Back to Journals » Medical Devices: Evidence and Research » Volume 18
Late-Onset Isolated Vitreous Hemorrhage After Micropulse Transscleral Cyclophotocoagulation: A Case Report and Insights for a Rare Complication
Authors Shihadeh W, Aleshawi A, Aburamadan Y, Al-Shalakhti M, Abu Najm A ![]() , Ibrahim AY
, Ibrahim AY
Received 3 July 2025
Accepted for publication 17 September 2025
Published 11 October 2025 Volume 2025:18 Pages 519—524
DOI https://doi.org/10.2147/MDER.S551399
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Wisam Shihadeh,1 Abdelwahab Aleshawi,1 Yara Aburamadan,2 Mohammed Al-Shalakhti,3 Amr Abu Najm,1 Ala’ Y’ Ibrahim3
1Division of Ophthalmology, Department of Special Surgery, Faculty of Medicine, Jordan University of Science and Technology, Irbid, 22110, Jordan; 2University College London, Hospital NHS Trust, London, UK; 3Faculty of Medicine, Yarmouk University, Irbid, 21163, Jordan
Correspondence: Wisam Shihadeh, Division of Ophthalmology, Department of Special Surgery, Faculty of Medicine Jordan University of Science and Technology, P. O. Box: 3030, Irbid, 22110, Jordan, Tel +962 79 5821582, Email [email protected]
Background: Micropulse transscleral diode cyclophotocoagulation (MP-TSCPC) has been developed as an alternative and safer approach to cyclodestructive procedures. While MP-TSCPC has an improved safety profile, reported complications of this procedure, though uncommon, include anterior chamber inflammation, mydriasis, hypotony, macular edema, corneal edema, phthisis bulbi, vitreous hemorrhage (VH), and conjunctival hemorrhage.
Case Presentation: We report a case of a 76-year-old male who underwent uneventful MP-TSCPC for the left eye due to moderate primary-open angle glaucoma. A few days following the procedure, dense VH developed without hyphema or suprachoroidal hemorrhage. The VH persisted despite observation, and pars plana vitrectomy was performed, the patient recovered quickly, and achieved a visual acuity of 6/12 with an intraocular pressure of 10 mmHg.
Conclusion: MP-TSCPC is considered a safe and effective procedure in glaucoma management. However, the treating ophthalmologist should always be aware of rare but potentially serious complications. In our case report, we report a case of dense VH without hyphema or suprachoroidal hemorrhage following MP-TSCPC.
Keywords: micropulse transscleral diode cyclophotocoagulation, vitreous hemorrhage, glaucoma, intraocular pressure
Introduction
Traditional transscleral diode cyclophotocoagulation (TSCPC), or continuous wave transscleral diode cyclophotocoagulation (CW-TSCPC), has been widely utilized since its production during the end of the past century. In this procedure, the pigmented epithelium layer of the ciliary body is targeted by a diode laser to destroy this structure and thus decrease production of aqueous humor.1–3 However, the continuous mode adopted in the CW-TSCPC can result in considerable ocular tissue damage, which leads to several complications, such as chronic hypotony, choroidal detachment, uveitis, phthisis bulbi, and sympathetic ophthalmia. Accordingly, micropulse transscleral diode cyclophotocoagulation (MP-TSCPC) has therefore been introduced as a safer alternative.4 The principle of MP-TSCPC is focused on directing the laser energy at the pars plana in repetitive, short pulses separated by cooling periods. It is theorized that the cooling periods allow the ocular tissues to scatter heat energy, thus preventing them from reaching coagulative threshold, with subsequent minimization of the ocular tissue damage and much less reported complications.5 Recent cadaveric investigations revealed that MP-TSCPC caused less tissue disruption to the ciliary body compared with CW-TSCPC treatments.6 The most commonly reported adverse effects after MP-TSCPC are mild and transient. They include anterior chamber reaction, pain, transient spikes in intraocular pressure (IOP), and corneal edema. Rare instances of persistent hypotony, choroidal detachment, permanent vision loss, and phthisis bulbi have been reported2 Vitreous hemorrhage post- MP-TSCPC is a rare complication and only reported three times previously.7,8 In this case, we report the development of vitreous hemorrhage (VH) after MP-TSCPC.
Case Presentation
A 76-year-old male, not known to have any medical illness, presented to our service with advanced primary open-angle glaucoma (POAG) in the right eye and moderate POAG in the left eye. Both eyes were uncontrolled by maximum tolerated medical therapy (including dorzolamide/timolol twice a day, brimonidine three times a day, and bimatoprost once a day). The patient has no history of anticoagulant use, hypertension, diabetes mellitus, cardiovascular diseases, other atherosclerotic diseases, ocular trauma, previous ocular surgery, or previous history of choroidal hemorrhage. The best-corrected visual acuity was 6/24 in both eyes, and the IOP was 32 mmHg in the right eye and 24 mmHg in the left. Anterior segment exam showed bilateral nuclear sclerosis. The posterior segment was unremarkable in both eyes apart from optic disc cupping which was more advanced in the right eye. The axial length was within the normal range. Ahmed glaucoma drainage device was implanted in the right eye successfully. The postoperative course was uneventful, and the IOP was controlled thereafter in the low teens. Uneventful MP-TSCPC under peribulbar anesthesia (using a combination of lidocaine and bupivacaine) was performed in the left eye using a MicroPulse P3 probe (utilizing the wavelength of 810 nm) with the Iridex Cyclo® G6 (IRIDEX, Mountain View, CA, USA) under the following settings: 2500mW× 80s ×31.3% duty cycle/ hemisphere.
In the first week after the procedure, the patient exhibited deterioration of visual acuity associated with pain in the left eye. The examination revealed a best-corrected visual acuity of counting fingers at 1-meter, low IOP (4 mmHg), severe +3 anterior chamber reaction with pupillary membrane, and serous choroidal effusion (Figure 1). The patient commenced on intense topical prednisolone eye drops and cycloplegic agents. The patient improved gradually over two weeks; the anterior chamber reaction and choroidal effusion were resolved and IOP built up to 10 mmHg. One week later (4 weeks from the MP-TSCPC), the vision dropped suddenly to hand motion, and the dilated fundus examination revealed dense VH with no evidence of retinal detachment or choroidal hemorrhage on B scan (Figure 2). This VH persisted and showed no improvement over the period of one month of observation. Accordingly, the patient underwent pars plana vitrectomy to treat the non-clearing VH. A standard uneventful 3-port 25G pars plana vitrectomy with phacoemulsification and posterior chamber intraocular lens implant were performed. There were no retinal breaks or detachments identified intraoperatively. The visual acuity recovered to 6/12 after surgery with IOP around 10 mmHg over the follow-up period.
 |
Figure 1 B-scan one week after the procedure revealing serous choroidal effusions (red star). |
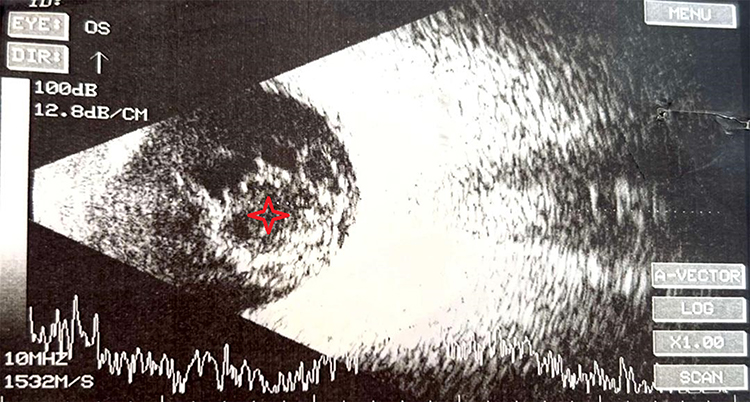 |
Figure 2 B scan four weeks after the procedure showing dense VH (red star). |
Discussion
To the best of our knowledge, this is the first report of late-onset isolated VH (without hyphema or choroidal hemorrhage) following MP-TSCPC. Three previous cases of VH following MP-TSCPC with different scenarios were reported in the literature. Aldaas et al report a case of choroidal hemorrhage and VH after MP-TSCPC in a myopic 82-year-old female who presented with blurry vision and pain in her right eye one day after MP-TSCPC and was found to have VH and choroidal hemorrhage.7 Although the choroidal hemorrhage resolved with steroids, the VH required pars plana vitrectomy.7 Shah et al reported two cases of hyphema and VH after the application of MP-TSCPC. The first case was a myopic 82-year-old woman with bilateral severe POAG for which she underwent MP-TSCPC of the right eye and at one week, a settled 2 mm hyphema and VH confirmed by B-scan were noted. At three months, the patient had a reasonable visual acuity, IOP of 12 mmHg and resolving VH, and the retina consultation deferred any surgical intervention.8 The second case was a patient with bilateral moderate-stage POAG who underwent MP-TSCPC in both eyes. At 2 weeks, the visual acuity of the right eye was counting fingers at one foot, IOP was 11 mmHg, and B scan revealed dense VH. The VH resolved spontaneously and, pars plana vitrectomy was not needed.8 Table 1 summarizes the 4 cases of VH after MP-TSCPC.
 |
Table 1 Summary for Cases of VH After MP-TSCPC |
While MP-TSCPC has an improved side effect profile when compared to CW-TSCPC, complications of this procedure have not been well established. The most common complications noted are anterior chamber inflammation, mydriasis, hypotony, macular edema, loss of visual acuity, corneal edema, phthisis bulbi, superficial punctate keratitis, and conjunctival hemorrhage in no particular order.3 VH is a rare postoperative complication of non-incisional ciliary ablation surgeries, and VH after MP-TSCPC procedures typically does not occur in isolation and, instead, has been associated with coexisting suprachoroidal hemorrhage or hyphema.7 Chen et al conducted a study on 60 eyes of Taiwanese patients who underwent MP-TSCPC, and none of the eyes developed VH.4 Moreover, Varikuti et al studied the outcomes of MP-TSCPC on 61 eyes and they reported no VH in any of the cases.9 Furthermore, Murtaza et al investigated the effect of MP-TSCPC on 115 eyes, and they also reported no VH in their study.3 Risk factors have been identified and these include high myopia, aphakia, vitrectomized eyes, high preoperative IOP, sudden reduction in IOP, and postoperative hypotony. Furthermore, systemic hypertension, preoperative anticoagulation use, atherosclerotic diseases were also significant systemic risk factors.10–12 The delayed hemorrhagic complications following glaucoma procedures typically occur days following the procedure in comparison to the intraoperative nature of the early type.13
Theories that may explain the development and pathophysiology of VH after the CW-TSCPC include direct trauma of the diode laser energy in the ciliary body and the pars plana.14 However, theories that may explain VH after MP-TSCPC may include rupturing or leaking of blood due to sudden variations in IOP that compress or decompress these vessels. In our patient, post-procedure hypotony may be a contributing factor in the development of VH, as the IOP dropped to 4 mmHg after the procedure. Other risk factors13 such as the use of anticoagulant, uncontrolled hypertension, atherosclerosis, high myopia, aphakia or pseudophakia, previous ocular trauma, previous intraocular surgery, and a previous history of choroidal hemorrhage, were not reported in our patient. Certain maneuvers, such as excessive pressure on the globe during surgery and retrobulbar anesthetic injections, may obstruct vortex venous and contribute to the development of VH.7 The decision was to proceed with pars plana vitrectomy to clear the VH as persistent VH has many clinical implications. Persistent non-clearing VH can contribute to more advanced glaucoma, proliferative vitreoretinopathy, obscuring the underlying pathology, and hemosiderosis bulb.15 Limitations to this study include being a single-patient case report and the absence of some perioperative details.
In conclusion, MP-TSCPC is considered a proper alternative procedure to CW-TSCPC as reported in many articles in the literature. However, MP-TSCPC is not without complications, and certain serious complications in a susceptible patient may develop. Accordingly, comprehensive medical and ocular history should be taken, adequate ocular examination should be performed, and risk factors for these complications should be adjusted. In our case report, we report the first case of severe uveitis and dense VH following MP-TSCPC. Further studies may be necessitated to understand the mechanisms of VH following MP-TSCPC.
Abbreviations
TSCPC, Traditional transscleral diode cyclophotocoagulation; CW-TSCPC, continuous wave transscleral diode cyclophotocoagulation; MP-TSCPC, Micropulse transscleral diode cyclophotocoagulation; VH, vitreous hemorrhage; POAG, primary open angle glaucoma; IOP, intraocular pressure.
Data Sharing Statement
Data sharing does not apply to this article as no datasets were generated or analyzed during the current study.
Ethics Approval and Consent to Participate
Institutional Review Board (IRB) approval was waived according to policies for single‑patient case reports.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report. A copy of the written consent is available for review by the Editor of this journal.
Funding
No funding was received.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Balbaid N, AlJodai M, Fairaq G, AlEnzi M, AlShahwan S. Micropulse transscleral cyclophotocoagulation (MP-CPC): efficacy endpoints for the treatment of refractory paediatric glaucoma - a retrospective case-series. BMC Ophthalmol. 2024;24(1):91. doi:10.1186/s12886-024-03358-0
2. Szilagyi Z, Kranitz K, Nagy ZZ, Recsan Z. Micropulse Transscleral Cyclophotocoagulation Results in Secondary Glaucoma. Life. 2023;13(5):1149. doi:10.3390/life13051149
3. Murtaza F, Kaba Q, Somani S, Tam ES, Yuen D. Micropulse Transscleral Cyclophotocoagulation in Non-Incisional Eyes with Ocular Hypertension and Primary Open-Angle Glaucoma. Clin Ophthalmol. 2024;18:1295–1312. doi:10.2147/OPTH.S447875
4. Chen HS-L, Yeh P-H, Yeh C-T, et al. Micropulse transscleral cyclophotocoagulation in a Taiwanese population: 2-year clinical outcomes and prognostic factors. Graefes Arch Clin Exp Ophthalmol. 2022;260(4):1265–1273. doi:10.1007/s00417-021-05468-7
5. Kelada M, Normando EM, Cordeiro FM, et al. Cyclodiode vs micropulse transscleral laser treatment. Eye. 2024;38(8):1477–1484. doi:10.1038/s41433-024-02929-1
6. Maslin JS, Chen PP, Sinard J, Nguyen AT, Noecker R. Histopathologic changes in cadaver eyes after MicroPulse and continuous wave transscleral cyclophotocoagulation. Can J Ophthalmol. 2020;55(4):330–335. doi:10.1016/j.jcjo.2020.03.010
7. Aldaas KM, Brasington C, Zhang AY. A Case of Choroidal and Vitreous Hemorrhage Following Micropulse Transscleral Cyclophotocoagulation. J Glaucoma. 2020;29(7):e57–e59. doi:10.1097/IJG.0000000000001529
8. Shah MK, Syal S, Desai RU, Khouri AS. Hyphema and vitreous hemorrhage after micropulse cyclophotocoagulation a case report. Eur J Ophthalmol. 2024;34(4):NP16–NP19. doi:10.1177/11206721241240505
9. Varikuti VNV, Shah P, Rai O, et al. Outcomes of Micropulse Transscleral Cyclophotocoagulation in Eyes With Good Central Vision. J Glaucoma. 2019;28(10):901–905. doi:10.1097/IJG.0000000000001339
10. Jeganathan VS, Ghosh S, Ruddle JB, Gupta V, Coote MA, Crowston JG. Risk factors for delayed suprachoroidal haemorrhage following glaucoma surgery. Br J Ophthalmol. 2008;92(10):1393–1396. doi:10.1136/bjo.2008.141689
11. Tuli SS, WuDunn D, Ciulla TA, Cantor LB. Delayed suprachoroidal hemorrhage after glaucoma filtration procedures. Ophthalmology. 2001;108(10):1808–1811. doi:10.1016/S0161-6420(01)00763-1
12. Chak M, Williamson TH. Spontaneous suprachoroidal haemorrhage associated with high myopia and aspirin. Eye. 2003;17(4):525–527. doi:10.1038/sj.eye.6700388
13. Chu TG, Green RL. Suprachoroidal hemorrhage. Surv Ophthalmol. 1999;43(6):471–486. doi:10.1016/S0039-6257(99)00037-5
14. Prager AJ, Anchala AR. Suprachoroidal hemorrhage after micropulse cyclophotocoagulation diode therapy. Am J Ophthalmol Case Rep. 2020;18:100659. doi:10.1016/j.ajoc.2020.100659
15. Shaikh N, Srishti R, Khanum A, et al. Vitreous hemorrhage - Causes, diagnosis, and management. Ind J Ophthalmol. 2023;71(1):28–38. doi:10.4103/ijo.IJO_928_22
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.