Back to Journals » Clinical Ophthalmology » Volume 14
Large Retinectomies for Retinal Detachment Complicated by Proliferative Vitreoretinopathy: Anatomical and Functional Outcome of Silicone Oil versus Perfluoropropane Gas
Authors Dimitrios B, Krassas G, Dettoraki M, Lavaris A, Sideri AM, Droutsas K, Moschos MM
Received 8 December 2019
Accepted for publication 23 July 2020
Published 15 September 2020 Volume 2020:14 Pages 2679—2686
DOI https://doi.org/10.2147/OPTH.S241479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Brouzas Dimitrios, George Krassas, Maria Dettoraki, Anastasios Lavaris, Anna-Maria Sideri, Konstantinos Droutsas, Marilita M Moschos
Department of Ophthalmology, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece
Correspondence: Brouzas Dimitrios
Department of Ophthalmology, School of Medicine, National and Kapodistrian University of Athens, 10 G. Papandreou Str, Byron-Athens 16231, Greece
Email [email protected]
Purpose: To assess the anatomic and functional outcomes of eyes undergoing vitrectomy and large retinectomy for the management of retinal detachment (RD) complicated by advanced proliferative vitreoretinopathy (PVR).
Methods: A total of 66 eyes of 63 patients with RD complicated by PVR were treated with vitrectomy and 180° or more retinectomy and silicone oil (n=46) or perfluoropropane gas (n=20) were used as intraocular tamponades.
Results: Retinal reattachment was achieved in 89.39% (59 eyes) of the cases. The mean follow-up was 33.7 months (range 12– 76 months). In gas-filled eyes, the final anatomic success rate was 85% (17 eyes) and in silicone oil-filled eyes was 91.3% (42 eyes) (p=0.46). After the initial retinectomy, the total anatomic success rate was 80.3% (53/66 eyes), 70% in gas-filled eyes (14/20 eyes) and 84.79% in silicone oil-filled eyes (39/46 eyes) (p=0.19). Visual acuity (VA) improved in 37 (56.06%) eyes, remained the same in 19 (28.78%) eyes and became worse in 10 (15.15%) cases. Best corrected VA was ≥ 20/200 in 22 eyes 33.33%. The final VA was associated with the preoperative VA (r=0.68), the preoperative status of the macula influence significantly the final visual acuity (p< 0.0001) and there is statistically significant difference in the final visual acuity between eyes with and without anatomic success (p< 0.05).
Conclusion: The large circumferential retinectomies can be beneficial in eyes with RD complicated by advanced PVR. No significant difference was found in anatomic success rate, and rate of complications between eyes with silicone oil tamponade and long acting gas undergoing large retinectomy. Regarding the final BCVA, slight difference was found in favor of gas-filled eyes.
Keywords: large retinectomies, proliferative vitreoretinopathy, silicone oil tamponade, perfluoropropane gas tamponade
Introduction
Proliferative vitreoretinopathy (PVR) is the most common cause of retinal detachment surgery failure and requires complex and challenging vitreoretinal surgery.1–3 Membrane peeling, scleral buckling, gas or silicone oil tamponade and extensive retinotomy or retinectomy constitute some surgical approaches necessary for the management of severe PVR. Since their first description in 1979, retinotomy and retinectomy are still widely used as a last resort when anterior PVR and retinal “shortening” cannot be relieved by membrane dissection or scleral buckle.4 Peripheral retina is cut or excised to preserve function of more visually significant posterior retina.
Both silicone oil and perfluoropropane gas (C3F8) have been used as tamponades in eyes undergoing retinectomy for PVR management but contradictory results have been reported regarding the surgical success rate and the severity of postoperative complications between the two types of intraocular tamponades.5–8
The aim of this study is to evaluate the anatomic and functional outcomes of large circumferential retinotomies and retinectomies in the management of complicated retinal detachment by proliferative vitreoretinopathy (PVR). We also compared the use of silicone oil versus C3F8 tamponade on the rate of retinal reattachment, functional outcome and intraocular pressure.
Subjects and Methods
A prospective study of all patients 66 eyes (63 patients) that underwent pars plana vitrectomy (PPV) with 180 degrees or more retinotomy and retinectomy for complex rhegmatogenous retinal detachment (RRD) was conducted between December 2010 and June 2016. Eyes with proliferative diabetic retinopathy, retinotomy of less than 180 degrees, inadequate follow-up and documentation were excluded. A minimum follow-up period of 6 months was required for inclusion into this study. Also, 3 patients with preoperative visual acuity better than 2/10 treated with gas were excluded from the study so as the two groups to have statistically comparative preoperative visual acuities.
All surgeries were performed by a single surgeon (D.B.). The standard three ports 20-gauge and 23-gauge PPV were used. The vitreous base was removed to the full extent possible and the epiretinal membranes were dissected with intraocular forceps. Two rows of intraocular diathermy were applied to the margin of the retina before creating a relaxing retinotomy to prevent hemorrhage. After diathermy, the retina was cut in all the cases by using intraocular scissors in 20 gauge vitrectomy and with the vitrectomy probe in 23 gauge vitrectomy. Retinotomy was made when foreshortening of the retina could not be relieved by removal of the epiretinal membranes or when the presence of subretinal proliferation would prevent retinal flattening and reattachment to the underlying retinal pigment epithelium. Retinotomy was followed by peripheral retinectomy with careful removal of the retina anterior to the incision. Retinectomy was circumferential and ≥180°. Hemostasis was maintained with cauterization and temporary elevation of intraocular pressure when needed. Retina was flattened with intraocular injection of perfluorocarbon liquid. Laser photocoagulation was applied in three rows along the posterior margin of the retinectomy. For postoperative tamponade, perfluoropropane (C3F8) in minimally expansive concentration (14%) or silicone oil (5000 and 5700 centistokes) was employed. At the end of surgery, retina was reattached in all eyes. Retinotomy extent was assessed intraoperatively in degrees.
All patients had 7 days face down positioning, irrespectively of silicone or gas tamponade.
Preoperative data included age, gender, eye, lens status (phakic, pseudophakic or aphakic), best corrected visual acuity (BCVA), intraocular pressure, number and details of previous operations and macula status for each patient. Postoperatively, the length of follow-up, BCVA, final intraocular pressure, retinal status, silicone oil tamponade versus gas tamponade and complications were recorded. The IOP was considered elevated when it was found to be equal to or greater than 22 mmHg and hypotony was defined as IOP equal to or less than 5mmHg.
Baseline PVR was graded intraoperatively according to the updated Retina Society Classification proposed by Machemer et al9 in 1991. Specifically, grade C “posterior PVR” referred to eyes with focal full-thickness retinal folds (C1) or diffuse contraction (C2) located posterior to the equator, “anterior PVR” included eyes with circumferential contraction (C4) or anterior traction on the retina at the vitreous base (C5) alone or with posterior PVR and “subretinal PVR” referred to eyes with subretinal fibrosis only (C3). The visual acuity was converted to logMAR for statistical reasons. “Count fingers” was defined as 1.7 logMAR, “hand motion” as 1.8 and “light perception” as 1.9.
All data were collected in a database and statistical analysis was performed using Fisher’s exact test or Mann–Whitney U-test.
The study was conducted at the 1st Department of Ophthalmology, “G. Gennimatas” General Hospital, University of Athens, Athens, Greece. All participants provided written informed consent. The study protocol followed the principles in the Declaration of Helsinki and was approved by the institutional review board of “G. Gennimatas” General Hospital, Athens, Greece.
Results
Baseline Characteristics
Of 69 eyes of 66 patients in the study were included 66 eyes of 63 patients 3 cases with VA better than 1/20 treated with gas were excluded from the statistical evaluation so as not to be statistical difference in preop VA between the two groups. There was a male predominance (male to female ratio 1.7:1). The mean age was 65.3 years with a range from 28 to 92 years. The mean follow-up time was 17.7 months (range 6–54 months).
The indications for vitrectomy and retinectomy in our study were primary RRD with PVR in 12 eyes (18.19%) and previous failed RD operation(s) in 54 eyes (81.81%).
Preoperatively, 13 (19.70%) eyes were phakic and 53 (80.3%) were pseudophakic. The mean number of previous operations was 1.04 (range: 0–3). Preoperative visual acuity ranged from light perception to 6/10 (Table 1).
 |
Table 1 Baseline Characteristics of the Patients |
Perfluoropropane (C3F8) was used as postoperative intraocular tamponade in 20 eyes and silicone oil tamponade was used in 46 eyes. The decision to perform retinectomy, PVR classification and the type of intraocular tamponade used were made during surgery (Table 2).
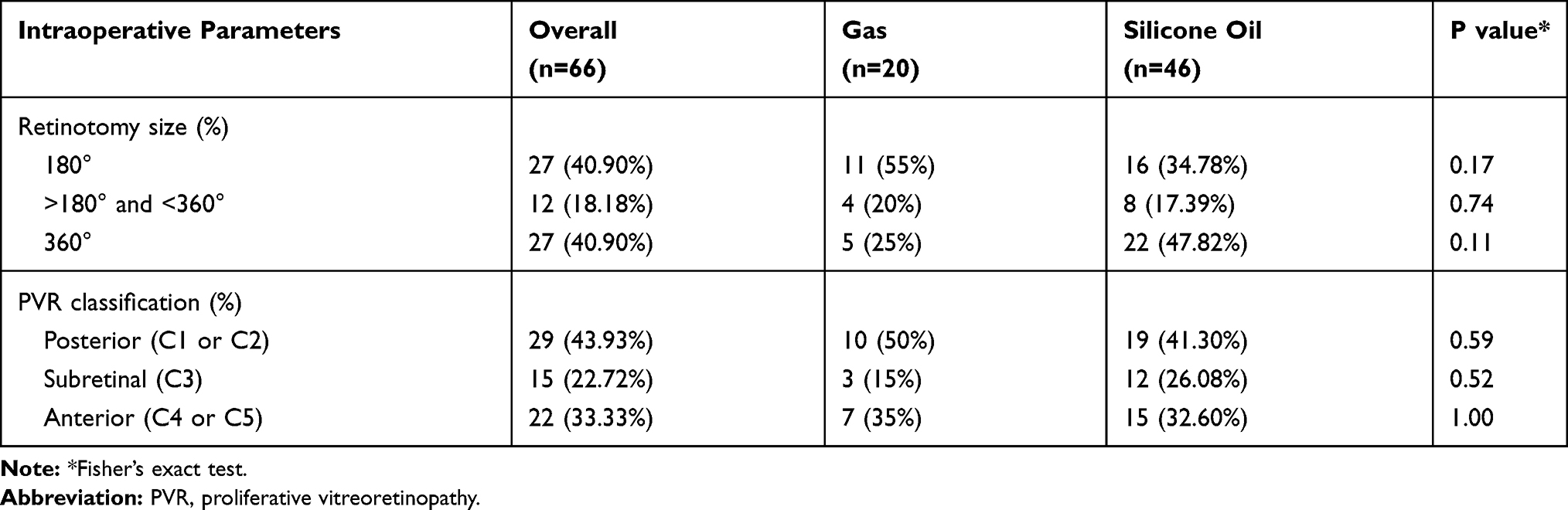 |
Table 2 Intraoperative Parameters |
Preoperatively, the age and gender of patients, the average BCVA, the type and number of previous vitreoretinal operations and previous lens extractions did not differ significantly between the two groups of intraocular tamponade.
Anatomic Outcome
Complete retinal reattachment was achieved in 89.39% (59 out of 66 eyes) in the last examination. After the initial retinectomy, the total anatomic success rate was 80.3% (53 eyes out of 66). In gas-filled eyes, the anatomic success rate was 70% (14 eyes out of 20) and in silicone oil-filled eyes, the anatomic success rate was 84.79% (39 eyes out of 46) (p=0.19). One silicone oil-filled eye and 3 gas-filled eyes with recurrent retinal detachment underwent further surgery and received silicone oil tamponade. Of the 9 cases with recurrent retinal detachment without further intervention one case of silicone group ended up with phthisis bulbi, 4 refused further surgery and 4 will consider surgery in the future. Recurrent PVR occurred in 3 (15%) gas-filled eyes and 6 (13.04%) eyes with silicone tamponade (p=0.23). In most cases the recurrent PVR started from the edges of retinectomy. Four (20%) eyes of gas tamponade group and 6 (13.04%) with silicone oil developed epiretinal membranes (p=0.48). Seven (15.21%) out of 46 eyes that received silicone tamponade presented with silicone oil in the anterior chamber and 2 (4.34%) eye that received silicone oil developed band keratopathy. Phthisis bulbi occurred in 1 (2.17%) eye with silicone oil (p=1.00) (Table 3).
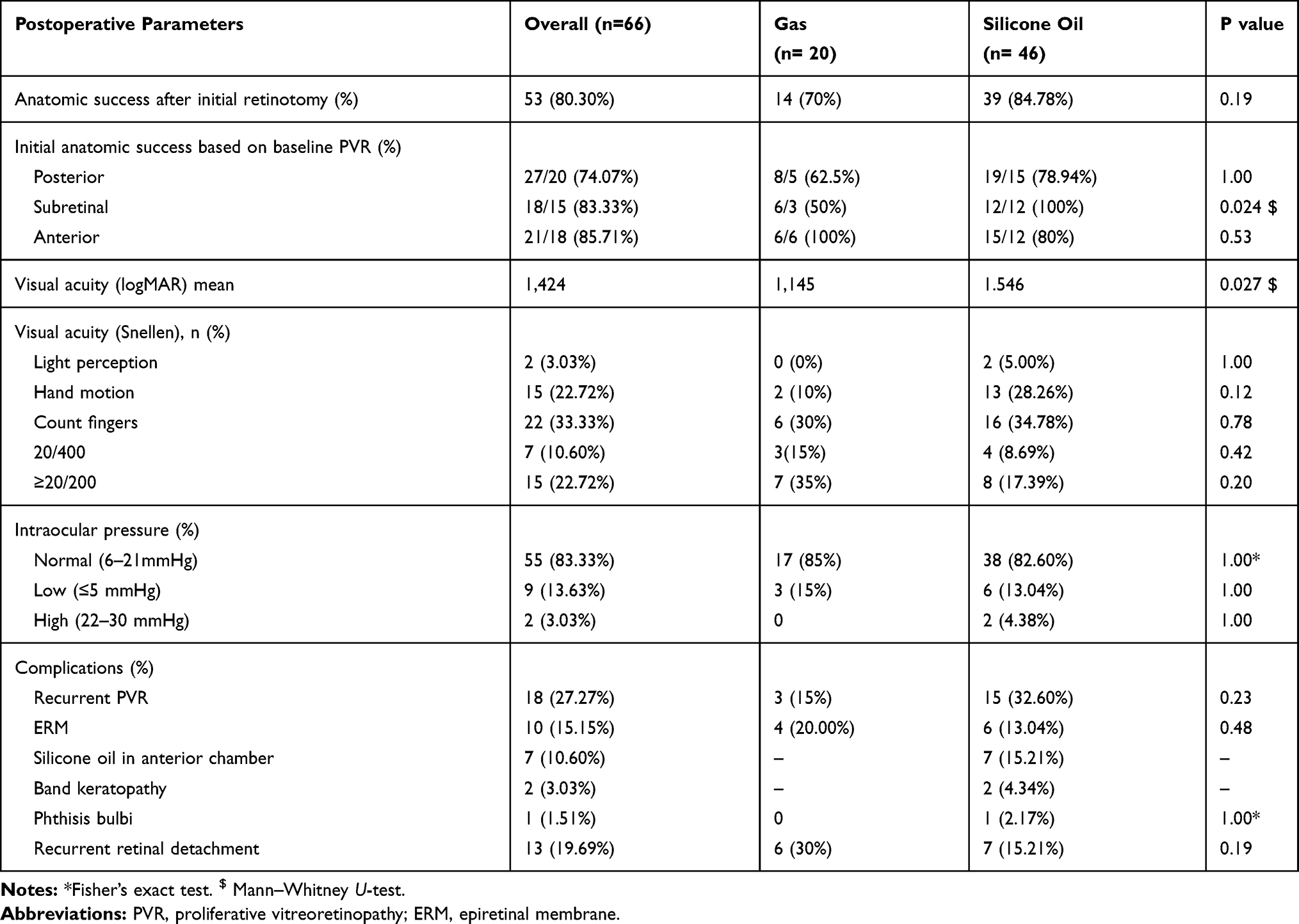 |
Table 3 Postoperative Findings |
Functional Outcome
The mean BCVA significantly improved from 1.679 logMAR preoperatively to 1.424 logMAR at the end of follow-up period in all cases (p=0.0052) (Figure 1). Visual acuity improved in 37 (56.06%) eyes, remained the same in 19 (28.78%) eyes and became worse in 10 (15.15%) cases. BCVA was ≥20/200 in 22 eyes (33.33%). No patient attained postoperative BCVA better than 0.30 logMAR. (Snellen visual acuity in silicone oil, gas filled, and in all cases are presented in Figure 2). The average BCVA at the end of follow-up period in gas-filled eyes (1.145 logMAR) was significantly different compared with the average postoperative BCVA in eyes which received silicone oil 1.546 logMAR in the last examination (p=0.0268). The final IOP was normal (range 6–21mmHg) in 55 (83.33%) eyes, low (≤5mmHg) in 9 (13.63%) eyes and elevated (22–30mmHg) in 2 (3.03%) cases. No statistically significant difference in the incidence of hypotony between the gas-filled and siliconized eyes was found (p=1.00) (Table 3). Silicone oil extraction was performed in 33 out of 46 eyes (71.73%) and no retinal detachment reoccurred until the end of the follow-up period. In 13 cases without silicone extraction, 4 cases (30.77%) refuse further surgery, 6 eye (46.15%) manifested hypotony, and in 3 (23.08%) presented reappearance of PVR.
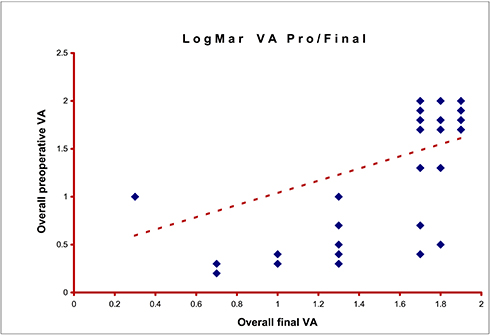 |
Figure 1 Overall logMar preoperative vs final VA. |
 |
Figure 2 Snellen visual acuity preop/postop in silicone oil, gas filled, and in all cases. |
Parameters that may affect final visual acuity are listed in Table 4. Final VA was associated with the preoperative VA (r=0.68), the preoperative status of the macula influence significantly the final visual acuity (p<0.0001) and there is statistically significant difference in the final visual acuity between eyes with and without anatomic success (p<0.05). No statistically significant relation was found between the final visual acuity and the age of patients, the subtypes of grade C PVR, the number of previous operations. A significant difference was found regarding the final BCVA between gas-filled eyes and Silicon filled eyes (p=0.0268).
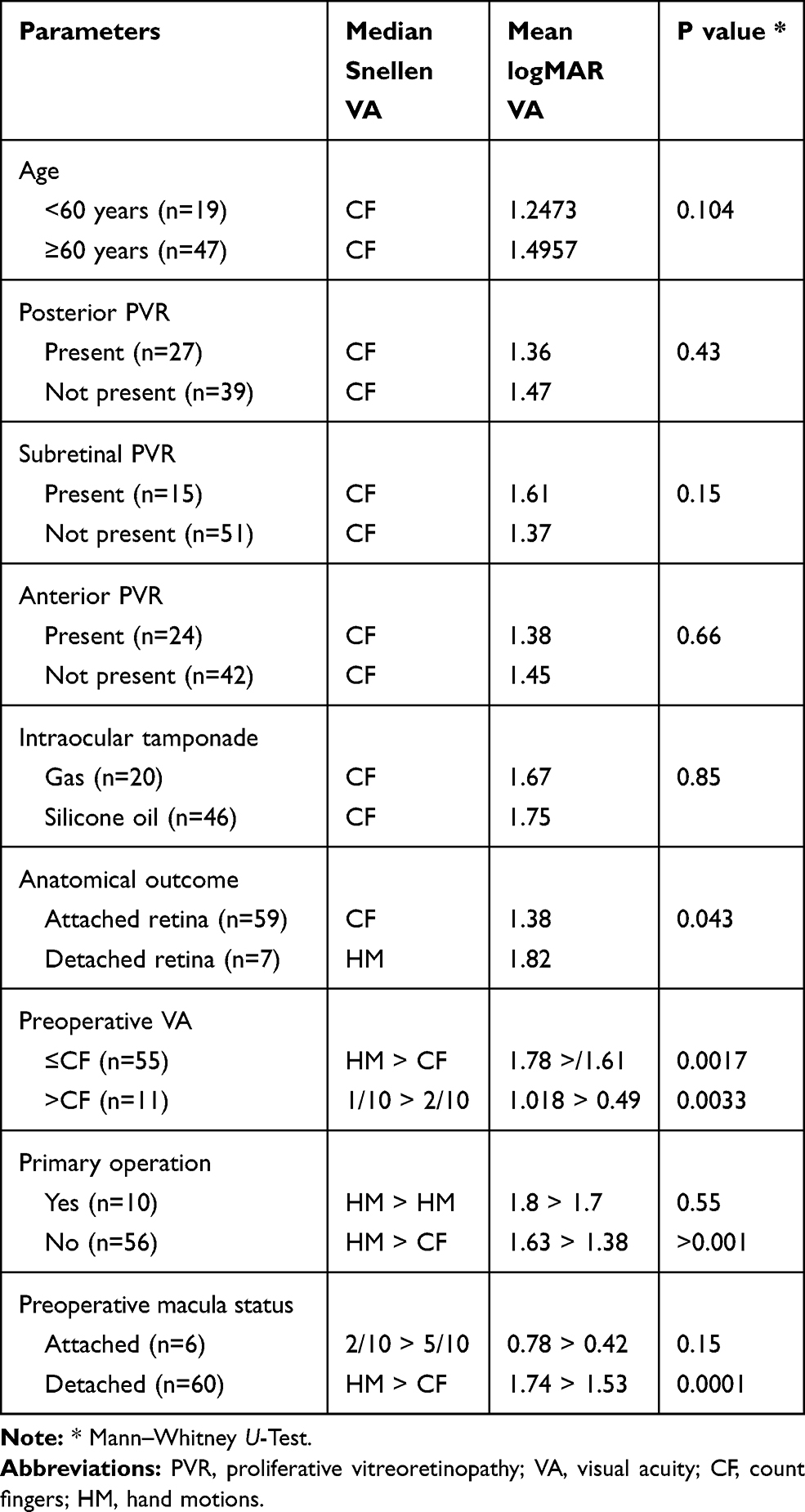 |
Table 4 Parameters That May Influence Final Visual Acuity |
Discussion
Retinectomy is a valuable surgical technique in the management of retinal detachment complicated by advanced PVR. The use of wide angle viewing systems facilitates visualization of anterior PVR and performance of peripheral retinectomy. Furthermore, the availability of perfluorocarbon liquids aids the removal of epiretinal membranes, leading to increased success rates in PVR surgery during the last years.
In our study, 89.39% (59 out of 66 eyes) of cases, which underwent large retinotomy and retinectomy for the management of complicated retinal detachment by PVR, attained complete retinal reattachment in the last examination. The current study is in accordance with previous studies of more than 180 degrees retinectomy surgery that achieved final anatomic success rates of 61%-90%.6,10-12 In our study, BCVA improved after surgery in (56.06%) of our patients and remained stable in (28.78%). BCVA of 20/200 or better was found in 33.33% of eyes postoperatively, which is in accordance with previous retinectomy reports with a functional success, defined as BCVA equal or more than 20/200, ranging from 10% to 59%.8,12-18 Grigoropoulos et al13 in 2007 studied 304 eyes with PVR and reported a visual improvement or stabilization in 69% of the cases and visual acuity equal or more than 6/60 in 27.7% of cases after retinectomy. In 2016 Wong et al in a retrospective study of 36 patients after silicone removal report improvement and stabilization in 63.9% of the cases after silicone removal.19 However, comparison among retinectomy studies is problematical because of differences, mainly, in inclusion criteria. Specifically, a variability concerning the indications for retinectomy exists, since many studies included cases with tractional RD, proliferative diabetic retinopathy, penetrating injury or endophthalmitis.10,11,13,14,20,21 Moreover, the extent of retinectomy varies among studies ranging from a few clock hours to 360° and different surgical techniques have been reported, including combined large radial retinotomy with circumferential retinectomy or radical anterior base dissection with lens removal and retinectomy.8,16
In 1993 the Silicone Study5 reported that silicone oil and C3F8 were equally effective as tamponades for eyes with severe PVR undergoing retinotomy. Similarly, in 2010 Shalaby6 observed that recurrent retinal detachment and postoperative hypotony after retinectomies were not associated with the type of intraocular tamponade. On the contrary, in 2005 Tseng et al7 and in 2006 Quiram et al8 found that the use of silicone oil was associated with better anatomic success rates than gas tamponade. Since most retinectomy studies used silicone oil as tamponade in all cases with RD and PVR, little information exists regarding the use of C3F8 and its outcome.10–17,20–22 In the current study, both C3F8 and silicone oil were studied as tamponades after large circumferential retinectomies in eyes with RD complicated with PVR. We found no statistically significant difference in the anatomic success rate, and rate of complications between the gas-filled and silicone-filled eyes undergoing extensive retinectomy, which was in accordance with the results of Silicone Study and Shalaby but regarding the BCVA we found slight difference in favor of gas-filled eyes.
Hypotony was present in 13.63% of eyes 13.04% in silicone-filled eyes and 15% in gas-filled eyes in the last examination in our study p=0.42. This result was comparable to those previously reported by other retinectomy studies in which hypotony rate ranged from 4.1% to 39%.12–14,16,18,22 In the Silicone Study,5 silicone oil was associated with a lower incidence of hypotony than long-acting gas in eyes with retinectomy. However, we found no statistically significant association between hypotony rate and intraocular tamponade. Recently, Shalaby6 also reported that hypotony was not associated with the type of tamponade used. Although the exact mechanism of postoperative hypotony in eyes with retinectomy is unknown, large areas of exposed retinal pigment epithelium leading to increased choroidoscleral outflow and tractional ciliary body detachment may account for decreased intraocular pressure.
In our study, the main causes of anatomical and functional failure were retinal detachment due to recurrent PVR and hypotony. Proliferation was developed at the site of retinectomy causing further retinal shortening but also at the posterior pole and macula.
Our study has several strengths, including the single surgeon performing all the procedures and the fact that it is a prospective study. In the majority of retinectomy studies, the procedures were performed by a number of different vitreoretinal surgeons using a range of surgical techniques.8,10,13,20 However, our study is limited by its relatively short follow-up period and by the fact that it is not a randomized one. Although there is no difference in PVR grade between gas-filled and silicone-filled eyes, we feel that patients’ related factors and surgeon’s preferences influence the allocation of the patients.
In conclusion, the current study suggests that large circumferential retinectomies can be beneficial in eyes with retinal detachment complicated by advanced PVR. Furthermore, no significant difference was found in anatomic success rate and rate of complications between eyes with silicone oil tamponade and long-acting gas undergoing large retinectomy. Regarding the VA we found slight difference in favor of long-acting gas. The study underlines that the postoperative visual function reflects the severity of the preoperative disease, since eyes attaining the best postoperative VA were those that had the best initial visual acuities and the best preoperative macular status.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Lewis H, Aaberg TM, Abrams GW. Causes of failure after initial vitreoretinal surgery for severe proliferative vitreoretinopathy. Am J Ophthalmol. 1991;111:8–14. doi:10.1016/S0002-9394(14)76889-8
2. Sternberg P
3. Wickham L, Ho-Yen GO, Bunce C, Wong D, Charteris DG. Surgical failure following primary retinal detachment surgery by vitrectomy: risk factors and functional outcomes. Br J Ophthalmol. 2011;95:1234–1238. doi:10.1136/bjo.2010.190306
4. Machemer R. [Cutting of the retina: a means of therapy for retinal reattachment (author’s transl)]. Klin Monbl Augenheilkd. 1979;175:597–601.
5. Blumenkranz MS, Azen SP, Aaberg T, et al. Relaxing retinotomy with silicone oil or long-acting gas in eyes with severe proliferative vitreoretinopathy. Silicone Study Report 5. The silicone study group. Am J Ophthalmol. 1993;116(5):557–564. doi:10.1016/S0002-9394(14)73196-4
6. Shalaby KA. Relaxing retinotomies and retinectomies in the management of retinal detachment with severe proliferative vitreoretinopathy (PVR). Clin Ophthalmol. 2010;4:1107–1114. doi:10.2147/OPTH.S4934
7. Tseng JJ, Barile GR, Schiff WM, Akar Y, Vidne-Hay O, Chang S. Influence of relaxing retinotomy on surgical outcomes in proliferative vitreoretinopathy. Am J Ophthalmol. 2005;140:628–636. doi:10.1016/j.ajo.2005.04.021
8. Quiram PA, Gonzales CR, Hu W, et al. Outcomes of vitrectomy with inferior retinectomy in patients with recurrent rhegmatogenous retinal detachments and proliferative vitreoretinopathy. Ophthalmology. 2006;113(11):2041–2047. doi:10.1016/j.ophtha.2006.05.039
9. Machemer R, Aaberg TM, Freeman HM, Irvine AR, Lean JS, Michels RM. An updated classification of retinal detachment with proliferative vitreoretinopathy. Am J Ophthalmol. 1991;112(2):159–165. doi:10.1016/S0002-9394(14)76695-4
10. Kolomeyer AM, Grigorian RA, Mostafavi D, Bhagat N, Zarbin MA. 360 degrees retinectomy for the treatment of complex retinal detachment. Retina. 2011;31:266–274. doi:10.1097/IAE.0b013e3181eef2c7
11. Bovey EH, De Ancos E, Gonvers M. Retinotomies of 180 degrees or more. Retina. 1995;15:394–398. doi:10.1097/00006982-199515050-00004
12. Tsui I, Schubert HD. Retinotomy and silicone oil for detachments complicated by anterior inferior proliferative vitreoretinopathy. Br J Ophthalmol. 2009;93:1228–1233. doi:10.1136/bjo.2008.140988
13. Grigoropoulos VG, Benson S, Bunce C, Charteris DG. Functional outcome and prognostic factors in 304 eyes managed by retinectomy. Graefes Arch Clin Exp Ophthalmol. 2007;245:641–649. doi:10.1007/s00417-006-0479-z
14. Faude F, Lambert A, Wiedemann P. 360 degrees retinectomy in severe anterior PVR and PDR. Int Ophthalmol. 1998;22:119–123. doi:10.1023/A:1006254721964
15. Tranos P, Vakalis A, Asteriadis S, Lokovitis E, Georgalas I, Stavrakas P. Anatomic and functional outcomes of retinectomy for the management of complicated retinal detachment with proliferative vitreoretinopathy. Ther Clin Risk Manag. 2015;11:1515–1521. doi:10.2147/TCRM.S89467
16. Lim AK, Alexander SM, Lim KS. Combined large radial retinotomy and circumferential retinectomy in the management of advanced proliferative vitreoretinopathy. Retina. 2009;29:112–116. doi:10.1097/IAE.0b013e318187f14a
17. Garnier S, Rahmi A, Grasswil C, Kodjikian L. Three hundred and sixty degree retinotomy for retinal detachments with severe proliferative vitreoretinopathy. Graefes Arch Clin Exp Ophthalmol. 2013;251:2081–2085. doi:10.1007/s00417-013-2298-3
18. Han DP, Lewis MT, Kuhn EM, et al. Relaxing retinotomies and retinectomies. Surgical results and predictors of visual outcome. Arch Ophthalmol. 1990;108:694–697.
19. Wong R, De Luca M, Shunmugam M, Williamson T, Laidlaw A, Vaccaro V. Visual outcome after removal of silicone oil in patients undergoing retinectomy for complex retinal detachment. Int J Ophthalmol. 2016;9:108–110. doi:10.18240/ijo.2016.01.18
20. de Silva DJ, Kwan A, Bunce C, Bainbridge J. Predicting visual outcome following retinectomy for retinal detachment. Br J Ophthalmol. 2008;92:954–958. doi:10.1136/bjo.2007.131540
21. Banaee T, Hosseini SM, Eslampoor A, Abrishami M, Moosavi M. Peripheral 360 degrees retinectomy in complex retinal detachment. Retina. 2009;29:811–818. doi:10.1097/IAE.0b013e31819bab1d
22. Tan HS, Mura M, Oberstein SY, de Smet MD. Primary retinectomy in proliferative vitreoretinopathy. Am J Ophthalmol. 2010;149(3):447–452. doi:10.1016/j.ajo.2009.10.017
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.