Back to Journals » Psychology Research and Behavior Management » Volume 7
Language of motivation and emotion in an Internet support group for smoking cessation: explorative use of automated content analysis to measure regulatory focus
Authors Johnsen JK, Vambheim SM ![]() , Wynn R
, Wynn R ![]() , Wangberg S
, Wangberg S
Received 25 September 2013
Accepted for publication 20 November 2013
Published 15 January 2014 Volume 2014:7 Pages 19—29
DOI https://doi.org/10.2147/PRBM.S54947
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Jan-Are K Johnsen,1 Sara M Vambheim,2 Rolf Wynn,3,4 Silje C Wangberg3,5
1Department of Clinical Dentistry, University of Tromsø, 2Department of Psychology, University of Tromsø, 3Division of Addiction and Specialized Psychiatry, University Hospital of North-Norway, 4Department of Clinical Medicine, University of Tromsø, Tromsø, 5Narvik University College, Narvik, Norway
Abstract: The present study describes a novel approach to the identification of the motivational processes in text data extracted from an Internet support group (ISG) for smoking cessation. Based on the previous findings that a “prevention” focus might be more relevant for maintaining behavior change, it was hypothesized that 1) language use (ie, the use of emotional words) signaling a “promotion” focus would be dominant in the initiating stages of the ISG, and 2) that the proportion of words signaling a prevention focus would increase over time. The data were collected from the ISG site, spanning 4 years of forum activity. The data were analyzed using the Linguistic Inquiry and Word Count application. The first hypothesis – of promotion focus dominance in the initiating stages – was not supported during year 1. However, for all the other years measured, the data showed that a prevention failure was more dominant compared with a promotion failure. The results indicate that content analysis could be used to investigate motivational and language-driven processes in ISGs. Understanding the interplay between self-regulation, lifestyle change, and modern communication channels could be of vital importance in providing the public with better health care services and interventions.
Keywords: self-regulation, behavior change, emotion, prevention
Introduction
It is of major interest to understand the underlying processes of behavior change and the maintenance of behavior change, and how successful change and the maintenance of change can be modified by information from, participation in, and guidance provided by Internet support groups (ISGs). ISGs can provide researchers with unique data, for instance through the storage of text-data from user communication, to support insight into the processes related to behavior change.1
In general, the Internet may be an excellent tool for the establishment, maintenance, and extension of a social network, regardless of spatial or temporal constraints.2 Many relationships formed online will be extended to “real life” and may also develop higher levels of intimacy faster than will relationships formed offline.3 The Internet facilitates the search for others sharing specific interests, while also gathering diverse people that would not otherwise interact.4 From an individual perspective, ISGs might be used to improve participants’ health, through access to professional health information as well as through sharing of peer experiences of health services, treatments and symptoms.5–7 Indeed, ISGs are growing in popularity and use among people suffering from different illnesses or problems, physical as well as mental. These groups, unlike their real-life counterparts, provide access to information and social interaction 24 hours a day. A previous study has suggested that making use of these sites may help individuals improve their knowledge and coping skills regarding their condition.8 For instance, studies of women with breast cancer have shown that their participation in ISGs connected the women with resources about cancer,9 led to the participants feeling better informed,10 and positively affected their perception of pain and possibly, pain management and control,11,12 although it did not affect survival rates.11 It is worth noting that participation in ISGs first and foremost appears to be related to nonspecific and personal effects, rather than specific health outcomes.13
Similarly, Christakis and Fowler14 and Fowler and Christakis15 have shown how important social networks can be for smoking cessation. They found that social ties, be it to a spouse, sibling, neighbor, friend, or coworker, strongly predict smoking status. Furthermore, they found strong clustering effects, which suggest that smoking cessation spreads throughout these social networks and increases the chances of the entire cluster continuing to smoke or not. This supports the idea that the decision to quit smoking is not merely a personal decision but might also reflect the choices of many interconnected individuals.
The inclusion of ISGs as a smoking cessation intervention is related to the general impact of social influence/peer leader approaches in tobacco prevention interventions and the related work on the influence of social networks.16,17 The notion guiding these interventions has been that teaching “resistance” skills (to help maintain behavior change) within the context of a peer relationship is important since peers, in general, appear to influence health behaviors among children and adolescents,18 including behaviors relating to tobacco use.19 Peer influence should also affect adults, although the effects might be less pronounced.20 The dynamics of group-based social support or peer influence is not well understood; however, these influences could work through norm development or peer modeling to influence the regulation of behavior. ISGs give users the chance to identify others who have successfully overcome barriers for smoking cessation or others who may be modeling the new desired role of a nonsmoker – this information is not necessarily available in ordinary social networks. If indeed, smoking cessation ISGs have been successful in influencing behavior through processes such as norm development or peer modeling, these processes should be detectable through an analysis of the communications between users in the network. The question then is to decide how to analyze the communication and which variables to measure. This study focused on self-regulation theory, as self-regulation of behavior has been used as the theoretical model for a wide variety of behavior change interventions and other studies of health behavior.21–24 A prior study examining smoking cessation found that self-efficacy beliefs were of importance to smoking-cessation rates, thus suggesting that self-regulation mechanisms are of importance to the success of smoking-cessation interventions.25
Self-regulation theory is often used to explain and predict goal-directed behavior and is essential in the appropriate implementation of new behaviors, such as smoking cessation (eg, coping skills).26 Interventions targeting smoking cessation have shown an effect on quit rates, but many participants seem to relapse within 6 months following the end of treatment.26 Hence, the understanding of how to maintain new behaviors over longer periods of time should be prioritized. Importantly, the goals related to either the process of quitting or the process of abstaining from smoking might be quite different and can be related to a specific theoretical approach to self-regulation.
Regulatory Focus Theory (RFT)27,28 distinguishes between two types of motivational regulation: promotion and prevention. Promotion places emphasis on desires and potential goals, whereas prevention places an emphasis on obligations and potential losses.29–32 A successful performance of meaningful behaviors over time appears to be related to the fit between the behavioral task and the regulatory focus,33 and regulatory focus has been shown to be an influential variable, in research on smoking cessation interventions as well as in other studies investigating lifestyle changes.34 Interestingly, although individuals might have an inherent disposition towards either promotion or prevention, research also shows that the regulatory focus could be activated momentarily by extraneous sources.35,36 For instance, studies of the framing of message content (eg, positive or negative outcomes) impacted the emotional and motivational systems related to Self-Discrepancy Theory (SDT).27,35 In other words, the message frame and its impact on the individual’s mindset might be highly relevant to understand how people go about behavior change. Whereas a mindset of challenging tasks and eager pursuit of positive end states (promotion) might be related to the initiation of behavioral change (eg, quitting smoking, dieting, etc.), the maintenance of new behaviors over time might be related to the preservation of desired end-states by avoiding losses (prevention). The findings of Fuglestad et al34 supported this notion for smoking cessation and weight loss interventions. In their work, a promotion focus predicted greater success in the initiation of behavior change (6 months), while a prevention focus predicted the long-term maintenance of new, healthy behaviors. Many health behaviors might thus be understood through the concept of regulatory focus and through the processes related to regulatory fit. Regulatory focus also appears to be related to the strategies utilized during behavior-related judgment, with promotion focus associated with affective processing and prevention focus associated with evaluative reasoning.37 All these have potential consequences for initiating and maintaining behavior change.
Interestingly, compared with the traditional ways of delivering health interventions, the unique context of information and communication technologies could represent a wider “message frame,” where relevant motivation could be drawn from the shared experiences of participants. Cognitive Dissonance Theory38 and Self-Perception Theory39 argue that verbalizing arguments for change is associated with a higher likelihood of successful behavior change, whereas verbalizing against change is associated with lower likelihood of successful behavior change. Research directed at addressing these issues has used methods specifically designed to tap into these experiences. In text-based contexts, perhaps the most direct approach is an analysis of the discourse.
Analysis of the data collected from ISGs could thus provide important information about the experiences and mindsets of participants. Analyzing what people talk about, for instance, through content analysis, is a relevant technique for accomplishing this, and both qualitative and quantitative content analyses have been used in studies of online health communication.40,41 It is valid to assume that communication in ISGs should reflect behavioral and/or cognitive experiences. Understanding the interplay between emotion and motivation occurring in health-related ISGs is central to a prediction of the behavior change that will occur. Since RFT has been used in investigations of smoking cessation, we chose to study whether the distinct dimensions of RFT – promotion versus prevention – could be inferred from ISG discourse, using content analysis. Previously, promotion focus and prevention focus have both been identified with experiences of distinct emotions;42,43 thus, we hypothesized it should be possible to infer these dimensions from the emotional content of ISG interaction.
Whether an intervention works is important but investigating how an intervention works is just as important. This study’s goal was to address the underlying processes in smoking cessation, as represented by language use and changes in language use over time. This study set out to 1) explore whether text data collected from an ISG targeting smoking cessation could be analyzed with regard to emotional words signifying promotion and prevention focus; and to 2) distinguish changes over time, which we proposed to be related to the initiation of quitting smoking and to subsequent maintenance of the behavior change. This was supported by findings related to regulatory focus and smoking cessation.34 Thus, we hypothesized that 1) language use signaling a promotion focus (emotional words) would be dominant in the initiating stages of the social network and that 2) the proportion of words signaling a prevention focus would increase over time. Also, we explored the change in the nonspecific emotional content over time, although no precise predictions could be made concerning emotional content (positive or negative emotions).
Material and methods
Slutta.no (http://slutta.no/) is a free, Internet-based, interactive smoking cessation program developed by The Norwegian Cancer Society, the software company PMAB (Preventive Media AB, Stockholm, Sweden), The Norwegian Centre for Integrated Care and Telemedicine, and the Norwegian Directorate for Health. The intervention website was announced in both local and national Norwegian media as a free service to aid in smoking cessation.
The site has since been updated, but in the period when the data were sampled, the site offered tailored information about the health risks related to smoking, the benefits of quitting smoking, and advice on how to resist the temptation to smoke, and it also offered social support to people struggling with smoking cessation. Registered users could engage in forum participation, where they could define, describe, and discuss experiences related to smoking and smoking cessation, and could also provide support. Because we wanted to study the activity of the ISG in a naturalistic manner, external interference (eg, moderation) was kept to a minimum. However, one of the authors had a role as a moderator, mainly for answering practical questions. The discussion forum of the ISG was reachable by a link on the front page of the website. No instructions were given for the use of the forum. In addition, each user had an individual profile, and other people were able to access the user profile in order to read about the user, to read the user’s diary, or leave a message in the user’s guestbook. The current study extracted data from the discussion forum of the online smoking cessation intervention. All posts from August 15, 2006 to July 3, 2009 were selected for analysis. Data from slutta.no was collected from a total number of 7,906 registered users, 71% female and 29% male. The mean age of participants was 36.45 years. When analyzed, the forum consisted of a total of 5,242 web pages, each containing a single discussion thread. There was a significant change in the activity throughout the study period, as measured by the word count. The number of words throughout the study period increased from 204,023 words in the first year to 960,240 words in the final year.1 The study was approved by the Regional Medical Ethics Committee for North Norway (approval number REK Nord 83/2005). Participants gave written informed consent when joining the forum. The participants could choose nicknames for their forum participation, allowing users to be known to each other by nickname. All the data were made anonymous when sampled for the study.
The message threads were converted from html format to text format, using HTMLasText (http://nirsoft.net/). The posts were analyzed by the Linguistic Inquiry and Word Count (LIWC2007).44 The LIWC2007 is a computer-based text analysis tool that calculates the degree to which different categories of words are present in text materials. The LIWC has previously been validated as a method for measuring verbal expression of emotion.45 The LIWC2007 utilizes dictionaries available in several languages, and a Norwegian translation of the LIWC2007 dictionary was used for all the analyses. The LIWC2007 dictionary defines several sets of word categories, and enables the user to measure how many times a particular word is used in a piece of text as well as the proportion (percentage) of the measured word categories in the complete text.
The promotion focus and prevention focus were measured by adding two specific sets of emotional words to the LIWC2007 dictionary. These words were chosen based on studies linking promotion versus prevention focus with the emotions “Agitation” and “Dejection.”27,29,43 This work-intensive and central process spanned several steps.
First, items were amassed based on the 12 affective items used by Roese et al43 to assess the dimensions of Dejection–Elation (promotion) and Agitation–Quiescence (prevention). For Dejection–Elation the words were: happy, satisfied, cheerful, disappointed, discouraged, and sad; for Agitation−Quiescence, these were: calm, quiet, serene, afraid, agitated, and uptight. These dimensions were treated as different emotional states, which signal either success or failure in task completion relative to the regulatory focus of an individual. Only the three negative concepts from each dimension (Agitation and Dejection) were selected, which was similar to the approach taken by Roese et al.43 Reducing the heterogeneity of the dimensions ensured that they included items that were equally used in natural language (ie, to avoid that differences were due to positive language being more common than negative language) and also minimized the risk that changes in nonspecific emotions over time would impact these findings (ie, that more positive words were used as the forum developed). Norwegian translations and approximations to these items were used, and synonyms were added using a current Norwegian dictionary.
Second, the dimensions were balanced with regards to the number of items included in each dimension. This resulted in two initial dimensions of approximately 40 items each.
Third, the dimensions were analyzed descriptively using a random sample of 1,228 threads. Words that were not used at all in this sample were removed from the dictionary. This process was then repeated and the dimensions were “balanced” with regard to the number of items. The resulting dictionary contained 20 items for Dejection, and 18 items for Agitation (Table S1). The following are examples of texts from the sampled material that were high in either Dejection or Agitation:
Dejection (disappointed, discouraged, sad)
Subject: Tired of smoking
I feel that I am tired of smoking, it does not taste good, but I am still smoking a lot. Wondering if I should quit immediately before my quit-date, but that thought often appears when I am smoking, and then after a while I will get another one. …When I read these pages I see there are many positive, motivating factors. Does anyone have any suggestions about what to do?
Subject: Failed, and I am sorry…
…I have failed horribly today, and I am really very sorry. I got very tired of the constant craving, and stopped chewing nicotine gum, which made everything much worse! Finally, I gave in and I have probably smoked 10 cigarettes today. But it feels really bad now. Does this mean it was all for nothing?
Agitation (afraid, agitated, uptight)
Subject: I am scared!
I am afraid I will not be able to quit smoking. I think about it every time I smoke a cigarette or think about cigarettes. I would like to quit but I keep thinking about the negatives and not the positives. This will not be easy.
Subject: Chronic pulmonary disease
[Response] I am too scared to look at that link. I am afraid that I have become ill from all this smoking, and this is the first time I have really felt how scared I am.
Because Agitation and Dejection had been constructed as mutually exclusive dimensions, there was a chance that these would exhibit dependence within each time period, as LIWC scores are mean percentage scores. However, due to the very high number of words per year and the high specificity of the regulatory focus dimensions (ie, low percentage scores for each dimension), this possibility was regarded as negligible.
The validity of the prevention failure (Agitation) and promotion failure (Dejection) constructs was investigated primarily by looking at the correlations with other variables from the LIWC analysis as both constructs should be associated with constructs that represented negative emotional content. Agitation and Dejection appeared to be equally related to the LIWC “Negative” emotion dimension (r=0.10 and 0.08, P<0.05). Also, the correlations with the LIWC “Positive” emotion dimension were nonsignificant (Agitation, r=−0.02; Dejection, r=0.01; P>0.05, ns). In keeping with other work on regulatory focus,46 the Dejection (promotion) and Agitation (prevention) dimensions were positively but modestly correlated (r=0.06, P<0.05).
The statistical analyses were performed using Statistica 7.0 (StatSoft, Tulsa, OK, USA). Parametric tests were used, corresponding to other studies using LIWC.47,48
Results
Regulatory focus
The research hypotheses related to the development of the Agitation and Dejection dimensions were investigated by analysis of variance (ANOVA) and planned comparisons. An ANOVA was performed, with Agitation and Dejection as dependent, within-subject variables and time as an independent variable (Figure 1). The analysis yielded a significant main effect of time, with fewer regulatory focus items being used as time progressed, F(3, 5238)=4.41 (P<0.01). A main effect was found for Agitation and Dejection items overall, F(1, 5238)=40.11 (P<0.00001), with Agitation words being used more frequently than Dejection words. However, the interaction effect between Agitation and Dejection over time was not significant, F(3, 5238)=1.63, P=ns. Planned comparisons between the mean number of Agitation and Dejection words were performed for each year, to specifically test our two hypotheses (Table 1). The analyses showed that mean Agitation scores were significantly higher than the Dejection scores for years 2–4 (in support of the second hypothesis that prevention words would be more common in the forum over time), but no significant difference was found for year 1 (disproving the first hypothesis that promotion words would be more common during the initiation of forum activity).
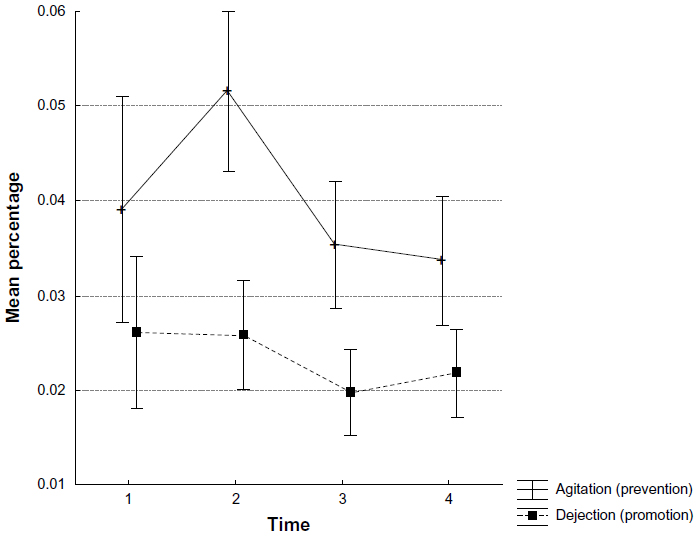 | Figure 1 Mean incidence of Agitation- and Dejection-related words over the 4 years of forum activity. |
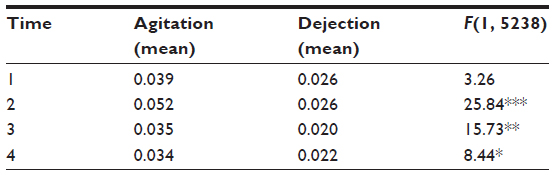 | Table 1 Contrast analysis for Agitation and Dejection means for years 1−4 |
Emotional content
In addition to the analyses of the custom-made dimensions of Agitation and Dejection, we used the predefined LIWC dimensions of Positive and Negative emotions to investigate the development of emotional content over time. ANOVA tests were run for the Positive and Negative dimensions (dependent variables) with time as an independent variable. The results showed a main effect of Negative emotions over time, F(3, 5238)=13.61 (P<0.00001), signifying a decrease in the use of negative emotional words over time. Also, a main effect was found for Positive emotions over time, F(3, 5238)=23.28 (P<0.0001). Thus, the use of positive emotional words increased over time.
Discussion
The results gave only partial support for the research hypotheses. The Dejection-related words, signaling a promotion focus (failure), were not more frequent in the early stages (year 1) of forum communication, as hypothesized. However, the results showed that the Agitation-related words, signaling a prevention focus (failure), were more dominant than promotion failure emotions for all the other years. This indicates that the content related to prevention failure was more frequently found in this smoking cessation setting, and suggests that a prevention focus might be a central mindset for individuals when preoccupied with behavioral change over time.34 Overall, the results showed that the proportion of nonspecific negative-emotion words decreased over time, while positive emotions increased over time. Thus, communication about smoking cessation became more positive over time.
To our knowledge, similar findings related to ISGs have not been reported previously, although the relationship between regulatory focus approaches and the success of various lifestyle interventions are relatively well documented. Matching the content or strategies of smoking cessation intervention to individuals’ tendencies towards either a promotion or a prevention focus has proven effective in increasing the efficiency of the intervention. In a study of antismoking advertisements, Zhao and Pechman49 were able to show that adolescents’ intentions not to smoke were positively influenced by the campaign when the campaign’s content was matched to their regulatory focus. This held true for either promotion or prevention focus. In essence, this constitutes ensuring regulatory fit between the strategies, behaviors, and cognitions included or inferred by an intervention, and the current mindset of the intervention recipient. People that experience regulatory fit feel right about what they do.50 This may be associated with the experience of motivation intensity, prospective feelings about future choices, and retrospective evaluations of past decisions.51 For instance, health information that fits with a recipients’ regulatory focus is more readily evaluated as valid and perceived as more easily processed.52 Also, the described health benefits to an intervention are regarded as more believable and desirable.50
Similarly, while regulatory fit might make an intervention more attractive and effective due to the participants “feeling right,” the lack of regulatory fit might make a health intervention less effective and/or attractive to participants when it does not “feel right.” Having a promotion or prevention focus might not be equally well-suited strategies for maintaining long-term behavior. Findings have linked a promotion and prevention focus, respectively, to different endpoints along several psychologically relevant dimensions. These include creativity versus self-control,53 change versus stability,54 and fun/enjoyment versus safety/security.55 The topic of this particular study, smoking cessation, might be said to lean towards the prevention side of these dichotomies (eg, self-control, stability, and safety/security). Perceived temporal qualities related to either initiating quitting or maintaining abstinence might be related to the regulatory focus. For instance, people seem to prefer products or offers that will help them prevent negative outcomes when the event is near, and promote positive outcomes when the event is distant.56 This might imply that promotion motivates the initiation of new behavior (towards a distant goal), whereas prevention is motivated by the threat of failure when a new behavior has been initiated. If we propose that a specific type or direction of behavior change is required or better suited to achieve lifestyle and health goals, this might pose a challenge with regard to the notion of regulatory fit. The question will then not be how to reach participants with a congruent regulatory focus but rather, how to reach those with an incongruent focus. Accommodation of both types could be attempted through computer-assisted tailoring techniques that seek to frame the intervention information and/or procedures in line with the participants’ motivational inclinations or that seek to induce an alternative motivational focus. Techniques to temporarily influence regulatory focus have been described related to consumer research.57
With regard to the finding of changes in nonspecific emotional content, the implications of these findings are not clear. While this suggests that communication related to smoking cessation became more positive, it cannot be concluded that this was associated with behavior change. Specifically, the assumption that users were communicating more positively because they were experiencing success with regard to smoking cessation might not hold. However, the value of emotional content in this respect should not be disregarded, as several studies have examined the health consequences of emotional expression. For instance, repression of negative emotions was associated with higher levels of anxiety, depression, and confusion in patients diagnosed with breast cancer compared with breast cancer patients who expressed their emotions.58 Other studies have shown that feelings of weakness, helplessness, lowered physical health, and quality of life can be attributed to the suppression of emotions.59–61 Petrie et al showed that the suppression of emotions led to physiological effects that in the long run could cause unfortunate changes in immune response.48
Studies have shown that a positive health outcome is associated with a high use of positive-emotion words, moderate use of negative-emotion words, and an increase in insight and causation words.62,63 One possible explanation of the observed linguistic patterns is that affective and cognitive attributions were changed and organized in a different and more advantageous way (ie, beneficial for health).47 Interestingly, the experience of positive emotions appears to be related to whether people will accept health risk communicated through interventions or advertisements – for instance, a series of experiments indicated that people experiencing positive moods had resources available to process aversive information concerning health, whereas people in negative moods did not have such resources available and were instead, engaged in mood repair.64 Negative emotions in this context can be caused by the communication scenarios and message, or be purely incidental. This is interesting since recent behavior change campaigns have focused on very aversive and negative consequences of certain behaviors (eg, smoking). If interventions such as the smoking cessation ISG have an actual effect on the mood of the participants, it might be argued that participation could encourage processing of aversive health information related to smoking by positively affecting the mood of the participants. ISGs, in health behavior interventions, could thus function as a potential venue for the provision of information concerning health risk.
Since this study used anonymous data, the mechanisms responsible for the changes over time cannot be identified precisely. However, there are several relevant theories that might explain the change processes in virtual groups. For instance, Parks65 described defining criteria for groups that function as communities. Concepts such as “collective action” and “patterned interaction” appear to be central to an understanding of virtual communities. Also, the “hyperpersonal perspective” on computer-mediated communication proposed by Walther66,67 is interesting to any investigation of virtual groups since this perspective focuses on the adaptive and selective uses of media, for instance, through linguistic behaviors as means of uncertainty reduction,66–68 making analyses of linguistic behavior and content highly relevant to understanding group behavior. We believe that both the processes related to the development of group norms in anonymous settings and the significance of role models in behavior change, might be central to understanding these results. Anonymous computer-mediated communication is believed to differ from face-to-face communication in many ways,69,70 perhaps most commonly in terms of self-disclosure71,72 and disinhibited behavior.73,74 In light of these phenomena, The Social Identity Model of Deindividuation Effects (SIDE)75 has been found useful in explaining behavioral change in anonymous groups. SIDE proposes that group norms will be made salient, as individual identities are not available, and that behavior and communication thus will adhere to these norms.76–78 In this particular case, since individuals’ goals and attitudes are “filtered out” through anonymity, the overall goals and norms pertaining to this setting (ie, quitting smoking and/or maintaining abstinence) are made more salient.1 The evidence that certain groups of words became more dominant as the forum developed might be linked to behaviors conforming to a norm of prevention, possibly due to a higher percentage of participants striving towards maintenance of the behavior change. It might be interesting to compare this limited analysis of emotional content with Language Style Matching analysis, in which the functional aspects of language (eg, prepositions, conjunctions, articles, etc) are shown to be related to experiences of group cohesion as well as group performance,79 attesting to the potential of linguistic analysis in understanding group processes. Obviously, the forum might also have affected the individual as part of the group, for instance, functioning as an outlet for thoughts about quitting smoking that might have been harder to communicate face-to-face.
Limitations
All the participants in the study were anonymous. This means that we were unable to analyze to what degree individuals were involved in the ISG and for how long. The continuous recruitment to the discussion forum, ie, the influx of new users in the beginning stages of smoking cessation, complicated the interpretation of the findings. However, previous research does indicate that predominant emotional and regulatory norms are set in place early in health-related discussion forums and remain relatively stable over time, regardless of the turnover of users.80 While we were able to control for the total amount of activity in the forum, we were not able to control for the fact that new users, likely in the first stages of change, entered the ISG throughout the study period. Also, the changes observed are sensitive to drop out (for instance, that people who are negative drop out), rather than to changes in the communication process.
A prior study of the same website has shown that self-regulation, in the form of self-efficacy beliefs, was of importance to smoking-cessation rates.25 While we believe this argues for the importance of self-regulation for smoking cessation, the present study did not provide a direct link between regulatory focus and smoking cessation rates as we did not have data on smoking cessation rates in our study.
It should also be noted that the mean percentage scores yielded for the regulatory focus items were very low and were beneath those advocated by the LIWC-manual, according to which scores under 0.5 are not recommended to be used.44 However, given the highly specific nature of the regulatory focus dimensions, we argue that this finding is an expression of specificity rather than nonvalidity. Also, uncommon behaviors that are novel or distinct might be argued to have larger effects than expected in the experience of participation in an online forum.40 The low percentage scores make the scores sensitive to measurement errors, but we believe the strict construction of the dimensions minimized this risk. Also, all the comparisons between variables were made only for the regulatory focus variables.
Conclusion
Computer-mediated communication can provide easy access to health and lifestyle interventions in ways previously unimagined. ISGs appear to be effective additions to computer-delivered interventions, and their contents might provide important information about ongoing psychological and behavioral processes. Automatic content analysis appears to be a promising tool for accessing these processes and can be used innovatively to address specific motivational dimensions. Understanding the interplay between self-regulation, lifestyle change, and the communication channels afforded by modern technology could be of vital importance in providing the public with better health care services and interventions.
Acknowledgments
The study was supported by grants from the Norwegian Foundation for Health and Rehabilitation and the Norwegian Directorate for Health. The Norwegian version of the LIWC dictionary was made available by Paul Moxnes at the Norwegian School of Management (BI).
Disclosure
The authors report no conflicts of interest in this work.
References
Vambheim SM, Wangberg SC, Johnsen JA, Wynn R. Language use in an internet support group for smoking cessation: development of sense of community. Inform Health Soc Care. 2013;38(1):67–78. | |
Wellman B, Quan Haase A, Witte J, Hampton K. Does the Internet increase, decrease, or supplement social capital? Social networks, participation, and community commitment. Am Behav Sci. 2001;45(3):436–455. | |
Bargh JA, McKenna KYA. The Internet and social life. Annual Rev Psychol. 2004;55(20):1–20. | |
Ferlander S, Timms D. Social capital and community building through the Internet: A Swedish case study in a disadvantaged suburban area. Sociol Res Online. 2007;12(5):1–8. | |
Kummervold PE, Wynn R. Health information accessed on the internet: the development in 5 European countries. Int J Telemed Appl. 2012;2012:297416. | |
Santana S, Lausen B, Bujnowska-Fedak M, Chronaki CE, Prokosch HU, Wynn R. Informed citizen and empowered citizen in health: results from an European survey. BMC Fam Pract. 2011;12:20. | |
Andreassen HK, Wangberg SC, Wynn R, Sørensen T, Hjortdahl P. [Health-related use of the Internet in the Norwegian population]. Tidsskr Nor Laegeforen. 2006;126(22):2950–2952. Norwegian. | |
Kalichman SC, Benotsch EG, Weinhardt L, Austin J, Luke W, Cherry C. Health-related Internet use, coping, social support, and health indicators in people living with HIV/AIDS: preliminary results from a community survey. Health Psychol. 2003;22(1):111–116. | |
Høybye MT, Johansen C, Tjørnhøj-Thomsen T. Online interaction. Effects of storytelling in an internet breast cancer support group. Psychooncology. 2005;14(3):211–220. | |
van Uden-Kraan CF, Drossaert CH, Taal E, Shaw BR, Seydel ER, van de Laar MA. Empowering processes and outcomes of participation in online support groups for patients with breast cancer, arthritis, or fibromyalgia. Qual Health Res. 2008;18(3):405–417. | |
Goodwin PJ, Leszcz M, Ennis M, et al. The effect of group psychosocial support on survival in metastatic breast cancer. N Engl J Med. 2001;345(24):1719–1726. | |
Lieberman MA, Golant M, Giese-Davis J, et al. Electronic support groups for breast carcinoma: a clinical trial of effectiveness. Cancer. 2003;97(4):920–925. | |
Barak A, Boniel-Nissim M, Suler J. Fostering empowerment in online support groups. Computers in Human Behavior. 2008;24:1867–1883. | |
Christakis NA, Fowler JH. The collective dynamics of smoking in a large social network. New Engl J Med. 2008;358(21):2249–2258. | |
Fowler JH, Christakis NA. Dynamic spread of happiness in a large social network: longitudinal analysis over 20 years in the Framingham Heart Study. BMJ. 2008;337:a2338. | |
Alexander C, Piazza M, Mekos D, Valente T. Peers, schools, and adolescent cigarette smoking. J Adolesc Health. 2001;29(1):22–30. | |
Valente TW, Hoffman BR, Ritt-Olson A, Lichtman K, Johnson CA. Effects of a social-network method for group assignment strategies on peer-led tobacco prevention programs in schools. Am J Public Health. 2003;93(11):1837–1843. | |
Stock S, Miranda C, Evans S, et al. Healthy Buddies: a novel, peer-led health promotion program for the prevention of obesity and eating disorders in children in elementary school. Pediatrics. 2007;120(4):e1059–e1068. | |
Maxwell KA. Friends: The role of peer influence across adolescent risk behaviors. J Youth Adolesc. 2002;31(4):267–277. | |
Gardner M, Steinberg L. Peer influence on risk taking, risk preference, and risky decision making in adolescence and adulthood: an experimental study. Dev Psychol. 2005;41(4):625–635. | |
de Ridder D, de Wit J. Self-regulation in health behavior: Concepts, theories, and central issues. In: de Ridder D, de Wit J, editors. Self-Regulation in Health/Behavior. Chichester: John Wiley & Sons Ltd; 2006:1–23. | |
Bäckström S, Wynn R, Sørlie T. Coronary bypass surgery patients’ experiences with treatment and perioperative care – a qualitative interview-based study. J Nurs Manag. 2006;14(2):140–147. | |
Bergvik S, Wynn R, Sørlie T. Nurse training of a patient-centered information procedure for CABG patients. Patient Educ Couns. 2008;70(2):227–233. | |
Tsang SK, Hui EK, Law BC. Self-efficacy as a positive youth development construct: a conceptual review. ScientificWorldJournal. 2012;2012:452327. | |
Wangberg SC, Nilsen O, Antypas K, Gram IT. Effect of tailoring in an internet-based intervention for smoking cessation: randomized controlled trial. J Med Internet Res. 2011;13(4):e121. | |
Thayer RE, Peters III DP, Takahashi PJ, Birkhead-Flight AM. Mood and behavior (smoking and sugar snacking) following moderate exercise: A partial test of self-regulation theory. Personality and Individual Differences. 1993;14(1):97–104. | |
Higgins ET. Beyond pleasure and pain. American Psychologist. 1997;52(12):1280–1300. | |
Higgins ET. Promotion and prevention: Regulatory focus as a motivational principle. Advan Experim Soc Psychol. 1998;30:1–46. | |
Lee AY, Aaker JL, Gardner WL. The pleasures and pains of distinct self-construals: the role of interdependence in regulatory focus. J Pers Soc Psychol. 2000;78(6):1122–1134. | |
Summerville A, Roese NJ. Self-report measures of individual differences in regulatory focus: a cautionary note. J Res Pers. 2008;42(1):247–254. | |
Bergvik S, Sørlie T, Wynn R. Approach and avoidance coping and regulatory focus in patients having coronary artery bypass graft surgery. J Health Psychol. 2010;15(6):915–924. | |
Bergvik S, Sørlie T, Wynn R, Sexton H. Psychometric properties of the Type D scale (DS14) in Norwegian cardiac patients. Scand J Psychol. 2010;51(4):334–340. | |
Rothman AJ. Toward a theory-based analysis of behavioral maintenance. Health Psychol. 2000;19(Suppl 1):S64–S69. | |
Fuglestad PT, Rothman AJ, Jeffery RW. Getting there and hanging on: the effect of regulatory focus on performance in smoking and weight loss interventions. Health Psychol. 2008;27(Suppl 3):S260–S270. | |
Roney CJR, Higgins ET, Shah J. Goals and framing: How outcome focus influences motivation and emotion. Personal Soc Psychol Bull. 1995;21(11):1151–1160. | |
Shah J, Higgins ET. Expectancy x value effects: regulatory focus as determinant of magnitude and direction. J Pers Soc Psychol. 1997;73(3):447–458. | |
Pham MT, Avnet T. Ideals and oughts and the reliance on affect versus substance in persuasion. J Consum Res. 2004;30(4):503–518. | |
Festinger L. A Theory of Cognitive Dissonance. Palo Alto, CA: Stanford University Press; 1957. | |
Bem DJ. Self-perception theory. In: Berkowitz L, editor. Advances in Experimental Social Psychology, vol 6. New York, NY: Academic Press; 1972:1–62. | |
Johnsen JA, Rosenvinge JH, Gammon D. Online group interaction and mental health: an analysis of three online discussion forums. Scand J Psychol. 2002;43(5):445–449. | |
Sillence E, Briggs P, Harris P, Fishwick L. Health websites that people can trust – the case of hypertension. Interact Comput. 2007;19(1):32–42. | |
Leone L, Perugini M, Bagozzi R. Emotions and decision making: Regulatory focus moderates the influence of anticipated emotions on action evaluations. Cogn Emot. 2005;19(8):1175–1198. | |
Roese NJ, Hur T, Pennington GL. Counterfactual thinking and regulatory focus: implications for action versus inaction and sufficiency versus necessity. J Pers Soc Psychol. 1999;77(6):1109–1120. | |
liwc.net [homepage on the Internet]. Linguistic inquiry and word count:LIWC2007. LIWC Inc; 2007. Available from: http://www.liwc.net/. Accessed December 1, 2013. | |
Kahn JH, Tobin RM, Massey AE, Anderson JA. Measuring emotional expression with the Linguistic Inquiry and Word Count. Am J Psychol. 2007;120(2):263–286. | |
Lockwood P, Jordan CH, Kunda Z. Motivation by positive or negative role models: regulatory focus determines who will best inspire us. J Pers Soc Psychol. 2002;83(4):854–864. | |
Owen JE, Klapow JC, Roth DL, Tucker DC. Use of the internet for information and support: disclosure among persons with breast and prostate cancer. J Behav Med. 2004;27(5):491–505. | |
Petrie KJ, Booth RJ, Pennebaker JW. The immunological effects of thought suppression. J Pers Soc Psychol. 1998;75(5):1264–1272. | |
Zhao G, Pechman C. The impact of regulatory focus on adolescents’ response to antismoking advertising campaigns. Journal of Marketing Research. 2007;44(4):671–687. | |
Cesario J, Grant H, Higgins ET. Regulatory fit and persuasion: transfer from “Feeling Right.” J Pers Soc Psychol. 2004;86(3):388–404. | |
Higgins ET. Making a good decision: value from fit. Am Psychol. 2000;55(11):1217–1230. | |
Lee AY, Aaker JL. Bringing the frame into focus: the influence of regulatory fit on processing fluency and persuasion. J Pers Soc Psychol. 2004;86(2):205–218. | |
Freitas AL, Liberman N, Higgins ET. Regulatory fit and resisting temptation during goal pursuit. J Experiment Soc Psychol. 2002;38(3):291–298. | |
Liberman N, Idson LC, Camacho CJ, Higgins ET. Promotion and prevention choices between stability and change. J Pers Soc Psychol. 1999;77(6):1135–1145. | |
Aaker JL, Lee AY. Understanding regulatory fit. Journal of Marketing Research. 2006;43:15–19. | |
Mogilner C, Aaker JL, Pennington GL. Time will tell: The distant appeal of promotion and the imminent appeal of prevention. J Consum Res. 2008;34(5):670–681. | |
Werth L, Förster J. How regulatory focus influences consumer behavior. Eur J Soc Psychol. 2007;37(1):33–51. | |
Iwamitsu Y, Shimoda K, Abe H, Tani T, Kodama M, Okawa M. Differences in emotional distress between breast tumor patients with emotional inhibition and those with emotional expression. Psychiatry Clin Neurosci. 2003;57(3):289–294. | |
Classen C, Koopman C, Angell K, Spiegel D. Coping styles associated with psychological adjustment to advanced breast cancer. Health Psychol. 1996;15(6):434–437. | |
Stanton AL, Danoff-Burg S, Cameron CL, et al. Emotionally expressive coping predicts psychological and physical adjustment to breast cancer. J Consult Clin Psychol. 2000;68(5):875–882. | |
Watson M, Greer S, Rowden L, et al. Relationships between emotional control, adjustment to cancer and depression and anxiety in breast cancer patients. Psychol Med. 1991;21(1):51–57. | |
Esterling BA, L’Abate L, Murray EJ, Pennebaker JW. Empirical foundations for writing in prevention and psychotherapy: mental and physical health outcomes. Clin Psychol Rev. 1999;19(1):79–96. | |
Pennebaker JW. Telling stories: the health benefits of narrative. Lit Med. 2000;19(1):3–18. | |
Agrawal N, Menon G, Aaker JL. Getting emotional about health. Journal of Marketing Research. 2007;44(1):100–113. | |
Parks MR. Social network sites as virtual communities. In: Papacharissi Z, editor. A Networked Self: Identity, Community, and Culture on Social Network Sites. New York, NY: Routledge; 2011:105–123. | |
Walther JB. Computer-mediated communication: Impersonal, interpersonal, and hyperpersonal interaction. Communication Research. 1996;23(1):3–43. | |
Walther JB. Group and interpersonal effects in international computer-mediated collaboration. Human Communication Research. 1997;23(3):342–369. | |
Tidwell LC, Walther JB. Computer-mediated communication effects on disclosure, impressions, and interpersonal evaluations: Getting to know one another a bit at the time. Human Communication Research. 2002;28(3):317–348. | |
Joinson AN. Understanding the Psychology of Internet Behaviour: Virtual Worlds, Real Lives. New York, NY: Palgrave Macmillan; 2003. | |
Joinson A, McKenna K, Postmes T, Reips UD, editors. The Oxford Handbook of Internet Psychology. Oxford: Oxford University Press; 2007. | |
Joinson AN. Knowing me, knowing you: reciprocal self-disclosure in Internet-based surveys. Cyberpsychol Behav. 2001;4(5):587–591. | |
Joinson AN. Self-disclosure in computer-mediated communication: The role of self-awareness and visual anonymity. Eur J Soc Psychol. 2001;31(2):177–192. | |
Joinson AN. Causes and implications of disinhibition on the Internet. In: Gackenbach J, editor. Psychology and the Internet: Intrapersonal, Interpersonal and Transpersonal Implications. San Diego, CA: Academic Press; 1998:43–60. | |
Joinson A. Social desirability, anonymity and Internet-based questionnaires. Behav Res Method Instrum Comput. 1999;31(3):433–438. | |
Reicher SD, Spears R, Postmes T. A social identity model of deindividuation phenomena. In: Stroebe W, Hewstone M, editors. European Review of Social Psychology, vol 6. Chichester: John Wiley & Sons Ltd; 1995:161–198. | |
Postmes T, Spears R, Lea M. The formation of group norms in computer-mediated communication. Human Communication Research. 2000;26(3):341–371. | |
Postmes T, Spears R, Sakhel K, de Groot D. Social influence in computer-mediated communication: The effects of anonymity on group behavior. Pers Soc Psychol Bull. 2001;27(10):1243–1254. | |
Sassenberg K, Boos M. Attitude change in computer-mediated communication: Effects of anonymity and category norms. Group Proc Intergroup Rel. 2003;6(4):405–422. | |
Gonzales AL, Hancock JT, Pennebaker JW. Language style matching as a predictor of social dynamics in small groups. Communication Research. 2010;37(1):3–19. | |
Sandaunet AG. A space for suffering? Communicating breast cancer in an online self-help context. Qual Health Res. 2008;18(12):1631–1641. |
Supplementary material
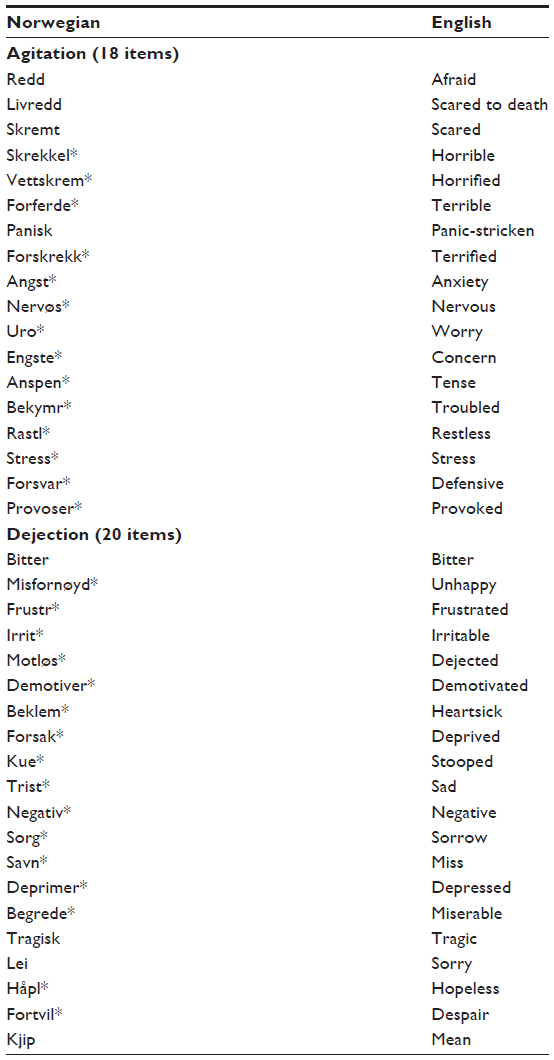 | Table S1 The final dictionary of Dejection- and Agitation-related words |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.