Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
Laparoscopic spleen-preserving pancreatic resection for epidermoid cyst in an intrapancreatic accessory spleen: case report and literature review
Authors Zhou B ![]() , Zhang Q, Zhan C, Ding Y, Yan S
, Zhang Q, Zhan C, Ding Y, Yan S
Received 14 February 2018
Accepted for publication 6 April 2018
Published 15 May 2018 Volume 2018:14 Pages 937—944
DOI https://doi.org/10.2147/TCRM.S165489
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Bo Zhou,1 Qiyi Zhang,1 Canyang Zhan,2 Yuan Ding,1 Sheng Yan1
1Division of Hepatobiliary and Pancreatic Surgery, Department of Surgery, The First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China; 2Department of Neonatology, Children’s Hospital, School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China
Introduction: An epidermoid cyst in an intrapancreatic accessory spleen (ECIPAS) is a rare non-neoplastic cyst, typically occurring in the pancreatic tail. It is difficult to preoperatively differentiate ECIPAS from other types of pancreatic neoplastic cysts.
Case presentation: We herein report a case of a 32-year-old man with a cystic tumor in the tail of the pancreas. The patient underwent a laparoscopic spleen-preserving distal pancreatectomy, and histological examination revealed the presence of ECIPAS. In addition, we also performed a literature review of 42 case reports of ECIPAS.
Conclusion: Although the preoperative diagnosis of ECIPAS is relatively difficult, familiarity with the imaging features, the clinical presentation and the location of the cyst could lead to a correct preoperative diagnosis of ECIPAS, which might thereby reduce the number of unnecessary resections.
Keywords: epidermoid cyst, accessory spleen, pancreas
Introduction
An epidermoid cyst in an intrapancreatic accessory spleen (ECIPAS) is extremely rare, with the prevalence of 1.7% in general population.1 The differential diagnosis of pancreatic cystic lesions is often challenging because of their similar findings on imaging. It is difficult to preoperatively differentiate ECIPAS from the “other” cystic neoplasms, such as a pancreatic pseudocyst, serous cystic neoplasm, mucinous cystic neoplasm, intraductal papillary mucinous neoplasm and lymphoepithelial cyst, or a solid pancreatic tumor, such as a pancreatic neuroendocrine tumor and solid pseudopapillary tumor, by using conventional imaging. Of the 51 cases of ECIPAS that have been reported in the English literature, only 5 cases were correctly diagnosed based on preoperative imaging.2–43 As ECIPAS is a non-neoplastic pancreatic cyst and has no malignant potential, a correct preoperative diagnosis could thereby reduce the number of unnecessary surgical resections of the pancreas. Herein, we report a case of a 32-year-old male with an ECIPAS and make a comprehensive review of the literature.
Case presentation
A 32-year-old male was admitted to The First Affiliated Hospital with a mass lesion on the pancreatic tail that was detected by abdominal ultrasound during an annual health checkup. No history of trauma or pancreatitis was recorded. He had normal vital signs and abdominal examination. Initial laboratory data also showed no abnormalities, including those for tumor markers such as carcinoembryonic antigen (CEA) or carbohydrate antigen 19-9 (CA19-9). Abdominal computed tomography (CT) revealed a well-defined cystic neoplasm, which was located in the tail of pancreas and approaching to splenic hilum (Figure 1A), without enhancement in the arterial phase (Figure 1B) and the portal phase (Figure 1C). Additionally, endoscopic ultrasonography (EUS) showed a 3.5 cm multilocular cystic lesion in the pancreatic tail with an internal nodule (Figure 1D). The cystic tumor did not communicate with the main pancreatic duct.
 | Figure 1 The abdominal computed tomography (CT) scan confirmed a well-defined cystic neoplasm in the pancreatic tail (A), without enhancement in the arterial phase (B) and the portal phase (C). Endoscopic ultrasonography (EUS) showed a 3.5 cm multilocular cystic lesion in the pancreatic tail with an internal nodule (D). |
Upon diagnosis of mucinous cystic neoplasms, the patient underwent a laparoscopic spleen-preserving distal pancreatectomy. Macroscopic analysis revealed that the mass in the tail of the pancreas was 4 cm at its greatest diameter and consisted of parenchymal and cystic components (Figure 2A). The gross pathology showed a well-demarcated, multilocular mass, containing colorless serous fluid. Microscopic analysis revealed a multilocular cyst surrounded by accessory splenic tissue in the pancreas parenchyma, and the cyst wall showed a thin multilayered squamous epithelium (Figure 2B). The final pathological diagnosis was epidermoid cyst originating from an intrapancreatic accessory spleen. His postoperative course was uneventful and he was discharged 8 days after the surgery.
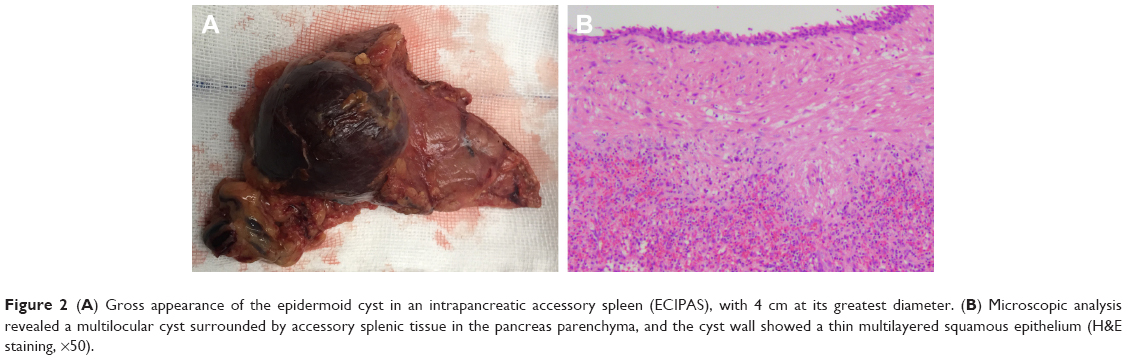 | Figure 2 (A) Gross appearance of the epidermoid cyst in an intrapancreatic accessory spleen (ECIPAS), with 4 cm at its greatest diameter. (B) Microscopic analysis revealed a multilocular cyst surrounded by accessory splenic tissue in the pancreas parenchyma, and the cyst wall showed a thin multilayered squamous epithelium (H&E staining, ×50). |
Ethical approval
The study was approved by the ethics committee of The First Affiliated Hospital of Zhejiang University School of Medicine. Written informed consent was obtained from the patient to have the case details and any accompanying images published.
Discussion
Accessory spleens occur in ~10% of the population and can be found in various anatomic locations other than the splenic hilum. Approximately 20% of accessory spleens occur in or around the tail of the pancreas.1 Epidermoid cysts of the spleen are rare entities, comprising <10% of true non-parasitic splenic cysts.44 An ECIPAS is extremely rare, with only a few reports describing their clinical characteristics. Currently, with the advancement of imaging techniques, such as CT, magnetic resonance imaging (MRI) and EUS, an increasing number of ECIPASs have been detected.
Since Davidson et al2 reported the first case of ECIPAS in 1980, 41 articles and 50 patients have been reported in the English literature (Table 1). Including the present case, 20 cases were men and 32 cases were women. The mean age of the patients was 45.4 years (range 12–70 years), and 32 cases (61.5%) were younger than 50 years. Additionally, >50% of the cases were incidentally detected,6,7,10,12,13,16,17,19–22,24–26,29–31,33,35,39,41–43 while the other symptoms included nausea, vomiting, abdominal pain and discomfort, back pain, epigastric pain and fever. In all cases, the tumors were located on the pancreatic tail. The cyst appeared to be multilocular in 31 cases and unilocular in 14 cases (no information for 7 cases). The average cyst size was 4.3 cm (range 1.4–15 cm). As ECIPAS occurs at a relatively young age and it is located in the pancreatic tail, it is always necessary to differentiate ECIPAS when identifying a pancreatic tail cystic mass in young patients.
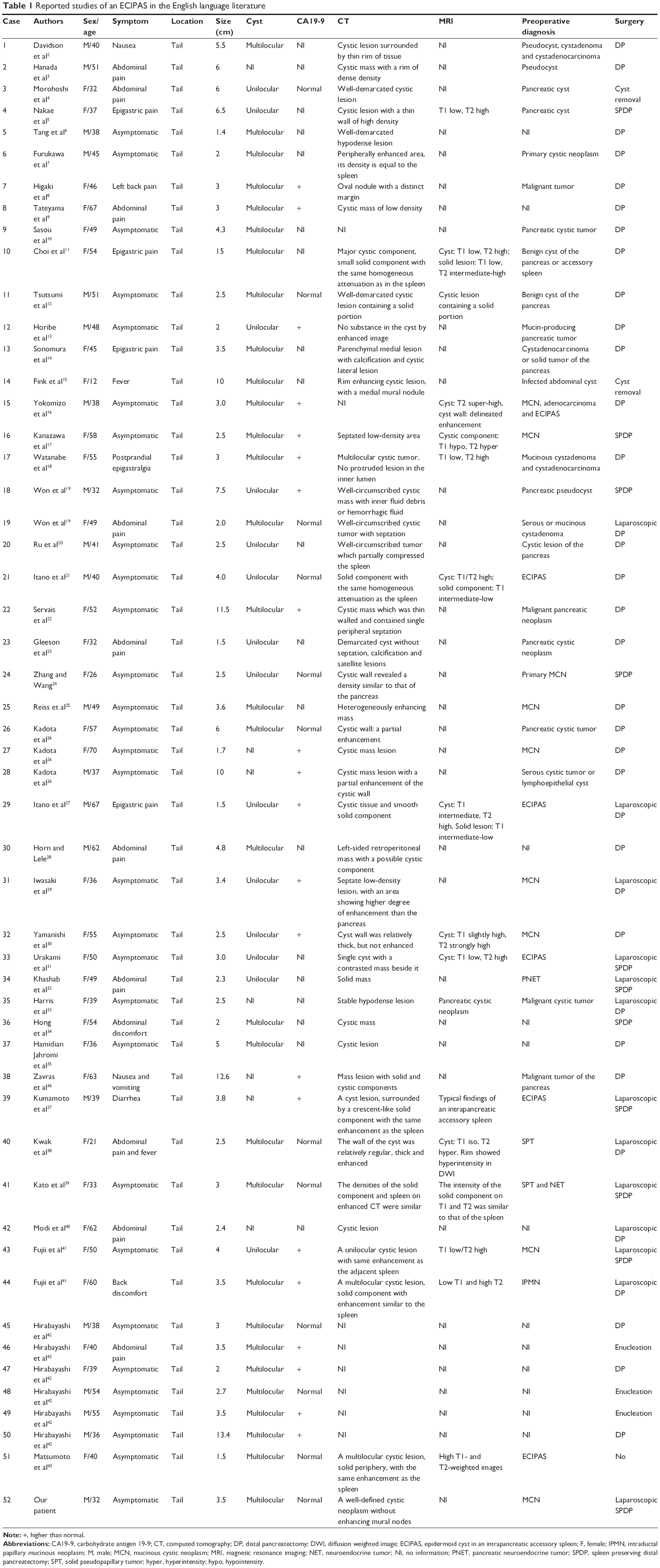 | Table 1 Reported studies of an ECIPAS in the English language literature |
An elevation of serum CA19-9 level was observed in 21 cases,8,9,13,16–19,22,26,27,29,30,36,37,41,42 and hence, it was difficult to preoperatively differentiate between an ECIPAS and pancreatic malignancy during clinical analysis. Higaki et al8 reported that the serum CA19-9 levels markedly decreased to normal levels after surgery in patients diagnosed with an ECIPAS, a result suggesting that the serum CA19-9 might be secreted from the ECIPAS.
Most cases of ECIPAS are diagnosed after surgical resection based on the pathological characteristics. A preoperative imaging diagnosis of an ECIPAS is extremely difficult. Only 5 cases (9.8%) among the 51 reported cases were diagnosed preoperatively, while 1 out of 5 cases correctly diagnosed preoperatively was followed up without resection. Notably, in the present case, abdominal CT and EUS also revealed pancreatic mucinous neoplasm. As there are no characteristic features to define the lesion on radiology, it is difficult to entirely differentiate the cystic pancreatic malignancy prior to surgery and histopathological examination.
Until now, few studies have reported the imaging characteristics of ECIPAS. Hu et al45 noted that an accessory spleen surrounding the cyst was a key component for correct diagnosis, and therefore the relationship of enhancement between the splenic parenchyma and the parenchymal component of the lesion for the differential diagnosis of a cystic mass in the pancreatic tail was important. Itano et al21 described that 8 of 13 cases showed a solid tumor component upon CT or MRI, and several reports mentioned retrospectively that the images of the solid component were similar to those of the spleen. In our review, a diagnosis of a mucinous cystadenoma, cystadenocarcinoma, pseudocyst, neuroendocrine tumor or a potential malignant tumor was suspected in most cases.21 Interestingly, 3 out of 52 cases were diagnosed as ECIPAS preoperatively based on the similar density in the solid component and spleen on CT or MRI.21,37,43 Furthermore, Motosugi et al46 suggested that superparamagnetic iron oxide-based (SPIO) MRI was the most reliable tool for identifying an ECIPAS, because reticuloendothelial tissues including spleen took up SPIO and the signal intensity of the tissues changes (drops). Unfortunately, our patient did not receive MRI examination preoperatively. All the findings suggest that, in the presence of a relatively large amount of splenic tissues, a correct diagnosis would be possible based on a careful examination of images prior to surgery. However, relatively small amounts of splenic tissues may not be useful in the diagnosis. Therefore, ECIPAS should be considered in the differential diagnosis of pancreatic cystic lesions.
Until now, the treatment of ECIPAS consists of follow-up and surgical removal, including open or laparoscopic surgery with or without splenic preservation. No death has been reported during operation or in the short-term postoperative period. Fujii et al41 suggested that laparoscopic distal pancreatectomy could be a useful, minimally invasive surgical approach for treating pancreatic cysts as well as for the treatment of benign or low-grade malignant tumors located in the pancreatic body or tail. As ECIPAS was reported not to have malignant potential, a correct preoperative diagnosis could thereby avoid unnecessary surgery.
Conclusion
An ECIPAS is an extremely rare disease entity. Enhancing the cystic wall of ECIPAS similar to the spleen was a helpful feature. To prevent any unnecessary surgical intervention, it is important to recognize the ECIPAS as the differential diagnosis of pancreatic cyst. Familiarity with the imaging features, the clinical presentation and the location of the cyst will help radiologists make a more confident diagnosis. Thus, making a definite preoperative diagnosis in most cases is possible.
Acknowledgments
This work was supported by grants from the General Research Projects of the Department of Education of Zhejiang Province (No Y201737812), Zhejiang Province Department of Laboratory Animal Science and Technology Plan Projects (No 2018C37115), and Key Research and Development Project of Science and Technology Department of Zhejiang Province (No 2015C03053).
Disclosure
The authors report no conflicts of interest in this work.
References
Halpert B, Alden ZA. Accessory spleens in or at the tail of the pancreas. a survey of 2,700 additional necropsies. Arch Pathol. 1964;77:652–654. | ||
Davidson ED, Campbell WG, Hersh T. Epidermoid splenic cyst occurring in an intrapancreatic accessory spleen. Dig Dis Sci. 1980;25(12):964–967. | ||
Hanada M, Kimura M, Kitada M, Nakajima T, Yamada K, Yoshii M. Epidermoid cyst of accessory spleen. Acta Pathol Jpn. 1981;31(5):863–872. | ||
Morohoshi T, Hamamoto T, Kunimura T, et al. Epidermoid cyst derived from an accessory spleen in the pancreas. A case report with literature survey. Acta Pathol Jpn. 1991;41(12):916–921. | ||
Nakae Y, Hayakawa T, Kondo T, et al. Epidermoid cyst occurring in a pancreatic accessory spleen. J Clin Gastroenterol. 1991;13(3):362–364. | ||
Tang X, Tanaka Y, Tsutsumi Y. Epithelial inclusion cysts in an intrapancreatic accessory spleen. Pathol Int. 1994;44(8):652–654. | ||
Furukawa H, Kosuge T, Kanai Y, Mukai K. Epidermoid cyst in an intrapancreatic accessory spleen: CT and pathologic findings. AJR Am J Roentgenol. 1998;171(1):271. | ||
Higaki K, Jimi A, Watanabe J, Kusaba A, Kojiro M. Epidermoid cyst of the spleen with CA19-9 or carcinoembryonic antigen productions: report of three cases. Am J Surg Pathol. 1998;22(6):704–708. | ||
Tateyama H, Tada T, Murase T, Fujitake S, Eimoto T. Lymphoepithelial cyst and epidermoid cyst of the accessory spleen in the pancreas. Mod Pathol. 1998;11(12):1171–1177. | ||
Sasou S, Nakamura S, Inomata M. Epithelial splenic cysts in an intrapancreatic accessory spleen and spleen. Pathol Int. 1999;49(12):1078–1083. | ||
Choi SK, Ahn SI, Hong KC, et al. A case of epidermoid cyst of the intrapancreatic accessory spleen. J Korean Med Sci. 2000;15(5):589–592. | ||
Tsutsumi S, Kojima T, Fukai Y, et al. Epidermoid cyst of an intrapancreatic accessory spleen – a case report. Hepatogastroenterology. 2000;47(35):1462–1464. | ||
Horibe Y, Murakami M, Yamao K, Imaeda Y, Tashiro K, Kasahara M. Epithelial inclusion cyst (epidermoid cyst) formation with epithelioid cell granuloma in an intrapancreatic accessory spleen. Pathol Int. 2001;51(1):50–54. | ||
Sonomura T, Kataoka S, Chikugo T, et al. Epidermoid cyst originating from an intrapancreatic accessory spleen. Abdom Imaging. 2002;27(5):560–562. | ||
Fink AM, Kulkarni S, Crowley P, Crameri JA. Epidermoid cyst in a pancreatic accessory spleen mimicking an infected abdominal cyst in a child. AJR Am J Roentgenol. 2002;179(1):206–208. | ||
Yokomizo H, Hifumi M, Yamane T, et al. Epidermoid cyst of an accessory spleen at the pancreatic tail: diagnostic value of MRI. Abdom Imaging. 2002;27(5):557–559. | ||
Kanazawa H, Kamiya J, Nagino M, et al. Epidermoid cyst in an intrapancreatic accessory spleen: a case report. J Hepatobiliary Pancreat Surg. 2004;11(1):61–63. | ||
Watanabe H, Yamaguchi Y, Ohtsubo K, et al. Epidermoid cyst of the intrapancreatic accessory spleen producing CA 19-9. Dig Endosc. 2004;16(3):244–248. | ||
Won JK, Lee YJ, Kang GH. Epithelial cysts in the intrapancreatic accessory spleen that clinically mimic pancreatic cystic tumor. Korean J Pathol. 2005;39:437–441. | ||
Ru K, Kalra A, Ucci A. Epidermoid cyst of intrapancreatic accessory spleen. Dig Dis Sci. 2007;52(5):1229–1232. | ||
Itano O, Shiraga N, Kouta E, et al. Epidermoid cyst originating from an intrapancreatic accessory spleen. J Hepatobiliary Pancreat Surg. 2008;15(4):436–439. | ||
Servais EL, Sarkaria IS, Solomon GJ, Gumpeni P, Lieberman MD. Giant epidermoid cyst within an intrapancreatic accessory spleen mimicking a cystic neoplasm of the pancreas: case report and review of the literature. Pancreas. 2008;36(1):98–100. | ||
Gleeson FC, Kendrick ML, Chari ST, Zhang L, Levy MJ. Epidermoid accessory splenic cyst masquerading as a pancreatic mucinous cystic neoplasm. Endoscopy. 2008;40(suppl 2):E141–E142. | ||
Zhang Z, Wang JC. An epithelial splenic cyst in an intrapancreatic accessory spleen. A case report. JOP. 2009;10(6):664–666. | ||
Reiss G, Sickel JZ, See-Tho K, Ramrakhiani S. Intrapancreatic splenic cyst mimicking pancreatic cystic neoplasm diagnosed by EUS-FNA. Gastrointest Endosc. 2009;70(3):557–558. | ||
Kadota K, Kushida Y, Miyai Y, et al. Epidermoid cyst in an intrapancreatic accessory spleen: three case reports and review of the literatures. Pathol Oncol Res. 2010;16(3):435–442. | ||
Itano O, Chiba N, Wada T, et al. Laparoscopic resection of an epidermoid cyst originating from an intrapancreatic accessory spleen: report of a case. Surg Today. 2010;40(1):72–75. | ||
Horn AJ, Lele SM. Epidermoid cyst occurring within an intrapancreatic accessory spleen. A case report and review of the literature. JOP. 2011;12(3):279–282. | ||
Iwasaki Y, Tagaya N, Nakagawa A, et al. Laparoscopic resection of epidermoid cyst arising from an intrapancreatic accessory spleen: a case report with a review of the literature. Surg Laparosc Endosc Percutan Tech. 2011;21(5):e275–e279. | ||
Yamanishi H, Kumagi T, Yokota T, et al. Epithelial cyst arising in an intrapancreatic accessory spleen: a diagnostic dilemma. Intern Med. 2011;50(18):1947–1952. | ||
Urakami A, Yoshida K, Hirabayashi Y, et al. Laparoscopic-assisted spleen preserving pancreatic resection for epidermoid cyst in an intrapancreatic accessory spleen. Asian J End Surg. 2011;4(4):185–188. | ||
Khashab MA, Canto MI, Singh VK, Hruban RH, Makary MA, Giday S. Endosonographic and elastographic features of a rare epidermoid cyst of an intrapancreatic accessory spleen. Endoscopy. 2011;43(suppl 2 UCTN):E193–E194. | ||
Harris AC, Chaudry MA, Menzies D, Conn PC. Laparoscopic resection of an epidermoid cyst within an intrapancreatic accessory spleen: a case report and review article. Surg Laparosc Endosc Percutan Tech. 2012;22(4):e246–e249. | ||
Hong R, Choi N, Sun K, Lim S, Han Y. Epidermoid cyst arising from an intrapancreatic accessory spleen: a case report and review of the literature. Oncol Lett. 2013;5(2):469–472. | ||
Hamidian Jahromi A, Fallahzadeh MK, Dela Cruz N, Chu Q. Epidermoid cyst arising from an intrapancreatic accessory spleen: a case report and a review of the literature. J La State Med Soc. 2013;165(3):153–156. | ||
Zavras N, Machairas N, Foukas P, Lazaris A, Patapis P, Machairas A. Epidermoid cyst of an intrapancreatic accessory spleen: a case report and literature review. World J Surg Oncol. 2014;12:92. | ||
Kumamoto Y, Kaizu T, Tajima H, Kubo H, Nishiyama R, Watanabe M. A rapidly growing epidermoid cyst in an intrapancreatic accessory spleen treated by laparoscopic spleen-preserving distal pancreatectomy: report of a case. Int Surg. Epub 2015 Jun 2. | ||
Kwak MK, Lee NK, Kim S, et al. A case of epidermoid cyst in an intrapancreatic accessory spleen mimicking pancreas neoplasms: MRI with DWI. Clin Imaging. 2016;40(1):164–166. | ||
Kato S, Mori H, Zakimi M, et al. Epidermoid cyst in an intrapancreatic accessory spleen: case report and literature review of the preoperative imaging findings. Intern Med. 2016;55(23):3445–3452. | ||
Modi RM, Kamboj AK, Swanson B, Conwell DL, Krishna SG. Epidermoid cyst within an intrapancreatic accessory spleen: endosonography and confocal endomicroscopy of an unusual pancreatic cystic lesion. Endoscopy. 2016;48(S 01):E332–E333. | ||
Fujii M, Yoshioka M, Shiode J. Two cases of an epidermoid cyst developing in an intrapancreatic accessory spleen identified during laparoscopic distal pancreatectomy. Intern Med. 2016;55(21):3137–3141. | ||
Hirabayashi K, Yamada M, Kono H, et al. Epidermoid cysts are a characteristic feature of intrapancreatic but not of extrapancreatic accessory spleens. Virchows Arch. 2017;471(1):91–98. | ||
Matsumoto K, Kato H, Okada H. Epidermoid cyst in an intrapancreatic accessory spleen diagnosed by typical radiographic images and endoscopic ultrasound fine-needle aspiration findings with contrast agent. Clin Gastroenterol Hepatol. 2018;16:e13–e14. | ||
Robbins FG, Yellin AE, Lingua RW, Craig JR, Turrill FL, Mikkelsen WP. Splenic epidermoid cysts. Ann Surg. 1978;187(3):231–235. | ||
Hu S, Zhu L, Song Q, Chen K. Epidermoid cyst in intrapancreatic accessory spleen: computed tomography findings and clinical manifestation. Abdom Imaging. 2012;37(5):828–833. | ||
Motosugi U, Yamaguchi H, Ichikawa T, et al. Epidermoid cyst in intrapancreatic accessory spleen: radiological findings including superparamagnetic iron oxide-enhanced magnetic resonance imaging. J Comput Assist Tomogr. 2010;34(2):217–222. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.