Back to Journals » Risk Management and Healthcare Policy » Volume 14
Knowledge on Menstruation and Practice of Menstrual Hygiene Management Among School Adolescent Girls in Central Ethiopia: A Cross-Sectional Study
Authors Bulto GA ![]()
Received 10 December 2020
Accepted for publication 24 February 2021
Published 5 March 2021 Volume 2021:14 Pages 911—923
DOI https://doi.org/10.2147/RMHP.S296670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Gizachew Abdissa Bulto
Department of Midwifery, College of Medicine and Health Sciences, Ambo University, Ambo, Ethiopia
Correspondence: Gizachew Abdissa Bulto
Department of Midwifery, College of Medicine and Health Sciences, Ambo University, P.O. Box 19, Ambo, Ethiopia
Email [email protected]
Background: Menstruation is a natural event that is a physiological and psychological milestone in women’s reproductive life. But Menstrual Hygiene Management (MHM) continues to be a monthly challenge for adolescent girls in low-income countries, including Ethiopia harming their school attendance, health, and daily life. Therefore, this study aimed to determine the practice of MHM and associated factors in central Ethiopia.
Methods: School-based cross-sectional study was employed among preparatory and high schools in Holeta Town from May 01 to 20, 2019. A systematic random sampling method was used to select study subjects. Data were collected through a self-administered questionnaire and analyzed using SPSS version 23. Both bivariate and multivariable logistic regression were carried out to identify associated factors.
Results: From a total of 403 respondents, 72.5% of school adolescents had good overall knowledge about menstruation and only 34.7% had adequate MHM practice. The study identified adolescents from urban residence (AOR=2.62, 95% CI: 1.53– 4.48), got information about menstruation from mothers (AOR=2.17, 95% CI: 1.18– 3.96) and teachers (AOR=5.09, 95% CI: 2.67– 9.67), school toilets with inside lock (AOR=2.82, 95% CI: 1.67– 4.76), not missing school during menstruation (AOR=4.2, 95% CI: 1.55– 11.41), experienced menstrual-related problems (AOR=2.63, 95% CI: 1.49– 4.64), experienced any whitish or gray discharge per-vagina (AOR=2.84, 95% CI: 1.66– 4.85) and having good overall knowledge about menstruation (AOR=1.94, 95% CI: 1.07– 3.52) were significantly associated with adequate MHM practice.
Conclusion: The study revealed three-fourth of adolescents had good overall knowledge and two-third of them had inadequate MHM practice. Rural residence, source of information on menstruation, school toilets with inside lock, experiencing menstrual-related problems, and overall knowledge were associated with adequate MHM practice. Therefore, working on enhancing the awareness of adolescent girls on menstruation and MHM practice and making school environments conducive to safe MHM practice were recommended.
Keywords: adolescent girls, knowledge, menstrual hygiene management, Ethiopia
Background
Adolescence is a transition period from childhood to adulthood life during which pubertal development and sexual maturation take place. Rapid transformations due to the hormonal changes that accelerate the physical, cognitive, and psychosocial growth usually occurs during adolescence.1–4 From the many changes during adolescence occurrence of menstruation or menarche is the natural event which is a physiological and psychological milestone in women’s reproductive life.5 Even though the occurrence of menstruation is a sign of normal female reproductive functions, it is bounded by several misbeliefs or misconceptions and girls do not feel free to discuss menstruation with other individuals in the public, classroom and even it can be a great taboo to discuss in the family.6–9
Studies from many low-income countries exhibited that many girls are not properly prepared and a very high number of girls start menstruating without having any idea of what is happening to them or why.7,10–12 For this reason, girls in low-income countries report facing stress, confusion, shame, and fear due to a lack of knowledge and poor menstrual hygiene practices.7,13 Additionally, there is a report of teasing and harassment from boys and classmates, not standing in class to answer questions, concerns about odour, and an embarrassing menstrual leak in the classroom among adolescent girls.6,14–17 Taboos surrounding menstruation often exclude girls from many aspects of social and cultural life including religious rituals during menstruation.18,19 Those factors increase the vulnerability of female adolescents to unhygienic practices during menstruation that leads to multiple infections including reproductive and urinary tract.20,21 Those are also highlighted as the main factors which have the most pronounced effect on the adolescent girl’s school attendance, quality, and enjoyment of education.6–8,14
Moreover, adolescent girls reported menstrual pain and lack of effective materials for safe MHM practices as a reason for school absenteeism.14,16,17 As a result, adolescent girls reported as they are frequently using folded, bunched up, or sewed cloth, tissues, or toilet paper, scraps of old cloth, or strips of an old blanket, which often leak and cause chafing, which made school attendance difficult.13,16,22 Water, Hygiene, and Sanitation (WASH) are the leading health-related risks for adolescents aged 10 to 14 years.2,23 In which more than half the schools in low-income countries lack sufficient latrines for girls.16 Improving the school environment and safe access to and use of toilets, sanitary materials and facilities were central interventions for safe MHM practices.21,23,24
Despite increasing local and global attention to MHM practice and its impact on adolescent girls, substantial knowledge gaps persevered.16 Menstruation and MHM practice continue to be a monthly challenge for women and girls across Ethiopia. This is mainly due to young girls often has limited knowledge of menstruation because of the taboo for discussing the issues, lack of access to appropriate sanitary protection products or facilities, and lack of WASH facilities in schools.25–27
Access to a safe, clean, and private space to manage monthly menses with dignity is a human right and public health issue for every menstruating girls and women.16,28 However, in Ethiopia, most school adolescents were practising unsafe menstrual hygiene during menstruation. Studies from Ethiopia revealed that the proportion of adolescent girls practising safe menstrual hygiene management were 21% in Sebeta town,25 (39.9%) in Nekemte Town,29 (29.8%) in Wegera district,27 and (39.7%) in Gedeo zone,10 (24.5%) in Bahir Dar Ethiopia30 and (46.4%) in Ambo Town.26
Although few studies highlighted the level of knowledge on menstruation and MHM practices among school adolescent girls in Ethiopia. Those studies mainly determined the level of safe or adequate MHM practice among school adolescents using the mean values from questions assessing adolescent girl’s menstrual hygiene practice and/or the type of absorbents used during menses, which is not consistent with a unified definition by the World Health Organization (WHO) and United Nations (UNICEF). The Joint Monitoring Program of the WHO and UNICEF in 2012 defined MHM practice as:
Adolescent girls using a clean menstrual management material to absorb or collect blood that can be changed in privacy as often as necessary for the duration of the menstruation period, using soap and water for washing the body as required and having access to facilities to dispose of used menstrual management materials.15,31
Based on this definition and criteria only a study conducted by Shallo et, al. had assessed MHM practice accordingly.26 Considering the diversities concerning socio-demographic (social, economic, and cultural) factors and access to schools WASH facilities for MHM in different parts of Ethiopia it is important to conduct a study on knowledge and practices of MHM in central Ethiopia. Therefore, this study was designed primarily to assess adolescent girls’ knowledge of menstruation and MHM practices and associated factors among secondary and preparatory school girls in Holeta Town, central Ethiopia. The result would be useful in helping stakeholders through determining MHM practice that is consistent with its definition and identifying factors that could affect their practice.
Methods
Study Design, Area, and Period
A school-based descriptive cross-sectional study was employed among adolescent school girls in Holeta town, Oromia special zone surrounding Finfinnee, Oromia region, central Ethiopia from May 01 to 20, 2019. The town is located 38 kilometers to the west of Addis Ababa and has an altitude of 2391 meters above sea level. There are three schools namely Burqa Harbu, Holeta high school, and Holeta preparatory in the town. The total number of school girl students in the town is 1832. There are two public health centers in the town. All regular menstruating adolescent girls attending school at Holeta preparatory and high schools during the data collection period and who were randomly selected were our study population.
Sample Size Determination and Sampling Procedure
The sample size was calculated using single population proportion formula with the assumption of a 95% confidence interval, the margin of error of 5%, 10% non-response, and 57% proportion of good menstrual hygiene practice from a previous study in Adama town.32 By adding a 10% non-response rate the final sample size was 415. The study units were allocated to all three schools proportional to their population size (number of adolescent girls). A systematic random sampling technique was employed to select 415 adolescent girls, by using the list of students from the class roster. Study subjects were selected every 4th individual by dividing the total number of adolescent girls (1832) to sample size.
Measurements
MHM, the practice was measured based on a definition developed by
UNICEF and WHO defining MHM practice as Adolescent girls using a clean menstrual management material to absorb or collect blood that can be changed in privacy as often as necessary for the duration of the menstruation period, using soap and water for washing the body as required and having access to facilities to dispose of used menstrual management materials.15,31
Accordingly, the practice of menstrual hygiene management was measured based on the use of a clean menstrual management material to absorb or collect blood during menstruation that can be changed in privacy (assign 1 point for: use of a disposable sanitary pad or new menstrual cloth or re-usable type of pad), adequate frequency of change (1 point for three or more over 24 hours), washing their genitalia (1 for washing twice or more per 24 hours with soap and water or with plain water), and adequate disposal of used material (1 for burying in toilet or burning). The value of those four criteria was added together and those adolescent girls who scored 1 for all four criteria were considered as having adequate or safe MHM practice and otherwise classified as inadequate or unsafe.15,26,33
Adolescent students who scored above the mean value was used to determine the cut-off point for good knowledge. Accordingly, all respondents who correctly responded to 9 and above questions out of 12 knowledge assessing questions were considered as having good overall knowledge on menstruation and menstrual management. Whereas, those who correctly responded to only 8 or less were considered as having poor overall knowledge of menstruation and menstrual management.17,29
Data Collection Tool, Procedures, and Quality Control
Data were collected through a self-administered questionnaire by using the Afan Oromo version questionnaire. The questionnaires for this study were adapted and modified accordingly from the united nations children’s fund and other related literature.10,15,29,34 Five trained female Midwife professionals (BSc) had collected the data and one supervisor with Masters level supervised the data collection process. One day of training was given for data collectors and supervisors, one week before the day of data collection. A pre-test was done on five percent of the sample at Ejere town preparatory and high schools and accordingly necessary modifications were made. Daily supervision was undertaken throughout the data collection period.
Data Processing and Analysis
The collected data were checked for completeness and entered into Epi info version 7.2.4 and exported to SPSS version 23 statistical software for analysis. Data cleaning was done before conducting the analysis. Bivariate analysis was done to identify those independent variables which have an association with the outcome variable at a p-value of less than 0.25. Hosmer and Lemeshow model test was done to check the model before fitting into the final regression model and it was found to be 0.932. Those variables which have association were fitted into the multiple logistic regression model and associated factors for MHM practice were identified based on the odds ratio with its 95% confidence interval and a P-value of less than or equal to 0.05.
Results
Socio-Demographic Characteristics of Respondents
A total of 403 female adolescents have fully responded, making the response rate of 97.1%. The majority of the respondents, 351 (87.1%) were from grade 9th to 10th, 360 (89.3%) belong to the Oromo ethnic group and 244 (60.5%) were orthodox religious followers. More than half 232 (57.6%) of adolescents were from urban residences and in 239 (59.3%) of them, their parents provide them pocket money regularly. In about 187 (46.4%) and 217 (53.8%) of respondents, their father and mother have no formal education respectively (Table 1).
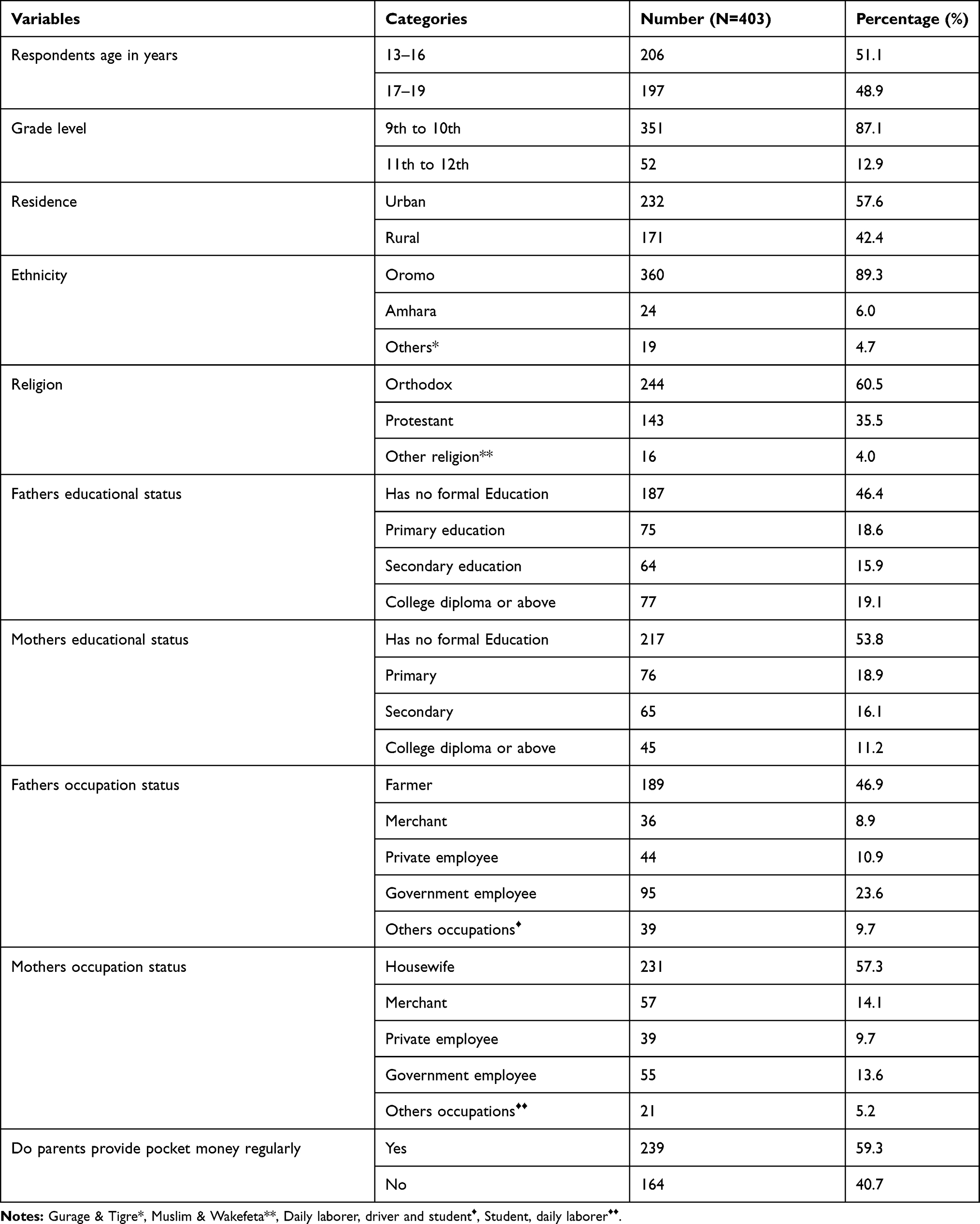 |
Table 1 Socio-Demographic Characteristics of School Adolescent Girls Holeta Town, Central Ethiopia 2019 |
Source of Information and Knowledge on Menstruation
Almost all, 379 (94.0%) of school adolescent girls had heard about menstruation before their menarche. Their main source of information were mothers for 174 (43.2%) adolescent girls. More than half 226 (56.1%) of adolescents freely discuss menstrual issues with their parents. The main reasons reported for not discussing the menstrual issues with parents were because of shamefulness 50 (12.4%), not habitual 65 (16.1%), and due to privacy/secrecy of issue 62 (15.4%). Only 186 (46.2%) of adolescents knew the causes of menstruation as a physiologic process and 301 (74.7%) knew as menstrual blood is from the uterus. Nearly three fourth 292 (72.5%) of school adolescents have a good overall knowledge about menstruation (95% CI: 68.0–77.2%) (Table 2).
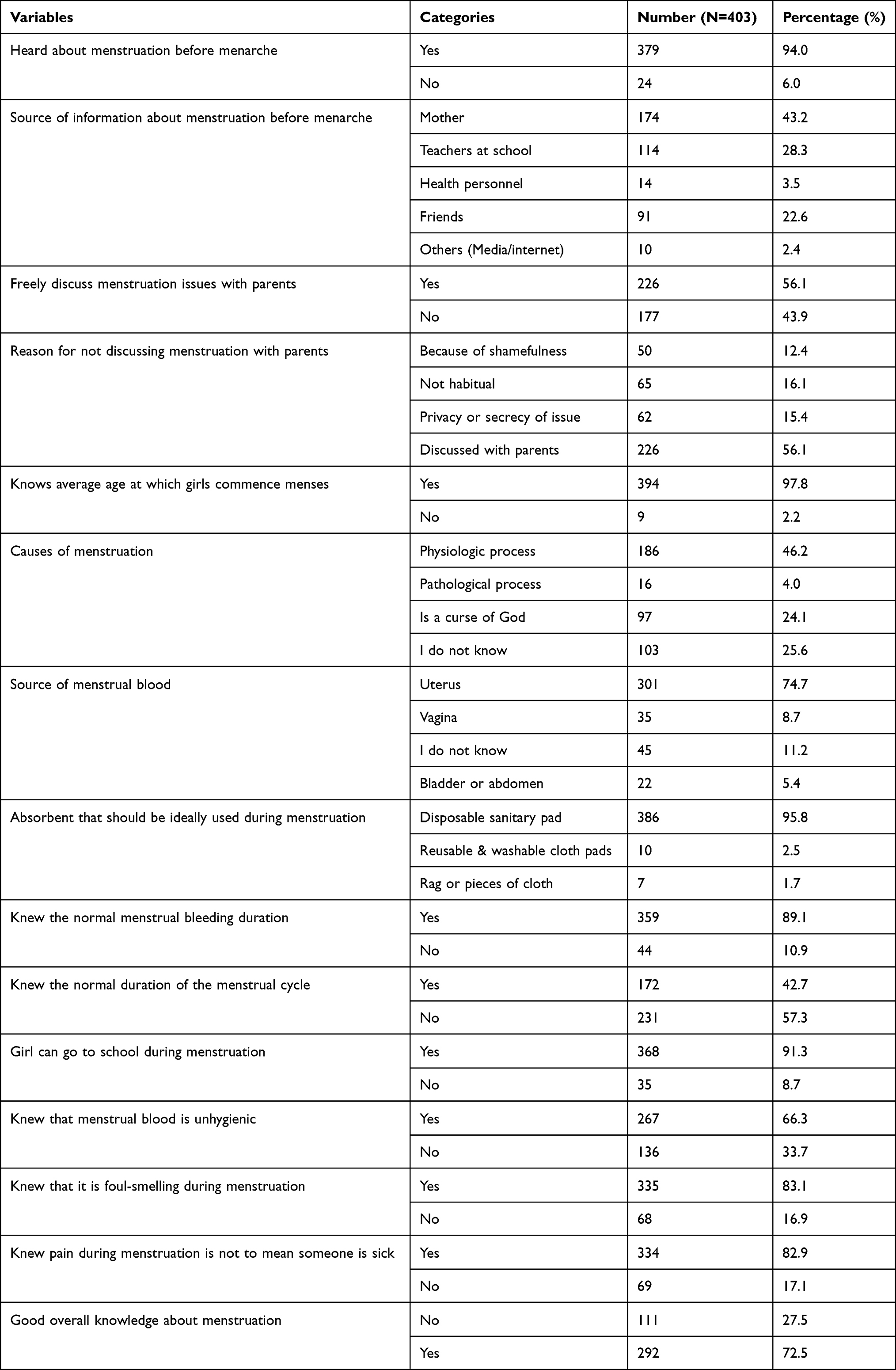 |
Table 2 Source of Information and Knowledge on Menstruation Among School Adolescent Girls in Holeta Town, Central Ethiopia 2019 |
Menstrual Hygiene Management Practices Among School Adolescents
The mean age at menarche among the school adolescent girls was 13.62 with a standard deviation of 1.47 years (ranging from 9 to 17 years). The majority of respondents 267 (66.3%) use disposable sanitary pads during menstruation and 45 (11.2%) use reusable sanitary pads. More than half 229 (56.8%) use soap and water for genital cleaning during menstruation. The majority of respondents 253 (62.8%) change their sanitary material during menstruation in school. Only about 185 (45.9%) of school adolescents were able to change their sanitary material three times or more per day during their menses. The current study found that only 140 (34.7%) (95% CI: 30.1–38.9%) had adequate menstrual hygiene management practices (Table 3).
 |
Table 3 Menstrual Hygiene Management Practices During Menstruation Among School Adolescent Girls in Holeta Town, Central Ethiopia 2019 |
School and Environmental-Related Factors
About 235 (58.3%) reported as there was a separate female toilet having an inside lock. More than three-fourth 271 (67.2%) of respondents had ever experienced menstrual-related health problems during menstruation. More than half, 220 (54.6%) of respondents reported as they had experienced difficulty in pursuing class sessions during menstruation. Almost one-third 126 (31.3%) of the students reported as they missed school because of their menses.
Factors Associated with Menstrual Hygiene Management Practice
On bivariate analysis; mothers educational status, fathers educational status, fathers occupation, place of residence, respondents age at interview, source of information on menstruation before menses (mothers and teachers at school), number of days missed school because of menstruation, having female toilets kept locked inside, overall knowledge on menstruation, ever experienced health problems during menstruation and ever experienced any whitish or gray discharge through the vagina were found to be significantly associated with adequate or safe menstrual hygiene management practice among school adolescents at a p-value of less than 0.2.
In multivariable logistic regression analysis respondents residence, source of information about menstruation (mother and teachers at schools), schools having inside lock female toilets, number of days missed school because of menstruation, experiencing health problems during menstruation, experiencing any whitish or gray discharge through the vagina and good overall knowledge about menstruation were factors identified to be associated with adequate or safe menstrual hygiene management practice among school adolescents.
The current study identified that students who were from the urban residence were 2.62 times more likely to have safe MHM practice than those from rural residences (AOR=2.62, 95% CI: 1.53–4.48). Those adolescents’ girls who got information about menstruation before menarche from their mothers (AOR=2.17, 95% CI: 1.18–3.96) and at schools from teachers (AOR=5.09, 95% CI: 2.67–9.67) were twice and five more likely to practice adequate/safe MHM than those who did not.
Students whose school toilets had female toilets with inside lock were 2.82 times more likely to have safe or adequate MHM practices than those who did not have (AOR=2.82, 95% CI: 1.67–4.76). Adolescent girls who missed their school for one day (AOR=3.69, 95% CI: 1.55–8.77) and did not miss school (AOR=4.2, 95% CI: 1.55–11.41) during their menses were 3.69 and 4.2 times more likely to practice safe MHM than those who missed more than one day respectively.
Adolescent girls who experienced health problems during menstruation were 2.6 times more likely to practice adequate MHM than those who did not experience (AOR=2.63, 95% CI: 1.49–4.64). Those students who ever experienced any whitish or gray discharge through the vagina were 2.8 times more likely to have adequate MHM practices than those who did not experience it (AOR=2.84, 95% CI: 1.66–4.85). Those adolescent girls who had good overall knowledge about menstruation were almost twice more likely to practice adequate or safe MHM than those who had poor knowledge (AOR=1.94, 95% CI: 1.07–3.52) (Table 4).
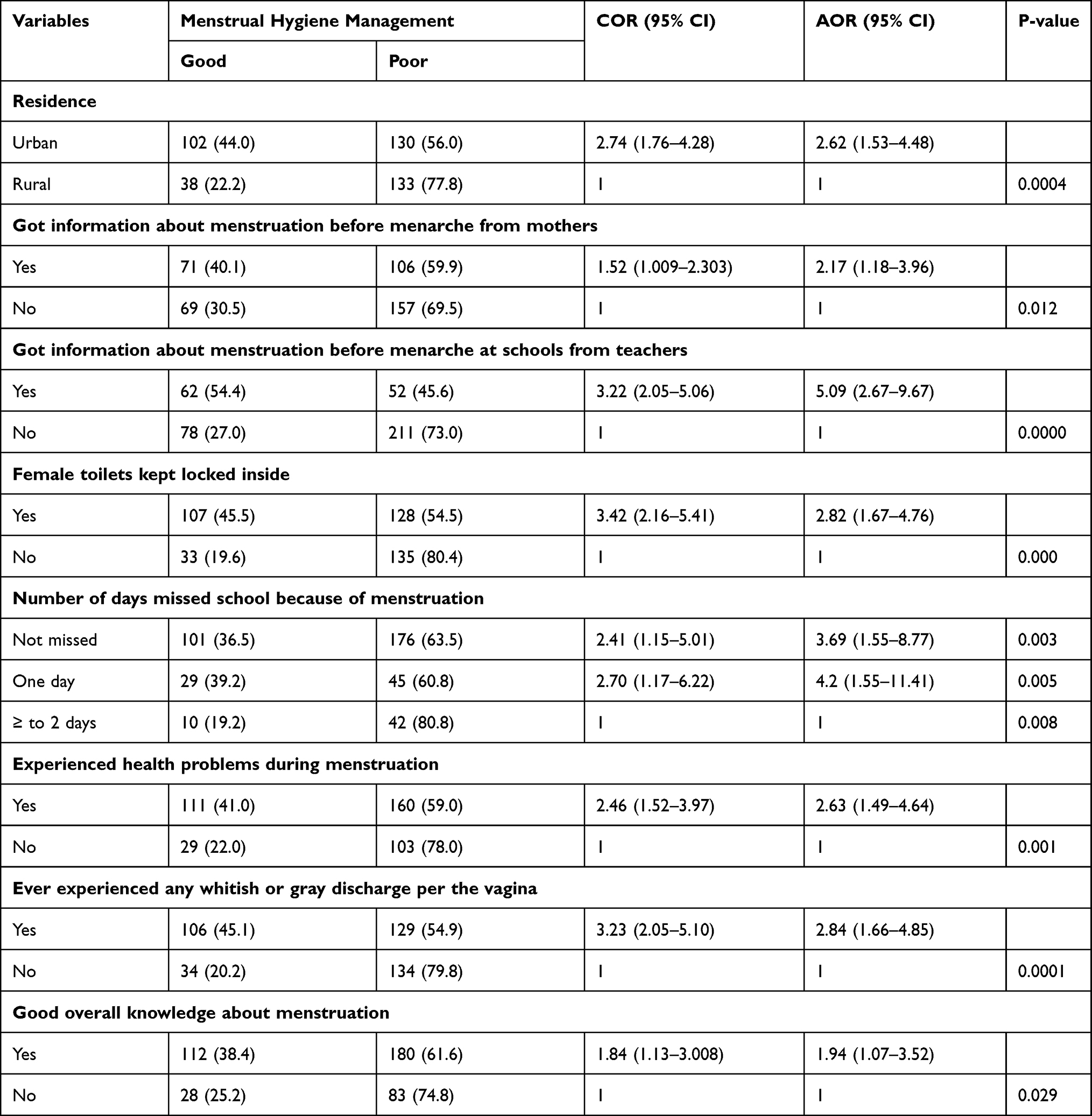 |
Table 4 Factors Associated with Menstrual Hygiene Management Practice Among School Adolescent Girls in Holeta Town, Central Ethiopia, 2019 |
Discussion
The current study found that only one-third of adolescent girls in the Preparatory and High Schools of Holeta Town had good or adequate menstrual hygiene management practices [34.7%, 95% CI: 30.1–38.9%]. This finding was nearly in line with studies done in Nekemte Town (39.9%),29 Wegera district (29.8%),27 and Gedeo zone (39.7%)10 Ethiopia.
But the current finding is higher than studies conducted in Kamuli district, Uganda 9.5% had adequate MHM,15 Bahir Dar Ethiopia 24.5%,30 and 21% in Sebeta town Ethiopia25 had safe or good MHM practice. The possible reason for this is might be due to the difference in socioeconomic characteristics and study period compared with the Kamuli district. The difference in the study period and setting in which Bahir Dar study was conducted with community-based involving both students and other adolescents. This mainly due to education plays an important role in increasing the awareness of MHM among students than other adolescents in the community. Additionally, there is improved attention from different stakeholders on MHM including school-based educational interventions which might have brought some improvement in both countries which is also supported by a systematic review done on MHM.35
The current finding was lower than studies conducted in Mehalmeda, Amhara region (90.9%),36 Boset district East Shewa zone (70.2%)37 had a good MHM practice. The study done in Ambo town which is 53.6% had unsafe MHM practice26 and Adama town (57%).32 It is also lower than the study conducted in Ghana (50.8%) had good MHM.22 The variations were mainly due to the differences in the measurements of MHM practice among those studies in which they have used the mean values of their responses from practice assessing questions.
Nearly three fourth of adolescent girls in preparatory and high schools had good overall knowledge about menstruation [72.5%, 95CI: 68.0–77.2%]. This is in agreement with a study done in the Boset district of East Shewa zone (70.9%).37 The current finding was higher than the study done in Nekemte Town Ethiopia 60.9% had good knowledge,29 Wegera district identified (34.3%)27 and Gedeo zone (31.7%) had good knowledge of menstruation.10 The possible reason for this might be due to the difference in the study period and study population in which the current study was conducted in town unlike that of the Wegera district and Gedeo Zone.
This finding is lower than the study done in the Amhara region Ethiopia 90.7% had a high level of knowledge about menstrual hygiene management.38 The possible reason for this is due to the difference in measurement of knowledge in which the current study used the mean value of responses, but the study in Mehalmeda used 50% as a cut of point to consider adolescents as having good knowledge.
The current study identified that students who were from the urban residence were likely to practice safe MHM than those who were from rural. This is in line with studies done in Mehalmeda, Amhara region students36 and Harbu districts, Ethiopia showed girls from urban areas were more likely to use a disposable sanitary napkin than their counterparts.17 This finding is also consistent with the result of the review of studies from resource-poor countries.39 This was because adolescents from urban were more likely to have access to different sources of information on menstruation and menstrual management and adolescents from rural have less access to materials and facilities used for MHM practices which is also supported by the findings from Jodhpur district of Rajasthan state,40 Zambia,41 and Ethiopia.17,30
Those adolescents who got information about menstruation before menarche from their mothers were twice more likely to have adequate MHM practices than those who did not. In agreement with this study done in Ambo town identified females who frequently discussed menses with their mothers were 70% less likely to manage their MHM safely.26 This finding is also supported by the review from low and middle-income countries.12 This might be due to those mothers who openly discuss menstruation with their daughters were likely to support them with the required materials.
Adolescents who got information about menstruation before menarche at schools from teachers were five times more likely to practice safe MHM than those who did not. In agreement with the study done in Mehalmeda, Amhara region.36 This finding is also consistent with a study done in Nigeria, which is an inappropriate experience of menarche and the use of unhygienic menstrual absorbents were common in girls who had no premenarcheal training than those who did.42 This is maybe since those adolescents who get relevant information at school from teachers either in class or through clubs were likely to be equipped with the necessary skills needed for safe MHM practices.
Adolescent girls whose school toilets had female toilets with inside lock almost three times more likely to practice adequate MHM than those who did not have. In agreement with this study done in the Boset district of the east Shewa zone found those who have access to WASH facilities were more likely to have good MHM practice.37 This is because students with school toilets with no inside locks were forced to wear wet sanitary materials until they find the appropriate place to change or dispose of it and fail to clean their genitalia privately.
The odds of practising safe MHM were higher among those adolescent girls who did not miss their school compared with those who had missed school. This is in agreement with the finding in Indonesia girls with poor MHM missed one or more days of school.8 This finding is also supported by the study done in Harbu districts of northeast Ethiopia in which school absenteeism was higher among those who did not use the disposable sanitary napkins as menstrual absorbent than their counterparts.17 This might be due to the fact that those who did not practice safe MHM were likely to be afraid of being suddenly stained with menstrual blood, ashamed or feeling insecure at school, concerned about odour, fear of teasing from other students, and have higher menstrual-related health problems than those who practice safe MHM. This is also supported by the study done in Uganda, in which MHM was associated with school attendance, with those changing three times a day or more had a higher school attendance rate.15
The current study also revealed that adolescent girls who ever experienced health problems during menstruation and experienced any whitish or gray discharge through the vagina were more likely to practice safe MHM than those who did not. This might be due to those adolescent girls’ who had experienced those problems were likely to have awareness on MHM and pay more attention to their vaginal discharge. Additionally, those school girls who had a history of whitish or gray vaginal discharge might have a fear that others could smell their menses from their previous experience so that they try to keep their menstrual hygiene. This is also supported by the finding from a study done in rural Uganda in which less whitish or green vaginal discharge was reported among those students who have fears that others could smell their menses.15
Those adolescent students who had good overall knowledge about menstruation were almost twice more likely to practice good MHM than those who had poor knowledge. The current finding is consistent with a study done in Sebeta town,25 Mehalmeda,36 Wegera district,27 and Gedeo zone10 Ethiopia. This is also supported by the finding from Bangladesh knowledge improved adolescents MHM practice.11,21 This finding is also supported by the review study from resource-poor countries.39 This could be since those adolescents who have a good overall knowledge might have more self-esteem and adequate skills in MHM practice.
The implications of this study for managers at different levels in the health and education systems in Ethiopia were as follows. A significant number that is nearly four out of six adolescent girls in the study area were practising unsafe MHM. It has also highlighted as there were disparities on MHM practices with residence, availability of female with inside loch toilets in schools, a source of information and overall knowledge on menstruation. Moreover, unsafe MHM practice is affecting school attendance and indirectly affecting adolescent girls school performance in the study area. Therefore, the findings from this study implied for designing an appropriate intervention through working on enhancing the awareness of adolescent school girls on menstruation and MHM practice and making school environments conducive for the safe MHM practices through equipping schools with adequate WASH facilities.
Limitations of the Study
Due to the cross-sectional nature of the study, it is difficult to establish a cause-and-effect relationship and the cultural sensitivity of the issue is not free from social desirability bias.
Conclusions
The study indicated overall only one-third of school adolescent’s girls in the study area practiced good menstrual hygiene management. Nearly one-third of school adolescent girls possessed good overall knowledge of menstruation. Respondents residence, source of information about menstruation (mother and teachers at schools), schools having female toilets with inside lock, number of days missed school because of menstruation, experienced health problems during menstruation, ever experienced any whitish or gray discharge through the vagina and having good overall knowledge about menstruation were factors identified to be associated with good MHM practice among school adolescent girls.
Therefore, all stakeholders should emphatically work on enhancing the awareness of adolescent girls on menstruation and MHM practice through teachers at schools, encouraging parent-adolescent girls’ discussion about menstruation, making school toilets conducive for female adolescents with an inside look; and providing support and guidance for those adolescents who miss school due to menstruation.
Abbreviations
MHM, menstrual hygiene management; WASH, water, sanitation and hygiene.
Data Sharing Statement
The datasets used in the current study can be accessed from the author upon reasonable request.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Research review committee of the College of Medicine and Health Sciences, Ambo University. Then an official letter of support was written to the Holeta town Education bureau and school administrations. Written informed consent was obtained from each study subject and their parents for under 18 years after they read the information sheet and the assent form. Data was collected without having any identifiers and the collected data were kept in a locked file along with the investigator.
Acknowledgments
I would like to express my heartfelt appreciation to Geleta Kabbe, Feyisa Alemayehu, Ashenafi Alemayehu, Girma Dinku, and Fatuma Kebi for their unreserved support during data collection, and data entry of this study. I also want to express my gratitude to all school directors, teachers who supported me during data collection and study respondents for their response.
Funding
No funding was received for this study.
Disclosure
The author declares that they have no competing interests.
References
1. Savi-çakar F, Tagay Ö, Ebru Ikiz F. Risky behaviors of adolescents: definitions and prevention. In:Columbus AM, editor. Advances in Psychology Research. Nova Science Publishers; Vol. 106; 2015:137–167.
2. World Health Organization. Adolescent health overview [Internet]. World Health Organization; 2020 [cited October 9, 2020]. Available from: https://www.who.int/health-topics/adolescent-health#tab=tab_1.
3. Fatusi OA, Hindin MJ. Adolescents and youth in developing countries: health and development issues in context. J Adolesc. 2010;33(4):499–508. doi:10.1016/j.adolescence.2010.05.019
4. WHO. Orientation programme on adolescent health for health-care providers [Internet]. Geneva, Switzerland; 2018: 6. Available from: https://www.who.int/maternal_child_adolescent/documents/pdfs/9241591269_op_handout.pdf.
5. Swenson I, Havens B. Menarche and menstruation: a review of the literature. J Community Health Nurs. 1987;4(4):199–210. doi:10.1207/s15327655jchn0404_3
6. UNICEF WASH. Menstrual hygiene management in ethiopia national baseline report from six regions of Ethiopia [Internet]. Addis Ababa, Ethiopia; 2017. Available from: https://www.unicef.org/ethiopia/media/3096/file/MenstrualHygieneManagementinEthiopia.pdf.
7. UNESCO. Puberty education & menstrual hygiene management good policy and practice in health education booklet. Paris: United Nations Educational, Scientific and Cultural Organization [Internet]; 2014. Available from: http://www.unesco.org/open-access/terms-use-ccbysa-en.
8. Davis J, Macintyre A, Odagiri M, Suriastini W, Cordova A. Menstrual hygiene management and school absenteeism among adolescent students in Indonesia: evidence from a cross-sectional school-based survey. Trop Med Int Health. 2018;23(12):1350–1363. doi:10.1111/tmi.13159
9. Mason L, Nyothach E, Alexander K, et al. We keep it secret so no one should know ’ – a qualitative study to explore young schoolgirls attitudes and experiences with menstruation in Rural Western Kenya. PLoS One. 2013;8(11):11. doi:10.1371/journal.pone.0079132
10. Belayneh Z, Mekuriaw B. Knowledge and menstrual hygiene practice among adolescent school girls in southern Ethiopia: a cross-sectional study. BMC Public Health. 2019;19(1):1595. doi:10.1186/s12889-019-7973-9
11. Kaur R, Kaur K, Kaur R. Menstrual hygiene, management, and waste disposal: practices and challenges faced by girls/women of developing countries. J Environ Public Health. 2018;2018:9. doi:10.1155/2018/1730964
12. Chandra-mouli V, Patel SV. Mapping the knowledge and understanding of menarche, menstrual hygiene and menstrual health among adolescent girls in low- and middle-income countries. Reprod Health. 2017;14(1):1–16. doi:10.1186/s12978-017-0293-6
13. Mcmahon SA, Winch PJ, Caruso BA, et al. The girl with her period is the one to hang her head ’ reflections on menstrual management among schoolgirls in rural Kenya. BMC Int Health Hum Rights. 2011;11(1):7.
14. Miiro G, Rutakumwa R, Nakiyingi-Miiro J, et al. Menstrual health and school absenteeism among adolescent girls in Uganda (MENISCUS): a feasibility study. BMC Womens Health. 2018;18(1):1–13. doi:10.1186/s12905-017-0502-z
15. Hennegan J, Dolan C, Wu M, Scott L, Montgomery P. Measuring the prevalence and impact of poor menstrual hygiene management: a quantitative survey of schoolgirls in rural Uganda. BMJ Open. 2016:6.
16. Sommer M, Sahin M. Advancing the global agenda for menstrual hygiene management for schoolgirls. Am J Public Health. 2013;103(9):1556–1559. doi:10.2105/AJPH.2013.301374
17. Tegegne TK, Sisay MM. Menstrual hygiene management and school absenteeism among female adolescent students in Northeast Ethiopia. BMC Public Health. 2014;14(1):1–14. doi:10.1186/1471-2458-14-1118
18. Van Eijk AM, Sivakami M, Thakkar MB, et al. Menstrual hygiene management among adolescent girls in India: a systematic review and meta-analysis. BMJ Open. 2016:6.
19. Alam M, Luby SP, Halder AK, et al. Menstrual hygiene management among Bangladeshi adolescent schoolgirls and risk factors affecting school absence: results from a cross-sectional survey. BMJ Open. 2017:7.
20. Das P, Baker KK, Dutta A, Swain T, Sahoo S. Menstrual hygiene practices, WASH access and the risk of urogenital infection in women from Odisha, India. PLoS One. 2015:1–16.
21. Haque SE, Rahman M, Itsuko K, Mutahara M, Sakisaka K. The effect of a school-based educational intervention on menstrual health: an intervention study among adolescent girls in Bangladesh. BMJ Open. 2014;4(7):1–9. doi:10.1136/bmjopen-2013-004607
22. Mohammed S, Larsen-Reindorf RE, Awal I. Menstrual hygiene management and school absenteeism among adolescents in Ghana: results from a school-based cross-sectional study in a rural community. Int J Reprod Med. 2020;2020:1–9. doi:10.1155/2020/6872491
23. World Health Organization. Global Accelerated Action for the Health of Adolescents (AA-HA!) Guidance to support country implementation [Internet]. Geneva: World Health Organization. Licence: CC BY-NC-SA 3.0 IGO; 2017. Available from: http://www.who.int/maternal_child_adolescent/documents/global-aa-ha-annexes.pdf?ua=1.
24. UNICEF. Menstrual Hygiene Management Range of Menstrual Hygiene Products; 2016:6
25. Birhane AD, Serbessa MK, Degfie TT. Menstrual hygiene management: a study of adolescent schoolgirls in sebeta town, oromia region, Ethiopia. Glob Drugs Ther. 2020;5:1–8.
26. Shallo SA, Willi W, Abubeker A. Factors affecting menstrual hygiene management practice among school adolescents in Ambo, Western Ethiopia, 2018: a cross-sectional mixed-method study. Risk Manag Healthc Policy. 2020;13:1579–1587. doi:10.2147/RMHP.S267534
27. Fisseha MA, Kebede Y, Yeshita HY. Menstrual hygiene practice and associated factors among secondary school girls in Wegera District, Northwest Ethiopia; a cross-sectional study. Comput Biol Bioinforma. 2017;5(1):6–11. doi:10.11648/j.cbb.20170501.12
28. Sommer M, Hirsch JS, Nathanson C, Parker RG. Comfortably, safely, and without shame: defining menstrual hygiene management as a public health issue. Am J Public Health. 2015;105(7):1302–1311. doi:10.2105/AJPH.2014.302525
29. Upashe SP, Tekelab T, Mekonnen J. Assessment of knowledge and practice of menstrual hygiene among high school girls in Western Ethiopia. BMC Womens Health. 2015;15(1):1–8. doi:10.1186/s12905-015-0245-7
30. Azage M, Ejigu T, Mulugeta Y. Menstrual Hygiene management practices and associated factors among urban and rural adolescents in Bahir Dar City administration, Northwest Ethiopia. Ethiop J Reprod Health. 2018;10(4):10–20.
31. Sommer M, Cherenack E, Blake S, Murat Sahin LB. WASH in Schools Empowers Girls’ Education: Proceedings of the Menstrual Hygiene Management in Schools Virtual Conference 2014. New York: United Nations Children’s Fund and Columbia University; 2015.
32. Anchebi H, Shiferaw Z, Fite O, Abeya G. Practice of menstrual hygiene and associated factors among female high school students in Adama Town. J Womens Health Care. 2017;6:3.
33. Sommer M, Chandraratna S, Cavill S, Mahon T, Phillips-howard P. Managing menstruation in the workplace: an overlooked issue in low- and middle- income countries. Int J Equity Health. 2016;15(1):86. doi:10.1186/s12939-016-0379-8
34. Michael J, Iqbal Q, Haider S, et al. Knowledge and practice of adolescent females about menstruation and menstruation hygiene visiting a public healthcare institute of Quetta, Pakistan. BMC Womens Health. 2020;20(1):1–8. doi:10.1186/s12905-019-0874-3
35. Sumpter C, Torondel B. A systematic review of the health and social effects of menstrual hygiene management. PLoS One. 2011;11(1):e62004. doi:10.1371/journal.pone.0062004
36. Gultie TK. Practice of menstrual hygiene and associated factors among female Mehalmeda high school students in Amhara regional state, Ethiopia. Sci J Public Health. 2014;2(3):189–195. doi:10.11648/j.sjph.20140203.18
37. Kitesa B, Getahun T, Wako K. Assessment of knowledge and practice of adolescent in-school girls towards menstrual hygiene management and determining factors in Lucy Village of Ethiopian Great Rift Valley, 2016. Int J Immunol. 2016;4(6):52–63. doi:10.11648/j.iji.20160406.12
38. Gultie T, Hailu D, Workineh Y. Age of menarche and knowledge about menstrual hygiene management among adolescent school girls in Amhara Province, Ethiopia: implication to health care workers & school teachers. PLoS One. 2014;9(9):1–9. doi:10.1371/journal.pone.0108644
39. Kuhlmann AS, Henry K, Wall LL. Menstrual hygiene management in resource-poor countries. Obstet Gynecol Surv. 2017;72(6):356. doi:10.1097/OGX.0000000000000443
40. Choudhary N, Gupta MK. A comparative study of perception and practices regarding menstrual hygiene among adolescent girls in urban and rural areas of Jodhpur district, Rajasthan. J Fam Med Prim Care. 2019;8(3):875–880.
41. Chinyama J, Chipungu J, Rudd C, et al. Menstrual hygiene management in rural schools of Zambia: a descriptive study of knowledge, experiences and challenges faced by schoolgirls. BMC Public Health. 2019;19(1):1–10. doi:10.1186/s12889-018-6360-2
42. Aniebue UU, Aniebue PN, Nwankwo TO. The impact of pre-menarcheal training on menstrual practices and hygiene of Nigerian school girls. Pan Africa Med J. 2009;2(9):1–9.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.