Back to Journals » Nursing: Research and Reviews » Volume 4
“Can nurse work environment influence readmission risk?” – a systematic review
Authors Ma C, Shang J, Stone P
Received 15 March 2014
Accepted for publication 13 May 2014
Published 21 July 2014 Volume 2014:4 Pages 91—101
DOI https://doi.org/10.2147/NRR.S46156
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Chenjuan Ma,1 Jingjing Shang,2 Patricia W Stone3
1The National Database of Nursing Quality Indicators, University of Kansas Medical Center, Kansas City, KS, 2Columbia University School of Nursing, 3Center for Health Policy, Columbia University School of Nursing, New York, NY, USA
Background: Readmissions have been targeted as events that can improve quality of care while reducing health care expenditures. While increasing evidence has linked nurse work environment to various patient outcomes, no systematic review has assessed evidence examining nurse work environment in relation to readmission.
Methods: This review was guided by the Institute of Medicine's Standards for Systematic Reviews. Comprehensive searches were conducted in PubMed, CINAHL, and PsycINFO, and were complemented by hand searching. Two reviewers independently completed full-text review and quality assessment using a validated tool.
Results: Ten studies met the inclusion criteria and were included for final review. Various methods were used to measure readmission and nurse work environment, and analyses were conducted at both the patient and hospital levels. Overall, associations between nurse work environment and readmission emerged, and better nurse work environments (particularly higher levels of nurse staffing) were associated with fewer readmissions.
Discussion: The interpretation of results from each study was limited by the differences in variable measures across studies and methodological flaws. The relationship between nurse work environment and readmission needs to be further confirmed by stronger evidence from studies using standardized measures and more rigorous research design.
Keywords: nurse work environment, nurse staffing, readmission, nursing, patient outcome
Introduction
Hospital readmissions are prevalent and costly, and therefore are a subject of growing scrutiny in many countries.1–3 With a global trend of reduction in length of hospital stay, readmission rates have been quite steady and have even increased for some medical conditions.3–5 For example, in Norway, a researcher reported an increase in 30-day readmission rate from 15% in 1999 to 17.4% in 2006;6 and in the US, approximately 20% of its Medicare patients were readmitted within 30 days of discharge in 2004, which was estimated at a cost of $17 billion.7 Landmark reports on patient safety including To Err is Human8 and Crossing the Quality Chasm9 by the Institute of Medicine, and specific regulations such as the American Hospital Readmission Reduction Program, which financially penalized 2,225 hospitals in 2012 a total of $250 million for excess readmission rates,10 have further highlighted the urgency in reducing preventable readmissions. Consequently, hospital executives are under unprecedented pressure to identify and implement effective interventions to reduce hospital readmissions.
In most developed countries, the nursing workforce constitutes the largest and most costly group of health care providers. For example, in the US, nursing accounts for as much as 44% of direct costs of inpatient care11 with over 1.5 million registered nurses (RNs) providing care to patients in hospitals.12 With round-the-clock bedside direct patient care nurses function as a surveillance system within their work environment for early detection of patient complications, adverse events, and other care needs.13 This surveillance is vital to prevent readmissions and can be influenced by the context of nurse work environments.
Nurse work environment, defined as “the organizational characteristics of a work setting that facilitate or constrain professional nursing practice”,14 is an important component of the hospital service delivery system and affects quality of nursing care. The nurse work environment is controllable by hospital administrators and can be an area for potential intervention to improve patient care and reduce hospital readmissions. Accordingly, the Institute of Medicine published a report Keeping Patients Safe: Transforming the Work Environment of Nurses,15 which highlighted the importance of nurse work environment in improving quality of care and patient outcomes and recommended health organizations to reform their nurse work environments.
There are several attributes of the nurse work environment such as staffing and resources adequacy, nursing foundation for quality of care, and administrative support of nurses. Previous studies related to nurse work environment are not consistent in terms of definition and measurement. Some measured nurse work environment broadly including all the aspects,16–18 while others only focused on the nurse staffing,19–21 a significant attribute that is relatively easier to be measured. Growing evidence has linked better nurse work environments to a variety of patient outcomes, including lower mortality rates, less failure-to-rescue, and nurse-reported quality of care.16,22–24 These findings suggest that improving hospital nurse work environment can result in better patient outcomes.
While increasing evidence on the nursing–outcomes relationship exists, a search of literature revealed that there has been no systematic review synthesizing and assessing the extant evidence of the role of nurse work environment in hospital readmission. To fill this gap in knowledge, the purpose of this study was to systematically review and evaluate studies examining the relationship between nurse work environment and readmission.
Methods
The Standards for Systematic Reviews was used to guide this review.25 The Standards for Systematic Reviews provides detailed recommendations for initiating a systematic review, finding and assessing individual studies, synthesizing the body of evidence, and reporting results. All recommendations were followed.
A comprehensive search was conducted by two reviewers (CM, JS) in three electronic databases: PubMed, CINAHL (Cumulative Index to Nursing and Allied Health Literature), and PsycINFO. Librarians with expertise in literature search in relevant areas were consulted to ensure an effective and accurate search. Nurse work environment can be measured by various surveys or assessments of the overall quality of nurse work environment or directly measured by nurse staffing levels. Therefore, search terms “readmission/s” and “rehospitalization/s” were used in various combinations with “work environment”, “working environment”, “work condition/s”, “working condition/s”, “nursing staff”, “nurse staffing”, “patient–nurse ratio/s”, “patient-to-nurse ratio/s”, “nurse–patient ratio/s”, “nurse-to-patient ratio/s”, “nursing hour/s”, “nursing care hour/s”, “RN mix”, and “skill mix”. In addition, reference lists of reviewed studies were hand searched for relevant articles.
Studies were considered eligible for review if they met the following criteria: original research examining the relationship between nurse work environment and readmission in hospital settings and published in English from January 2000 through January 2014. Two reviewers (CM, JS) assessed study eligibility. First, CM independently screened titles and abstracts, which JS then reviewed and confirmed eligibility. A second round screening was further conducted for final eligibility by the reviewers independently assessing the full text of the articles identified as relevant in the first round screening. Differences in eligibility assessments were resolved by discussion.
The following data were extracted from each study: research objective(s), study design, country, setting, study population, sample size, work environment and readmission measures, unit of analysis, confounding variables, analytic models, and findings. In addition, journal and year of publication of each reviewed study were noted. The quality of eligible studies was also assessed using a validated tool that includes 14 criteria and yields a summary score for each study.26 The original tool was slightly modified to meet the needs of this review by removing three items focusing on interventional and/or randomized control studies, which are not applicable to most observational studies. The remaining items assess internal validity, external validities, and overall clarity in writing, which are essential to the study quality. The final quality score for each study could range from 0–22, with a higher score indicating higher quality. To ensure the consistency of the criteria interpretation, the reviewers independently assessed one study and compared the results. After discussion and resolving the differences in interpretation, the reviewers independently assessed all the other articles. For those articles with three or more items with different scores, the reviewers discussed and reassessed to resolve all discrepancies.
Results
Study selection
The comprehensive search of the three databases yielded 301 articles (PubMed 164, CINAHL 87, and PsycINFO 50). After removing duplicates, 220 articles were screened for eligibility; 208 articles were excluded after title and abstract review. The main exclusion reasons were: no measure of work environment (146 articles), review (23 articles), news articles and editorials (10 articles), non-published dissertations (4 articles), no readmission measures (10 articles), and relationship between work environment and readmission not tested (15 articles). The reviewers independently assessed the full text of the remaining 12 studies and two were further excluded because the relationship of the variables of interest was not tested. Hand search of the reference lists of eligible studies found no extra articles. This resulted in ten studies for final review (Figure 1).
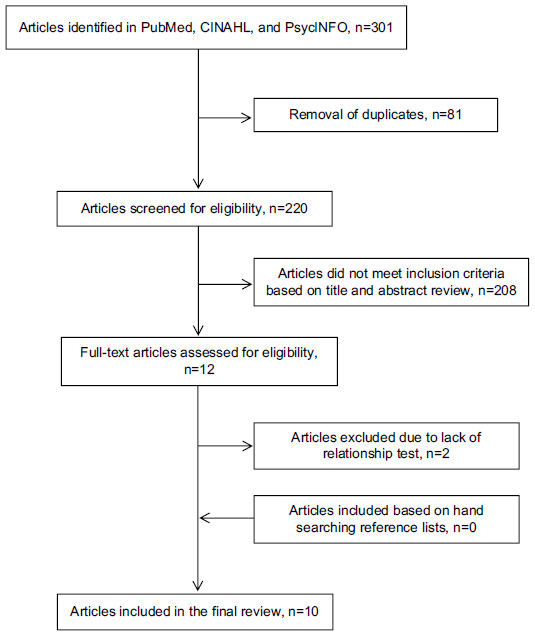 | Figure 1 Flow diagram for article selection. |
Characteristics of the studies
Characteristics of the reviewed studies are displayed in Table 1. Eight of the reviewed studies (80%) were conducted in the US;27–34 the other two were conducted in Canada (n=1, 10%)35 and Belgium (n=1, 10%).36 All included studies were multisite observational designs (seven were cross-sectional, two were retrospective, and one was prospective). The number of study sites varied from four hospitals to 4,091 hospitals.
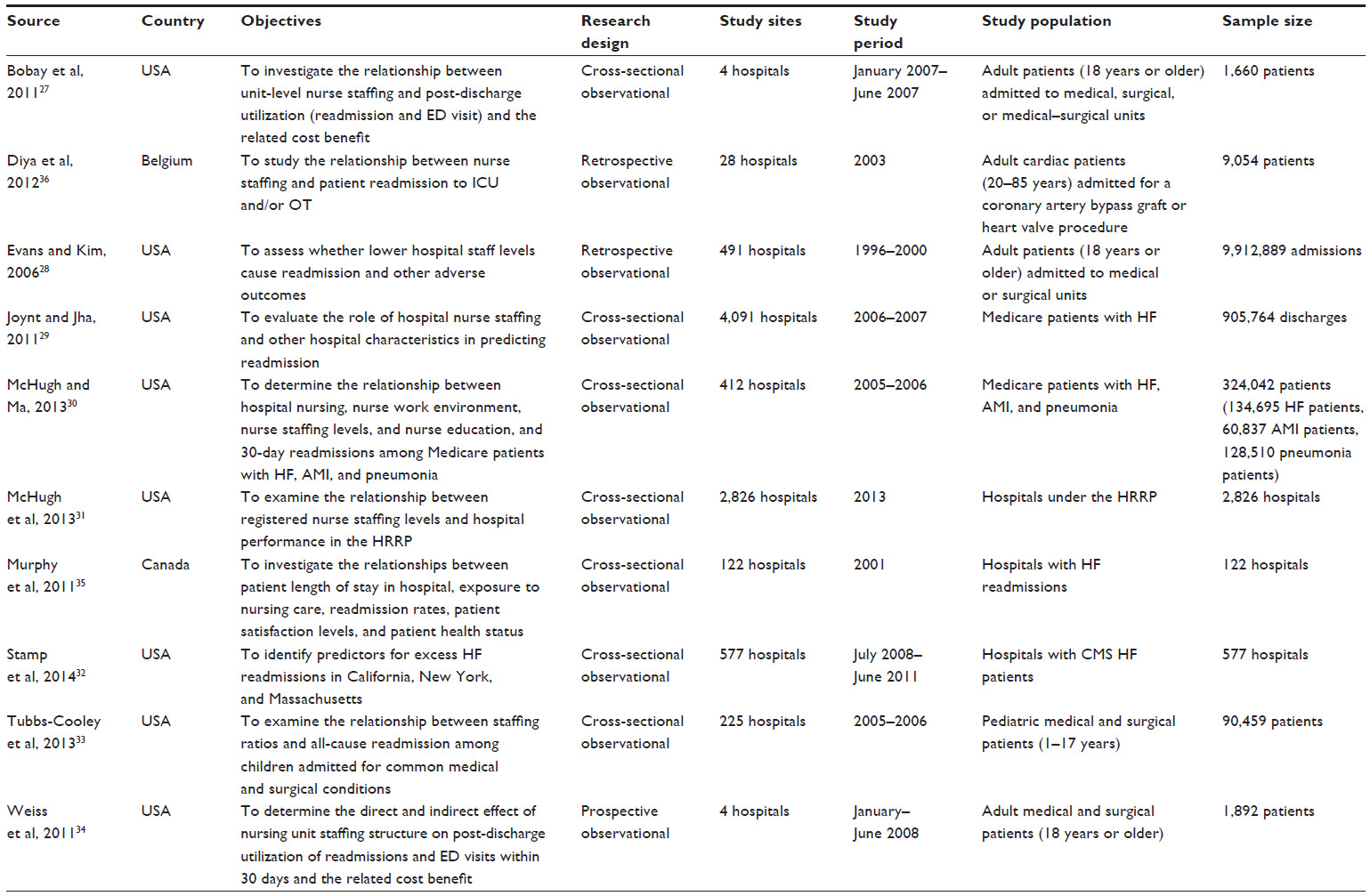 | Table 1 Characteristics of reviewed studies |
The levels of analysis and types of patients varied across studies. The majority of the studies (n=7, 70%) were conducted at the patient level.27–30,33,34,36 Of these, four (57%) studied adult patients (three focused on general adult medical/surgical patients27,28,34 and one focused on adult cardiac patients36), two (29%) focused on Medicare patients (one on patients with heart failure29 and the other on patients with diverse diagnoses such as heart failure, acute myocardial infarction, and pneumonia30), and one (14%) targeted on pediatric patients with general medical and surgical conditions.33 Three (30%) of the reviewed studies were conducted at hospital level.31,32,35 Of these, one focused on hospitals subject to the US Centers for Medicare and Medicaid Services’ (CMS) Hospital Readmission Reduction Program,31 one included hospitals with heart failure readmissions,35 and the third was on hospitals with CMS heart failure patients.32 The sample sizes varied and ranged from 1,660–9,912,889 patients for patient level studies and from 122–2,826 hospitals for studies conducting hospital-level analysis.
In half of the studies (n=5), researchers used readmission as the sole outcome,29–33 while in the other half researchers included other patient outcomes such as mortality,28,35,36 hospital length of stay,28,35 emergency department visit,27,34 and patient satisfaction.35 In all ten reviewed studies, researchers examined the relationship between readmissions and the nurse staffing component of the nurse work environment. One article also examined the overall quality of nurse work environment (measured by the Practice Environment Scale of the Nursing Work Index) in relation to readmission.30
Outcome measures
Table 2 summarizes the measures of the variables of interest and results in each study. Different time frames and definitions were used to identify readmissions. In the majority of studies (n=9, 90%), researchers operationalized readmission as 30 days from previous hospital discharge.27–35 However, in one study, researchers measured readmissions into the intensive care unit/operation room during the same hospital stay and did not specify its time frame.36 In addition to 30-day readmission, 7-day readmission was also used in the study by Evans and Kim28 and 14-day readmission was used in the study by Tubbs-Cooley et al.33 Furthermore, differences in the definitions of readmission were also observed in terms of the diagnostic relationship between index admission and readmission. In five studies (40%), researchers counted readmissions for any reason (all-cause) within the predefined time frame to calculate readmission rates.29–33 Of these, four research teams adopted CMS’s standardized all-cause readmission definition.29–32 In two studies, researchers measured readmissions only as those with a diagnosis that was the same as the primary diagnosis of the index admission or a comorbid condition of index admission.27,34 In one study, investigators defined readmissions as those admissions within 30 days of previous discharges and for the same diagnosis as the index admission;35 this was the strictest definition of readmissions among all the reviewed articles. In two studies, the researchers did not explicitly state how they defined readmissions (eg, all-cause, related, or in other ways).28,36
 | Table 2 Summary of measures of variables of interest and results |
Readmission was also treated differently in the statistical analyses. Seven patient-level studies treated readmission as a dichotomous variable indicating whether a patient was readmitted or not,27–30,33,34,36 while the three hospital-level studies (30%) used hospital readmission rates by calculating the proportion of patients readmitted for each hospital.31,32,35
Independent variable measures
As mentioned previously, only one research team included a survey measure of the nurse work environment.35 In all studies there was a measure of nurse staffing; however, different methods were used to calculate levels of nurse staffing. The most frequently used nurse staffing measure was nursing hours per patient day (eg, RN hours per patient day, non-RN hours per patient day, and total nursing hours per patient day).27,31,32,34–36 Researchers also calculated nurse staffing levels as the patient-to-nurse ratios.30,33 Joynt and Jha defined nurse staffing as the full-time equivalent nurses per 1,000 patient days.29 Evans and Kim employed an untraditional method to identify nurse staffing levels; they defined nurse staffing as the number of admissions over the next two days divided by the average of this value from the previous 8 weeks, which according to the authors measured the effective staff level faced by a patient.28
Results of reviewed studies
There were variations in the reported readmission rates. In five (50%) studies, researchers reported readmission rates of the study patients:27,28,30,33,34 the highest 30-day readmission rate was observed among Medicare patients with heart failure (23.3%),30 and the lowest 30-day readmission rate was observed among pediatric patients with common medical and surgical conditions (1.9%).33 Weiss et al reported both the all-cause readmission rate of 11.9% and the unplanned related readmission rate of 9.7% among adult general medical and surgical patients.34 One research team reported readmission rates by patient severity of illness and staffing levels instead of a direct report of the overall readmission rate among the study patients.36 In four studies, researchers reported hospital readmission rates or number of readmissions. In one of those studies, researchers reported the median readmission rate of 25.7% (interquartile 2.1%–30.0%) across hospitals.29 In another study, researchers reported that on average, the hospital had 98 readmissions for heart failure from July 2008 to June 2011.32 In the other two studies, investigators reported the percentage of study hospitals with/without CMS excess readmission rates31 or hospitals with readmission rates over 1%.35
In seven (70%) studies, researchers found a relationship between better work environment and lower hospital readmission rates.29–34,36 In another study (10%), researchers found that nurse work environment (measured as the nurse staffing) impacted readmission risk; however, this relationship was only identified in some of the models/subsamples.28 Two (20%) research teams did not identify any relationships between nurse work environment and readmissions.27,35
The relationship between work environment and readmission was found in studies analyzed at both the patient level and hospital level. For example, a patient-level study by McHugh and Ma reported that adding one additional patient per nurse was associated with lower odds of 30-day readmissions (7% lower for heart failure patients, 6% lower for pneumonia patients, and 9% lower for acute myocardial infarction patients) and patients discharged from hospitals with good (versus poor) work environment was associated with 7% lower odds for heart failure, 10% lower odds for pneumonia, and 6% lower odds for acute myocardial infarction readmissions.30 McHugh et al also reported in a hospital-level study that hospitals with higher nurse staffing levels had 25% lower odds of having excess readmission rates that resulted in penalties by CMS.31 In the study by Evans and Kim, a significant relationship between nurse staffing and readmission was more likely to be observed in patient groups with either highest mortality counts or mortality rates. In the two studies in which researchers found no significant relationships between nurse work environments and readmissions, the researchers, however, found that nurse staffing (ie, the indicator used for nurse work environment in these studies) was significantly associated with other patient outcomes including emergency department visits and length of stay.27,35
Methodological quality of studies
In general, all included studies were deemed to have a fair to good quality with the quality scores ranging from 17–22 out of 22 possible points. Indeed, the majority (n=8, 80%) of the articles had a quality score above 20. However, it should be noted that there were a couple of frequently observed weaknesses across the reviewed studies. None of the studies were experimental or semi-experimental designs which limited the interpretation of the findings. In the study with the lowest score, the researchers employed justified and appropriate analytic methods; however, these models did not fully address the research questions.35 In two of the ten studies, researchers conducted power analysis; however, this should not be considered as a major weakness of the other eight studies given their fairly large sample size (number of study patients ranged from 1,660–9,912,889 and number of study hospitals ranged from 122–2,826).
Discussion
This is the first systematic review examining evidence of the relationship between nurse work environment and readmission. It was found that a significant association between better nurse work environment (particularly the nurse staffing component of the work environment) and fewer readmissions was reported in the majority of the reviewed studies. This is consistent with the evidence showing significant associations between the nurse work environment, staffing, and other patient outcomes.23,37,38
However, it should also be noted that in two studies researchers did not identify relationships between nurse work environment and readmission.27,35 In one study, the authors explained that this failure may be due to the small sample size.27 Another possibility is the homogeneity of the study sample because all the data were extracted from 16 units (medical, surgical, or medical–surgical) in four hospitals that were within one health care system. Last, in both these studies, nurse work environment was only measured by nurse staffing measures.
This review suggests that there is sparse evidence examining the role of nurse work environment using a comprehensive definition in preventing/reducing readmissions. Only one study was found in which the researchers examined the overall quality of nurse work environment using a survey measure.30 Given its complexity, a challenge in conducting studies examining nurse work environment is how to accurately measure its quality. This is limited by the available valid and reliable instruments. McHugh and Ma used the Practice Environment Scale of the Nursing Work Index to measure the overall quality of nurse work environment,30 which has been endorsed by the National Quality Forum as a nurse sensitive measure39 and has been used across different clinical settings and countries.40 A limitation of this instrument is that it has five domains that developed from the characteristics of Magnet hospitals within the US, which may not reflect all the aspects of the nurse work environments of interest.
Also, little consistency was found in the definitions of readmissions, which can result in difficulties in comparing results across studies. Research on readmission can be traced back to the 1950s among psychiatric patients (eg, patients with schizophrenia).41–43 Despite rapid increase in readmission research, measures of readmissions have not been unified. Conceptually, researchers usually considered readmission as the subsequent admission of a patient to a hospital within a defined reference period. However, the operative definitions of readmission varied across studies. One cause of this variation is the disagreements in the length of a reasonable time frame between index admission and readmission. Researchers have used various time frames to define readmission, which can range from days to 1 year. In the past decade, the 30-day readmission has emerged as the most frequently applied measure because studies have shown that readmissions within 30 days following previous discharge are more likely related to quality of hospital care.7,44 CMS has adopted the 30-day time frame to calculate hospital readmission rates for the Hospital Readmission Reduction Program and public report on the Hospital Compare website as a metric of hospital care quality.
Readmissions were also defined differently upon their relation with the diagnoses of index admissions. Generally, three concepts were applicable: all-cause readmission, unplanned readmission, and related readmission. The proponents of using all-cause readmission argued that readmission for any reason is likely to be an undesirable outcome of care.45 However, others criticized this usage by arguing that some readmissions within the time frame of interest are intentionally scheduled as part of the patients’ plan of care and therefore should not be considered a proxy of care quality. These researchers included only unplanned readmissions in their study.27,34,46 The most restricted definition is the related readmission, which is defined as a readmission where the diagnosis is the same as the primary diagnosis of the index admission, a comorbid condition present on index admission, or a complication associated with index admission. Literately, this definition of readmission best reflects the quality of care patients receive. However, there is also a criticism that no reliable way has been established to determine whether a readmission is related to the previous hospital stay based on the limited numbers of documented reasons of readmissions.45 In addition, readmissions not directly related to index admissions may be also potentially avoidable.
Similar methodological issues were found in the reviewed studies. In all studies, the researchers employed observational designs (cross-sectional, retrospective, or prospective). The nature of the research design determines their inability to identify causality. Consequently, caution should be made when interpreting the results from these studies. On the other hand, given the nature of health services research, it is unlikely that a large enough randomized control trial will be feasible. Therefore, understanding how the investigators controlled for potential biases and confounding is critical. For example, one study has several strengths including using the CMS risk-adjusted standardized 30-day readmission measure and matching hospitals based on a long list of observed variables to create a set of hospitals for an “apples to apples” comparison to examine hospital nurse staffing levels in relation to readmission rates.31 However, despite the reviewers’ efforts, the interpretation of results was still limited by its cross-sectional research design. Another limitation is the use of administrative data sets to examine the nurse work environment, which is often limited to the indirect measure of nurse staffing. Additionally, staffing information in administrative data often includes both nurses providing direct patient care and those not.38 Therefore, this method is not precise and is likely to introduce measurement error.
Clinical implications
This review is informative to various health care stakeholders, particularly hospital executives who are under tremendous pressure, resulting from potential readmission penalties, to optimize hospital nursing to improve quality of care and reduce readmissions. The results indicate that creating a favorable nurse work environment facilitating professional nursing practice is a potentially effective way to reduce readmissions. Nurses’ participation in hospital affairs, foundations for quality of care, manager supervisory ability, collegial relationships between nurses and other health professionals, and adequate nurse staffing are some important attributes of the nurse work environment. Hospitals can initiate their work environment improvement programs from these specific areas. Moreover, other researchers have shown that improving hospital nurse work environments can be accomplished at little cost.47
One concern of hospital executives regarding increasing nurse staffing levels is that they are associated with a direct cost. This may lead to the reluctance of hiring more nurses; however, researchers have documented that the cost of increasing nurse staffing can be set off, at least partially, by the ensuing improvement in quality of care and patient outcomes.48,49 Regulatory mandates may also be considered by policymakers as an effective way to improve hospital quality through improved nurse work environments. For instance, California in the US implemented a mandate of a minimum patient-to-nurse staffing ratio, which has resulted in some success in improving nurse staffing in general as well as in hospitals serving vulnerable patients.50 In addition, reshaping the current health care payment system may be considered in order to give hospitals more incentives to improve nurse work environment beyond strict regulations such as the readmission penalties.27,34
In this review, it was found that readmissions were not uncommon and readmission rates were very high for some conditions. With a rapidly increasing older population and reduction in length of hospital stay, patients’ risk for readmissions will continue to be high or even increase if no effective prevention interventions are implemented. A critical initial step for any readmission reduction intervention is a reliable and standardized measure of readmission rates as reference and for future comparison. This review found that various definitions and measures were used in identifying readmissions across studies. Adopting measures created by large well-known health care agencies and organizations (eg, CMS, Agency for Health Research and Quality, and National Cancer Institute) that have been tested with large data sets and well maintained is recommended. The finding that readmission rates varied across patient groups with different medical conditions suggests that two patient groups deserve high attention: patients with (1) conditions of high readmission rates such as heart failure; and (2) conditions with other adverse events, particularly in hospitals with limited financial and clinical resources.
Suggestions for future research
As indicated by this review, more rigorous research is desired to provide stronger evidence examining the relationship between nurse work environment and readmission. First, standardized valid and reliable tools should be used to measure work environment and readmission. For example, many hospitals routinely survey employees on their work environments;17,51 including these types of survey results would increase the ability of researchers to estimate the impact of the comprehensive measure of nurse work environment on readmission. Second, given that the research designs in current studies have limited the result interpretations, longitudinal research design that can determine causal relations is needed. Finally, the wide use of administrative data suggests that more advanced statistical methods also should be considered and employed in future research, such as the instrumental variable method that helps control underlying unmeasured differences in study settings.
Limitations
This review has several limitations. It only included articles in English and published from 2000. Given the dramatic changes in health care settings in the past decade, limiting the search to publications from 2000 is justified. Despite comprehensive search strategies applied in the literature search process, there is still a chance that relevant articles may be missed. Although hand searching of reference lists was conducted, the reviewers did not reach out for gray literature which may result in publication bias. This review is a narrative review of relevant articles. Meta-analysis was considered but was not conducted because of incompletion of required statistics for meta-analysis in some studies.
Conclusion
This review examined empirical evidence on the nursing–readmission relationship and suggested that improving nurse work environment (overall and/or the nurse staffing component) can be considered a strategy to prevent readmissions. Meanwhile, given the relatively small number of eligible articles, more studies with rigorous research design are desired to further examine the relationship between nurse work environment and readmission.
Acknowledgment
The authors would like to thank the librarians at the University of Kansas for their assistance in searching the literature.
Disclosure
The authors report no conflicts of interest in this work.
References
Bueno H, Ross JS, Wang Y, et al. Trends in length of stay and short-term outcomes among Medicare patients hospitalized for heart failure, 1993–2006. JAMA. 2010;303(21):2141–2147. | |
Heggestad T. Do hospital length of stay and staffing ratio affect elderly patients’ risk of readmission? A nation-wide study of Norwegian hospitals. Health Serv Res. 2002;37(3):647–665. | |
Monette M. Hospital readmission rates under the microscope. CMAJ. 2012;184(12):E651–E652. | |
Goodman DC, Fisher ES, Chang CH. After Hospitalization: A Dartmouth Atlas Report on Post-Acute Care for Medicare Beneficiaries. Lebanon, NH: The Dartmouth Institute for Health Policy and Clinical Practice; 2011. Available from: http://www.dartmouthatlas.org/downloads/reports/Post_discharge_events_092811.pdf. Accessed June 10, 2014. | |
Dobrzanska L, Newell R. Readmissions: a primary care examination of reasons for readmission of older people and possible readmission risk factors. J Clin Nurs. 2006;15(5):599–606. | |
Bjorvatn A. Hospital readmission among elderly patients. Eur J Health Econ. 2013;14(5):809–820. | |
Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418–1428. | |
Kohn LT, Corrigan JM, Donaldson MS; Institute of Medicine. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000. | |
Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001. | |
Rau J. Medicare to penalize 2,211 hospitals for excess readmissions [webpage on the Internet]. Menlo Park, CA: Kaiser Health News; 2012 [updated October 12, 2012]. Available from: http://www.kaiserhealth news.org/stories/2012/august/13/medicare-hospitals-readmissions-penalties.aspx. Accessed June 10, 2014. | |
Kane NM, Siegrist RB Jr. Understanding Rising Hospital Inpatient Costs: Key Components of Cost and the Impact of Poor Quality. Chicago, IL: The Heartland Institute; 2002. Available from: http://news.heartland.org/sites/all/modules/custom/heartland_migration/files/pdfs/14629.pdf. Accessed June 10, 2014. | |
Bureau of Labor Statistics. Occupational Outlook Handbook 2010–2011 Ed. Registered Nurses. Available from: http://www.bls.gov/ooh/healthcare/registered-nurses.htm. Accessed April 16, 2014. | |
Kutney-Lee A, Lake EH, Aiken LT. Development of the hospital nurse surveillance capacity profile. Res Nurs Health. 2009;32(2):217–228. | |
Lake EH. Development of the Practice Environment Scale of the Nursing Work Index. Res Nurs Health. 2002;25(3):176–188. | |
Page A; Institute of Medicine. Keeping Patients Safe: Transforming the Work Environment of Nurses. Washington, DC: National Academy Press; 2004. | |
Aiken LH, Sloane DM, Clark S, et al. Importance of work environments on hospital outcomes in nine countries. Int J Qual Health Care. 2011;23(4):357–364. | |
Choi J, Boyle DK. Differences in nursing practice environment among US acute care unit types: a descriptive study. Int J Nurs Stud. Epub March 12, 2014. | |
Friese CR, Lake ET, Aiken LH, Silber JH, Sochalski J. Hospital nurse practice environments and outcomes for surgical oncology patients. Health Serv Res. 2008;43(4):1145–1163. | |
Wiltse Nicely KL, Sloane DM, Aiken LH. Lower mortality for abdominal aortic aneurysm repair in high-volume hospitals is contingent upon nurse staffing. Health Serv Res. 2013;48(3):972–991. | |
McGahan M, Kucharski G, Coyer F. Nurse staffing levels and the incidence of mortality and morbidity in the adult intensive care unit: a literature review. Aust Crit Care. 2012;25(2):64–77. | |
Carthon JM, Kutney-Lee A, Jarrin O, Sloane D, Aiken LH. Nurse staffing and postsurgical outcomes in black adults. J Am Geriatr Soc. 2012;60(6):1078–1084. | |
Friese CR. Nursing Organization and Outcomes for Surgical Oncology Patients [dissertation]. Philadelphia, PA: University of Pennsylvania; 2005. | |
Needleman J, Buerhaus P, Pankratz VS, Leibson CL, Stevens SR, Harris M. Nurse staffing and inpatient hospital mortality. N Engl J Med. 2011;364(11):1037–1045. | |
Djukic M, Kovner CT, Brewer CS, Fatehi FK, Cline DD. Work environment factors other than staffing associated with nurses’ ratings of patient care quality. Health Care Manage Rev. 2013;38(2):105–114. | |
Institute of Medicine. Finding What Works in Health Care: Standards for Systematic Reviews. Washington, DC: Institute of Medicaine; 2011. Available from: http://www.iom.edu~/media/Files/Report%20Files/2011/Finding-What-Works-in-Health-Care-Standards-for-Systematic-Reviews/Standards%20for%20Systematic%20Review%202010%20Insert.pdf. Accessed June 10, 2014. | |
Kmet LM, Lee RC, Cook LS. Standard Quality Assessment Criteria for Evaluating Primary Research Papers. Alberta: Alberta Heritage Foundation for Medical Research; 2004. Available from: http://www.ihe.ca/documents/HTA-FR13.pdf. Accessed June 10, 2014. | |
Bobay K, Yakusheva O, Weiss M. Outcomes and cost analysis of the impact of unit-level nurse staffing on post-discharge utilization. Nurs Econ. 2011;29(2):69–78, 87. | |
Evans WN, Kim B. Patient outcomes when hospitals experience a surge in admissions. J Health Econ. 2006;25(2):365–388. | |
Joynt KE, Jha AK. Who has higher readmission rates for heart failure, and why? Implications for efforts to improve care using financial incentives. Circ Cardiovasc Qual Outcomes. 2011;4(1):53–59. | |
McHugh MD, Ma C. Hospital nursing and 30-day readmissions among Medicare patients with heart failure, acute myocardial infarction, and pneumonia. Med Care. 2013;51(1):52–59. | |
McHugh MD, Berez J, Small DS. Hospitals with higher nurse staffing had lower odds of readmissions penalties than hospitals with lower staffing. Health Aff (Millwood). 2013;32(10):1740–1747. | |
Stamp KD, Flanagan J, Gregas M, Shindul-Rothschild J. Predictors of excess heart failure readmissions: implications for nursing practice. J Nurs Care Qual. 2014;29(2):115–123. | |
Tubbs-Cooley HL, Cimiotti JP, Silber JH, Sloane DM, Aiken LH. An observational study of nurse staffing ratios and hospital readmission among children admitted for common conditions. BMJ Qual Saf. 2013;22(9):735–742. | |
Weiss ME, Yakusheva O, Bobay KL. Quality and cost analysis of nurse staffing, discharge preparation, and postdischarge utilization. Health Serv Res. 2011;46(5):1473–1494. | |
Murphy GT, Birch S, O’Brien Pallas L, Kephart G, MacKenzie A. Nursing inputs and outcomes of hospital care: an empirical analysis of Ontario’s acute-care hospitals. Can J Nurs Res. 2011;43(1):126–146. | |
Diya L, Van den Heede K, Sermeus W, Lesaffre E. The relationship between in-hospital mortality, readmission into the intensive care nursing unit and/or operating theatre, and nurse staffing levels. J Adv Nurs. 2012;68(5):1073–1081. | |
Aiken LH, Clarke SP, Sloane DM, Lake ET, Cheney T. Effects of hospital care environment on patient mortality and nurse outcomes. J Nurs Adm. 2008;38(5):223–229. | |
Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002;288(16):1987–1993. | |
National Quality Forum. National Voluntary Consensus Standards for Nursing-Sensitive Care: An Initial Performance Measure Set. Washington, DC: National Quality Forum; 2004. | |
Warshawsky NE, Havens DS. Global use of the Practice Environment Scale of the Nursing Work Index. Nurs Res. 2011;60(1):17–31. | |
Israel RH, Johnson NA. Discharge and readmission rates in 4,254 consecutive first admissions of schizophrenia. Am J Psychiatry. 1956; 112(11):903–909. | |
Jenkins RL, Bemiss EL Jr, Lorr M. Duration of hospitalization, readmission rate, and stability of diagnoses in veterans hospitalized with neuropsychiatric diagnoses. Psychiatr Q. 1953;27(1):59–72. | |
Michtom J, Goldberg N, Offenkrantz W, Whittier J. Readmission rates for state mental hospital patients discharged on maintenance ataractics; findings with a matched control group and methodological considerations. J Nerv Ment Dis. 1957;125(3):478–480. | |
Payment policy for inpatient readmissions. In: Medicare Payment Advisory Commision. Report to the Congress: Promoting Greater Efficiency in Medicare. Washington, DC: Medicare Payment Advisory Commision; 2007:103–120. | |
Keenan PS, Normand SL, Lin Z, et al. An administrative claims measure suitable for profiling hospital performance on the basis of 30-day all-cause readmission rates among patients with heart failure. Circ Cardiovasc Qual Outcomes. 2008;1(1):29–37. | |
Horwitz LI, Grady JN, Lin Z, et al. 2013 Measure Updates and Specifications: Hospital-Wide All-Cause Unplanned Readmission Measure. Woodlawn, MD: Centers for Medicare and Medicaid Services; 2013. | |
Mark BA, Lindley L, Jones CB. Nurse working conditions and nursing unit costs. Policy Polit Nurs Pract. 2009;10(2):120–128. | |
Dall TM, Chen YJ, Seifert RF, Maddox PJ, Hogan PF. The economic value of professional nursing. Med Care. 2009;47(1):97–104. | |
Rothberg MB, Abraham I, Lindenauer PK, Rose DN. Improving nurse-to-patient staffing ratios as a cost-effective safety intervention. Med Care. 2005;43(8):785–791. | |
McHugh MD, Brooks Carthon M, Sloane DM, Wu E, Kelly L, Aiken LH. Impact of nurse staffing mandates on safety-net hospitals: lessons from California. Milbank Q. 2012;90(1):160–186. | |
Osatuke K, McNamara B, Pohl M, et al. Response rates and incentives in a national employee survey: the case of the Veterans Administration. Applied HRM Research. 2013;13(1):37–50. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.