Back to Journals » International Medical Case Reports Journal » Volume 18
Large Anterior Cervical Spine Schwannoma Causing Dysphagia: Case Report
Authors Joniec A ![]() , Mikolajczyk J
, Mikolajczyk J ![]() , Godlewski B
, Godlewski B ![]()
Received 14 February 2025
Accepted for publication 18 June 2025
Published 21 June 2025 Volume 2025:18 Pages 735—739
DOI https://doi.org/10.2147/IMCRJ.S522776
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Aleksander Joniec, Jedrzej Mikolajczyk, Bartosz Godlewski
Department of Orthopaedics and Traumatology, with Spinal Surgery Ward, Scanmed – St. Raphael Hospital, Cracow, Poland
Correspondence: Aleksander Joniec, Department of Orthopaedics and Traumatology, with Spinal Surgery Ward, Scanmed – St. Raphael Hospital, ul. Adama Bochenka 12, Cracow, 30-693, Poland, Email [email protected]
Introduction: Schwannomas are rare benign tumours of Schwann cell origin that rarely undergo malignant transformation and are most often (25– 45%) found in the head and neck region. We present a case of a large schwannoma arising directly from the anterior aspect of the cervical spine (C6-C7-Th1) that caused considerable oesophageal displacement and compression, manifesting as dysphagia.
Case Report: A 52-year-old male patient sought medical advice on account of intermittent dysphagia and a sense of pressure in the neck, in the absence of pain or neurological deficits. A magnetic resonance (MRI) scan and a subsequent open/surgical biopsy revealed a large schwannoma on the anterior aspect of the spine at C6-C7-Th1 causing compression of the oesophagus. Following a neurosurgical consultation, a radical gross resection of the tumour was carried out from an anterior approach, with no neurological complications. A histological examination of the tumour confirmed the initial diagnosis and a follow-up MRI scan demonstrated complete resection.
Conclusion: This case of successful treatment of a large schwannoma at the C6-C7-Th1 level highlights the importance of both MR imaging and biopsy in pre-operative planning. An anterior approach, routinely employed in cervical spine surgery, made it possible to perform a radical resection without neurological complications or the need to stabilise the cervical spine, which expedited the patient’s return to full fitness.
Keywords: schwannoma, dysphagia, cervical spine, anterior approach
Introduction
Schwannomas (neurilemmomas) are benign neoplasms arising out of Schwann cells, which form sheaths around cranial, peripheral and autonomic nerves. Schwannomas are rare lesions, accounting for as little as approx. 5% of all benign soft-tissue tumours. They are most commonly (25–45% of cases) found in the head and neck region.1 A schwannoma usually develops as a slowly growing, asymptomatic solitary mass. There is little risk of malignant transformation (8–13.9%).2 It can displace the internal jugular vein and carotid arteries; oesophageal impingement is rare.3 We present a case of a large schwannoma arising from the anterior aspect of the cervical spine (C6-C7-Th1) that caused considerable oesophageal displacement and compression, manifesting, among others, as dysphagia.
Case Report
A 52-year-old man made an appointment with his primary care physician on account of intermittent difficulty swallowing and, as he called it, “a strange sense of pressure” in the neck. He did not report significant pain and there were no neurological deficits. Additional work-up, including a magnetic resonance (MRI) scan, revealed a 5×4.3 x 3.2 cm tumour-like lesion in the neck contiguous with the anterior aspect of the cervical spine at the cervicothoracic junction (C6-C7-Th1). The lesion caused considerable oesophageal compression and displacement to the left, and significantly narrowed the oesophageal lumen (Figure 1A). The patient was initially referred to an Oncological Surgery Ward, where an open/surgical biopsy of the tumour revealed a schwannoma. In view of the uncommon location of the tumour on the anterior aspect of the spine and its large size, oncological surgeons did not choose to operate and requested an additional neurosurgical consultation to qualify the patient for surgical tumour resection. Following the consultation and a review of the MRI scan, the patient was qualified for resection of the tumour from a right anterior approach, typically employed in cervical spine procedures. The first stage of the surgery involved exposure of the anterior aspect of the cervical spine slightly cephalad to the location of the lesion. The incision was then extended caudally to expose the tumour mass resting on the anterior aspect of the spine at the level of C6-C7-Th1. A radical gross resection of the tumour was performed (Figure 2), its size corresponded with the size shown in the MRI scan. The excised tumour was submitted for a histological examination. The operators failed to identify a nerve branch in the region of the excised tumour that could potentially be the tumour’s site of origin. Following the surgery, the patient did not develop any new neurological deficits and the dysphagia subsided. He was able to move normally on his own and was discharged home in a good overall and neurological condition on the second post-operative day. A histological examination confirmed the earlier biopsy results, revealing an encapsulated tumour formed of spindle-shaped cells forming highly cellular (Antoni A) and poorly cellular (Antoni B) regions. A follow-up MRI scan at two months post-surgery demonstrated complete resection of the tumour and no evidence of compression (Figure 1B).
 |
Figure 1 MRI scans taken before (A) and after (B) surgical resection of the tumour at the C6-C7-Th1 level. The pre-operative images demonstrate significant compression and displacement of the oesophagus to the left. The tumour mass is indicated by the yellow arrows, while the red arrow indicates the compressed/displaced oesophagus. Post-operative images present status post complete resection of the tumour and absence of oesophageal compression/displacement. |
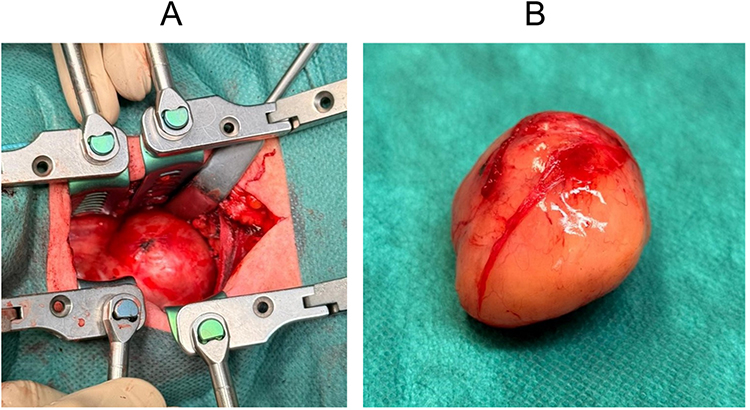 |
Figure 2 Gross appearance of the tumour in the operating field (A) and following complete resection (B). |
Discussion
Schwannomas are benign tumours developing from Schwann cells, forming sheaths of cranial, peripheral and autonomic nerves. They may develop at various locations, including in the head and neck region, where their sites of origin comprise anatomic structures such as the cranial nerves V–XII, brachial plexus and sympathetic trunk.4 The rate of growth of schwannomas partly depends on the individual predisposition of the patient, but generally they grow slowly, increasing by 1–3 mm in a year.5,6 Owing to this characteristic, watchful waiting and waiving surgery is sufficient in some cases. Suggested tools to aid in making the decision to operate include calculation of the tumour volume growth rate.7
In the literature, the most common site of origin of schwannomas has been the vestibular branch of cranial nerve VIII,8 while schwannomas arising from other sites in this region have been reported less frequently. Tumours developing in the region of cervical spine constitute a considerable challenge to the surgical team in view of the complex anatomy and proximity of a number of critical structures such as the carotid arteries and jugular veins, nerves as well as the oesophagus and trachea, which may give rise to complications9 such as an oesophageal perforation and subsequent infection as described by Ahn et al.10 A key factor with procedures in this region is to preserve intact nerve function as neural damage can lead to hoarse voice, dysphagia (vagus nerve) or dysphagia (hypoglossal and accessory nerves),11 these often being the only complaints the patient reports before surgery. The case of our patient is a good illustration of the clinical difficulties related to this location of the tumour, and so stresses the importance of careful preoperative planning and the expertise of the operating team in performing surgery in this region.
An additional diagnostic difficulty is the tendency of schwannomas of the neck to present clinically merely as palpable nodules without causing any other symptoms.12 In the case of our patient, a notable feature was dysphagia secondary to considerable compression of the oesophagus. An MRI scan was used to assess the tumour’s location and precisely determine tumour size, allowing for precisely planning the resection procedure. Additionally, a pre-operative histologic examination was an important element of the planning because the radiographic appearances of a schwannoma may be difficult to distinguish from those of other tumours or non-neoplastic lesions, particularly neurofibromas.13 Paragangliomas and lymphomas must be considered potential differential diagnoses as well, adding to the difficulty of the clinical decision-making process. A biopsy combined with an MRI scan makes it possible to establish a preliminary diagnosis, which is of key importance for choosing an optimal treatment.14 Schwannomas often exhibit strong S100 immunostaining which might prove useful in the identification process of the lesion.15
An important characteristic of schwannomas is a well-developed capsule and detachment of the tumour from the surrounding tissues,16 which usually makes it possible to resect the tumour without damage to adjacent tissues.17 These features make surgical resection effective in treating schwannomas, allowing the patient to return to full fitness soon.18 In our patient, the tumour was resected completely without damage to the bony structures of the spinal column or destabilization of the spine so that cervical stabilisation was not necessary.
The described approach was warranted by the size and localization of the lesion. It is important to understand that a different technique might be beneficial for schwannomas presenting different characteristics, as described by Rais et al.19 A rare case of left parapharyngeal schwannoma presenting similarly to our patient, however a different approach was described, with a second endo-buccal incision made, as a consequence of the tumour volume and different positioning in the neck area compared to our patient.
These cases accentuate the importance of careful pre-operative planning and meticulous surgical approach, which differs depending on the properties of the tumour. Literature describes similarly presenting patients, yet this case stands out, because of the combination of non-specific symptoms, use of exhaustive identification methods, in-depth pre-operative planning and an anterior approach, most commonly used in cervical spine surgery. This perspective might prove useful for other specialists as an extension of their understanding of this pathology and expand their treatment arsenal accordingly.
Conclusion
This case report describes the successful treatment of a large schwannoma on the anterior aspect of the cervical spine at the C6-C7-Th1 level that produced considerable compression and displacement of the oesophagus, presenting as dysphagia. Key diagnostic steps involved an MRI scan, which served to precisely assess the tumour’s size and location, and a biopsy, which confirmed the tumour’s histology. An anterior surgical approach made it possible to perform a radical gross resection without neurological complications or the need to stabilize the spinal column. Post-operative convalescence was uneventful, and a follow-up MRI scan confirmed complete resection and absence of oesophageal compression. This case report highlights the importance of a comprehensive approach to the diagnosis and treatment and of careful pre-operative planning. The use of magnetic resonance imaging as a key imaging tool and the histological confirmation allowed for early determination of the lesion’s characteristics, which was indispensable in deciding on the treatment to use. In view of the presence of a capsule around schwannomas and the possibility of safely separating these tumours from adjacent structures, surgical resection remains an effective and safe treatment ensuring good therapeutic outcomes.
Abbreviation
MRI, Magnetic Resonance Imaging.
Institutional Review Board Statement
In accordance with local standards, the Institutional Review Board does not require ethical approval or institutional review board approval for reporting individual cases or case series when informed consent is provided by the patient. According to Article 31, Section 2 of the Act on the Professions of Doctor and Dentist, written informed consent was obtained from the patient for the disclosure of information included in this case report.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weber AL, Montandon C, Robson CD. Neurogenic tumors of the neck. Radiol Clin North Am. 2000;38(5):1077–1090. doi:10.1016/s0033-8389(05)70222-0
2. Kanatas A, Mücke T, Houghton D, Mitchell DA. Schwannomas of the head and neck. Oncol Rev. 2009;3(2):107–111. doi:10.1007/s12156-009-0015-6
3. Nikte H, Virmani N, Dabholkar J. Cervical root schwannoma: a case series. Int J Otorhinolaryngol Head Neck Surg. 2016;2(1):43–46. doi:10.18203/issn.2454-5929.ijohns20160069
4. Moukarbel RV, Sabri AN. Current management of head and neck schwannomas. Curr Opin Otolaryngol Head Neck Surg. 2005;13(2):117–122. doi:10.1097/01.moo.0000156172.70521.07
5. Xing MH, Sandler ML, Tuttle RM, et al. Abnormal growth rate of a benign cervical sympathetic chain schwannoma. Otolaryngol Case Rep. 2021;19:100295. doi:10.1016/j.xocr.2021.100295
6. Lubelski D, Pennington Z, Ochuba A, et al. Natural history of brachial plexus, peripheral nerve, and spinal schwannomas. Neurosurgery. 2022;91(6):883–891. doi:10.1227/neu.0000000000002118
7. Alemi AS, Heaton CM, Ryan WR, El-Sayed I, Wang SJ. Volumetric growth of cervical schwannoma as a predictor of surgical intervention. Otolaryngol--Head Neck Surg Off J Am Acad Otolaryngol-Head Neck Surg. 2017;156(1):152–155. doi:10.1177/0194599816669500
8. Propp JM, McCarthy BJ, Davis FG, Preston-Martin S. Descriptive epidemiology of vestibular schwannomas. Neuro-Oncol. 2006;8(1):1–11. doi:10.1215/S1522851704001097
9. Yee TJ, Swong K, Park P. Complications of anterior cervical spine surgery: a systematic review of the literature. J Spine Surg Hong Kong. 2020;6(1):302–322. doi:10.21037/jss.2020.01.14
10. Ahn D, Sohn JH, Kim H, Yeo CK. Large esophageal schwannoma mimicking thyroid tumor with egg-shell calcification on preoperative ultrasonography. Asian J Surg. 2017;40(3):236–239. doi:10.1016/j.asjsur.2014.04.002
11. Ijichi K, Kawakita D, Maseki S, Beppu S, Takano G, Murakami S. Functional nerve preservation in extracranial head and neck schwannoma surgery. JAMA Otolaryngol-- Head Neck Surg. 2016;142(5):479–483. doi:10.1001/jamaoto.2016.0113
12. Biswas D, Marnane CN, Mal R, Baldwin D. Extracranial head and neck schwannomas--a 10-year review. Auris Nasus Larynx. 2007;34(3):353–359. doi:10.1016/j.anl.2007.01.006
13. Kumar N, Tan WLB, Wei W, Vellayappan BA. An overview of the tumors affecting the spine-inside to out. Neuro-Oncol Pract. 2020;7(Suppl 1):i10–i17. doi:10.1093/nop/npaa049
14. Maciejczak A, Gasik R, Kotrych D, et al. Spinal tumours: recommendations of the polish society of spine surgery, the polish society of oncology, the polish society of neurosurgeons, the polish society of oncologic surgery, the polish society of oncologic radiotherapy, and the polish society of orthopaedics and traumatology. Eur Spine J. 2023;32(4):1300–1325. doi:10.1007/s00586-023-07546-2
15. Behuria S, Rout T, Pattanayak S. Diagnosis and management of schwannomas originating from the cervical vagus nerve. Ann R Coll Surg Engl. 2015;97(2):92–97. doi:10.1308/003588414X14055925058355
16. Ku HC, Yeh CW. Cervical schwannoma: a case report and eight years review. J Laryngol Otol. 2000;114(6):414–417. doi:10.1258/0022215001905913
17. Godlewski B, Klauz G, Czepko R. Thoracic nerve root schwannoma filling the spinal canal almost entirely without any neurological deficits. Anesthesiol Pain Med. 2016;6(1):e33886. doi:10.5812/aapm.33886
18. Strong MJ, Yee TJ, Khalsa SSS, et al. Resection of a lumbar intradural extramedullary schwannoma: 2-dimensional operative video. Oper Neurosurg Hagerstown Md. 2021;21(1):E38. doi:10.1093/ons/opab097
19. Rais MA, Naouri Y, Awad AK. A rare case of left parapharyngeal space large schwannoma of unknown origin. J Surg Case Rep. 2023;2023(1):rjac578. doi:10.1093/jscr/rjac578
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.