Back to Journals » Patient Preference and Adherence » Volume 20
Latent Physical Activity Patterns and Their Related Factors in Breast Cancer Patients During Chemotherapy Intervals
Authors Shi S, Chang G, Xie C, Xiao J ![]() , Liu Y, Cai S
, Liu Y, Cai S
Received 4 September 2025
Accepted for publication 25 December 2025
Published 29 January 2026 Volume 2026:20 561144
DOI https://doi.org/10.2147/PPA.S561144
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Emma Veale
Siqi Shi,1 Guangting Chang,2 Chunying Xie,1 Jingjing Xiao,3 Yanling Liu,4 Shu Cai1
1School of Nursing, Guangdong Pharmaceutical University, Guangzhou, Guangdong, People’s Republic of China; 2School of Nursing, Guangzhou Xinhua College, Guangzhou, Guangdong, People’s Republic of China; 3Department of Nursing, Guangdong Women and Children Hospital, Guangzhou, Guangdong, People’s Republic of China; 4Department of Obstetrics, Guangdong Women and Children Hospital, Guangzhou, Guangdong, People’s Republic of China
Correspondence: Shu Cai, School of Nursing, Guangdong Pharmaceutical University, 283 Jianghai Avenue, Haizhu District, Guangzhou, Guangdong, 510310, People’s Republic of China, Email [email protected]
Objective: Previous research on breast cancer patients has primarily examined singular behavioral indicators, often overlooking the coexistence and interaction between physical activity and sedentary behavior—particularly screen-based sedentary time. This study aims to identify the latent activity pattern categories among breast cancer patients during chemotherapy intervals and explore their associated factors to inform targeted behavioral interventions.
Methods: A cross-sectional survey was conducted with 292 breast cancer patients undergoing chemotherapy intervals at four general hospitals in Foshan, Guangdong Province. Latent Profile Analysis (LPA) was applied as a person-centered analytic approach to identify distinct activity pattern profiles. Data were collected using a general information questionnaire, the Adult Sedentary Behavior Questionnaire (ASBQ), the Chinese version of the International Physical Activity Questionnaire (IPAQ-SC), the Exercise Self-Efficacy Scale (ESES), the Perceived Social Support Scale (PSSS), and the Hospital Anxiety and Depression Scale (HADS).
Results: The activity patterns of breast cancer patients were categorized into three groups: Moderate Activity-Dominant Group (37.33%), Screen-Sedentary High-Risk Group (8.22%), and Activity-Sedentary Coexistence Group (54.45%). Logistic regression analysis showed that, compared to the Moderate Activity-Dominant Group, patients with low exercise self-efficacy and higher anxiety and depression levels were more likely to be classified into the Screen-Sedentary High-Risk Group and Activity-Sedentary Coexistence Group. Higher education levels and being on medical leave were associated with a higher probability of belonging to the Activity-Sedentary Coexistence Group (all P < 0.05).
Conclusion: Activity patterns in breast cancer patients show significant heterogeneity. Healthcare providers should pay attention to the individual physical activity characteristics of patients and offer personalized physical activity guidance. Tailored interventions that meet the needs of breast cancer patients should be developed to improve health outcomes.
Keywords: breast cancer, physical activity, sedentary behavior, latent profile analysis, exercise self-efficacy
Background
The Global Burden of Disease (GBD) study shows that the global burden of breast cancer has increased significantly, and the number of breast cancer cases is expected to continue to rise through 2050, posing a serious threat to women’s health and lives.1 Chemotherapy, as an important treatment for breast cancer, is often accompanied by side effects such as vomiting, insomnia, edema, and cancer-related fatigue. These side effects not only worsen the patients’ physical discomfort but also significantly impact their mental health and quality of life.2 To alleviate these symptoms, breast cancer patients often adopt sedentary behaviors, such as prolonged sitting, during chemotherapy intervals to rest and maintain their physical condition.3 Studies have shown that 57% to 79% of breast cancer patients’ waking hours are spent sitting during chemotherapy breaks, with screen-related sedentary behavior being particularly common.4,5
A large body of evidence indicates that the total sedentary time of breast cancer patients is closely associated with the risk of disease recurrence and mortality.6 Sedentary behavior, especially prolonged screen use, is one of the independent predictors of breast cancer mortality.7 Prolonged sitting not only reduces social opportunities for patients but also is associated with worsened mental health.8 In contrast, regular physical activity offers significant health benefits for cancer survivors, including improved cardiovascular function, reduced cancer-related fatigue, alleviation of anxiety and depression, and ultimately, enhanced quality of life.9–11 Crucially, the interplay between these two behaviors is complex and has direct health implications. For instance, research using isotemporal substitution models demonstrates that replacing sedentary time with physical activity—even light-intensity activity like walking—is associated with a significantly reduced risk of all-cause and cause-specific mortality.12 This highlights that physical activity and sedentary behavior are not merely opposites but coexist in a person’s daily routine; increasing one often displaces the other, with meaningful consequences for health.13 Some international organizations suggest that physical activity and total sedentary time should be considered together as part of overall movement behavior, rather than focusing on only one behavior.14,15 Therefore, when considering the impact of physical activity and sedentary behavior on breast cancer patients, their synergistic effects must be taken into account. However, previous research on physical activity in breast cancer patients has often focused on single behavioral indicators and has not fully considered the coexistence of physical activity and sedentary behavior at the individual level, particularly lacking in-depth attention to screen-based sedentary time. To better understand the activity patterns of breast cancer patients in a more comprehensive manner, a method that simultaneously considers both physical activity and sedentary behavior is needed.
Latent Profile Analysis (LPA) is a statistical method based on individual manifest variables that can identify and categorize different activity patterns,16 using cluster analysis to explore heterogeneity in physical activity and sedentary behavior among patient populations. Previous studies have used latent class models to investigate different types of activity patterns, with each subtype maintaining local independence. For instance, Park et al17 used LPA to examine the combination patterns of light physical activity and sedentary behavior in 534 patients with dyslipidemia in South Korea, identifying three distinct activity patterns. These studies show that LPA effectively combines the characteristics of physical activity and sedentary behavior, revealing the latent categories of different activity patterns. Beyond its ability to incorporate multiple behavioral indicators, LPA offers a person-centered analytical perspective that reveals underlying subgroups within a population, providing a clearer understanding of behavioral heterogeneity that cannot be captured by traditional variable-centered approaches.
However, there is limited application of LPA for activity pattern classification in breast cancer patients. Therefore, this study aims to use LPA to explore the distribution characteristics of activity patterns during chemotherapy intervals in breast cancer patients and identify the associated factors for different categories, which may in turn support the development of more personalized and practical behavioral intervention strategies in clinical settings.
Methods
This study adopted a convenience sampling approach and was conducted between September 2023 and December 2023 in four hospitals in Foshan, Guangdong Province, China: Foshan Maternal and Child Health Hospital, Guangdong Provincial Hospital of Integrated Traditional Chinese and Western Medicine (Foshan), Sixth Affiliated Hospital of South China University of Technology, and the Seventh Affiliated Hospital of Southern Medical University. Inclusion criteria: (1) Aged ≥ 18 years; (2) Diagnosed with breast cancer through pathological examination and hospitalized; (3) In chemotherapy intervals; (4) Clear consciousness with no communication barriers; (5) Informed consent and voluntary participation in the study. Exclusion criteria: (1) Patients with severe heart, lung, or other major organ diseases that would limit participation in daily physical activity, as determined by their attending physician or based on medical records; (2) Patients with diagnosed mental disorders or severe psychological conditions; (3) Patients with exercise contraindications as advised by clinicians; (4) Patients who were unaware of their diagnosis of breast cancer (eg, not informed by family or medical staff), as verified through clinical communication. For Latent Profile Analysis (LPA), at least 200 cases are recommended to ensure model stability.18 The final sample size of 292 exceeded this recommended threshold, indicating adequate statistical power for stable profile estimation. After obtaining permission from the hospital administration and the breast surgery department, and securing written informed consent from all participants, the researcher collected questionnaire data from patients during their chemotherapy intervals. Ultimately, In this study, a final cohort of 292 subjects was included.
Investigation Tools
General Information Questionnaire
This questionnaire was self-developed by the research team based on a comprehensive literature review and clinical experience, and reviewed by five experts in oncology nursing and behavioral medicine to ensure content validity and clarity. The questionnaire collected demographic and clinical characteristics, including age, body mass index (BMI), residence, education level, marital status, number of children, employment status, household registration type, family monthly income, and type of medical insurance. Disease-related information was also obtained, such as disease stage, number of chemotherapy cycles, pain, sleep quality, Charlson Comorbidity Index (CCI), disease duration, and surgical methods. Pain and sleep quality were assessed through patient self-report. Pain was categorized as none, mild, moderate, or severe, while sleep quality was classified as good, average, poor, or very poor according to the patient’s overall experience during the previous week.
Adult Sedentary Behavior Questionnaire (ASBQ)
This questionnaire was developed by domestic scholar Tian Tian in 201919 to assess sedentary behavior in adults in China. The questionnaire consists of 10 self-administered closed-ended questions, measuring the time spent on 10 daily activities over the past week. The test-retest reliability of the questionnaire is 0.82. According to previous studies, sedentary behavior is defined as a duration of more than 6 hours per day.
Exercise Self-Efficacy Scale (ESES)
The Exercise Self-Efficacy Scale (ESES) used in this study is based on Bandura’s guidelines for constructing self-efficacy scales.20 This scale was translated and revised by domestic scholar Li Dan based on foreign scales.21 It comprehensively considers multiple factors, including physiological, psychological, physical environment, and social environment, and includes 15 items. The rating of the entries uses a 5-point Likert scale, with scores ranging from 1 (representing “completely no confidence”) to 5 (representing “completely confident”). The total score ranges from 15 to 75 points, with higher scores indicating stronger exercise self-efficacy. The Cronbach’s α coefficient for this scale is 0.963.
International Physical Activity Questionnaire – Short Form (IPAQ-SC)
The Chinese version of the International Physical Activity Questionnaire – Short Form (IPAQ-SC) was translated and adapted by Qu Ningning et al,22 and contains six items that assess walking, moderate, and vigorous physical activity during the past seven days. Total physical activity is calculated as MET-minutes/week (MET-min/week) by multiplying the MET value of each activity by the daily activity time and number of days. According to the IPAQ scoring protocol, physical activity levels are classified into high, moderate, and low categories. The Chinese version has demonstrated good reliability and validity in previous studies and has been widely used in Chinese populations.
Perceived Social Support Scale (PSSS)
The Perceived Social Support Scale (PSSS) is designed to assess an individual’s perceived social support from family, friends, and significant others. The scale was originally developed by Zimet et al23 and later translated and revised into Chinese by Jiang Qianjin.24 It contains 12 items across three dimensions, each rated on a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree). Higher scores indicate stronger perceived social support. In this study, the Cronbach’s α coefficient for the PSSS was 0.89.
Hospital Anxiety and Depression Scale (HADS)
Developed by Zigmond and Snaith in 198325 this scale is used to screen for anxiety and depression symptoms in hospitalized patients (non-psychiatric). The scale includes two dimensions: anxiety (7 items) and depression (7 items). Each item is scored on a 0–3 scale, with higher scores indicating more severe anxiety or depression symptoms. The validated Chinese version of the HADS translated and evaluated by Sun Zhenxiao et al was used in this study.26 The Cronbach’s α coefficient for this scale in this study is 0.956.
Data Collection Method
Before the formal data collection, a pilot test involving 15 breast cancer patients undergoing chemotherapy was conducted to evaluate the clarity, completeness, and feasibility of the questionnaire package. Based on the pilot results, minor adjustments were made to the general information section where necessary. The revised questionnaire was reviewed and confirmed by four senior breast cancer specialists before being used in the formal survey, ensuring the scientific rigor and appropriateness of the instrument. After obtaining permission from the hospital administration and the breast surgery department, the researcher was responsible for collecting relevant data from patients during their previous chemotherapy intervals. Before the survey, the purpose and content of the study were explained to the breast cancer patients, and they were guided to complete the survey using a standardized script. Questionnaires with incomplete responses were excluded during data collection. To minimize potential selection bias, consistent inclusion and exclusion criteria and standardized recruitment procedures were applied across all participating hospitals. A total of 314 questionnaires were distributed, and 292 valid questionnaires were returned, resulting in an effective response rate of 93%.
Statistical Methods
Statistical analysis was conducted using Mplus 8.3 and SPSS 26.0 software. Using the latent class number 1 model as the baseline, the number of latent classes was gradually increased, and model fit was tested to select the optimal model. Common evaluation criteria include: Information criteria: Akaike Information Criterion (AIC),27 Bayesian Information Criterion (BIC),28 and adjusted Bayesian Information Criterion (aBIC), with smaller values indicating better fit. Common likelihood ratio test indicators include the Likelihood Ratio Test (LMRT) and the Bootstrap Likelihood Ratio Test (BLRT).29,30 Classification quality indicators: Entropy (ranging from 0 to 1), with values closer to 1 indicating higher classification accuracy.31 If the P-value for BLRT and LMRT is < 0.05, it indicates that the model with k latent classes fits better than the model with k-1 classes. The three continuous indicators (PA in MET-min/week, screen-based SB in minutes/day, and total SB in minutes/day) were standardized using Z-scores before conducting the LPA to place them on a comparable scale and facilitate model convergence. For data analysis, Chi-square tests, one-way ANOVA, and multiple logistic regression analysis were performed. The significance level was set at α = 0.05.
Results
Participants and Sociodemographic Characteristics
The ages of the patients ranged from 26 to 81 years, with a mean age of 52.32 ± 11.07 years. As shown in Table 1, most participants were between 40 and 59 years old, and half of the sample lived in urban areas. Regarding education, 38.4% had an elementary school education or below. A large proportion of patients were on medical leave during treatment. More than half of the participants had agricultural household registration, and 40.4% reported a monthly household income between 2000 and 5000 RMB. With respect to medical insurance, 69.9% were covered by resident insurance and 26.4% by the New Rural Cooperative Medical Insurance. In terms of clinical characteristics, 71.6% experienced mild pain, and 50.0% reported average sleep quality during chemotherapy intervals. Additionally, 72.3% had a Charlson Comorbidity Index score of 3 or above, and 45.9% had a disease duration of six months or less. Regarding treatment history, 68.5% underwent breast-conserving surgery, while 77.7% had received four or more chemotherapy cycles.
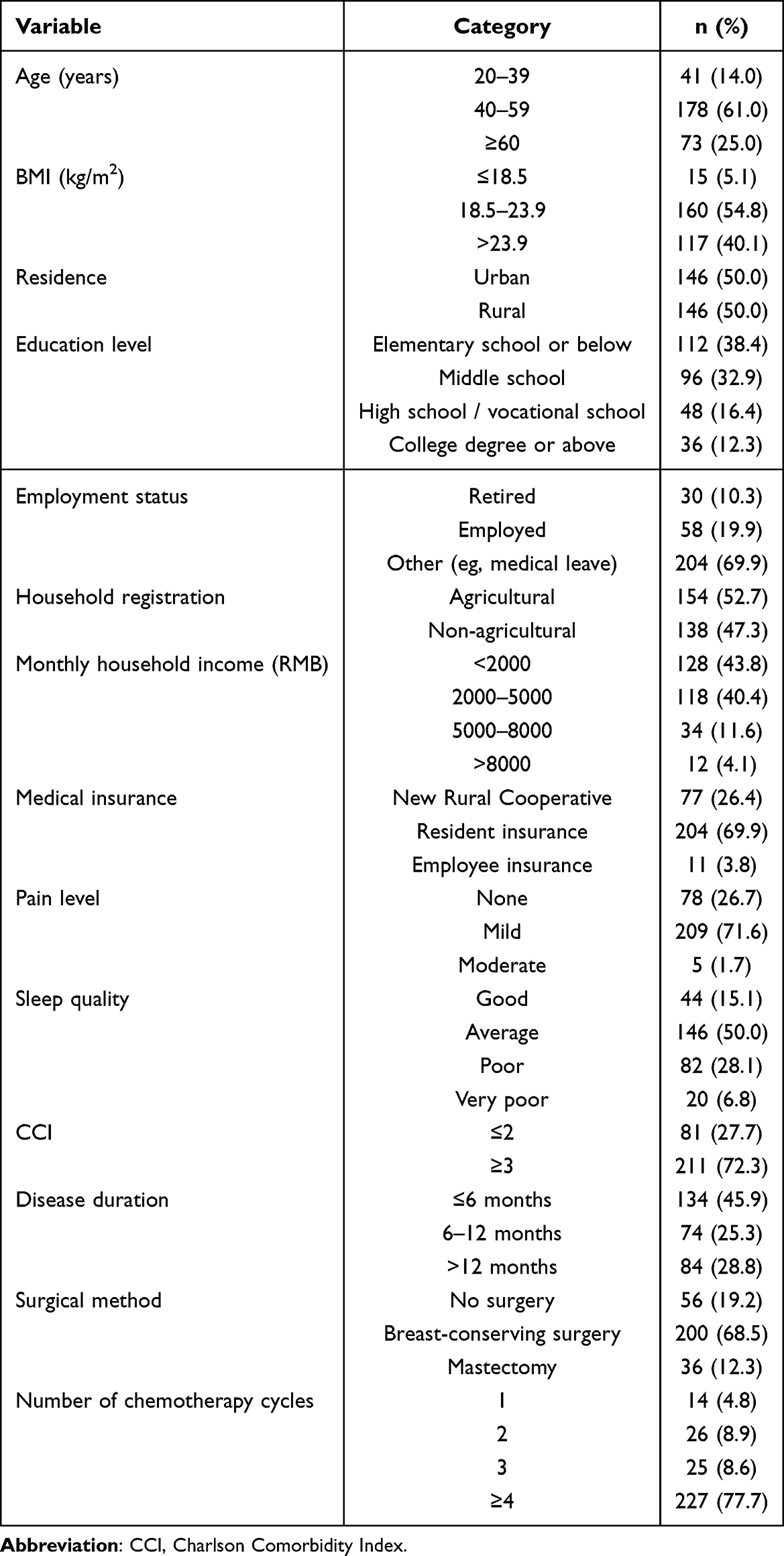 |
Table 1 Sociodemographic and Clinical Characteristics of Participants (N = 292) |
Latent Profile Analysis of Activity Patterns in Breast Cancer Patients
As shown in Table 2, the model fit indices for latent class numbers ranging from 1 to 5 indicated that both AIC and aBIC values continuously decreased as the number of profiles increased, suggesting that model fit improved with more categories. However, the BIC value reached its lowest point at the 3-class model before rising again, indicating that excessive categorization might affect the model’s validity. The entropy value was highest for the 3-class model, indicating good classification reliability. Likelihood ratio tests (LMR and BLRT) showed significant results (P < 0.05) for all models with additional profiles, supporting the extension of categories. Based on these considerations, the 3-profile model was determined to be the optimal solution.
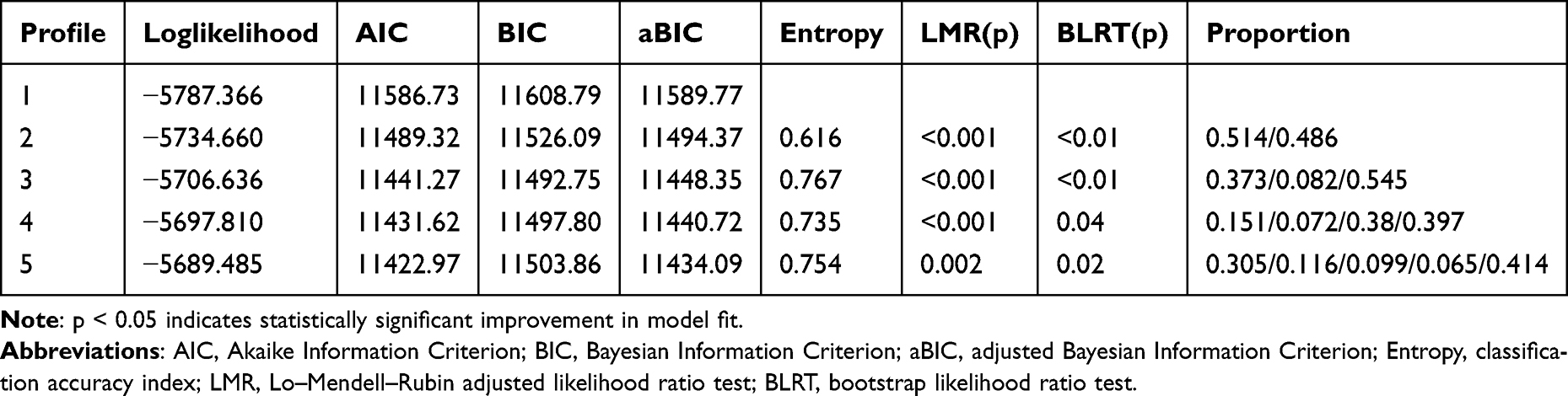 |
Table 2 Potential Profile Analysis of Activity Patterns |
Characteristics and Naming of Latent Activity Pattern Categories in Breast Cancer Patients
Based on the analysis, a potential profile of patient activity patterns was drawn, as shown in Figure 1. Three latent categories of activity patterns in breast cancer patients were identified and named based on their characteristics. Category 1 (109 patients, 37.33%): This category exhibited the highest total physical activity, with both screen-related sedentary behavior and total sedentary time lower than those in Categories 2 and 3. Therefore, it was named the “Moderate Activity-Dominant Group”. “Screen-Sedentary High-Risk Group” (24 patients, 8.22%): This category had the lowest physical activity score compared to Categories 1 and 3, and both sedentary behavior and screen-related sedentary behavior were higher than in the other two categories. Specifically, screen time accounted for about half of the total sedentary time. Thus, this category was named the “Screen-Sedentary High-Risk Group.”Category 3 (159 patients, 54.45%): This category had a physical activity score lower than Category 1 but higher than Category 2, with both screen-related sedentary behavior and total sedentary behavior significantly higher. This category exhibited a coexistence of physical activity and high sedentary behavior, so it was named the “Activity-Sedentary Coexistence Group.” As shown in Table 3.
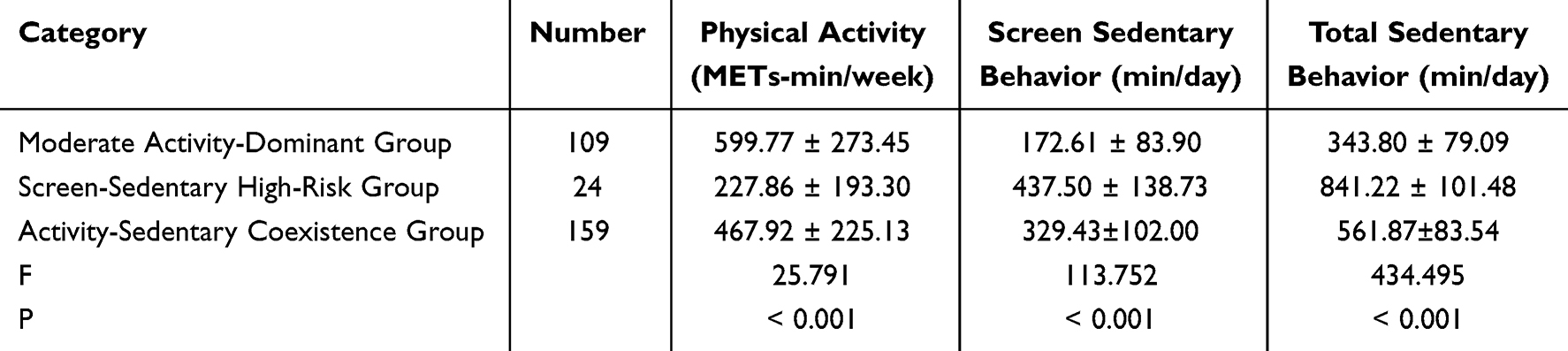 |
Table 3 Activity Patterns of Breast Cancer Patients in Different Potential Categories (n=292) |
 |
Figure 1 Latent Profile Analysis of Activity Patterns in Breast Cancer Patients. |
Differences in Baseline Characteristics Among the Three Activity Pattern Categories
There were statistically significant differences in age, education level, employment status, family monthly income, pain status, sleep quality, exercise self-efficacy, social support, and scores on the Hospital Anxiety and Depression Scale (HADS) among the three activity pattern categories: Moderate Activity-Dominant Group, Screen-Sedentary High-Risk Group, and Activity-Sedentary Coexistence Group (P < 0.05). However, no statistically significant differences were observed between the categories in terms of BMI, household registration type, and medical insurance type (P > 0.05). The detailed comparisons are shown in Table 4.
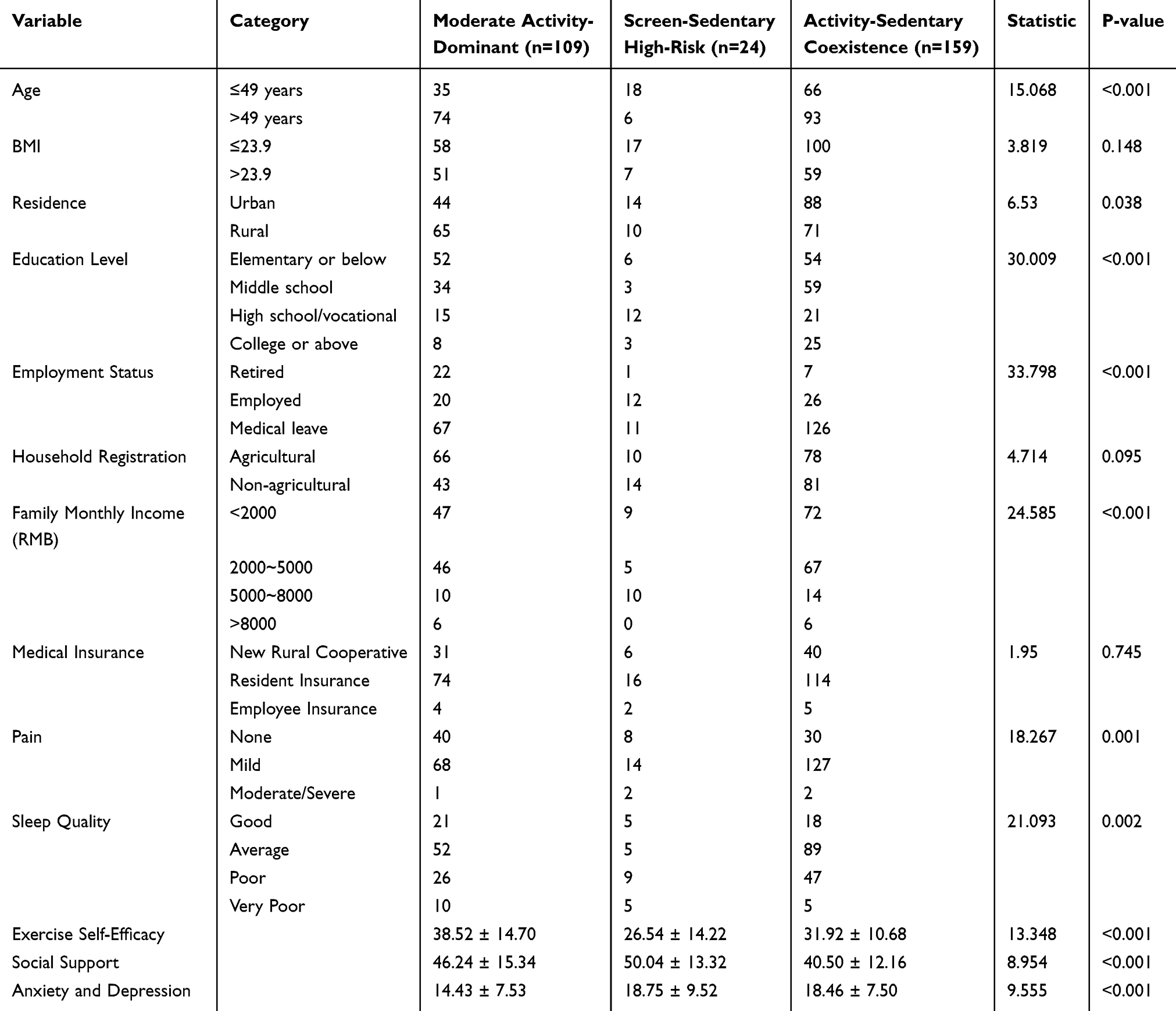 |
Table 4 Univariate Analysis of Latent Profiles of Activity Patterns in Breast Cancer Patients |
Multinomial Logistic Regression Analysis of Latent Activity Pattern Profiles in Breast Cancer Patients
A multinomial logistic regression analysis was performed using the three latent activity pattern profiles as the dependent variable (with the “Moderate Activity-Dominant Group” as the reference category). Variables that were statistically significant in the univariate analysis were entered into the model as independent variables. Multicollinearity diagnostics showed that the variance inflation factor (VIF) values were all below 10, indicating no significant multicollinearity among the variables. The results showed that education level (with elementary school or below as the reference), employment status (with retired as the reference), exercise self-efficacy, and hospital anxiety and depression levels were significant factors associated with latent activity pattern classification among breast cancer patients during chemotherapy intervals (P < 0.05). Only variables that remained statistically significant in the final model are presented in Table 5.
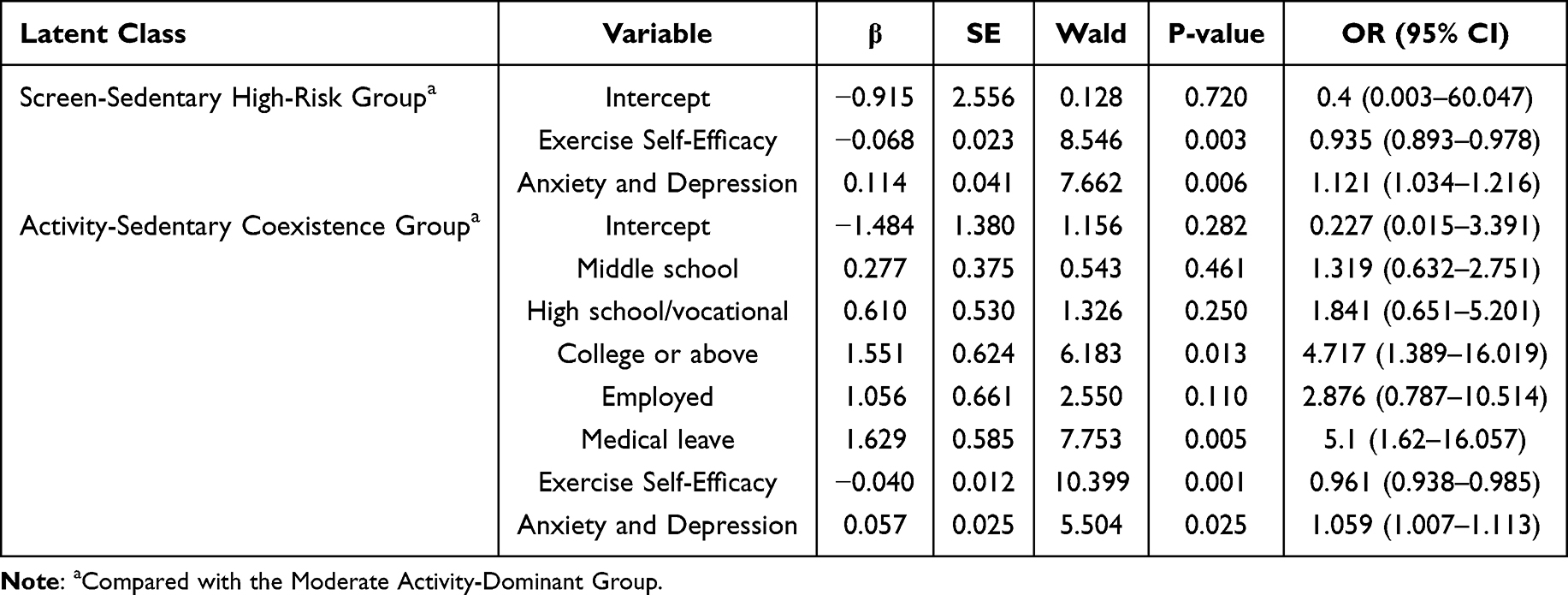 |
Table 5 Multinomial Logistic Regression Analysis of Related Factors |
Discussion
Breast cancer patients in this study generally demonstrated low levels of physical activity. No participants met the criteria for high physical activity. Sedentary behavior was widespread during chemotherapy intervals, with many patients spending prolonged periods sitting each day, especially in screen-based sedentary activities. Latent profile analysis further revealed significant heterogeneity in patients’ activity patterns, which were categorized into three distinct types: Moderate Activity-Dominant Group, Screen-Sedentary High-Risk Group, and Activity-Sedentary Coexistence Group. This classification aligns with the concept of time-use epidemiology, which integrates both sedentary behavior and physical activity throughout the day to provide a more comprehensive understanding of individual behavioral patterns and their health implications.32 Similar heterogeneity in activity patterns has been reported in older adults in Chinese communities, with clusters such as active, moderately active, and sedentary types.33 In comparison, breast cancer patients in this study showed a more pronounced clustering of sedentary behavior, particularly screen-based sitting time, and a clear lack of moderate-to-vigorous physical activity. This may be associated with treatment-related side effects during chemotherapy, as physical discomfort is a common barrier to physical activity among cancer patients.34 Therefore, it is essential for clinicians to closely monitor sedentary behavior in breast cancer patients and implement early identification and targeted interventions based on different activity pattern types. For patients in the Screen-Sedentary High-Risk Group, personalized physical activity plans supported by mobile health technologies may help increase the proportion of moderate-to-vigorous activity and potentially reduce prolonged sedentary behavior. The identification of these three distinct subgroups also provides clinicians with a clearer behavioral framework to guide personalized intervention planning rather than relying on generalized recommendations.
The results of this study showed that patients with a college degree or higher and those on medical leave were more likely to fall into the Activity-Sedentary Coexistence Group. Although individuals in this group engaged in some physical activity, their overall activity levels remained low. Compared with patients with lower education levels, those with higher education were more likely to have sedentary occupations, which is consistent with previous research findings.35 Additionally, individuals with higher education are generally more capable of accessing health-related information and may be more inclined to engage in voluntary physical activity during their leisure time. For patients on medical leave, the absence of work responsibilities may be associated with substantial unstructured time—a situation strongly correlated with increased sedentary behavior, as evidenced by multinational data identifying unemployment as a key sociodemographic factor for high sedentary time.36 However, these patients often have a strong desire for recovery, which may motivate them to participate in therapeutic activities, contributing to the coexistence of both physical activity and prolonged sitting in their daily routines. Therefore, healthcare professionals are advised to provide tailored health education and behavioral guidance for patients classified into the Activity–Sedentary Coexistence Group. Interventions for this subgroup should simultaneously focus on increasing structured moderate-to-vigorous physical activity and reducing prolonged sitting time, rather than targeting either behavior alone. Practical and achievable activity plans can be designed, and wearable devices may be used to monitor daily activity levels, helping patients gradually reduce the health risks associated with prolonged sedentary behavior. This dual-focused approach reflects the behavioral characteristics of the coexistence pattern and offers a more precise basis for designing targeted clinical interventions.
This study found that breast cancer patients with low exercise self-efficacy were more likely to be classified into the Screen-Sedentary High-Risk Group and the Activity-Sedentary Coexistence Group. This finding is consistent with the results of Szczuka et al.37 A possible explanation is that chemotherapy-related side effects—such as changes in body image, reduced social engagement, and increased psychological burden—may hinder patients from gaining a sense of benefit from short-term exercise.38 Notably, exercise self-efficacy showed stronger associations with patients in the Screen-Sedentary High-Risk Group. This suggests that improving exercise self-efficacy may be associated with lower sedentary behavior, particularly screen time, which aligns with previous findings.39 One possible reason is that patients in the Activity-Sedentary Coexistence group already engage in some physical activity, and self-efficacy may be more closely related to maintaining their current activity levels, with weaker associations with reductions in sedentary time. In contrast, those in the Screen-Sedentary High-Risk Group often exhibit low overall motivation for activity and are highly dependent on screen-based sedentary behavior, resulting in significantly higher sedentary durations. In addition, enhancing exercise self-efficacy may be an important correlate of adopting healthier activity patterns. Healthcare providers should work to correct patients’ negative beliefs about physical activity, help them recognize its benefits, and support them in overcoming personal barriers. By strengthening confidence in maintaining regular exercise through targeted behavioral strategies, clinicians may more effectively reduce sedentary behavior—particularly screen-based sitting—among patients with low exercise self-efficacy.
The results of this study indicated that patients with higher scores on the Hospital Anxiety and Depression Scale (HADS) were more likely to be classified into the Screen-Sedentary High-Risk Group and the Activity-Sedentary Coexistence Group. This finding is consistent with existing literature, which has identified anxiety and depression as important correlates of prolonged sedentary behavior.40 Moreover, the associations of anxiety and depression were more pronounced in the Screen-Sedentary High-Risk Group compared to the Activity-Sedentary Coexistence Group. One possible explanation is that breast cancer patients often experience fear of treatment, uncertainty about disease progression, and physiological impairments due to surgery,41 which may reduce their interest in the external environment and be associated with social withdrawal.42 These psychological responses may contribute to patients’ reliance on screen-based sedentary behavior as a way to escape reality and manage emotional discomfort. However, some studies have shown that interrupting sedentary time can help reduce the incidence of anxiety and depression. Even short-term reductions in sedentary behavior and increases in physical activity have been found to improve emotional well-being in cancer patients.43 Therefore, healthcare professionals should ensure that patients are well informed about their diagnosis to help them accept their condition. Regular psychological assessments and emotional support should be integrated into care plans to help patients maintain a positive mental state and reduce their dependence on sedentary coping mechanisms, while also enabling clinicians to identify high-risk individuals early and provide timely intervention.
This study has several limitations. First, the assessment of physical activity and sedentary behavior relied on self-reported questionnaires, which may introduce recall bias and social desirability bias. Second, patients who were unaware of their breast cancer diagnosis were excluded based on clinical communication, which may have led to selection bias. Third, as a cross-sectional study, causal relationships cannot be inferred. Fourth, although a priori sample size considerations were made based on methodological recommendations for latent profile analysis, no formal statistical power calculation was conducted, which may influence the precision of subgroup comparisons. Fifth, some potential confounding factors may not have been fully controlled, despite collecting key demographic and clinical variables. Sixth, the smallest latent class included a limited number of participants, and the sample was drawn from a single geographic region, which may restrict generalizability. Future studies using longitudinal designs, objective measures of physical activity, and larger multi-center samples are warranted to validate these findings.
Conclusion
This study identified three distinct activity pattern subgroups among breast cancer patients during chemotherapy intervals, characterized by overall low-to-moderate physical activity and prolonged sedentary time. The observed associations between education level, employment status, exercise self-efficacy, and anxiety/depression with subgroup membership are consistent with existing evidence and highlight potentially modifiable behavioral and psychological factors. From a clinical perspective, Screen-Sedentary High-Risk patients may benefit from interventions focused on reducing screen-based sedentary time, whereas patients in the Activity–Sedentary Coexistence Group may require a dual emphasis on increasing physical activity and reducing prolonged sitting. Individuals with low exercise self-efficacy may particularly benefit from supportive counseling and strategies that enhance confidence in physical activity participation. Subgroup-specific behavioral pathways and the stability of the three-class latent profile solution should be considered exploratory. Future multi-center longitudinal studies using both subjective and objective measures are needed to validate these findings and further refine subgroup-tailored behavioral interventions.
Ethics Statement
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of The Sixth Affiliated Hospital of South China University of Technology (Approval No: 2023280). The research activities for this study (including patient recruitment and data collection) were primarily carried out at The Sixth Affiliated Hospital of South China University of Technology. Members of our research team were based at this hospital during the study period under a practicum and collaborative research agreement. Written informed consent was obtained from all individual participants included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sha R, Kong XM, Li XY, Wang YB. Global burden of breast cancer and attributable risk factors in 204 countries and territories, from 1990 to 2021: results from the Global Burden of Disease Study 2021. Biomark Res. 2024;12(1):87. doi:10.1186/s40364-024-00631-8
2. Pan XX, Chen MG, Chen W. Analysis of influencing factors of adverse reactions during chemotherapy for breast cancer and traditional Chinese medicine intervention measures. Maternal Child Health Care China. 2024;39(7):1284–12. doi:10.19829/j.zgfybj.issn.1001-4411.2024.07.031
3. Welch WA, Solk P, Auster-Gussman L, et al. Longitudinal sedentary time and symptoms in breast cancer patients during chemotherapy using ecological momentary assessment. Med Sci Sports Exerc. 2023;55(5):966–974. doi:10.1249/MSS.0000000000003115
4. Kim RB, Phillips A, Herrick K, et al. Physical activity and sedentary behavior of cancer survivors and non-cancer individuals: results from a national survey. PLoS One. 2013;8(3):e57598. doi:10.1371/journal.pone.0057598
5. Sabiston CM, Brunet J, Vallance JK, Meterissian S. Prospective examination of objectively assessed physical activity and sedentary time after breast cancer treatment: sitting on the crest of the teachable moment. Cancer Epidemiol Biomarkers Prev. 2014;23(7):1324–1330. doi:10.1158/1055-9965.EPI-13-1179
6. Tremblay MS, Aubert S, Barnes JD, et al. Sedentary Behavior Research Network (SBRN) - Terminology Consensus Project process and outcome. Int J Behav Nutr Phys Act. 2017;14(1):75. doi:10.1186/s12966-017-0525-8
7. Swain CTV, Nguyen NH, Eagles T, et al. Postdiagnosis sedentary behavior and health outcomes in cancer survivors: a systematic review and meta-analysis. Cancer. 2020;126(4):861–869. doi:10.1002/cncr.32578
8. Zainordin NH, Karim NA, Shahril MR, Abd Talib R. Physical activity, sitting time, and quality of life among breast and gynaecology cancer survivors. Asian Pac J Cancer Prev. 2021;22(8):2399–2408. doi:10.31557/APJCP.2021.22.8.2399
9. Yeganeh L, Willey S, Wan CS, et al. The effects of lifestyle and behavioural interventions on cancer recurrence, overall survival and quality of life in breast cancer survivors: a systematic review and network meta-analysis. Maturitas. 2024;185:107977. doi:10.1016/j.maturitas.2024.107977
10. Aune D, Markozannes G, Abar L, et al. Physical activity and health-related quality of life in women with breast cancer: a meta-analysis. JNCI Cancer Spectr. 2022;6(6):pkac072. doi:10.1093/jncics/pkac072
11. de Paula Barbosa K, da Silva LGT, Garcia PA, et al. Effectiveness of Pilates and circuit-based exercise in reducing arthralgia in women during hormone therapy for breast cancer: a randomized, controlled trial. Support Care Cancer. 2021;29(10):6051–6059. doi:10.1007/s00520-021-06180-2
12. Chang Q, Zhu Y, Liu Z, et al. Replacement of sedentary behavior with various physical activities and the risk of all-cause and cause-specific mortality. BMC Med. 2024;22(1):385. doi:10.1186/s12916-024-03599-2
13. Ross R, Chaput JP, Giangregorio LM, et al. Canadian 24-hour movement guidelines for adults aged 18–64 years and adults aged 65 years or older: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. 2020;45(10 (Suppl. 2)):S57–S102. doi:10.1139/apnm-2020-0467
14. Tremblay MS, Carson V, Chaput JP, et al. Canadian 24-hour movement guidelines for children and youth: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. 2016;41(6 Suppl 3):S311–S327. doi:10.1139/apnm-2016-0151
15. Okely AD, Ghersi D, Loughran SP, et al. A collaborative approach to adopting/adapting guidelines. The Australian 24-hour movement guidelines for children (5–12 years) and young people (13–17 years): an integration of physical activity, sedentary behaviour, and sleep. Int J Behav Nutr Phys Act. 2022;19(1):2. doi:10.1186/s12966-021-01236-2
16. Wang J, Wang X. Structural Equation Modeling: Applications Using Mplus.
17. Park S, Park SY, Oh G, Oh IH. Latent profiles based on light physical activity, sedentary behavior, perceived body shape, and body mass index in patients with dyslipidemia influence their quality of life. Int J Environ Res Public Health. 2019;16(20):4034. doi:10.3390/ijerph16204034
18. Zhang L. Exploration of sample size and parameter estimation issues in the application of structural equation modeling. J Sci Technol Educ. 2017;3:75–76. doi:10.16871/i.cnki.kiwhe.201701.034
19. Tian T, Gu BW. Development and reliability-validity test of the Chinese Adult Sedentary Behavior Questionnaire. Chin J Health Educ. 2019;35(6):525–529+45. doi:10.16168/j.cnki.issn.1002-9982.2019.06.010
20. Bandura A. Guide for constructing self-efficacy scales. In: Pajares F, Urdan T, editors. Self-Efficacy Beliefs for Adolescents. Information Age Publishing; 2006:337–377.
21. Li D, Wang YM. Study on exercise self-efficacy scale for community elderly. Nursing Research. 2008;22(8):746–747. doi:10.3969/j.issn.1009-6493.2008.08.054
22. Qu NN, Li KJ. Reliability and validity of the Chinese version of the international physical activity questionnaire. Chin J Epidemiol. 2004;25(3):265–268. doi:10.3760/j.issn:0254-6450.2004.03.021
23. Zimet GD, Powell SS, Farley GK, Werkman S, Berkoff KA. Psychometric characteristics of the multidimensional scale of perceived social support. J Pers Assess. 1990;55(3–4):610–617. doi:10.1080/00223891.1990.9674095
24. Jiang QJ. Perceived social support scale. Chin J Behav Med Sci. 2001;10(10):41–43.
25. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
26. Sun ZX, Liu HX, Jiao LY, et al. Reliability and validity of hospital anxiety and depression scale. Chin J Clin. 2017;11(2):198–201. doi:10.3877/cma.j.issn.1674-0785.2017.02.005
27. Akaike H. A new look at the statistical model identification. IEEE Trans Automat Contr. 1974;19(6):716–723. doi:10.1109/TAC.1974.1100705
28. Dziak JJ, Coffman DL, Lanza ST, Li R, Jermiin LS. Sensitivity and specificity of information criteria. Brief Bioinform. 2020;21(2):553–565. doi:10.1093/bib/bbz016
29. Arminger G, Stein P, Wittenberg J. Mixtures of conditional mean-and covariance-structure models. Psychometrika. 1999;64(4):475–494. doi:10.1007/BF02294568
30. Nylund-Gibson K, Asparouhov T, Muthén B. Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo Simulation Study. Struct Equ Model. 2007;14:535–569. doi:10.1080/10705510701575396
31. Tein JY, Coxe S, Cham H. Statistical power to detect the correct number of classes in latent profile analysis. Struct Equ Model. 2013;20(4):640–657. doi:10.1080/10705511.2013.824781
32. Song JC, Li HJ, Wang ZS. Application of time-use epidemiology in the field of physical activity research. China Sport Sci. 2020;40(1):79–88. doi:10.16469/j.css.202001008
33. Lu Y, Jiang Y, Chu AQ, et al. Latent classes of activity patterns and their relationship with cognitive function in community-dwelling older adults. J Nurs Sci. 2023;38(7):101–105. doi:10.3870/j.issn.1001-4152.2023.07.101
34. Lavallée JF, Abdin S, Faulkner J, Husted M. Barriers and facilitators to participating in physical activity for adults with breast cancer receiving adjuvant treatment: a qualitative metasynthesis. Psychooncology. 2019;28(3):468–476. doi:10.1002/pon.4980
35. Yao P, Zhong Y, Wei Z. Association between sedentary behavior, depressive symptoms, and the risk of all-cause and cause-specific mortality among U.S. cancer survivors. BMC Cancer. 2025;25(1):570. doi:10.1186/s12885-025-13578-2
36. Koyanagi A, Stubbs B, Vancampfort D. Correlates of sedentary behavior in the general population: a cross-sectional study using nationally representative data from six low- and middle-income countries. PLoS One. 2018;13(8):e0202222. doi:10.1371/journal.pone.0202222
37. Szczuka Z, Banik A, Abraham C, Kulis E, Luszczynska A. Associations between self-efficacy and sedentary behaviour: a meta-analysis. Psychol Health. 2021;36(3):271–289. doi:10.1080/08870446.2020.1784419
38. Compernolle S, De Cocker K, Cardon G, De Bourdeaudhuij I, Van Dyck D. Older adults’ perceptions of sedentary behavior: a systematic review and thematic synthesis of qualitative studies. Gerontologist. 2020;60(8):572–582. doi:10.1093/geront/gnz127
39. Yang Y, Jia W, Wu K, Xu L, Jiao Y. Factors associated with sedentary behavior among breast cancer patients during chemotherapy: a cross-sectional study based on COM-B model. Medicine. 2025;104(33):e43948. doi:10.1097/MD.0000000000043948
40. Stubbs B, Vancampfort D, Firth J, et al. Relationship between sedentary behavior and depression: a mediation analysis of influential factors across the lifespan among 42,469 people in low- and middle-income countries. J Affect Disord. 2018;229:231–238. doi:10.1016/j.jad.2017.12.104
41. Paolucci T, Bernetti A, Paoloni M, et al. Therapeutic alliance in a single versus group rehabilitative setting after breast cancer surgery: psychological profile and performance rehabilitation. Biores Open Access. 2019;8(1):101–110. doi:10.1089/biores.2019.0011
42. Jin HY, Zhang XJ, Fang Q, et al. Status and influencing factors of social avoidance and distress in patients after breast cancer surgery. Maternal Child Health Care China. 2021;36(7):1613–1616. doi:10.19829/j.zgfybj.issn.1001-4411.2021.07.048
43. Kindred MM, Pinto BM, Dunsiger SI. Predictors of sedentary behavior among colorectal survivors. Support Care Cancer. 2019;27(6):2049–2056. doi:10.1007/s00520-018-4452-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.