Back to Journals » Clinical Ophthalmology » Volume 14
Laser-Assisted Adjustable Suture Technique in Strabismus Surgery
Authors Hannon AA, Elalfy M, Elborgy ES, Hegazy SM ![]()
Received 13 September 2020
Accepted for publication 10 November 2020
Published 11 December 2020 Volume 2020:14 Pages 4347—4354
DOI https://doi.org/10.2147/OPTH.S281756
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ahmed A Hannon,1 Mohamed Elalfy,2 Ebrahim S Elborgy,3 Sherif M Hegazy3
1Pediatric Ophthalmology and Strabismology Department, Research Institute of Ophthalmology, Cairo, Egypt; 2Cornea and Refractive Department, Research Institute of Ophthalmology, Cairo, Egypt & Queen Victoria Hospital, West Sussex, UK; 3Retina Department, Research Institute of Ophthalmology, Cairo, Egypt
Correspondence: Ahmed A Hannon
Pediatric Ophthalmology and Strabismology Department, Research Institute of Ophthalmology, Cairo, Egypt
Tel +201000101743
Email [email protected]
Purpose: The aim of this study was to assess the efficacy and safety of a new technique (argon laser-assisted lysis of the adjustable suture) in strabismus surgery.
Patients and Methods: Recession of lateral rectus muscle was done and was secured to the sclera at the predetermined recession position after suspending it 1.5– 2.5 mm farther. A 10-0 nylon suture was placed at the original insertion site, passed under the previously tied muscle suture knot, and tied, advancing the muscle to the new scleral insertion. Postoperatively in the same day of surgery, if the targeted slight overcorrection was not achieved, a topical anesthetic was given, and argon laser was used to cut the nylon suture providing additional muscle recession.
Results: Forty-two patients with exotropia were included: 11 children and 31 adults. Eleven (26.2%) patients became orthophoric immediately following muscle recession. Thirty-one (73.8%) patients were undercorrected with a mean residual angle of 8.2± 3.3 pd. After laser-assisted release of the suture, 12 (28.6%) patients were orthophoric, with 4 (9.5%) patients still undercorrected and 26 (61.9%) patients overcorrected. By the end of 6 months postoperatively, the overall success rate of the procedure was 88.1%, with only 5 (11.9%) patients with exotropia.
Conclusion: The laser-assisted adjustable suture technique had an overall success rate of 88.1% with only 11.9% of the patients showing exotropia. The technique can help achieve successful alignment.
Keywords: recession, laser-assisted adjustable suture, strabismus, lateral rectus muscle
Introduction
Exotropia is a common form of strabismus, with an incidence of 1% in the general population.1 Treatment of exotropia entails either conservative measures or operative correction. When conservative measures fail to correct the condition, lateral rectus recession and/or medial rectus resection constitute the definitive treatment.2
Lateral rectus recession is a procedure that has demonstrated varying rates of success, ranging from 66% for bilateral lateral rectus recession to 79.5% for unilateral recession resection.3 Meanwhile, considerable percentages of patients may either suffer from residual exotropia (undercorrection) or have some degree of esotropia (overcorrection), requiring reoperation.2
To overcome this complication, adjustable sutures can be applied immediately following muscle resection/recession to enable the surgeon achieving accurate alignment.4,5
Many techniques were described for adjustable sutures including bow tie6 and sliding noose7 techniques. These techniques carry several drawbacks including unequal length of muscle sutures after retying, non-quantitative amount of adjustment, and inability to interrupt the procedure upon demand of the anesthesiologist,8 slippage of the muscle, the need for more manipulations to locate the suture during adjustment, and increased incidence of suture granulomas.7
The current study endeavored to introduce a new technique that may avoid the drawbacks of the aforementioned adjustable suture techniques. The aim of this work was to assess the efficacy and safety of argon laser-assisted lysis of the adjustable suture in strabismus surgery.
Patients and Methods
Ethical Considerations
The study obtained approval from the Ethics Committee of the Research Institute of Ophthalmology, Cairo, Egypt, and was conducted in accordance with the Declaration of Helsinki. Patients and/or their parents were informed about the surgical procedure and the possibility of postoperative suture lysis in the clinic, and informed consent was obtained prior to study commencement.
We intend to share the individual de-identified participants’ data. Data will be accessible through direct contact with the corresponding author, beginning 12 months and ending 36 months following article publication.
Eligibility Criteria
This study was conducted between November 2018 and October 2019. The study included patients of both genders (17 males and 25 females), aged ≥10 years, with intermittent exotropia (basic type) who had no previous strabismus surgery. Patients with other types of intermittent exotropia and those who had any previous strabismus surgery were excluded.
Technique
All lateral recti muscles were recessed through fornix incision; muscles were recessed using the following adjustable technique.
The lateral rectus muscle was isolated. A double-armed 6-0 polyglactin (Vicryl; Ethicon Inc, Pasadena, CA) was passed and locked to the muscle 1.5 to 2.00 mm from the insertion. The muscle was disinserted. A previously set caliper to the planned amount of recession was used to mark the entrance points for the scleral tunnels. The entry marks were made one muscle width apart and the sutures were placed through 3-mm scleral tunnels to emerge near to one another in a parallel configuration to the insertion plane. The caliper was reset to 2 mm. The suture arms were pulled up, measured for the 2-mm caliper distance, tied, and trimmed as in the hang-back technique leaving the muscle hanging back 2 mm behind the new insertion site.
Similar to the technique that has been first described by Coats,9 a needle of single-armed 10-0 nylon suture was passed under the previously tied muscle suture, knot then passed through the sclera anterior and parallel to the insertion line. Then, the ends of this suture were tied together. As this suture was tightened, the muscle crept anteriorly to the new scleral insertion. After tightening the nylon suture, the muscle crept anteriorly to the new scleral insertion. The two ends of the 10-0 nylon suture were trimmed and buried in the sclera. Two more 10-0 nylon sutures were passed under the muscle suture knot; then passed through the sclera, tightened, trimmed, and buried in the same way. The conjunctiva was closed with 6-0 vicryl.
On planning for muscle recession, we aimed at a small postoperative under correction because the releasable suture is not helpful in postoperative overcorrection. The millimeters of recession for a specific target angle were determined from a standard chart.
Postoperatively, on the same day, the assessment was done using an alternate prism cover test. If alignment was satisfactory, the sutures were left in place. If more recession was needed, the nylon sutures were cut using argon laser and the muscle slid back, producing an additional recession of 2 mm (Figure 1).
 |
Figure 1 Laser-assisted adjustable Lateral rectus recession (for example 6 mm): (A) After suturing the muscle to the sclera according to the planned amount of recession (6 mm), the suture arms were pulled up, measured for 2-mm caliper distance, tied, and trimmed as in hang-back technique leaving the muscle hanging back 2 mm behind the new insertion site. (B) A needle of single-armed 10-0 nylon suture was passed under the previously tied muscle suture knot; then, passed through the sclera anterior and parallel to the insertion line. (C) After tightening the nylon suture, the muscle crept anteriorly to the new scleral insertion. The two ends of the 10-0 nylon suture were trimmed and buried in the sclera. (D) If more recession was needed, the nylon sutures were cut using argon laser and the muscle slid back, producing an additional recession of 2 mm. |
The target postoperative angle was defined according to previous studies as slight overcorrection not exceeding 10 pd.10,11 Previous studies reported that slight postoperative overcorrection was associated with long-term favorable outcomes11–13 and recommended aiming for some overcorrection.6,15,16
The argon laser settings were a 50-um spot size, duration of 0.1 second, and a power setting between 0.450 and 0–600 W. A Hoskins lens was used in each case.
All patients were followed up regularly for 6 months after surgery. Successful outcome was defined as distance ocular alignment from 0 to 10 pd at 6 months postoperatively.
Statistical Analysis
Statistical analysis was conducted using Statistical Package for Social Sciences, version 26. Numerical variables were expressed as mean±standard deviation (SD), and comparison between groups was performed using either independent samples T-test (for two unpaired groups) or repeated measures ANOVA (for more than two paired groups). Categorical variables were summarized as frequencies (counts) and percentages. Association between two categorical variables was done using Fisher’s exact test (instead of Pearson’s Chi square test) as more than 20% of the cells had expected count less than 5. Significance was adopted at p≤0.05.
Results
The present study included 42 patients: 11 children and 31 adults. The mean age of participants was 27±11.4 years old. The mean preoperative angle was 37.0±7.9 pd, ranging from 25 to 50 pd. Adjustment of lateral rectus was carried out bilaterally in 21 patients (50%), whereas the adjustment was performed on the left side in 10 patients (23.8%) and on the right side in 11 patients (26.2%). The mean amount of lateral recti recession was 7.1±1.2 mm (Table 1).
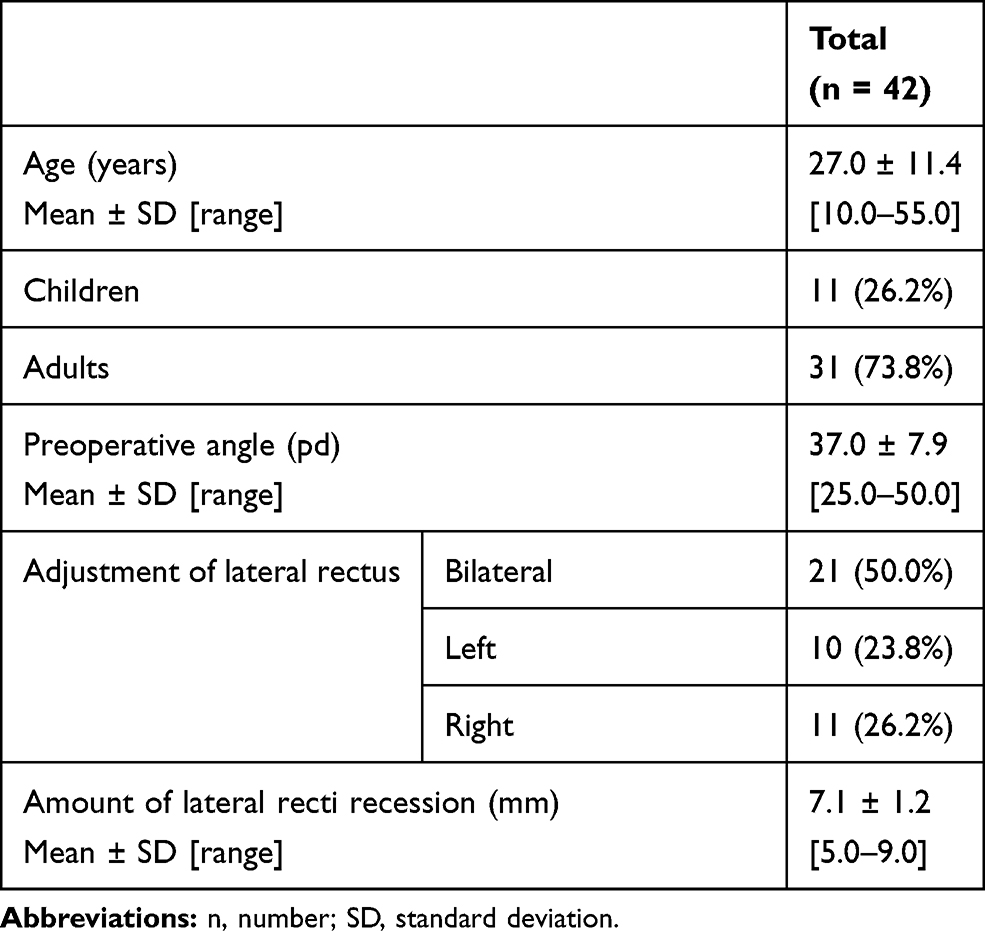 |
Table 1 Preoperative and Operative Data of the Studied Patients (Total n = 42) |
Following muscle recession and before adjustment, eleven (26.2%) patients became orthophoric, they all underwent unilateral laser adjustment to make them towards the esotropia side, post adjustment and in the first day they were all esotropic but they became all orthophoric by the sixth month of follow-up. Before adjustment, 31 (73.8%) patients still had some degree of exotropic deviation (undercorrected), with a mean immediate postoperative exodeviation angle of 8.2±3.3 pd (ranging from 2 to 18; Table 2). They underwent either unilateral (10 cases) or bilateral (21 cases) adjustment. Post adjustment, 12 cases were orthophoric, 15 cases were esotropic, and only 4 cases continued to be exotropic in the first day post adjustment. These four cases were found to be exotropic by the end of the sixth month.
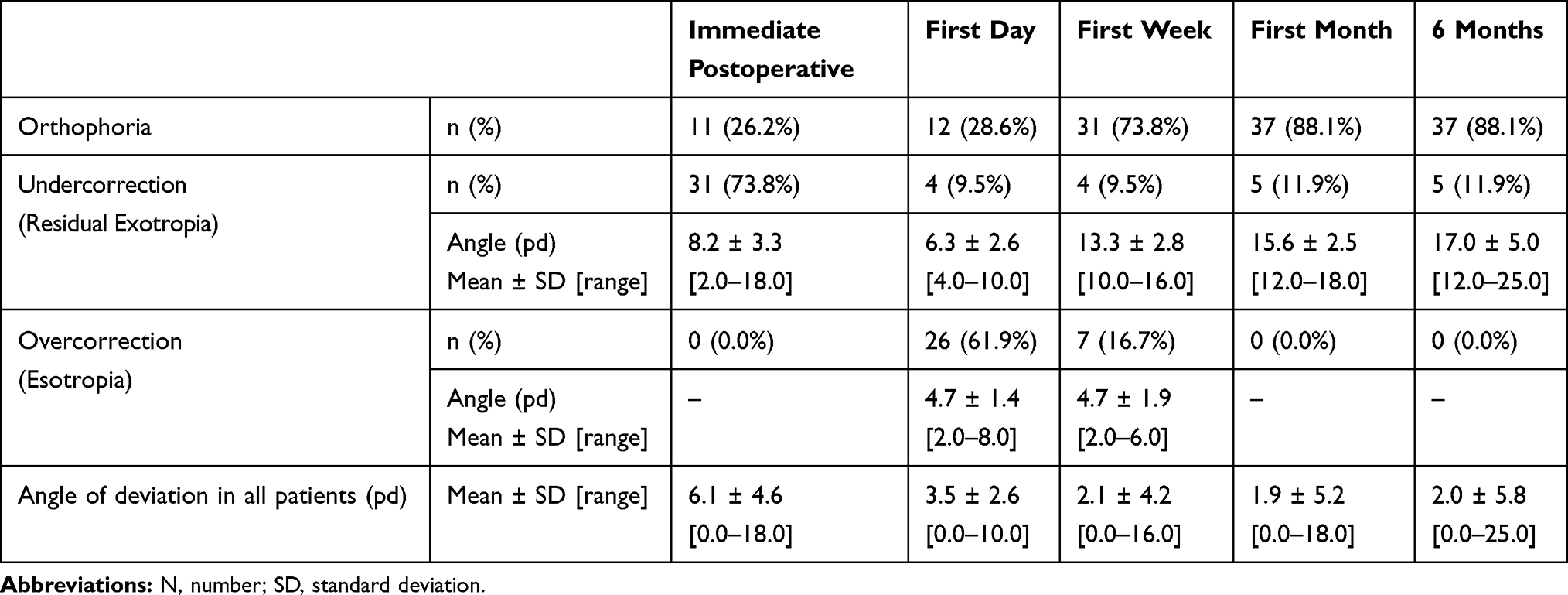 |
Table 2 Postoperative Adjustment Angle, Follow-Up and Success Rate in the Studied Patients (Total n = 42) |
Following adjustment of all cases including the orthophoric ones and on the first postoperative day, 12 (28.6%) patients were orthophoric. Residual exotropia was still recorded in four (9.5%) cases, with a mean residual angle of 6.3±2.6 pd. The targeted slight esotropia (overcorrection) was observed in 26 (61.9%) patients, with a mean angle of 4.7±1.4 pd (ranging from 2 to 8 pd). The angle of deviation was 10 pd or less in all patients, with a mean overall angle of 3.5±2.6 pd (ranging from 0 to 10 pd; Table 2).
At the first postoperative week, 31 (73.8%) patients were orthophoric. Residual exotropic drift was still present in the four (9.5%) cases, with increased mean angle (13.3±2.8 pd). Esotropia was observed in seven (16.7%) patients, with a mean residual angle of 4.7±1.4 pd. The mean overall angle of deviation was 2.1±4.2 pd (ranging from 0 to 16 pd; Table 2).
At the first postoperative month, 37 (88.1%) patients were orthophoric. Residual exotropia was still present in the four cases mentioned before plus one orthophoric case who became exotropic (11.9%), with a mean angle of 15.6±2.5 pd (ranging from 12 to 18 pd). The mean overall angle of deviation of 1.9±5.2 pd (ranging from 0 to 18 pd; Table 2).
At the end of the sixth month postoperatively, the five cases recorded at the end of the first month still suffered from exotropic drift, with a mean angle of exotropic deviation of 17.0±5.0 pd (ranging from 12 to 25 pd). None of the patients had overcorrection (esotropic drift). The percentage of patients with successful correction (angle of deviation ≤10 pd) was 88.1%. The overall mean angle of deviation was 2.0±5.8 pd (ranging from 0 to 25 pd; Table 2).
Repeated measures ANOVA was carried out and revealed that the mean angle of strabismus decreased significantly (p<0.001) postoperatively before adjustment compared to the preoperative level. Further, significant decrease was observed also on the first postoperative day after adjustment compared with immediate postoperative measurement (p=0.034). Further, later changes in angle measurements were non-significant (p>0.05; Figure 2).
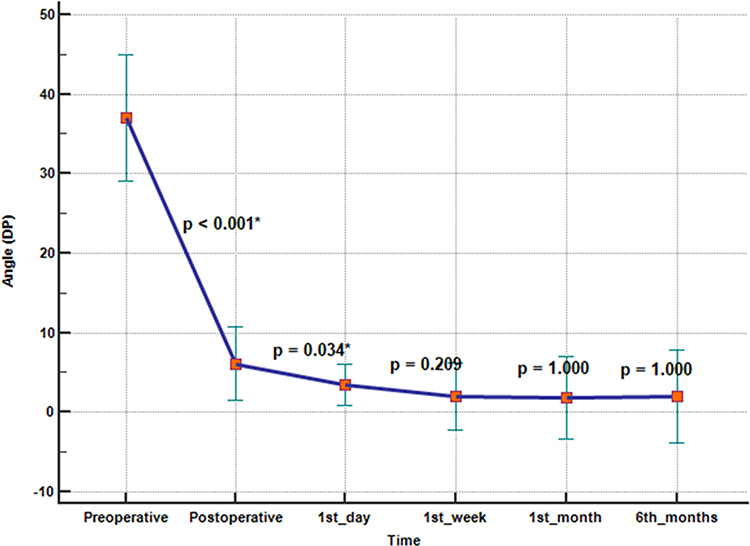 |
Figure 2 Changes in angle (pd) in the studied patients during the study period (*significant at p ≤ 0.05). |
Patients with successful outcome at 6 months postoperatively and the five failed cases were compared according to potential factors that may affect the outcome. Though the percentage of children in the failed group was higher than in the success group (40% vs 24.3%), this difference did not reach statistical significance (p=0.593). Patients who experienced failure of the procedure had significantly higher mean preoperative angle of deviation (47.0±4.5 vs 35.7±7.3 pd; p=0.002), longer mean amount of lateral rectus recession (8.4±0.9 vs 6.9±1.2 mm; p=0.009), higher mean immediate postoperative angle (13.4±3.1 vs 5.1±3.8 pd; p<0.001), and they all underwent bilateral adjustment (p=0.048; Table 3).
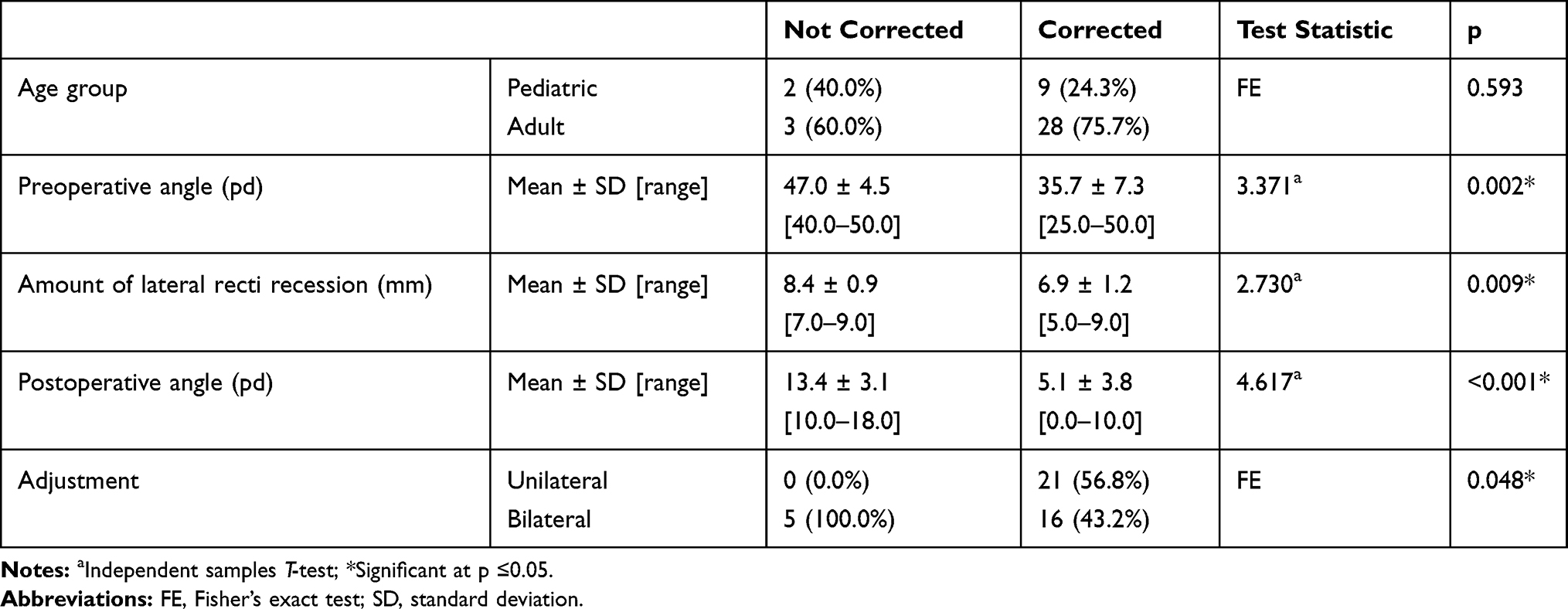 |
Table 3 Analysis of Potential Factors Affecting Success Rate of Adjustable Suture at 6 Months Postoperative (Total n = 42) |
None of the patients was lost to follow-up during the study period and no major complications were recorded.
Discussion
One of the most common complications for patients undergoing strabismus surgeries is inappropriate correction, whether over- or undercorrections. To overcome this complication, a variety of methods can be employed, including the use of adjustable suture. The aim of the present study was to assess the efficacy and safety of a new technique (argon laser-assisted lysis of the adjustable suture) in strabismus surgery. Up to the best of the authors’ knowledge, the use of argon laser in adjustable suture technique following strabismus surgery has not been described before in the literature.
The new technique described in the current study attempted to avoid the limitations of commonly used adjustable suture techniques, such as the bowtie, sliding noose, and ripcord. Lysis of the sutures using argon laser was achieved through the generation of heat, resulting in cutting of the suture. The use of argon laser for lysis of sutures does not require learning new operative skills by ophthalmologists. Moreover, the new technique involves placing the suture just anterior and parallel to the original insertion. From our point of view, placing the second traction suture inferior to the plane of the muscle and keeping it exposed as described by Coats9 to facilitate surgical cutting of the second suture using a sharp object could produce a rotational effect when the rectus muscle contracts; therefore, it is more functionally acceptable to place the suture at the same muscle plane.
After muscle recession and before adjustment, 26.2% of patients in our series became orthophoric, while73.8% still had some degree of exotropic deviation. After adjustment, we aimed at a small postoperative overcorrection. Therefore, all patients in our series, including those who were orthophoric after strabismus surgery, were subjected to adjustment to attain slight overcorrection not exceeding 10 pd.
We performed adjustment on the same day of surgery in our series of patients. Several previous studies recommended adjustment within the immediate postoperative period to prevent the development of potential complications, such as healing of the conjunctiva or adherence of the muscle to the sclera.5,17–20 Nevertheless, Agrawal et al21 performed adjustment 48 hours after the strabismus surgery.
At the end of the current study, 6 months after surgery, five cases still suffered from exotropia. The success rate was 88.1%. None of our patients had overcorrection (esodeviation) at the end of the 6 months follow-up period.
As previously stated, we aimed at a slight overcorrection in our patients, so as to avoid postoperative exodrift and to achieve a successful long-term outcome. All patients who were overcorrected at postoperative day 1 had a favorable outcome and were orthophoric at 6 months after surgery. However, failed cases at 6 months after surgery comprised four patients who were undercorrected (exodeviation) after adjustment plus one orthophoric patient who had exodrift later. Several previous studies have found a significant association between postoperative overcorrection and favorable long-term outcome.12–14 This is due to the occurrence of exodrift postoperatively, which was associated with higher recurrence rate.22–24 Consequently, several studies recommended a target of slight esotropia not exceeding 10 pd.10,11 On the other hand, overcorrection of 10 pd or above was reported to increase the risk of consecutive esotropia.25
Similar rates of success were reported by previous studies. Agrawal et al21 compared between adjustable and non-adjustable suture recession and reported a success rate of 89.4% in the adjustable suture group at 6 months postoperatively. Kamal et al17 compared the use of adjustable and non-adjustable sutures in children with primary horizontal strabismus. They found a success rate at the end of 6 months of 86.67% in the adjustable suture group. Kamlesh et al19 reported that at the end of 12th week postoperatively, 90% of the patients with adjustable suture were within 10 pd of orthophoria.
However, lower rates of success were also reported in the literature. Zhang et al26 reported a success rate of 74.8% in adults at 12 weeks after surgery. Vasconcelos et al27 found that the success rate at 1 year after surgery in patients with exotropia undergoing adjustable suture recession was only 50.0%. Chalifoux et al18 found that the overall success rate for alignment at 4–6 months postoperatively was 74.6% in patients undergoing adjustable suture technique.
Variations in the rate of success reported at the end of studies can be explained by the variability in patients’ age, type of strabismus, technique of adjustable sutures, and the defined angle of successful alignment.
Potential factors that may have affected the outcome at 6 months after the surgery were evaluated in the current study. Factors that were significantly related to failed procedure included higher mean preoperative angle of deviation, longer mean amount of lateral rectus recession, higher mean immediate postoperative angle, and the need of bilateral adjustment.
Chalifoux et al18 similarly pointed to the effect of preoperative angle on success as patients with preoperative deviation of 40 pd or more had a significantly lower surgical success rate (63.8%) than patients with a deviation less than 40 pd (80%).
The effect of immediate postoperative angle on success was also highlighted by Liebermann et al28 and Mireskandari et al.29 Liebermann et al28 concluded that achieving the target range was most probably the most important determinant of success, whether adjustable sutures were used or not. Moreover, Mireskandari et al29 reported also that patients who met the target range had a significantly higher rate of success than patients who did not meet the target (83.6% vs 63.7%). Meanwhile, the use of adjustable suture procedure allows for achieving the target angle in a higher proportion of patients; thus, the success rate is increased in those patients.29
Literature points to a tendency of surgeons to use adjustable sutures in adults, rather than in children.5,30 This can be explained by the expectations of surgeons that children would not cooperate during examination and adjustment, as well as a fear of increased time, cost, and risks of surgery.4 However, we found no effect of age on the success rate at the end of 6 months after surgery. Our finding is supported by other studies performed on children who reported success rates that ranged from 74% to 88%.5,6,17,31–33 These rates are comparable to those achieved in adults.
Complications following the performance of adjustable suture include those of strabismus surgery plus procedure-specific complications such as vagal stimulation during adjustment, increase of postoperative inflammation (7%) and granuloma (1.7–13%),7,34 exposure of sutures, and slipping of suture knot (in 0.3–0.8% of the cases).35,36 We did not encounter any of these complications in the current study, which may favor the adoption of its technique.
The present work demonstrated that the laser-assisted lysis of adjustable sutures had an overall success rate of 88.1% with only 11.9% of the patients showing exotropia. Moreover, this technique is simple, does not require major surgical skills, and is frequently used in the treatment of glaucoma.37
The present study is the first to describe the use of argon laser in lysis of adjustable sutures following strabismus surgery. In addition, the sample included patients with one type of deviation (exotropia), unlike many of the previous studies that included patients with eso-and exo-deviations and thus the interpretation of their results was difficult. Patients were followed up for a convenient period of time, with no loss to follow-up. On the other hand, our study was subject to some limitations. A larger sample of size is required before ascertaining the results obtained in our study. Also, it would be better to compare between the new technique and the traditional technique of suture release.
Conclusion
The laser-assisted releasable suture technique can help achieve successful alignment. Patients with lower preoperative angle of deviation, irrespective of age, have a significantly higher probability of success.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Babu S, Goel Y, Chaudhary RB, et al. Comparison of adjustable sutures versus nonadjustable sutures in intermittent exotropia. Eur J Ophthalmol. 2018;28(3):264–267. doi:10.5301/ejo.5001063
2. Hassan S, Haridas A, Sundaram V. Adjustable versus non-adjustable sutures for strabismus. Cochrane Database Syst Rev. 2018;3:Cd004240. doi:10.1002/14651858.CD004240.pub4
3. Sun Y, Zhang T, Chen J. Bilateral lateral rectus recession versus unilateral recession resection for basic intermittent exotropia: a meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2018;256:451–458. doi:10.1007/s00417-018-3912-1
4. Guyton DL. A testimony for Postop’ adjustable sutures in strabismus surgery, on the 25th (Silver) anniversary of Arthur Jampolsky’s original description. Binocul Vis Strabismus Q. 2001;16(4):241–242.
5. Hakim OM, El-Hag YG, Haikal MA. Releasable adjustable suture technique for children. J AAPOS. 2005;9(4):386–390. doi:10.1016/j.jaapos.2005.02.015
6. Chan TK, Rosenbaum AL, Hall L. The results of adjustable suture technique in paediatric strabismus surgery. Eye (London, England). 1999;13(Pt 4):567–570. doi:10.1038/eye.1999.140
7. Nihalani BR, Whitman MC, Salgado CM, Loudon SE, Hunter DG. Short tag noose technique for optional and late suture adjustment in strabismus surgery. Arch Ophthalmol. 2009;127(12):1584–1590. doi:10.1001/archophthalmol.2009.305
8. Tsai CB. Adjustable suture strabismus surgery in pediatric patients using pull-string technique. Taiwan j Ophthalmol. 2017;7(1):38–43. doi:10.4103/tjo.tjo_15_17
9. Coats DK. Ripcord adjustable suture technique for use in strabismus surgery. Arch Ophthalmol. 2001;119(9):1364–1367. doi:10.1001/archopht.119.9.1364
10. Ruttum MS. Initial versus subsequent postoperative motor alignment in intermittent exotropia. J AAPOS. 1997;1(2):88–91. doi:10.1016/s1091-8531(97)90004-5
11. McNeer KW. Observations on the surgical overcorrection of childhood intermittent exotropia. Am Orthoptic J. 1987;37(1):135–150. doi:10.1080/0065955X.1987.11981748
12. Kanjanawasee P, Praneeprachachon P, Pukrushpan P. Relation between early postoperative deviation and long-term outcome after unilateral lateral rectus recession and medial rectus resection for adult exotropia. Int J Ophthalmol. 2018;11(8):1358–1362. doi:10.18240/ijo.2018.08.17
13. Oh JY, Hwang JM. Survival analysis of 365 patients with exotropia after surgery. Eye (London, England). 2006;20(11):1268–1272. doi:10.1038/sj.eye.6702091
14. Jung EH, Kim SJ, Yu YS. Factors associated with surgical success in adult patients with exotropia. J AAPOS. 2016;20(6):511–514. doi:10.1016/j.jaapos.2016.08.011
15. Isenberg SJ, Abdarbashi P. Drift of ocular alignment following strabismus surgery. Part 2: using adjustable sutures. Br J Ophthalmol. 2009;93(4):443–447. doi:10.1136/bjo.2007.136382
16. Hasebe S, Nakatsuka C, Nonaka F, Fujiwara H, Ohtsuki H. Accuracy of suture adjustment in adjustable strabismus surgery evaluated at the initial postoperative examination. Jpn J Ophthalmol. 2002;46(3):279–284. doi:10.1016/s0021-5155(01)00522-6
17. Kamal AM, Abozeid D, Seif Y, Hassan M. A comparative study of adjustable and non-adjustable sutures in primary horizontal muscle surgery in children. Eye (London, England). 2016;30(11):1447–1451. doi:10.1038/eye.2016.144
18. Chalifoux E, Alkharashi M, Superstein R, et al. Adjustable surgical treatment of adult exotropia: postoperative target angles and surgical success. Can J Ophthalmol/ J Canadien D’ophtalmologie. 2016;51(4):254–257. doi:10.1016/j.jcjo.2016.02.017
19. Kamlesh BS, Goel Y, et al. Comparison of adjustable sutures versus nonadjustable sutures in intermittent exotropia. 2018;28(3):264–267. doi:10.5301/ejo.5001063
20. Muralidhar R, Churawan L, Sekar M, Chidambaram AP, Mugdha P, Ramamurthy D. Outcome of delayed adjustable strabismus surgery in children using a bow-tie optional adjustable technique. Indian J Ophthalmol. 2019;67(2):258–262. doi:10.4103/ijo.IJO_398_18
21. Agrawal S, Singh V, Singh P. Adjustable recessions in horizontal comitant strabismus: a pilot study. Indian J Ophthalmol. 2015;63(7):611–613. doi:10.4103/0301-4738.167117
22. Lim SH, Hwang BS, Kim MM. Prognostic factors for recurrence after bilateral rectus recession procedure in patients with intermittent exotropia. Eye (London, England). 2012;26(6):846–852. doi:10.1038/eye.2012.55
23. Lim SH, Hong JS, Kim MM. Prognostic factors for recurrence with unilateral recess-resect procedure in patients with intermittent exotropia. Eye (London, England). 2011;25(4):449–454. doi:10.1038/eye.2011.12
24. Tibrewal S, Singh N, Bhuiyan MI, Ganesh S. Factors affecting residual exotropia after two muscle surgery for intermittent exotropia. Int J Ophthalmol. 2017;10(7):1120–1125. doi:10.18240/ijo.2017.07.16
25. Pineles SL, Deitz LW, Velez FG. Postoperative outcomes of patients initially overcorrected for intermittent exotropia. J AAPOS. 2011;15(6):527–531. doi:10.1016/j.jaapos.2011.08.007
26. Zhang MS, Hutchinson AK, Drack AV, Cleveland J, Lambert SR. Improved ocular alignment with adjustable sutures in adults undergoing strabismus surgery. Ophthalmology. 2012;119(2):396–402. doi:10.1016/j.ophtha.2011.07.044
27. Vasconcelos GC, Almeida HC. Adjustable versus non-adjustable suture techniques for concomitant horizontal strabismus: a comparative study. Arq Bras Oftalmol. 2015;78(6):352–355. doi:10.5935/0004-2749.20150093
28. Liebermann L, Hatt SR, Leske DA, Holmes JM. Adjustment versus no adjustment when using adjustable sutures in strabismus surgery. J AAPOS. 2013;17(1):38–42. doi:10.1016/j.jaapos.2012.10.017
29. Mireskandari K, Schofield J, Cotesta M, Stephens D, Kraft SP. Achieving postoperative target range increases success of strabismus surgery in adults: a case for adjustable sutures? Br J Ophthalmol. 2015;99(12):1697–1701. doi:10.1136/bjophthalmol-2014-306258
30. Keech RV, Scott WE, Christensen LE. Adjustable suture strabismus surgery. J Pediatr Ophthalmol Strabismus. 1987;24(2):97–102.
31. Dawson E, Bentley C, Lee J. Adjustable squint surgery in children. Strabismus. 2001;9(4):221–224. doi:10.1076/stra.9.4.221.694
32. Engel JM, Rousta ST. Adjustable sutures in children using a modified technique. J AAPOS. 2004;8(3):243–248. doi:10.1016/j.jaapos.2004.01.007
33. Awadein A, Sharma M, Bazemore MG, Saeed HA, Guyton DL. Adjustable suture strabismus surgery in infants and children. J AAPOS. 2008;12(6):585–590. doi:10.1016/j.jaapos.2008.06.005
34. Eustis HS, Elmer TR
35. Budning AS, Day C, Nguyen A. The short adjustable suture. Can J Ophthalmol/ J Canadien D’ophtalmologie. 2010;45(4):359–362. doi:10.3129/i10-012
36. Sami DA. Conjunctival incisions for strabismus surgery: a comparison of techniques. Techniq Ophthalmol. 2007;5:125–129. doi:10.1097/ito.0b013e3181565102
37. Ramakrishna S, Nelivigi S, Sadananda AM, Ganesh S. Study of efficacy and timing of laser suture lysis in reducing intraocular pressure after trabeculectomy with mitomycin-C. Oman J Ophthalmol. 2016;9(3):144–149. doi:10.4103/0974-620X.192264
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.