–24 years in Chimaltenango, Guatemala. Participants were purposively sampled for equal representation of users (n=8) and nonusers (n=8) of contraception. Of the nonusers, half (n=4) wanted to delay childbearing by 2 years or more and thus met the definition of having an unmet need for family planning.9
Suggested questions for elicitation research in the literature informed the semi-structured interview guide.10,11 Questions adapted from previous instruments such as the DHS were used to ask women about their contraceptive knowledge, behavior, and sociodemographic variables.12 The interview guide is provided as a supplementary file. The interview guide was translated from English to Spanish to Kaqchikel, a local Mayan language. Participants were recruited from two rural districts of Patzún, Chimaltenango by the research assistant, a young Kaqchikel female, through the help of a local NGO (non-governmental organization), Renacimiento. Women were approached at home to explain the study, and asked screening questions to ensure users and nonusers of contraception were recruited. Interviews were mostly conducted in the participants’ homes during the day when their husbands were not home. When privacy was a concern, the interview was conducted in the local health center. The research assistant was present in all the interviews and translated between Kaqchikel and Spanish as needed. Interviews were conducted from May to July 2013, audio-recorded and transcribed verbatim. Original content in Kaqchikel and Spanish was analyzed in both languages by the investigator and the research team using content analysis and the constant comparison method. Codes were developed, revised, and then organized into themes related to barriers for accessing and using family planning. NVivo 9 software was used to manage data analysis. Details on methodological and ethical aspects of this intercultural research study are published elsewhere.9,13 A COREQ checklist for qualitative studies is provided as a supplementary file.
The results presented in this paper draw from analysis of quotes that were coded as, “clear case of unmet need or not,” “ambiguous case of unmet need or not unmet need,” and “unmet need for family planning – ambiguous or clearcut.”
Results
Description of study participants
Sixteen Kaqchikel Indigenous women from two rural districts of Patzun, Chimaltenango, Guatemala participated in the interviews. The participants ranged from 20–24 years of age (mean=22.4) (Table 1).
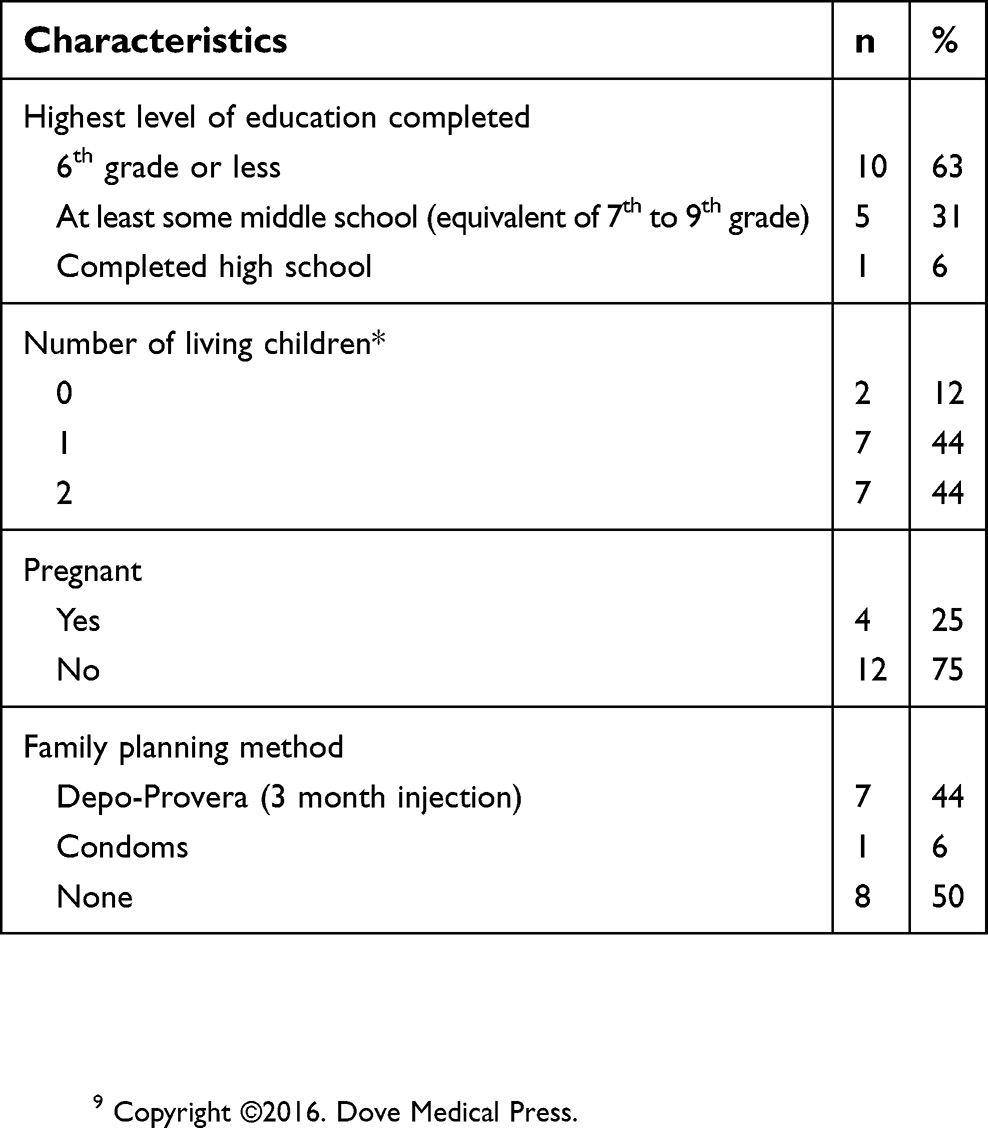 | Table 1 Descriptive characteristics of study participants (n=16) |
Clear case of met need for family planning
Some participants had a clear case of met need for family planning that would be captured accurately by a cross-sectional tool, such as a DHS questionnaire. For example, one participant used the 3-month injection, Depo-Provera, in order to space her pregnancies:
I“Yes? Which method are you using?”
R“The 3 month injection.”
Using the DHS flowchart for classifying met or unmet need for family planning (Figure 1), this woman would be classified as Group 1–Using to Limit.
Another clear case was a participant who was not currently using a family planning method but who wanted a child and was currently pregnant.
P“No, not any more, I mean, now [I’m not using family planning]… I’m expecting another baby.”
I“Ah yes, yes I see. So now you are expecting another baby?”
P“Yes.”
I“Yes. And when you got pregnant, now that you are pregnant, did you want another child now, or did you want to wait a bit before having another son or daughter?”
P“Well, when… I mean… When I wanted to be pregnant, I told my husband that yes, I wanted another child, or another baby.”
This woman would be classified as Group 2–No Unmet Need (Figure 1).
Clear case of unmet need for family planning
Similarly, one participant had a clear or classic case of unmet need for family planning that would be accurately captured by the DHS. This woman was not using any family planning methods but wanted to wait three more years before having another child.
P“Um, for the moment [I would not use family planning] maybe not yet, no, but for the future maybe yes.”
I“Maybe yes?”
P“Yes. Maybe yes.”
I“And how long would you like to wait before having your next child?”
P“In three years”
I“Three more years?”
P“Three more years.”
This woman would be classified as Group 4–Unmet Need for Spacing (Figure 1).
Ambiguous cases of met or unmet need for family planning
Some participants did not clearly fall within DHS classifications for met or unmet need. We describe how these participants’ responses may in some cases misclassify or fail to capture their met or unmet need for family planning.
Successful use of traditional methods
Women who are using traditional methods and who wish to limit or delay a pregnancy are considered to have an unmet need because they are not using a modern method of family planning. Several participants were using traditional methods. One woman, for example, had used a traditional method during her first year of marriage to successfully delay pregnancy. Yet despite the successful use of a traditional method, this woman would still be classified as having an unmet need on the DHS.
P“Well, we [my husband and I] were thinking that it was time for us to have a child [after one year of being married].” Well yes. Like one is a bit more prepared. Already economically. Or maybe already with the necessary things. Because when one is already pregnant… or one just gets together and can become pregnant, but one is not ready. So we were deciding that it was better to wait a bit, get a bit of money, and like that.
I“This was when you were married?”
P“Aha.”
I“And were you using a method at the beginning of your marriage?”
P“At the beginning, well, we used the collar [rhythm method]
I“The rhythm method. Aha. A traditional method?”
P“Yes.”
I“Right, so this was what you did during your first year [of marriage]?”
P“Yes.”
I“And then after this you stopped, or, then you weren’t so worried about it [using the rhythm method], because you had decided you wanted to have children?”
P“Yes.”
Complexity of “wantedness”
For pregnant or postpartum amenorrheic women who are not using contraception (Group 2 in Figure 1), the “wantedness” of the pregnancy or the last birth at that time determines whether a woman is classified as having an unmet need or not. The complexity and ambiguities of “wantedness” were apparent in the interviews with participants. Participants’ responses were not always clear cut in terms of “wantedness.” As one participant explains:
I“And when you became pregnant, in that moment did you want to have a baby or would you have preferred to wait?”
P“I would say maybe yes in that moment, I don’t know. So we didn’t realize, because one wants a bit of time to think about it, but when you least expect it, this happens. Well it’s God’s blessing: seeing it, it’s already growing.”
Another participant explains that her pregnancy was not planned earlier in the interview but when asked whether it was desired, her response is equivocal.
I“I just wanted to confirm, your son is… how many months old is he?”
P“Um 9… Now he is 10 months old”
I“Right. And you told me this is your first son, right?”
P“Yes.”
I“And when you became pregnant, was it that you already wanted children, or you wanted to wait a bit longer before having children?”
P“Who knows? I don’t know. Well… [in Kaqchikel]
Research assistant: “You see; they had not planned it. Aha. It just happened.”
I“It just happened, right? But once you were pregnant, was it something that you wanted, or not?”
P“Well yes, once it’s like that, one has to be… well yes, yes.”
I“Yes?”
P“Aha.”
Unmet or met need as a trajectory
Over the course of the interview, some participants revealed details that would change their initial classification. Met or unmet need for family planning status can be seen as a trajectory and pinpointing one moment in time may obscure met or unmet need. Two participants who were classified through the DHS questionnaire as having a met need indicated that their previous pregnancies had been mistimed. These women were classified as having a met need because they were currently using contraception to space their pregnancies (Group 1 in Figure 1). Whether the women had wanted their previous pregnancies at the time or not would be relevant to the DHS, as they are using contraception. For example, one of these participants had only just started using Depo-Provera. If the DHS questionnaire had been administered just 3 months earlier she would have not been using contraception and the “wantedness” of her recent pregnancy would have been a relevant consideration to determine her met or unmet need (Group 2 in Figure 1).
For other participants, a latent met or unmet need for family planning became apparent as the interview progressed.
Throughout the course of the interview, two participants revealed that they were planning to start using family planning methods in the future. These women would be classified by the DHS as having an unmet need. However, their plans to use contraception in the near future indicate a latent met need for family planning. Met need status for these women is concealed but likely to be soon realized.
I“What do you think about family planning?”
P“That it’s good to practice, because it helps for the child to grow well and not to have another one so soon. Well for me, I’d like to use it, or, we’re planning to use it [family planning].”
I“Since you’ve been thinking of using a method like the pill, or something, when were you thinking of starting?”
P“Well: this month.”
Latent unmet need
For another participant, a latent unmet need for family planning became apparent. This participant would be classified by the DHS as having a met need as her last pregnancy was wanted and her menstruation had yet to return (Group 2 in Figure 1). She explained that she was interested in using family planning in the future but over time revealed that her husband and family would not be supportive, and this would be prohibitive for her using family planning. Therefore, in the future, she will likely have an unmet need for family planning.
Laughter obscuring clear response
Participants laughed frequently when asked about family planning.
For example, some participants laughed when asked if they were using family planning or why they were not:
I“Some couples use different ways or methods to space or avoid a pregnancy, are you currently using some kind of method?”
P“No, no.”
I“And why not?”
P“No, no (laughter). I don’t think of anything.”
And
I“So in your case, um, why are you not using methods at the moment?”
P“In my case? Well, I don’t know, because, not yet (laughter).”
Others laughed when questioned about the timing of the pregnancy and whether they had wanted to wait:
P“We waited a year [before becoming pregnant with our daughter].”
I“Right. And would you have wanted to wait a bit longer? Or were you wanting to have a child right away?”
P“I don’t know (laughter). Well we were thinking it was time to have a child…”
And
I“And for the baby you have now; did you want to have this baby now or did you want to wait?”
P“Mmm, [He] wanted to have it, but already (laughter).”
Laughter is likely used by women as a way to deflect questions about family planning, which may be an uncomfortable topic in this context. However, in some cases, after continuing to establish trust during the semi-structured interview, participants were more specific in their responses to questions about family planning. In contrast, DHS questionnaire administrators, who ask women why they are not using a method to prevent pregnancy, are provided with a running list of reasons to check off. We suspect that the commensurate trust may not be gained through a cross-sectional survey such as the DHS, leading to incomplete or inaccurate responses.
Discussion
Our findings illustrate the complexity of women’s family planning status and the framings of ambiguity from women’s narratives that may make it difficult to classify a woman using the current DHS questionnaires, illustrated in Figure 1. Some participants could be classified easily using the DHS questionnaire, as shown by the examples of clear cases of met or unmet need. This was not the case for many others, whose experiences of family planning are silenced by the dominant static binary of met and unmet need for family planning.
Our data show that a women’s family planning status should be understood as a dynamic trajectory rather than a static experience. As a way to reflect the diversity of women’s experiences with regards to family planning, we suggest modifying the DHS classifications to incorporate latent met and unmet need as sub-classifications. For example, women who indicate they would use a modern family planning method in the future would be categorized as having a latent met need. These women have indicated their intention to use family planning and some may have previous experience using methods. They also represent low-hanging fruit for policymakers hoping to reduce unmet need for family planning because their previous family planning experience or current family planning intentions make them more likely to use family planning once access is ensured. A question about future intentions to use contraception already exists in the DHS (Q812), however, data from this question has been underused, with some exceptions, such as in Morocco, where contraceptive intentions were found to be strong predictors of future use.14 These findings run parallel to those of others who have called for more categories of met and unmet need; , and found real met need, real no need, perceived no need, and perceived unmet need, all to be useful categories for family planning policy in Benin and Mali.15
Unmet need, as a static measure, does not capture the changes to a woman’s status over time.16 Our findings support a growing evidence base that the need for family planning should be treated as a trajectory rather than static dichotomy. Research from Malawi has recommended sequencing family planning behaviors over time and examining a couple’s relationship for a more comprehensive understanding of unmet need as behaviors are not only dynamic over time but relationship-specific.17 Empirical evidence from rural Ghana also asserts that reproductive preferences or intentions are not stable over time.18
Our data suggest that there should be a greater acknowledgment of traditional family planning methods. This is exemplified by the participant who successfully used traditional methods to space her pregnancies. Findings from a study in Burkina Faso suggest the lack of follow-up questions regarding traditional methods on the DHS questionnaire may result in underreporting of these methods.19 In Ghana, traditional methods, often used in combination with modern methods, are also not captured adequately.20 There is some evidence of the effectiveness of traditional methods as studies of modern fertility awareness-based methods, such as the Standard Days Method, have shown comparable rates of effectiveness to modern contraceptives.21,22 There is also a growing interest in improving the knowledge of and determining the effectiveness of web and app-based fertility-awareness-based methods.23,24 It has been suggested that these new solutions are needed in order to address the large number of women with unmet need worldwide.25 However, in order to achieve this, the current DHS definition of unmet need must first be modified to recognize these modern traditional methods.
In a given context, a woman’s understanding of the “wantedness” of a pregnancy must be understood more completely. This was exemplified by the participants who described their pregnancies as mistimed yet still viewed them as wanted because “it’s God’s blessing” or “one has to be”. Others have posited that the concept of the right or wrong timing of a pregnancy, may not be adequately captured as dichotomous variables.26 Additional questions to probe a woman’s understanding and expression of the “wantedness” of her pregnancy may be needed. The retrospective questioning of the “wantedness” of a pregnancy or recent birth, posed to pregnant and amenorrheic women, is problematic and subject to ambiguity due to the differences in understanding of terms such as wanted/unwanted, planned/unplanned and intended/unintended.27,28
Many participants laughed and had trouble articulating an answer about the timing of their last birth or when asked about the reasons for not using modern methods. In this context, the laughter may be an indication of the discomfort women feel discussing family planning, a taboo topic in Guatemala in general and particularly for Indigenous women.13,29 Similarities may be found in other contexts where discussing sex is taboo. However, through the course of an interview and after the building of a rapport, women reveal details they may otherwise not have been comfortable enough to reveal in a short, cross-sectional survey such as the DHS. Consequently, we argue that policy solutions directed at meeting the unmet need for family planning would benefit from qualitative research, such as the elicitation interviews conducted in this study, to provide a fuller and in some cases more accurate understanding of met or unmet need for family planning.
Our study has several limitations. Our sample was limited to young, married Indigenous Guatemalan women. It is possible that a larger sample including women at different stages of their reproductive years may have yielded additional themes. Qualitative research is not meant to provide statistically generalizable results and similar analyses in different contexts should also be conducted. However, the results of this study may hold true in similar contexts.
Conclusion
The empirical examples from the in-depth elicitation interviews in this study provided insight into how women’s experiences of family planning may be silenced by the dominant static and binary definition of met versus unmet need for family planning. They illustrate the complexity of women’s family planning status and the ambiguities in classification. Examining family planning status as a trajectory through qualitative investigations can provide a deeper understanding of a woman’s current, past and future family planning status. We suggest incorporating a sub-classification of latent met and unmet need to the current DHS classifications to help capture the diversity in women’s experiences of family planning. We hope that others will continue to explore the complexities of the lived experience of unmet need for family planning in different contexts to improve the framing of this important indicator.
Abbreviation list
DHS, demographic and health surveys; MDG, millennium development goal; SDG, sustainable development goal; NGO, non-governmental organization.
Ethics approval and informed consent
Research ethics approval for this project was obtained from the ethics committee of the University del Valle in Guatemala and the Health Sciences Research Ethics Board of the University of Toronto in Canada. Informed written consent was obtained from all participants prior to the interviews.
Consent for publication
Consent to publish was obtained through the informed consent forms.
Data availability
Data sharing of the qualitative data sets is not possible as this would jeopardize participants’ anonymity.
Acknowledgments
The authors thank the Renacimiento and Population Council Organizations in Guatemala; research assistants Silvia Tum and Hermelinda Teleguario; and research consultant Wankar Chacach. This research was supported by funding from the Canadian Institutes of Health Research and the Institute for Global Health Equity and Innovation at the University of Toronto. The funding bodies did not have a role in the study design or data collection, analysis, or interpretation.
Author contributions
ER is the senior author who conceptualized and designed the study, collected the data and played a substantial role in the analysis and interpretation of data. IK was involved in data analysis and interpretation and was a major contributor in writing the manuscript. Both authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1.
2. Cleland J, Harbison S, Shah IH. Unmet need for contraception: issues and challenges. Stud Fam Plann. 2014;45(2):105–122. doi:10.1111/j.1728-4465.2014.00380.x
3.
4. Starbird E, Norton M, Marcus R. Investing in family planning: key to achieving the sustainable development goals. Glob Heal Sci Pract. 2016;4(2):191–210. doi:10.9745/GHSP-D-15-00374
5. Norton M, Johnson B, Bayer E, et al. United States Agency for International Development Bureau for Global Health Office of Health. Washington, DC: Disease, and Nutrition Child Survival and Health Grants Program (CSHGP) Technical Reference Materials Family Planning; 2013.
6. Westoff CF New estimates of unmet need and the demand for family planning. DHS Comparative Reports No. 14. Calverton, Maryland; 2006.
7. Bradley SEK, Croft TN, Fishel JD. Revising Unmet Need for Family Planning: DHS Analytical Studies No. 25. 2012;(January):63.
8. Figueroa W, Lopez F, Remez L, Prada E, Drescher J. Early childbearing in Guatemala: a continuing challenge. Issues Brief (Alan Guttmacher Inst). 2006;(5):1–20. Available from:
9. Richardson E, Allison K, Gesink D, Berry A. Barriers to accessing and using contraception in highland Guatemala: the development of a family planning self-efficacy scale. Open Access J Contracept. 2016;7:77. doi:10.2147/OAJC.S95674
10. Montano D, Kasprzyk D. Theory of reasoned action, theory of planned behavior, and the integrated behavioral model. In: Glanz K, Rimer B, Viswanath K, editors. Health Behavior and Health Education.
11. Middlestadt SE, Bhattacharyya K, Rosenbaum J, Fishbein M, Shepherd M. The use of theory based semistructured elicitation questionnaires: formative research for CDC’s prevention marketing initiative. Public Health Rep. 1996;(Suppl 1):18–27. Available from:
12.
13. Richardson EZL, Allison KR, Teleguario H, et al. “Taking care” in intercultural research. Int J Qual Methods. 2017;16(1):160940691668082. doi:10.1177/1609406916680823
14. Curtis SL, Westoff CF. Intention to use contraceptives and subsequent contraceptive behavior in Morocco. Stud Fam Plann. 1996;27(5):239–250. Available from:
15. Sinai I, Igras S, Lundgren R. A practical alternative to calculating unmet need for family planning. Open Access J Contracept. 2017;8:53–59. doi:10.2147/OAJC.S137705
16. Jain AK, Obare F, RamaRao S, Askew I. Reducing unmet need by supporting women with met need. Int Perspect Sex Reprod Health. 2013;39(3):133–141. doi:10.1363/3913313
17. Furnas HE. Capturing complexities of relationship-level family planning trajectories in Malawi. Stud Fam Plann. 2016;47(3):205–221. doi:10.1111/j.1728-4465.2016.00064.x
18. Debpuur C, Bawah AA. Are reproductive preferences stable? Evidence from Rural Northern Ghana. Genus. 2002;58:63–89. Available from:
19. Rossier C, Senderowicz L, Soura A. Do natural methods count? Underreporting of natural contraception in Urban Burkina Faso. Stud Fam Plann. 2014;45(2):171–182. doi:10.1111/j.1728-4465.2014.00383.x
20. Marston C, Renedo A, Nyaaba GN, Machiyama K, Tapsoba P, Cleland J. Improving the measurement of fertility regulation practices: findings from qualitative research in Ghana. Int Perspect Sex Reprod Health. 2017;43(3):111. doi:10.1363/43e4517
21. Arévalo M, Jennings V, Sinai I. Efficacy of a new method of family planning: the standard days method. Contraception. 2002;65(5):333–338. doi:10.1016/S0010-7824(02)00288-3
22. Manhart MD, Duane M, Lind A, Sinai I, Golden-Tevald J. Fertility awareness-based methods of family planning: A review of effectiveness for avoiding pregnancy using SORT. Osteopath Fam Physician. 2013;5(1):2–8. doi:10.1016/j.osfp.2012.09.002
23. Duane M, Contreras A, Jensen ET, White A. The performance of fertility awareness-based method apps marketed to avoid pregnancy. J Am Board Fam Med. 2016;29(4):508–511. doi:10.3122/jabfm.2016.04.160022
24. Fehring RJ, Schneider M, Raviele K, Rodriguez D, Pruszynski JE. Randomized comparison of two internet-supported methods of natural family planning randomized comparison of two internet- supported fertility awareness based methods of family planning. Contraception. 2013;88(1):24–30. doi:10.1016/j.contraception.2012.10.010
25. Simmons RG, Shattuck DC, Jennings VH. Assessing the efficacy of an app-based method of family planning: the dot study protocol. JMIR Res Protoc. 2017;6(1):e5. doi:10.2196/resprot.6886
26. Askew I. Unmet need and unintended pregnancy: the bigger picture. Population Council; 2013. Available from:
27. Barrett G, Wellings K. What is a “planned” pregnancy? empirical data from a British study. Soc Sci Med. 2002;55:545–557. Available from:
28. Miller WB, Jones J. The effects of preconception desires and intentions on pregnancy wantedness. J Popul Res. 2009;26:327–357. doi:10.2307/41110945
29. Chirix García ED. Los cuerpos y las mujeres kaqchikeles. Desacatos. 2009;30:149–160.
Supplementary materials
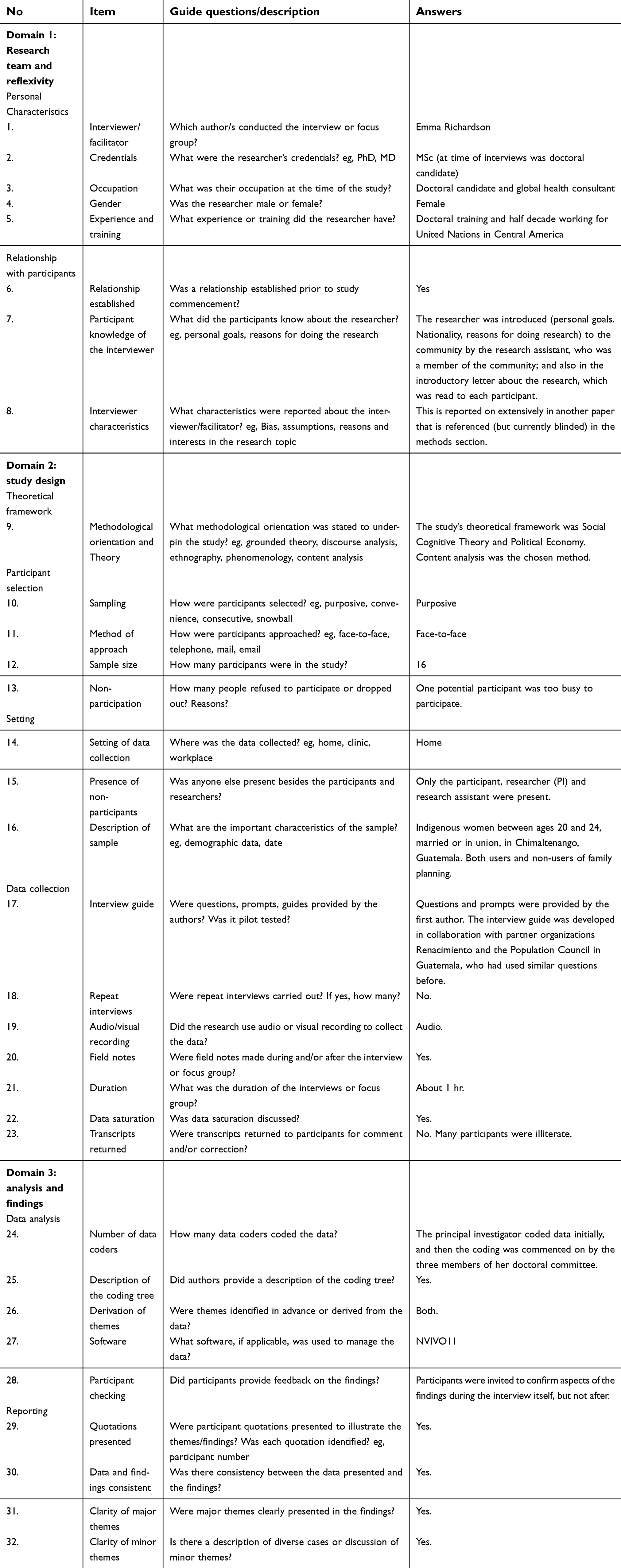 | Table S1 Consolidated criteria for reporting qualitative studies (COREQ): 32-item checklist |
Elicitation Interview Guide
Screening questions:
How old are you?
[The following screening questions will only be asked if one of the categories of respondents is already close to being filled:]
Would you like to have (a/another) child, or would you prefer not to have any (more) children?
If want a/another child – how long would you like to wait from now before the birth of (a/another) child?
Some couples use various ways or methods to delay or avoid a pregnancy. Are you currently doing something or using any method to delay or avoid getting pregnant?
If yes, which method are you using?
[If participant fits into a category for which enough interviews have already been carried out, this will be explained to the participant. If not, the interview will continue].
General information
What is your name?
What is your ethnicity?
Which languages do you speak?
How old are you?
Schooling & work
Did you go to school?
Do you still go to school?
If yes – which grade are you in?
If no – what is the highest grade you completed?
Are you able to read and write?
Are you working in a paid job at the moment? If yes, which job?
General ideas about family and pregnancy
Among your friends and sisters, how do you talk about pregnancy and having a family? [Probe as necessary: Are children something that is planned or not planned?]
Current – marriage and children
Are you currently married or living together with a man as if married?
Have you ever been pregnant?
Do you have any children?
If yes, how many?
Have any of your children died?
[If the answer is yes, offer a supportive response such as “I’m sorry to hear that”]
Are you pregnant now?
Now I have some questions about the future. Would you like to have (a/another) child, or would you prefer not to have any (more) children?
If want a/another child – how long would you like to wait from now before the birth of (a/another) child?
Knowledge of contraception:
There are various ways or methods that a couple can use to delay or avoid a pregnancy. Which of these ways or methods have you heard about?
Use of family planning:
Some couples use various ways or methods to delay or avoid a pregnancy. Are you currently doing something or using any method to delay or avoid getting pregnant?
If yes, which method are you using?
Impressions of family planning and self-efficacy
There are different kinds of family planning. When we say family planning we want you to think of modern methods of family planning, such as the pill, injectables, implants, condoms, spermicide, IUD and male or female sterilization.
How do you feel about family planning?
What would be the advantages or good things that would happen if you used family planning?
What would be the disadvantages or bad things that would happen if you used family planning?
What kind of person do you think typically uses family planning? [Probe as necessary: Imagine someone who uses family planning. How would you describe that person? What are they like?]
What kind of person do you think would never use family planning? [Probe as necessary: Imagine someone who never uses family planning. How would you describe that person? What are they like?]
What makes it difficult or impossible for you to use family planning? [Depending on barriers mentioned, probe – how confident do you feel in overcoming [different barriers]].
What makes it easier for you to use family planning?
If you want to use family planning, how confident are you that you can? [Why?]
Who do you think would object or disapprove if you used family planning?
Who do you think would approve or support you if you used family planning?
Do you have any other thoughts about family planning you would like to share?
Thank you! Would you like to receive a summary of results from this study?
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.