Back to Journals » Patient Preference and Adherence » Volume 14
“Mastering a New Life Situation” – Patients’ Preferences of Treatment Outcomes in Early Rheumatoid Arthritis – A Longitudinal Qualitative Study
Authors Landgren E ![]() , Bremander A
, Bremander A ![]() , Lindqvist E
, Lindqvist E ![]() , Nylander M, Van der Elst K
, Nylander M, Van der Elst K ![]() , Larsson I
, Larsson I ![]()
Received 11 March 2020
Accepted for publication 3 June 2020
Published 13 August 2020 Volume 2020:14 Pages 1421—1433
DOI https://doi.org/10.2147/PPA.S253507
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ellen Landgren,1– 3 Ann Bremander,1,3– 5 Elisabet Lindqvist,1,2 Maria Nylander,3,6 Kristien Van der Elst,7 Ingrid Larsson1,3,8
1Department of Clinical Sciences, Section of Rheumatology, Lund University, Lund, Sweden; 2Department of Rheumatology, Skåne University Hospital, Lund, Sweden; 3Spenshult Research and Development Centre, Halmstad, Sweden; 4Department of Regional Health Research, University of Southern Denmark, Odense, Denmark; 5Danish Hospital for Rheumatic Diseases, University Hospital of Southern Denmark, Sonderborg, Denmark; 6Swedish Rheumatism Association, Stockholm, Sweden; 7Department of Rheumatology, University Hospitals Leuven, Leuven, Belgium; 8School of Health and Welfare, Halmstad University, Halmstad, Sweden
Correspondence: Ingrid Larsson
School of Health and Welfare, Halmstad University, PO Box 823, Halmstad S-30118, Sweden
Tel +46 35 167965
Email [email protected]
Purpose: To explore patients’ preferred treatment outcomes during their first two years with rheumatoid arthritis (RA).
Patients and Methods: A qualitative, longitudinal, multicenter study with interviews at two time points was performed in Sweden. Individual interviews were conducted at time point 1 with 31 patients with RA, defined as disease duration of ≤ 1 year and treatment for 3– 7 months. Seven focus group interviews and five individual interviews were conducted at time point 2 with 22 patients 12– 20 months after treatment initiation. The interviews were analyzed using the Qualitative Analysis Guide of Leuven. A core category with four related concepts emerged.
Results: The core finding of patient-preferred treatment outcomes was “mastering a new life situation”. Patients preferred to experience control of the disease by controlling the symptoms and by experiencing absence of disease. To experience autonomy by regaining former activity level, experiencing independence, and being empowered was another preferred outcome. Patients preferred to regain identity through being able to participate, experience well-being, and regain former self-image. To experience joy in everyday life through vitality and believing in the future was another preferred outcome. Patients’ preferences developed over time from the acute phase of controlling the symptoms and wanting to return to the life they lived prior to diagnosis, to a more preventive way of self-management and empowerment to master the new life situation.
Conclusion: The patients’ preferred treatment outcomes during the first two years with RA were to master their new life situation and changed from a preference to return to a life lived prior disease onset, to a preference of living with quality of life, despite RA. This study increases the understanding of patients’ preferred treatment outcomes in the early disease course and can be a foundation for tailoring interventions to be more person-centered and to improve long-term treatment outcomes.
Keywords: focus groups, interviews, multicenter, patient perspective, rheumatic diseases
Introduction
Rheumatoid arthritis (RA) is a chronic, systemic, inflammatory joint disease and is the most common inflammatory rheumatic disease. The prevalence of RA is 0.5–1%1 and the female to male ratio is three to one. The prevalence increases with age and is highest in women older than 65 years, but people of all ages can be affected.2 Morning stiffness, symmetric arthritis, fatigue, and general illness are common symptoms of RA affecting functioning and quality of life. The etiology is unknown, but both genetic and environmental causes affect the risk of getting RA,2 and having a first degree relative with RA is the strongest known risk factor for developing the disease.3 Treatment consists of conventional or biological disease-modifying antirheumatic drugs (DMARDs) with the primary goal of suppressing disease activity and achieving remission or low disease activity.4 Other important goals of the treatment are to improve health-related quality of life through suppressed inflammation, control of the symptoms, prevention of disabilities, normalization of function, and the possibility for participating in work and leisure.4 Early treatment is important to achieve disease control and 40–50% of the patients who receive treatment within six months from disease onset will reach low disease activity or remission.5,6 Living with RA can affect the emotional and social aspects of life and patients can experience a struggle to cope with and master the illness.7–9
Patients experience unmet needs such as pain and fatigue, despite effective pharmacological treatment.10–13 The integration of patients’ preferences has been advocated into the assessment of treatment in order to be able to satisfy these “unmet needs” and to improve the quality of care for patients with RA.14,15 Smolen et al4 recommend that shared decision-making between healthcare professionals and the patient should be incorporated4 and integrating patients’ preferences into daily practice can lead to better health outcomes in terms of adherence and satisfaction.16 Moreover, shared decision-making contributes to a more equal relationship between the patient and healthcare professionals that can strengthen safety, participation, and independence for the patients.17 The importance of taking patients’ values and preferences into account in shared decision-making about care and treatment outcomes are highlighted in both the international treatment guidelines for RA and the European recommendations for the role of the nurse in the management of chronic inflammatory arthritis and should be used by all healthcare professionals in the treatment of RA.18–20
Research shows that patients with an established RA prefer the treatment to reduce symptoms, increase independence and well-being, and provide an increased quality of life.12,21–25 Patients’ preferences might not be the same, early in the disease course of a chronic disease as in established disease. However, research about patient preferences in the first years of RA is scarce.26 It is thus important to explore patients’ preferences of treatment outcomes when a person has recently been diagnosed with a chronic disease such as RA to be able to implement shared decision making. The objective of this study was thus to explore patients’ preferred treatment outcomes during the first two years with RA.
Patients and Methods
Design
This qualitative study has an explorative, longitudinal, and multicenter design with an inductive approach,27,28 and was conducted in collaboration with a patient research partner.29 The present study was part of the European Qualitative research project on Patient-preferred outcomes in Early Rheumatoid Arthritis (EQPERA)30 and presents the Swedish findings. Patients’ preferences and experiences may change in a rapidly evolving chronic disease why a longitudinal qualitative design was chosen.30
Participants
Patients from two rheumatology clinics in the southern part of Sweden were purposively invited to participate in the study. The clinics were situated in four different cities, representing both university hospitals and regional rheumatology specialist outpatient clinics, and offered the same standardized care. The inclusion criteria were: a diagnosis of RA according to the American College of Rheumatology/European League Against Rheumatism 2010 criteria,31 disease duration of ≤ 1 year, DMARDs treatment for 3–7 months, ≥18 years of age and to be able to speak, read and write the Swedish language.30 Thirty-one patients participated in individual interviews at the first time point (T1), and 22 of these were willing to participate in a focus group or individual interviews at the second time point (T2). The sociodemographic data of the participants are presented in Table 1. Patients in the present study were treated according to standard clinical practice with early treatment, which followed the National Pharmacological Guidelines32 and met the multidisciplinary team after six weeks on DMARD treatment. Five patients at T1 and three patients at T2 participated in the Nordstar study, a Nordic randomized study of early treatment comparing methotrexate and prednisolone to combinations of methotrexate and a biologic DMARD.33 Patients were invited to participate in the present study by their rheumatologist or by a nurse at their rheumatology clinic. Further information about the study was then given by the first or the last author (EL or IL).
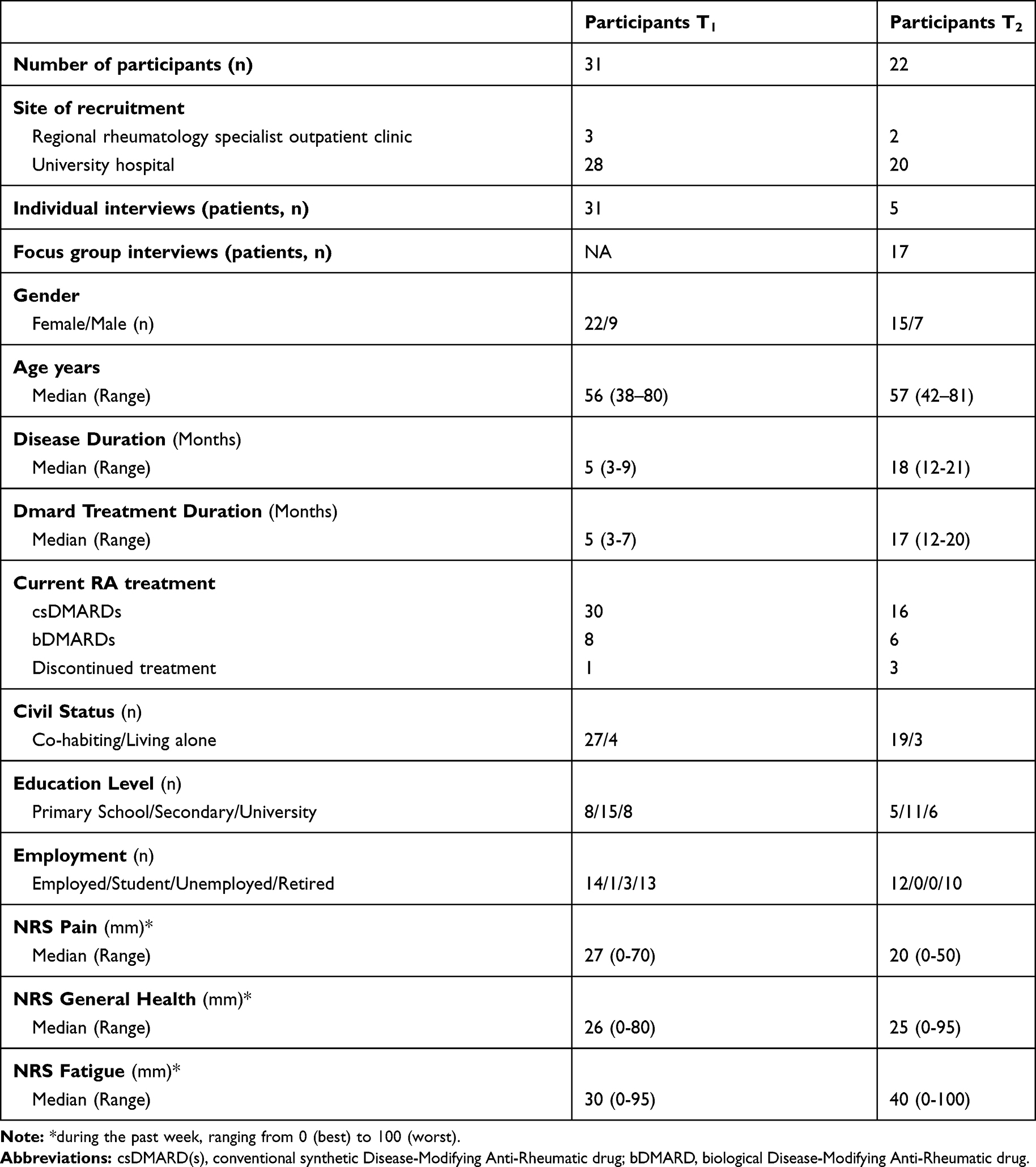 |
Table 1 Participant Demographic, Clinical, and Self-Reported Health Characteristics Grouped by Interview Time Point |
Data Collection
The data collection took place during 2017–2018. The interview guides, based on the EQPERA study protocol,30 included predefined topics with open-ended questions. All the questions related to the aim of the study; patients’ preferences of treatment outcomes. Questions such as “Can you describe how your RA affects your life?”,”Which outcomes of your RA and antirheumatic treatment are important for you at this moment?”, “Which expectations did you have about your antirheumatic treatment at the start of treatment?” and “To what extent do the expectations you had at the start of your treatment match your current expectations?”. The reason for selecting individual interviews at T1 was to create a safe environment for the participants to share their opinions and experiences in the new situation of living with a chronic disease. Focus groups were considered preferable at T2 for helping the patients’ exchange perspectives and experiences. Individual interviews were optional at T2 if it was preferred by the patient.30 All the interviews were digitally recorded and transcribed verbatim.
T1 took place 3–7 months after DMARD treatment initiation30 during 2017–2018. The time point was chosen to collect the patients’ earliest views after getting the diagnosis. The individual interviews were conducted by the first or the last author (EL or IL). Face-to-face, semi-structured interviews were conducted at the rheumatology clinic or in the patients’ homes. The individual interviews at T1 lasted between 16 and 127 minutes with a median of 43 minutes.
T2 took place 12–20 months after DMARD treatment initiation,30 during 2018 when pharmacological treatment was supposed to be settled. Seventeen patients participated in seven focus groups with two-three participants in each group. Five patients were interviewed individually at T2. The focus group interviews were conducted by the first author (EL), with the last author (IL) observing group interactions and taking notes. Focus group interviews took place at the rheumatology clinics and lasted between 54 and 110 minutes with a median of 78 minutes. The individual interviews at T2 were performed by the first author (EL), at the rheumatology clinic or on the phone depending on the patients’ wishes. The individual interviews at T2 lasted between 20 and 58 minutes with a median of 35 minutes.
Data Analysis
Interviews at both time points were analyzed using a constant comparison method according to the Qualitative Analysis Guide of Leuven (QUAGOL).34 QUAGOL is a 10-step analysis guide where transcripts were read repeatedly to grasp their essential information. There is a process of constant comparison between the authors’ interpretation and the patient’s story. The first five steps are a preparation of the coding process and the last five steps are where the coding starts. Fragments were coded and grouped into potential concepts and the final coding process took place in the qualitative software, NVivo 12 plus (QSR International, London, UK). The analysis was made individually by the first author (EL) in close collaboration with the last author (IL) and frequently discussed within the interdisciplinary research group involving a patient research partner (MN) during the process. As recommended in QUAGOL, the interdisciplinary teamwork optimized the process of conceptualization and provided a nuanced understanding of the data, and a consensus from the coding process was finally reached. Saldaña´s guiding questions for analyzing longitudinal data were adopted for the longitudinal analysis. The 16 guiding questions help the researcher to stay focused on changes over time, descriptive questions to describe the changes and analytic questions to guide the researcher to richer levels of interpretations and analysis.28,35
Results
The patient-preferred treatment outcomes in the first two years of RA were to mastering a new life situation, which entailed the patients wanting to be able to cope with the disease and not wanting to be restricted by the disease in any way. The patients’ preferences developed from an acute need for help to reestablish and master their life situation at T1 to a more resilient way of mastering the new life situation by themselves at T2. The core category “Mastering a new life situation” included four concepts; experiencing control of the disease, experiencing autonomy, regaining identity, and experiencing joy in everyday life and ten sub-concepts (Table 2). The concepts described below are illustrated by quotes from T1 and T2.
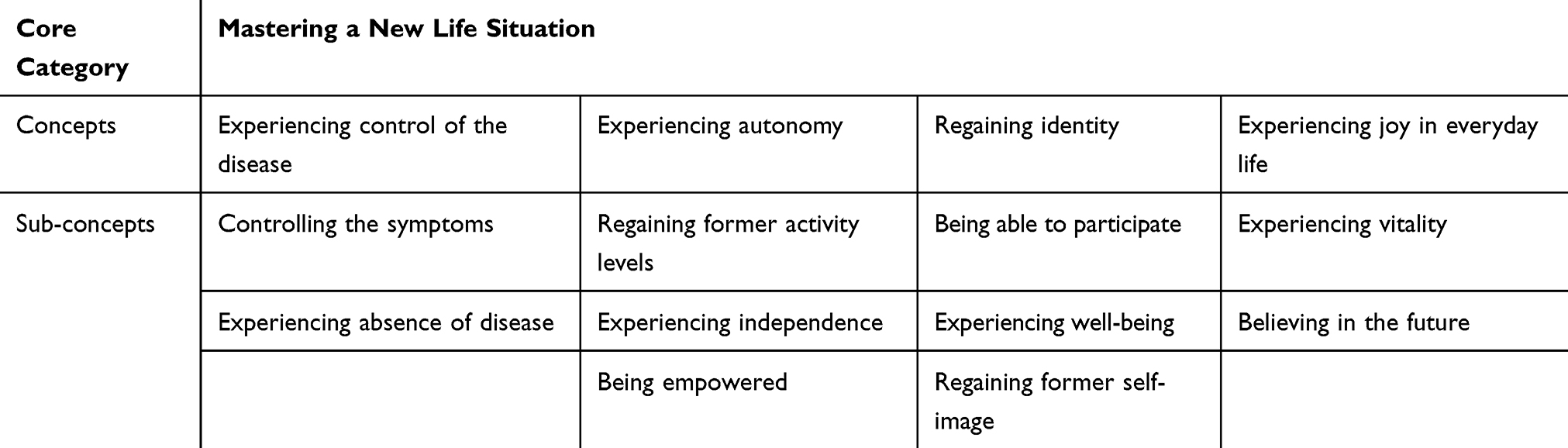 |
Table 2 Overview of Patient-Preferred Outcomes in Early Rheumatoid Arthritis |
To Experience Control of the Disease
A patient-preferred treatment outcome was to experience control of the disease, by controlling the symptoms and experiencing an absence of disease. Controlling physical symptoms were rather less emphasized over time as a preferred treatment outcome if the pharmacological treatment had been effective, and the symptoms were less bothering. Experiencing an absence of disease became more multifaceted over time because the patients also had experiences of different non-pharmacological treatment strategies to control the disease and to master the new life situation.
Controlling the Symptoms
Patients described that pain, swollen joints, and joint stiffness had a major impact on health and quality of life at T1, and they requested acute help to control the symptoms in order to take control of the disease. They were more nuanced about controlling the symptoms at T2. If the patients had experienced a flare with major physical disabilities, they still requested help to control the symptoms. However, the physical symptoms were generally not as highly prioritized as previously. The patients described a desire for stable low disease activity at T2 and had become reconciled with the diagnosis and tried to master the new life situation as long as the disease did not deteriorate.
“But then I hope that I notice it [RA] as little as possible, that it should not affect my everyday life” (Male, 42 years old, T1)
Fatigue was spoken of due to pain or age at T1, but the patients did not refer to fatigue as a symptom of the disease or as a side effect to pharmacological treatment. However, fatigue was perceived as overwhelming and a major symptom that was hard to control at T2. Fatigue became more distressing while other symptoms were suppressed by effective pharmacotherapy. Patients even described a preference for physical symptoms such as pain rather than experiencing fatigue, because they felt that physical symptoms were easier to cope with in experiencing control of the disease. Fatigue was limiting and difficult to master.
“It feels like I can sleep 26 hours in a day, I can sit and fall asleep at work, I am that tired. It’s something that I suffer from, very very much” (Female, 42 years old, T2)
Experiencing Absence of Disease
Absence of disease was expressed as not being reminded of the disease at T1. The patients expected an effective pharmacological treatment to be able to control the disease and to master the new life situation. They preferred less medication at both time points, and the first feelings of gratitude for the effective pharmacological treatment slightly changed to a growing fear of side-effects of the drugs at T2. They described an unsatisfactory bond to the drugs and wanted to gradually be free from medication. Furthermore, the pharmacological treatment increased the feeling of illness and the pills were associated with the dissatisfying feeling of being a patient.
Fewer side effects from pharmacological treatment was a major expectation of treatment outcome at T2. The treatment was expected to improve the health and quality of life and not cause more or new problems. Patients spoke of how they adapted their lives to comply with drug administration and side effects, which had been a greater concern at T2 compared to T1.
“Get started now so it won’t get any worse. Try to dampen it. Try to stop it in some way. Although it’s not possible to stop it, try to put it in the box” (Female, 56 years old, T1)
”Yes, it reminds me that I’m sick. If I take that pill, it’s because I have this [RA], that’s how it is” (Female, 73 years old, T2)
Effective non-pharmacological treatment was preferred at T2, including physiotherapy, occupational therapy, nursing care, and counselling. The patients had experienced positive health effects by using non-pharmacological treatments and highlighted these treatment modalities to control the disease and to experience the absence of disease. Furthermore, engaging in physiotherapy or occupational therapy contributed to the possibility of meeting other patients and learning from each other. The support and guidance from experienced healthcare professionals were expressed as an important part of the treatment to control the disease and master the new life situation.
“Physical joy, you feel better overall. Because that’s how it is when we go and exercise, it helps a lot for the pain too. The pain is reduced a lot’ (Female, 56 years old, T2)
Experiencing Autonomy
Experiencing autonomy was a preferred treatment outcome in order to master a new life situation, and included regaining former activity levels, experiencing independence, and being empowered. The patients’ preference to regain former activity levels remained over time. The preferred outcome of experiencing independence decreased over time while the importance of being empowered increased.
Regaining Former Activity Levels
Patients preferred to regain former activity levels with no physical limitations from the disease. Patients performed activities in a different way at T1 as prior to the onset of RA due to restricted function. Retired patients described a more adaptive way of living, being able to rest when they experienced bad days while patients with a more fixed schedule were more troubled and experienced problems in keeping up with their regular tasks. The patients described an adaption to the fact that everything takes a longer time to perform. They were eager to be able to perform activities of daily living and to regain their physical activity, which led to feelings of autonomy.
”To me, it felt like I was a prisoner in my own body. (…) you are trapped in yourself so to say. That’s why you become, I was really sad” (Female, 57 years old, T2)
The fear of physical restrictions was no longer as present at T2, but not be limited in any way was still an important treatment outcome. They had gained knowledge and had a strong desire to adapt to a healthy lifestyle in order to experience autonomy. The patients had positive experiences of physical activity at T2 and were motivated to do physical exercise: they found an association between improved strength and less fatigue, and between exercise and decreased pain and depression. Exercise generally increased their quality of life.
”One consequence of my illness is that I have become healthier, health is more in focus, I think more and more about my, working out is the hardest part, but it’s what I do, which I feel best from” (Male, 58 years old, T2)
The patients’ preferences at both time points were to be able to work and to maintain their economic standard. Being on sick leave affected their financial situation, which in turn limited plans for the future and their everyday life and thus also their autonomy. This led to feelings of unease, not only for the patient but for the whole family, and had to be considered while mastering the new life situation.
Experiencing Independence
Experience independence was an important part of autonomy. Patients described at T1 a sense of desperation to experience the same level of independence as prior to the RA onset. They expressed an unwillingness to use mobility aids, or assistive tools, as well as to ask for help or assistance from others due to their limited abilities. The patients described a fear of living a life being dependent on others and not being able to fend for themselves. Everyday life was described at T2 as being easier and not as restricted as they had feared at T1 due to the experience that they could live without help from others. Experiencing independence was thus not prioritized as a treatment outcome to the same degree.
“Yeah, get by myself. Don’t have to rely on anyone. That’s my freedom” (Female, 68 years old, T1)
Being Empowered
A patient-preferred treatment outcome was being empowered and thus experiencing autonomy. There was a need for knowledge about the disease and treatment at T1, and living in uncertainty affected their possibility of mastering the new life situation. There was a need to accept the diagnosis and know how to cope with RA at T1, while at T2 the patients described that it was difficult to accept RA and that it was like a process of conciliation in how to be empowered in order to master the disease and cope with the symptoms through self-management. The need for knowledge and comfort was an even more preferred treatment outcome at T2. Patients requested increased confidence in their abilities to feel empowered, which they gained through knowledge that helped them to master the new life situation.
”But, if you know what it is, then you can handle it in a completely different way than when you do not know what it is. Because then, you get worried in a completely different way when you don’t know why you are in pain. I know that it is why, yes, but I can take my painkillers, so, I know it will be reduced, and you can handle that pain in a different way then” (Female, 41 years old, T1)
Regaining Identity
The patients’ preferred treatment outcome was to regain identity by being able to participate, experiencing well-being, and regaining former self-image. Patients preferred to participate in different life situations as they had done prior to the RA diagnosis. This was important at both time points in order to regain one’s identity. A focus on emotional well-being and self-image became more important to master the new life situation with RA over time.
Being Able to Participate
Being able to participate was an important treatment outcome since RA restricted the patients’ ability to interact socially and to manage different life roles. The patients avoided participating in social situations due to pain or fatigue and they avoided making plans because they feared having to cancel the plans at T1. The onset of RA affected their relationships with everyone they knew, which also affected their spouses’ social life. The patients described the limitation in social interactions at T2 as being of similar importance as at T1 and they preferred to regain their former identity.
“Life isn’t fun for the person you live with either. My husband felt very lonely himself and it was not fun for him either” (Female, 57 years old, T2)
Being able to participate also included workability, which was a treatment outcome that affected the possibility to master the new life situation. Patients described that they evaluated the effectiveness of the treatment at T1 through their workability, and if they could work, the disease was deemed to be under acceptable control. Some patients had changed jobs and some still experienced difficulties at work at T2.
“For my part, when you have so many years left to work, it’s stressful if you really can, I only have a basic school education and I started working already physically when I was young. Will I be able to cope?” (Female, 48 years old, T2)
Work was mentioned at both time points but sometimes work affected the ability to perform housework and to participate in leisure activities, since they were too tired after a working day to do something else. Participation in work was, however, important for their identity and great efforts were made to master the new life situation.
Experiencing Well-being
Experiencing emotional well-being and thus regaining one’s identity was an important treatment outcome in order to master the new life situation at both time points. Emotional well-being was influenced by concerns about the future and was described in terms of unintentional changes in life due to RA, feelings of misery and uncertainty about disabilities and future health, work, and everyday life. Patients experienced initial relief and gratitude for being helped and diagnosed at T1, and described a variety of positive feelings and depressed mood, anxiety, fear, and grief over having a diagnosis of a chronic disease. Patients were more anxious and frustrated at T2, which affected their ability to regain their identity. Some described a transition from hope to despair and they experienced a low point after a good phase. Their emotional well-being was influenced by increased depressed mood and frustration despite their physical symptoms being under better control. Uncertainty about the future created great concern and had a negative impact on emotional well-being as well as their identity.
“I’ve been really sad. I’ve felt like I’m not the same person” (Female, 38 years old, T1)
Regaining Former Self-Image
Patients preferred to regain their self-image as it was prior to the onset of RA in order to recapture their identity and master the new life situation. They preferred not to be seen or identified as a sick person. Patients experienced a change of self-image at T1 due to their inability to participate in a social context in comparison with how it was prior to the onset of RA. Family and friends had talked about that the patients’ behavior and mannerisms had changed, and the patients described restrictions in fulfilling life roles that impacted on their quality of life. They feared not being able to recapture their professional persona. Their profession was closely related to their identity, which was important to maintain. Patients described a disliked calmer lifestyle with a changed social life and/or work and changed identity at T2.
“I tried to work, study, be a mother, be a wife, but I couldn’t do anything” (Female, 44 years old, T2)
The patients experienced a changed self-image and self-esteem when RA affected physical appearance. Patients were frustrated by hair loss, development of weak nails, and weight gain/loss due to side-effects of the pharmacological treatment or because they were not able to continue an active lifestyle at T1. The physical appearance was important for the patients but at the same time, they experienced a lack of empathy and understanding from people around them when the disease lacked visible attributes. Not being reminded of the disease and physical side effects were major issues affecting the identity. Self-image was still an important outcome at T2, and patients expressed a desire not to look sicker than they were, and that RA should not be visible. Some patients preferred to have pain than having hair loss and had thus discontinued the treatment.
“Above all, it’s that I shouldn’t lose my hair. Oh God, what I’m nagging about my hair. It’s just that it’s the top priority for me right now. (…) When I feel that I almost have bald patches. You get that when you are a cancer patient, I just have pain in my joints. I shouldn’t need to get bald (…) My God it’s just hair, but at the same time I don’t feel so sick that I need to lose all my hair. Then I will feel even sicker than I really am” (Female, 42 years old, T2)
Experiencing Joy in Everyday Life
Experiencing joy in everyday life was a preferred treatment outcome and included experiencing vitality and believing in the future. Experiencing joy in everyday life became more important over time for patients in order to master the new life situation. Patients were most satisfied with the treatment outcomes and expressed feelings of hope and belief in the future at T1, while at T2 their preferred treatment outcome was expressed as an increased desire to experience vitality through enthusiasm, energy, good sleep, and good spirits.
Experiencing Vitality
Symptoms of the disease such as pain and fatigue together with experiencing physical disabilities affected temper, patience, enthusiasm, and the possibility to enjoy everyday life at both time points. It also drained their energy and affected sleep. The patients described a need to rest during the day, which led to poor sleep during the night and difficulties in mastering the new life situation.
“You lose your desire. Simply, when you’re sick. You lose your lust for life and you lose the desire to … hang out and to … yes. Life loses its meaning simply” (Female, 56 years old, T1)
The effective treatment reduced pain and vitality and joy in everyday life was regained at T2, which together contributed to an increased ability to master the new life situation with RA. A positive attitude, good spirits, and joy in everyday life was an important treatment outcome at T2. Concerns about a restful sleep were more evident at T2 and patients described disturbed sleep as; sleeping too much, sleeping too little, waking up due to pain or falling asleep all the time, resulting in loss of vitality.
” I’m much more tired and I feel powerless sometimes, and sometimes, in the middle of the day, I’m like a car running out of gas, it becomes a total stop” (Female, 74 years old, T2)
” Why am I so tired? If there were any pills against it.” (Female, 45 years old, T2)
Believing in the Future
The patients sought to be hopeful, experience longevity, and to have a meaningful life, which was of importance in order to experience joy in everyday life. Hopefulness was described as having a positive way of thinking, and longevity was expressed as a fear of a shorter life and a desire to live a long life despite RA at T1. The patients felt more depressed at T2 and expressed a need for comfort and support from the healthcare professionals to believe in the future in order to master the new life situation. The importance of experiencing joy in everyday life was expressed at T2. The disease had aroused reflections about life and the importance of enjoying and utilizing life to master the new life situation.
”One consequence is that if it’s positive or negative I don’t know, but you get a reminder that you cannot live, that you are not healthy forever. So maybe you are taking more advantage of life, at least I’ve started to think like that. “(Female, 46 years old, T2)
Discussion
The core findings from the study are that patients’ preferred treatment outcome during the first two years with RA is to master the new life situation. Regardless of the time, patients with early RA had to master the new life situation after diagnosis and treatment initiation. The patients developed a more accepting and resilient state of mind with a focus on mastering the new life situation in the long-term perspective. The preferred treatment outcome changed from mastering the life situation with help from healthcare professionals to a desire for empowerment and self-management to master the life situation more independently. Recurring preferences were being able to experience a sense of freedom and being able to live without physical, mental, and social limitations. The patients were eager to return to the life they lived prior to the disease at the disease onset and treatment initiation. These results from patients with early RA are in line with previous studies among patients with established RA where preferred treatment outcomes were to minimize the personal impact of RA, regain health, and to live a normal life.21,23,24 Research into preferred treatment outcomes among patients with early RA is limited but results from the Belgian study in the EQPERA project revealed that patients with early RA strive to return to a normal life,26 which is similar to our results. Results from this study can help healthcare professionals to better understand the dynamic process of patients’ preferred treatment outcomes early in the disease process to prevent the development of unmet needs, increase patient satisfaction, and improve quality of care through tailored interventions to improve long-term treatment outcomes.
Fatigue was a symptom that was difficult to cope with for patients in the present study, and it became even more distressing over time when other symptoms were assuaged due to effective treatment. It is known from earlier studies that fatigue is a common symptom, which is difficult to control in patients with RA despite ongoing treatment.36–38 Fatigue affects psychosocial, physical, emotional aspects, and has a negative impact on health-related quality of life.11,21,24,39,40 Results from the longitudinal study of Belgian patients in the EQPERA project showed less fatigue over time, which is in contrast to our findings26 and perhaps implies a cultural difference.
Preferences for non-pharmacological treatment to control the disease emerged in the longitudinal perspective. Patients valued the early support from physiotherapists, occupational therapists, social workers, and nurses, and this positive experience was reinforced over time. This might have been influenced by the fact that they met the multidisciplinary team as part of the standard care at the clinic. Patients used treatment strategies from different healthcare professionals to be able to feel independent and empowered and gained positive health effects from those treatment modalities. Previous studies with patients with established RA have reported the importance of patient preferred continuity, easy access, and inter-personal relationships with healthcare professionals with good knowledge of RA.17,41 Patients with early RA in the present study also described an added value of interacting with other patients at the clinic during non-pharmacological treatment sessions. Emotional support through meetings with other patients is an important and positive effect of rehabilitation42,43 which should be taken into consideration in the development of care for patients with chronic diseases such as RA.
Patients tried to adopt a healthier lifestyle after being diagnosed with RA, for example, they tried to improve their level of physical activity to experience autonomy. Earlier studies have demonstrated that physical activity in patients with established RA may be understood as a resource for increased health and quality of life.44,45 A study of patients with early RA also concluded that awareness is a motivation to change patterns of physical ability in a positive way.46 Patients experienced a fear of being dependent early in the disease course, which reduced over time due to experiences of independence despite RA. The focus on self-management and empowerment to master the disease increased over time. Independence and self-management were crucial for patients, which is supported by findings from earlier studies that indicate the importance of being able to self-manage one’s household, social interactions, and to regain control and incorporate RA in life.21,47 Being independent and feeling empowered may improve adherence and support shared decision-making.48
Mastering life with RA entails both mental and physical processes. Physical limitations may lead to new procedures, which can lead to a re-thinking of one’s identity. A previous study showed that patients with established RA also needed to accept changes in life and adjust to a new level of normality by incorporating RA into one’s identity,47 which underlines the present study’s result that patients need to adjust daily tasks in order to be able to master the new life situation. Patients also prefer to maintain their social interactions and to manage life roles when mastering the new life situation. Previous research shows that participation is to be experiencing a feeling of belonging, a feeling of inclusion, and of maintaining the patient’s self-image.49 In the present study, patients with early RA valued their professional persona, which underlines previous research showing that patients favor work and avoid social interactions if they have to choose.50 It is a challenge to balance personal life and work life and the struggle can impair the patients’ normal life-roles.51 To experience autonomy was also expressed in terms of the preference of maintaining an economic standard that remained over time. Being on sick leave affected the patients negatively both economically and in regard to their plans for the future. RA is associated with an economic burden for both the patients and society.38 Financial concerns in relation to patients with rheumatoid arthritis have previously been reported in a negative way.52 The patients in the present study expressed restrictions on physical and social participation that also affected their loved ones. The patients’ partners are vital for the patients’ disease management, but many have a psychosocial burden. Significant others also have to make adjustments, and the patient may feel that she/he has failed others and may be apprehensive about future activities.8,53
Maintaining one’s physical appearance was a preference that increased over time. It was crucial that the disease should not affect the patients’ identity, and they resisted having a patient identity. Some patients even paused their treatment due to side-effects that affected their looks and character. Previous research has demonstrated a correlation between depression and the patient’s concerns about her/his appearance when living with RA, which is something that should be routinely assessed.54 Another study with patients with established RA addresses the difficulties of living with a deteriorating self-image and problems finding clothes and shoes due to deformities,55 which differs from concerns among the patients in the present study about physical appearance early in the disease. The treatment of early RA has been more aggressive during the last decade with better long-term treatment outcomes thus generating differing patient preferences from those previously held, which highlights the significance of the study’s result. Patients in the present study expressed concerns about the future, emphasizing the need for support from healthcare professionals. Patients expressed a preference for experiencing energy and enthusiasm in everyday life and for having a meaningful life, summarized in the preference to experience joy in everyday life. Previous research underlines the uncertain life with RA that may unsettle the patients’ vision and plans for the future. It is important that healthcare professionals identify and consider the patients’ experiences of living with chronic conditions such as RA. Interventions that focus on the patients’ experiences of RA might help to facilitate the latter’s capacity to reevaluate the situation and live well with RA.51 Treatment goals may differ when healthcare professionals focus on inflammatory disease activity while the patient prefers other health-related personal treatment goals.38 A previous study demonstrated a challenge in the care of patients with early RA regarding the disagreement in physician-perceived and patient-perceived remission.56 Healthcare professionals also need to focus on the patient’s preferred treatment outcomes already from the start of the treatment, to improve shared decision-making, and improve patient care.57 We found that patients’ perspective might change during the first year of living with the disease, emphasizing the importance of shared decision-making in all stages of the disease. Implementing shared decision-making, a cornerstone in person-centered care is challenging and requires a commitment across the health care system.58 Most patients want to be more involved in decisions about their care, however, not all patients have the knowledge and the power to participate in shared decision-making. This imbalance between the patient and healthcare professionals needs to be acknowledged and dealt with early in the disease course.59
Methodological Considerations
Trustworthiness is defined according to the four criteria of credibility, dependability, confirmability, and transferability.60 Several strategies were used to verify the trustworthiness throughout the research process. Credibility was strengthened through the number of participants being interviewed at different clinics and when data saturation was reached. Dependability was strengthened by the fact that the research process is well described and all steps in the data analysis have been carefully reported.Quotes from the interviews were used to verify the findings. All the interviews began with the same question to ensure stability and had follow-up questions to avoid misunderstanding. A limitation could be the different durations of the interviews, 16–127 minutes at T1 is a wide variation. However, the interviews generated rich data both in terms of variation and depth. The interdisciplinary team discussions including a patient partner culminated in a broad view of the data with a consensus of the result, thus strengthening the dependability. To strengthen confirmability, both interviewers were rheumatology nurses and familiar with the subject area but attempted to remain open to all variations in experiences that emerged and were relevant to the aim and were not caregivers to the patients in the present study. It could be seen as both a strength and a limitation to have a pre-understanding. During the research process, the authors’ pre-understanding was discussed and critically reflected on in order to broaden our awareness of the risk of biased interpretation. In terms of transferability, the sample size can be regarded as sufficient for ensuring variations in the experiences of the same topic. Even if most of the patients were from a University hospital clinic the usual care and treatment strategy follows national and international guidelines. The findings can be transferable for other contexts with the same patient group and may also be of value to patients with other chronic diseases early in their disease course.
Conclusion
The patient-preferred treatment outcome after being diagnosed with RA was mastering a new life situation. Experiencing disease control and autonomy as well as regaining identity and joy in everyday life, were of importance when adapting to life with a chronic disease. In the early course of RA, patients’ preferences changed from one of a return to the life lived prior to the disease to one of living with a quality of life despite RA. These are meaningful findings and results from this study can help healthcare professionals to better understand the dynamic process of patients’ preferred treatment outcomes early in the disease process to prevent the development of unmet needs, increase patient satisfaction, and improve quality of care through tailored interventions to improve long-term treatment outcomes. These findings adhere well to the person-centered process within the person-centered framework.
Data Sharing Statement
The data supporting the results reported in the manuscript will not be shared as ethical approval for the study requires that the transcribed interviews are kept in locked files, accessible only to the researchers.
Ethical Considerations
The study was carried out in accordance with the ethical principles of the Declaration of Helsinki61 and approved by the Regional Ethical Review Board in Lund, Sweden (2016/618, 2017/205). Written informed consent was obtained from all participants. Oral and written information about the study, voluntary participation, and the possibility of withdrawing at any time without given a reason or affecting their healthcare and treatment was provided by the first or last author (EL, IL).
Acknowledgments
The authors would like to thank all participants in this study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet. 2016;388(10055):2023–2038. doi:10.1016/S0140-6736(16)30173-8
2. Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet. 2010;376(9746):1094–1108. doi:10.1016/S0140-6736(10)60826-4
3. Kuo C-F, Grainge MJ, Valdes AM, et al. Familial aggregation of rheumatoid arthritis and co-aggregation of autoimmune diseases in affected families: a nationwide population-based study. Rheumatology. 2017;562017:928–933.
4. Smolen JS, Breedveld FC, Burmester GR, et al. Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Ann Rheum Dis. 2016;75(1):3–15. doi:10.1136/annrheumdis-2015-207524
5. Einarsson JT, Willim M, Ernestam S, Saxne T, Geborek P, Kapetanovic MC. Prevalence of sustained remission in rheumatoid arthritis: impact of criteria sets and disease duration, a Nationwide Study in Sweden. Rheumatology. 2019;58(2):227–236. doi:10.1093/rheumatology/key054
6. Aletaha D, Smolen JS. Diagnosis and management of rheumatoid arthritis: a review. JAMA. 2018;320(13):1360–1372. doi:10.1001/jama.2018.13103
7. Bala SV, Samuelson K, Hagell P, et al. Living with persistent rheumatoid arthritis: a BARFOT study. J Clin Nurs. 2017;26(17–18):2646–2656. doi:10.1111/jocn.13691
8. Bergstrom M, Sverker A, Larsson Ranada A, et al. Significant others’ influence on participation in everyday life - the perspectives of persons with early diagnosed rheumatoid arthritis. Disabil Rehabil. 2018;42:1–9.
9. Ostlund G, Bjork M, Thyberg I, et al. Emotions related to participation restrictions as experienced by patients with early rheumatoid arthritis: a qualitative interview study (the Swedish TIRA project). Clin Rheumatol. 2014;33(10):1403–1413. doi:10.1007/s10067-014-2667-2
10. Feldthusen C, Jacobsson L, Mannerkorpi K, Grimby-Ekman A, Forsblad-D’Elia H. Explanatory factors and predictors of fatigue in persons with rheumatoid arthritis: A longitudinal study. J Rehabil Med. 2016;48(5):469–476. doi:10.2340/16501977-2090
11. Repping-Wuts H, Uitterhoeve R, van Riel P, van Achterberg T. Fatigue as experienced by patients with rheumatoid arthritis (RA): A qualitative study. Int J Nurs Stud. 2008;45(7):995–1002. doi:10.1016/j.ijnurstu.2007.06.007
12. van Tuyl LH, Sadlonova M, Hewlett S, et al. The patient perspective on absence of disease activity in rheumatoid arthritis: a survey to identify key domains of patient-perceived remission. Ann Rheum Dis. 2017;76(5):855–861. doi:10.1136/annrheumdis-2016-209835
13. Alexandros AD, Eleftherios P, Paraskevi VV. Rheumatoid arthritis treatment. a back to the drawing board project or high expectations for low unmet needs? J Clin Med. 2019;8(8):1237. doi:10.3390/jcm8081237
14. Sverker A, Ostlund G, Thyberg M, Thyberg I, Valtersson E, Bjork M. Dilemmas of participation in everyday life in early rheumatoid arthritis: a qualitative interview study (The Swedish TIRA Project). Disabil Rehabil. 2015;37(14):1251–1259. doi:10.3109/09638288.2014.961658
15. Hsiao B, Fraenkel L. Incorporating the patient’s perspective in outcomes research. Curr Opin Rheumatol. 2017;29(2):144–149. doi:10.1097/BOR.0000000000000372
16. Street RL
17. Larsson I, Bergman S, Fridlund B, Arvidsson B. Patients’ experiences of a nurse-led rheumatology clinic in Sweden: A qualitative study. Nurs Health Sci. 2012;14(4):501–507. doi:10.1111/j.1442-2018.2012.00723.x
18. Bech B, Primdahl J, van Tubergen A, et al. 2018 update of the EULAR recommendations for the role of the nurse in the management of chronic inflammatory arthritis. Ann Rheum Dis. 2019;79:61.
19. Singh JA, Saag KG, Bridges SL
20. Smolen JS, Landewe R, Bijlsma J, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann Rheum Dis. 2017;76(6):960–977. doi:10.1136/annrheumdis-2016-210715
21. Ahlmen M, Nordenskiold U, Archenholtz B, et al. Rheumatology outcomes: the patient’s perspective. A multicentre focus group interview study of Swedish rheumatoid arthritis patients. Rheumatology. 2005;44(1):105–110. doi:10.1093/rheumatology/keh412
22. Sanderson T, Hewlett S, Richards P, Morris M, Calnan M. Utilizing qualitative data from nominal groups: exploring the influences on treatment outcome prioritization with rheumatoid arthritis patients. J Health Psychol. 2012;17(1):132–142. doi:10.1177/1359105311410758
23. Sanderson T, Morris M, Calnan M, Richards P, Hewlett S. What outcomes from pharmacologic treatments are important to people with rheumatoid arthritis? Creating the basis of a patient core set. Arthritis Care Res (Hoboken). 2010;62(5):640–646. doi:10.1002/acr.20034
24. Carr A, Hewlett S, Hughes R, et al. Rheumatology outcomes: the patient’s perspective. J Rheumatol. 2003;30(4):880–883.
25. van Tuyl LH, Hewlett S, Sadlonova M, et al. The patient perspective on remission in rheumatoid arthritis: ‘You’ve got limits, but you’re back to being you again’. Ann Rheum Dis. 2015;74(6):1004–1010. doi:10.1136/annrheumdis-2013-204798
26. van der Elst K, Meyfroidt S, De Cock D, et al. Unraveling patient-preferred health and treatment outcomes in early rheumatoid arthritis: a longitudinal qualitative study. Arthritis Care Res (Hoboken). 2016;68(9):1278–1287. doi:10.1002/acr.22824
27. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. Philadelphia: Wolters Kluwer; 2016.
28. Saldaña J. Longitudinal Qualitative Research: Analyzing Change Through Time. Walnut Creek, Calif.: AltaMira Press; 2003.
29. de Wit MP, Berlo SE, Aanerud GJ, et al. European League Against Rheumatism recommendations for the inclusion of patient representatives in scientific projects. Ann Rheum Dis. 2011;70(5):722–726. doi:10.1136/ard.2010.135129
30. Van der Elst K, Bremander A, De Groef A, et al. European Qualitative research project on Patient-preferred outcomes in Early Rheumatoid Arthritis (EQPERA): rationale, design and methods of a multinational, multicentre, multilingual, longitudinal qualitative study. BMJ Open. 2019;9(3):e023606. doi:10.1136/bmjopen-2018-023606
31. Aletaha D, Neogi T, Silman AJ, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–2581. doi:10.1002/art.27584
32. Förening SR. Riktlinjer för läkemedelsbehandling vid reumatoid artrit [Guidelines for drug therapy in rheumatoid arthritis]. 2019.
33. Glinatsi D, Heiberg MS, Rudin A, et al. Head-to-head comparison of aggressive conventional therapy and three biological treatments and comparison of two de-escalation strategies in patients who respond to treatment: study protocol for a multicenter, randomized, open-label, blinded-assessor, Phase 4 study. Trials. 2017;18(1):161.
34. Dierckx de Casterle B, Gastmans C, Bryon E, Denier Y. QUAGOL: a guide for qualitative data analysis. Int J Nurs Stud. 2012;49(3):360–371. doi:10.1016/j.ijnurstu.2011.09.012
35. Saldaña J. Analyzing change in longitudinal qualitative data. Youth Theatre J. 2002;16(1):1–17. doi:10.1080/08929092.2002.10012536
36. Olsen CL, Lie E, Kvien TK, Zangi HA. Predictors of fatigue in rheumatoid arthritis patients in remission or in a low disease activity state. Arthritis Care Res (Hoboken). 2016;68(7):1043–1048. doi:10.1002/acr.22787
37. Primdahl J, Hegelund A, Lorenzen AG, Loeppenthin K, Dures E, Appel Esbensen B. The Experience of people with rheumatoid arthritis living with fatigue: a qualitative metasynthesis. BMJ Open. 2019;9(3):e024338. doi:10.1136/bmjopen-2018-024338
38. Taylor PC, Moore A, Vasilescu R, Alvir J, Tarallo M. A structured literature review of the burden of illness and unmet needs in patients with rheumatoid arthritis: a current perspective. Rheumatol Int. 2016;36(5):685–695. doi:10.1007/s00296-015-3415-x
39. Hewlett S, Cockshott Z, Byron M, et al. Patients’ perceptions of fatigue in rheumatoid arthritis: overwhelming, uncontrollable, ignored. Arthritis Rheum. 2005;53(5):697–702. doi:10.1002/art.21450
40. Nikolaus S, Bode C, Taal E, van de Laar MA. Fatigue and factors related to fatigue in rheumatoid arthritis: a systematic review. Arthritis Care Res (Hoboken). 2013;65(7):1128–1146. doi:10.1002/acr.21949
41. Primdahl J, Wagner L, Horslev-Petersen K. Being an outpatient with rheumatoid arthritis–a focus group study on patients’ self-efficacy and experiences from participation in a short course and one of three different outpatient settings. Scand J Caring Sci. 2011;25(2):394–403. doi:10.1111/j.1471-6712.2010.00854.x
42. Vaks K, Sjostrom R. Rheumatoid arthritis patients’ experience of climate care. J Exercise Rehabil. 2015;11(6):337–344. doi:10.12965/jer.150228
43. Zuidema RM, Repping-Wuts H, Evers AWM, Van Gaal BGI, Van Achterberg T. What do we know about rheumatoid arthritis patients’ support needs for self-management? A scoping review. Int J Nurs Stud. 2015;52(10):1617–1624. doi:10.1016/j.ijnurstu.2015.05.008
44. Loeppenthin K, Esbensen B, Ostergaard M, Jennum P, Thomsen T, Midtgaard J. Physical activity maintenance in patients with rheumatoid arthritis: a qualitative study. Clin Rehabil. 2014;28(3):289–299. doi:10.1177/0269215513501526
45. Malm K, Bremander A, Arvidsson B, Andersson ML, Bergman S, Larsson I. The influence of lifestyle habits on quality of life in patients with established rheumatoid arthritis-A constant balancing between ideality and reality. Int J Qual Stud Health Well-Being. 2016;11(1):30534. doi:10.3402/qhw.v11.30534
46. Qvarfordt M, Andersson MLE, Larsson I. Factors influencing physical activity in patients with early rheumatoid arthritis: A mixed-methods study. SAGE Open Medicine. 2019;7. doi:10.1177/2050312119874995
47. Flurey CA, Morris M, Richards P, Hughes R, Hewlett S. It’s like a juggling act: rheumatoid arthritis patient perspectives on daily life and flare while on current treatment regimes. Rheumatology. 2014;53(4):696–703. doi:10.1093/rheumatology/ket416
48. Oshotse C, Zullig LL, Bosworth HB, Tu P, Lin C. Self-efficacy and adherence behaviors in rheumatoid arthritis patients. Prev Chronic Dis. 2018;15:E127. doi:10.5888/pcd15.180218
49. Sverker A, Thyberg I, Valtersson E, Bjork M, Hjalmarsson S, Ostlund G. Time to update the ICF by including socioemotional qualities of participation? The development of a “patient ladder of participation” based on interview data of people with early rheumatoid arthritis (the Swedish TIRA study). Disabil Rehabil. 2019;42:1–8.
50. Sverker A, Thyberg I, Ostlund G, Waltersson E, Thyberg M. Participation in work in early rheumatoid arthritis: a qualitative interview study interpreted in terms of the ICF. Disabil Rehabil. 2014;36(3):242–249. doi:10.3109/09638288.2013.789086
51. Toye F, Seers K, Barker KL. Living life precariously with rheumatoid arthritis - a mega-ethnography of nine qualitative evidence syntheses. BMC Rheumatol. 2019;3(1):5. doi:10.1186/s41927-018-0049-0
52. Kumar K, Reehal J, Stack RJ, Adebajo A, Adams J. Experiences of South Asian patients in early inflammatory arthritis clinic: a qualitative interview study. Rheumatol Adv Pract. 2019;3(2):rkz017. doi:10.1093/rap/rkz017
53. Matheson L, Harcourt D, Hewlett S. ‘Your whole life, your whole world, it changes’: partners’ experiences of living with rheumatoid arthritis. Musculoskeletal Care. 2010;8(1):46–54. doi:10.1002/msc.165
54. Monaghan SM, Sharpe L, Denton F, Levy J, Schrieber L, Sensky T. Relationship between appearance and psychological distress in rheumatic diseases. Arthritis Rheum. 2007;57(2):303–309. doi:10.1002/art.22553
55. Pedraz-Marcos A, Palmar-Santos AM, Hale CA, et al. Living with rheumatoid arthritis in spain: a qualitative study of patient experience and the role of health professionals. Clin Nurs Res. 2018;1054773818791096.
56. Turk SA, Rasch LA, van Schaardenburg D, et al. Pain, sleep and emotional well-being explain the lack of agreement between physician- and patient-perceived remission in early rheumatoid arthritis. BMC Rheumatol. 2018;2(1):16. doi:10.1186/s41927-018-0024-9
57. Fautrel B, Alten R, Kirkham B, et al. Call for action: how to improve use of patient-reported outcomes to guide clinical decision making in rheumatoid arthritis. Rheumatol Int. 2018;38(6):935–947. doi:10.1007/s00296-018-4005-5
58. McCormack B, McCance TV. Development of a framework for person-centred nursing. J Adv Nurs. 2006;56(5):472–479. doi:10.1111/j.1365-2648.2006.04042.x
59. Joseph-Williams N, Elwyn G, Edwards A. Knowledge is not power for patients: a systematic review and thematic synthesis of patient-reported barriers and facilitators to shared decision making. Patient Educ Couns. 2014;94(3):291–309. doi:10.1016/j.pec.2013.10.031
60. Lincoln YS, Guba EG. Naturalistic Inquiry. Beverly Hills, Calif.: Sage; 1985.
61. Association WM. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.