Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Knowledge of Prevention Measures and Information About Coronavirus in Romanian Male Patients with Severe Mental Illness and Severe Alcohol Use Disorder
Authors Matei V ![]() , Pavel A
, Pavel A ![]() , Giurgiuca A, Roșca A
, Giurgiuca A, Roșca A ![]() , Sofia A, Duțu I, Tudose C
, Sofia A, Duțu I, Tudose C ![]()
Received 24 August 2020
Accepted for publication 31 October 2020
Published 26 November 2020 Volume 2020:16 Pages 2857—2864
DOI https://doi.org/10.2147/NDT.S278471
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Roger Pinder
Valentin Matei,1,2 Alexandru Pavel,1,2 Ana Giurgiuca,1,2 Alina Roșca,1,2 Arina Sofia,1,2 Irina Duțu,1,2 Cătălina Tudose1,2
1Psychiatry Department, University of Medicine and Pharmacy “Carol Davila”, Bucharest, Romania; 2 2nd Clinical Ward, “Prof. Dr. Alexandru Obregia” Psychiatric Hospital, Bucharest, Romania
Correspondence: Alexandru Pavel Email [email protected]
Purpose: Patients with severe mental illness (SMI) and alcohol use disorder (AUD) are at higher risk for contracting coronavirus-19 (COVID-19) and for poor outcomes of COVID-19 infection. One reason for this could be the lack of knowledge regarding preventive measures against COVID-19 and the inability of the psychiatric patients to discern misinformation from facts.
Patients and Methods: The study design was cross-sectional. We applied one questionnaire that evaluated knowledge of prevention measures and information about COVID-19 (comprised of two sections, each with five questions). The first section evaluated knowledge regarding the official WHO prevention measures against COVID-19, and the second consisted of false information about COVID-19 which examined the ability to identify misinformation about COVID-19. These questionnaires were applied face-to-face to psychiatric male inpatients from a tertiary psychiatric hospital in Bucharest diagnosed with SMI or severe alcohol disorder (SAUD) and to male controls from the community, matched by age and education. Mean scores of patients and controls were compared using Mann–Whitney test.
Results: There were 115 male psychiatric patients in total (65 SMI and 50 SAUD) and 57 controls included after the matching procedure. We found statistically significant lower (P< 0.05) scores for psychiatric patients compared to controls regarding the prevention and general knowledge of COVID-19 (P< 0.001), the WHO information about prevention measures (P=0.041), and the ability to identify misinformation about COVID-19 (P< 0.001). The fact that psychiatric patients have less knowledge about prevention measures against COVID-19 and a reduced capacity to discern misinformation suggests that we need to identify new methods to convey correct information to these patients and also to better equip them to handle misinformation regarding COVID-19.
Conclusion: Patients with SMI and SAUD are less informed regarding COVID-19 infection and preventive measures compared to controls, while being prone to believing false information about COVID-19 as well.
Keywords: coronavirus, COVID-19, severe mental illness, alcohol use disorder
Introduction
People with severe mental illness (schizophrenia, schizoaffective disorder, bipolar disorder, and major depression) (SMI) have a significantly higher mortality rate and a 10–30 years shorter life expectancy compared to the general population.1 Probable causes for this discrepancy include an overall poor physical health,2 poor lifestyle choices,3 an ongoing history of marginalization,4–6 deficient access to adequate healthcare,7 socioeconomic disadvantage,8 lack of social support,9 and experiencing pervasive stigma and discrimination.10 The excess mortality is by large the result of inefficient prevention, identification, and treatment of somatic disorders.11
Like patients with SMI, people with alcohol use disorders (AUD) also have increased morbidity12 and mortality,13 caused by deleterious lifestyle choices including: high rates of smoking,14 social challenges,15 poor access to healthcare, and delayed treatment for their physical problems,16 relative to the general population.
Recent data indicates that individuals with mental disorders may also be at higher risk for contracting the virus as well as having poor outcomes of COVID-19 infection.17–20 Established risk factors for COVID-19 infection in this population include:20,21 challenges in appraising health information and complying with preventive behaviors, limited healthcare access, precarious living arrangements or homelessness, and the higher prevalence of comorbid medical conditions (such as cardiovascular disease, cancers, and chronic obstructive pulmonary disease) known to increase the risk of contracting COVID-19 as well as worsening its outcome. What is more, both susceptibility to COVID-19 infection22 and its mortality rate seem greater than double in the male population compared to the female population.19
Additionally, recently published studies support the hypotheses that SMI patients are at an increased risk of both COVID-19 infection and poor outcome of the disease.23
Both SMI and AUD are associated with important cognitive deficits, including executive dysfunction, making these patients more prone to impairments in goal formation, planning, attention, inhibition of response, or coordinating complex cognition.24,25 In addition, people with SMI and AUD comprise a marginalized group26,27 with lower educational attainment28,29 and health literacy30,31 on average, compared to the general population.
All the above factors make it arguably more difficult for patients with SMI and AUD to correctly identify and apply proper preventive measures against COVID-19 infection. This is particularly problematic considering the often-breakneck pace at which large quantities of information, both true and false, about the pandemic circulate. Further complicating things are the frequent changes in directives and recommendations from health officials.32
In the absence of a vaccine and efficient medication for COVID-19 infection,33 the strict adherence to non-pharmaceutical interventions (NPIs) (social distancing, wearing a mask, hands hygiene etc.) represents the most important therapeutic armamentarium against COVID-19 infection.
At the time of writing (October 26, 2020) there have been 41,570,883 reported cases of COVID-19 and 1,134,940 deaths worldwide.34 More concerning is that the COVID-19 pandemic, the uncertainty regarding future lockdowns and its consequences,35 are likely to continue for the foreseeable future.36
Correct information is paramount to disease prevention. Patients with SMI and AUD need, as the rest of the population, to be properly informed about COVID-19 means of transmission and prevention. Even though SMI and AUD patients are not fully representative for the entire population of psychiatric inpatients, we consider the sample of the patients with SMI and AUD to be representative enough for patients who have a psychiatric disorder sufficiently grave to warrant hospital admission during a time of pandemic, when admissions were used only as a last resort. The goal of our study is to assess the prevention and general knowledge of male patients with SMI and AUD regarding COVID-19.
Subjects and Methods
We designed a cross-sectional study in order to assess our hypothesis using a questionnaire (called from here on “the prevention and general knowledge questionnaire”) with 10 statements: five true assertions, based on the first five WHO statements regarding prevention measures against COVID-1934 (named “the WHO prevention measures questionnaire”), and five wrong assertions (produced by us and called “the fictitious questionnaire”) about COVID-19 infection and preventive measures. The purpose of the WHO prevention measures questionnaire was to examine if the targeted population knew the “official” (WHO designed) and unanimous accepted prevention measures against COVID-19, while the purpose of the “the fictitious questionnaire” was to observe if the patients could correctly identify false information regarding COVID-19 infection and prevention measures against it. The WHO statements included in WHO prevention measures questionnaire are: 1) “regularly and thoroughly clean your hands”; 2) “maintain at least 1 meter distance between yourself and others”; 3) “avoid touching eyes, nose and mouth”; 4) “cover your mouth and nose with your bent elbow or tissue when you cough or sneeze then dispose of the used tissue immediately”; and 5)
stay home and self-isolate even with minor symptoms such as cough, headache, mild fever, until you recover. If you have a fever, cough and difficulty breathing, seek medical attention, but call by telephone in advance if possible and follow the directions of your local health authority.
The five made-up (wrong) assertions used in the fictitious questionnaire were: 1) “pregnant women are the most vulnerable to COVID-19 infection”; 2) “the risk of COVID-19 infection is 1%”; 3) “the virus cannot be transmitted by touching metal or plastic surfaces”; 4) “virus is mainly spread through contaminated food”; and 5) “an efficient vaccine will be available in one month”. Each statement had a true/false response option, and 1 point was awarded for each correct answer (1 point for each true answer from the WHO prevention measures questionnaire and 1 point for each false answer correctly identified as false from the the fictitious questionnaire). Therefore the total score for the prevention and general knowledge questionnaire (10 questions) reflects preventive and general knowledge regarding infection with COVID-19, the score of the WHO prevention measures questionnaire (five questions) regarding preventive measures reflects the level of knowledge about prevention of COVID-19 infection, and the score obtained on the fictitious questionnaire (five fictitious questions) reflects the ability of patients to discern misinformation regarding COVID-19. The maximum score for the WHO prevention measures questionnaire was 5, the same for the fictitious questionnaire. The score for the prevention and general knowledge questionnaire was created by adding the scores of the WHO prevention measures questionnaire and the fictitious questionnaire, with 10 being the highest possible score. Higher scores indicate better knowledge about prevention of COVID-19 infection and the capacity to identify the misinformation.
The questionnaire was applied face-to-face, during hospitalization, to a total of 115 male psychiatric patients comprised of 65 SMI patients, 50 Severe Alcohol Use Disorder (SAUD) patients (that is patients with complicated alcohol withdrawal syndrome severe enough to necessitate hospitalization) hospitalized in a tertiary psychiatric hospital from Bucharest after lockdown was instated (in Bucharest lockdown was instated between March 16–May 14, 2020) and 69 male controls. Due to the fact that during lockdown selective admission was instated in order to minimize risk of COVID-19 transmission, our sample consists of patients with severe enough disorder to warrant admission during this pandemic. Given the lack of data regarding the level of information concerning prevention against COVID-19 in the groups of patients and controls we could not estimate the sample size. The control sample was randomly selected from the community through raters placed in residential areas and near major shopping centers. All the male persons over 18 years old that agreed to participate and signed an informed consent were included. The cohorts were matched by age and education using the case-control matching algorithm of the IBM SPSS Statistics 26, prioritizing exact matches and using the maximum value of fuzz permitted to keep the alpha level over 0.05 between groups. There was no formal teaching on COVID-19 information prior to filling out the questionnaire. Formal education about COVID-19 infection and prevention was offered to all patients after filling out the questionnaire. For the psychiatric patients, the questionnaire was applied when each senior psychiatrist considered his patients clinically well enough to attend to the questionnaire.
We compared the group of patients (SMI and SAUD) with controls, then compared each sub-group individually with controls. The SMI and SAUD groups were also compared which each other.
The Protocol of the study was approved by the hospital IEC and all participants signed a written informed consent form. The study was conducted in accordance with the Declaration of Helsinki.37 Descriptive statistics were used to characterize the samples. Scores were compared using Mann–Whitney test (for non-parametric data distribution). Results were considered statistically significant at alpha=0.05, 2-tailed. For more clarity we presented both the mean and median results. Percentual differences between groups have been reported using the mean scores. All analyses have been carried with SPSS Statistics.
Results
There were 115 male psychiatric patients in the whole group of patients (65 SMI and 50 SAUD) and 57 controls included after the matching procedure. The demographic and social characteristics of the samples are described in Table 1.
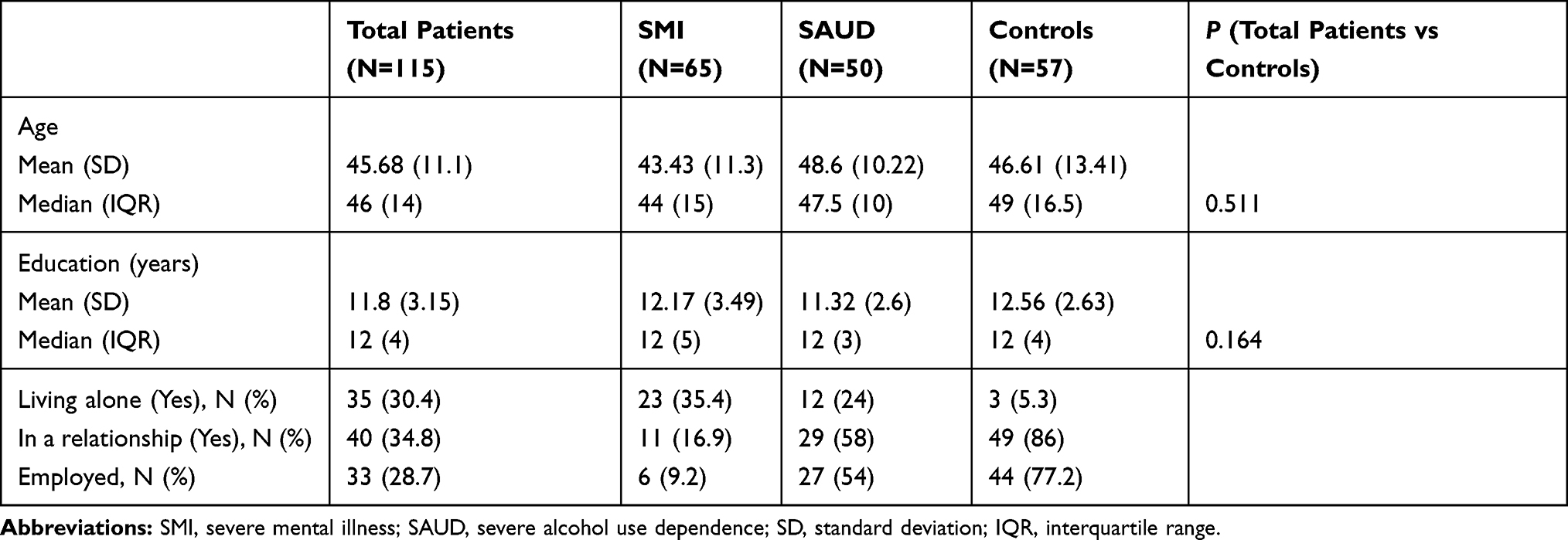 |
Table 1 Social and Demographic Characteristics |
Results of between-groups analysis regarding questionnaire answers are presented in Table 2.
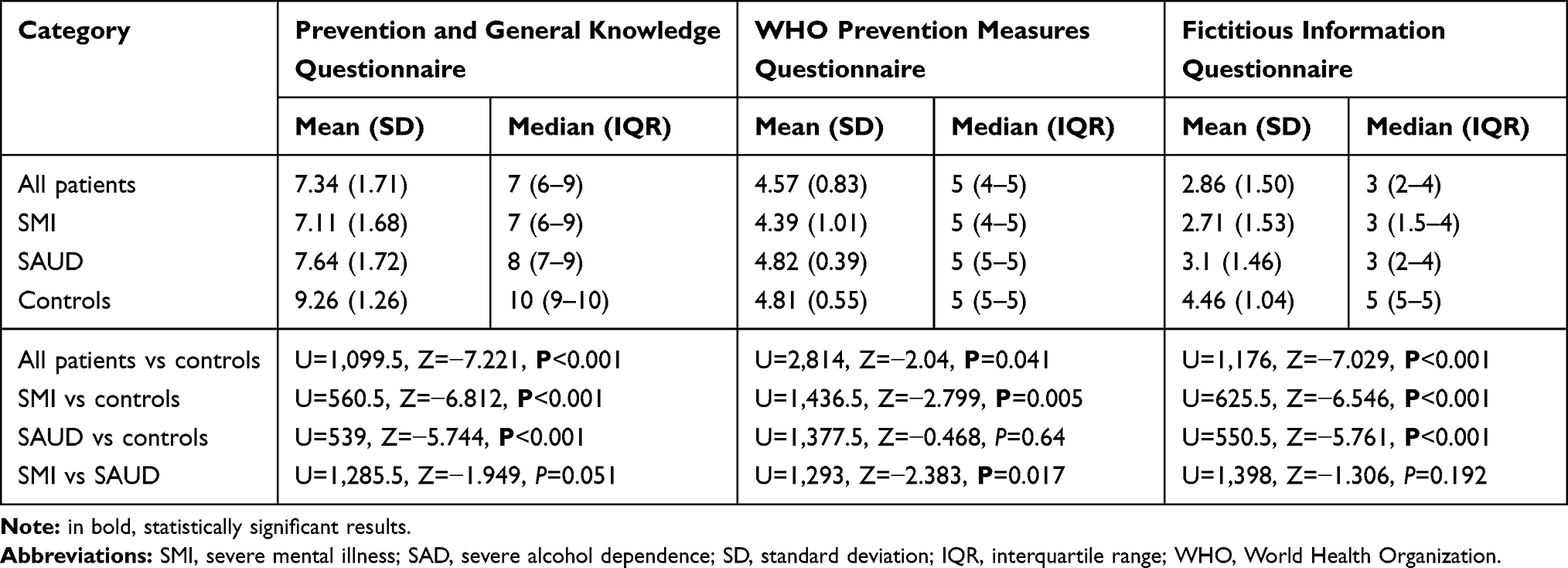 |
Table 2 Questionnaire Results |
The whole group of psychiatric patients (SMI and SAUD) had significantly lower scores regarding prevention and general knowledge about COVID-19, with psychiatric patients scoring an average of 19.2% (on the mean results) poorer than controls.
On the WHO prevention measures questionnaire, psychiatric patients scored an average of 4.8% lower compared to controls. Psychiatric patients also scored an average of 32% lower than controls on the fictitious questionnaire.
SMI patients had a significantly lower score compared to controls regarding prevention and general knowledge about COVID-19 with a 21.5% lower mean score. Regarding the WHO prevention measures questionnaire, SMI patients had an 8.4% lower mean score compared to controls. The same group had a 35% lower mean score on the fictitious questionnaire compared to controls.
Patients with SAUD had significantly lower scores on the prevention and general knowledge questionnaire, with a 16.2% mean score difference. There was a similar score between SAUD group and controls on the WHO prevention measures questionnaire. Patients with SAUD had significantly lower scores on the fictitious questionnaire compared to controls with 27.2% mean score difference.
SAUD patients also scored better in all questionnaire categories compared to SMI patients, with mean score differences of 5.3% on the prevention and general knowledge questionnaire, 8.6% on the WHO prevention measures questionnaire, and 7.8% on the fictitious questionnaire, but only the differences between the WHO prevention measures questionnaire scores reached statistical significance.
Discussion
To our knowledge, this is the first study to evaluate COVID-19 information in male psychiatric inpatients.
Male patients with SMI and SAUD, categorized as a group of patients with a psychiatric disorder, are less informed regarding COVID-19 preventive measures recommended by WHO and were more likely to believe fictitious information compared to controls. The average score difference between psychiatric patients and controls was smallest (almost 5%) for the WHO prevention measures questionnaire. This represents encouraging news because the information campaign performed by WHO together with local government agencies seems to have reached this vulnerable group as well. On the other hand, when discussing large scale events such as the COVID-19 pandemic, even a 5% difference could be very important.
The highest difference was in the fictitious questionnaire, where psychiatric patients performed worse than controls (mean difference between scores was 32%). This could be interpreted as an indication that psychiatric patients had more difficulties to correctly identify false information.
SMI patients performed significantly worse than controls both in knowledge of WHO preventive measures and in identification of false information. SAUD patients identified the WHO prevention measures with the same level of accuracy as the control group but performed as poorly as SMI patients in “the fictitious questionnaire”.
The fact that SMI male patients have significantly lower knowledge of COVID-19 compared to male general population can lead to important consequences regarding both individual risk and the risk of exposing others to the disease. Prevention measures may be less efficacious in this group, which may prove deleterious to the efforts to contain the pandemic. Traditional methods of communicating information may be insufficient for SMI patients. Some of the differences can be explained by social causes, both SMI and SAUD patients being less exposed than controls to social circumstances where they putatively could exchange information; more of our SMI and SAUD patients have no occupation, are single, and live alone compared to controls.
The severity of the pathology, cognitive impairment, motivation, and insight could also contribute to these results. It is possible that some patients might not comprehend relatively simple statements, and this can equally interfere with the ability to apprehend preventative measures against COVID-19 spread and the accuracy of SMI patients to answer epidemiologic screening questions. However, SAUD male patients have similar knowledge of “official” WHO COVID-19 information compared to the male general population.
With all this taken into account, both groups of psychiatric patients performed poorer than controls on “the fictitious questionnaire”. These lower scores indicate a possible vulnerability of this group of patients to accepting misinformation as facts. Accurate knowledge and information are essential for human beings to be able to make rational decisions and operate in society.38 This is even further emphasized during massively disruptive events, such as the 2020 COVID-19 global pandemic.39 The consequences of spreading false information could case cyberchondria,40 poor health related decisions,41 and, in the extreme, deaths due to the inability of an individual or health official to assess the severity of a situation and implement the necessary actions.42,43
SMI and SAUD patients have decreased cognitive performance that could make them more likely to accept biased information as true7 compared to controls. For instance, some cognitive functions are considered to play an important role in processing misinformation and may be impaired in these patients, such as: fluency,44 analytical thinking,45,46 and numeracy skills.47–49 These are also often related to accuracy in judgment and decision-making across a wide range of domains50 and “intuitive” vs “reflective” thinking styles.51,52
The fact that both patients with SMI and SAUD performed poorly on “the fictitious questionnaire” strongly suggests that these groups are particularly inclined to believe misinformation and that methods for making these patients less susceptible to misinformation should be developed.
However, whether there is an important discrepancy within the psychiatric patients’ group (as obviously is for controls) between being well informed and acting accordingly, that remains to be evaluated, although there are studies that suggest a possible link between trusting false information and disrespecting reliable medical advice.53
There is some evidence that certain methods may reduce the susceptibility to misinformation towards COVID-19 in the general population: conveying scientific information in a way that is perceived as an attempt to be open and transparent,54 choosing not to acquire information about COVID-19 from social media,55 developing numeracy skills, and critical thinking skills.53 However, this hypothesis has not been thoroughly studied in psychiatric patients.
A better understanding of how psychiatric male patients comprehend evidence about COVID-19 is of paramount importance in order to better tailor the dissemination of information toward this particular vulnerable group.
The mental health consequences of the ongoing pandemic are still unknown, but evidence suggest a possible increase in affective and anxiety disorders and likely a deleterious evolution of all patients with psychiatric illnesses.56,57 In this manner, mental health professionals should be prepared to offer help either in face-to-face scenarios or online through telemedicine to persons in need, including medical staff.58
During these pandemic times, the delivery of information to promote mental healthcare should definitely be an ongoing duty. Since social distancing must be used at any possible moment, we should use telepsychiatry as frequent as possible.59 It is efficient regarding psychoeducation, which is very important for offering correct information about COVID-19 prevention and for combating misinformation about COVID-19 in psychiatric patients.60 What is more, it is considered a cost-effective alternative to traditional psychiatry.61 During this pandemic hospital, access has been limited, so digital means of communication should be used whenever possible in order to minimize exposure and still offer the patients the services and support that they need62 and that includes offering correct information about COVID-19 prevention and combating misinformation in the most efficient manner, tailored for this group of patients. The best method for offering information and preventing misinformation about COVID-19 in psychiatric patients, both face-to-face and using telemedicine, remains to be developed.
Limitations
While our results are promising, they should be interpreted while taking into consideration the study limitations. The sample size was rather small and limited from a geographical standpoint making our results less likely to be generalized to the entire population. The control sample was included from patients from different residential areas and from shopping centers. This could imply the fact that these persons could have been either better informed or less informed than the general population regarding prevention measures, which could affect the sub-sample of the controls.
Even though SMI and SAUD represent severe enough diseases to warrant hospital admission during a pandemic they do not represent the totality of psychiatric illnesses that could have been urgently admitted, thus limiting our sample. Even though male patients seem more vulnerable to misinformation and having worse COVID-19 infection outcome compared to female patients, this does not infer a gender gap in these matters, warranting future studies involving both male and female psychiatric patients.
Conclusion
Patients with SMI and SAUD are less informed regarding COVID-19 infection and preventive measure compared to controls. They are also prone to believing false information regarding COVID-19 compared to controls. Understanding how to better tailor the communication of proper information for psychiatric patients may be of vital importance for this particular group.
Acknowledgements
We would like to thank the medical staff of the “Prof. Dr. Alexandru Obregia“ Hospital.
Funding
There was no funding involved in designing of the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. De Hert M, Dekker JM, Wood D, Kahl KG, Holt RIG, Möller HJ. Cardiovascular disease and diabetes in people with severe mental illness position statement from the European Psychiatric Association (EPA), supported by the European Association for the Study of Diabetes (EASD) and the European Society of Cardiology (ESC). Eur Psychiatry. 2009;24(6):412–424. doi:10.1016/j.eurpsy.2009.01.005
2. De Hert M, Correll CU, Bobes J, et al. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry. 2011;10(1):52–77. doi:10.1002/j.2051-5545.2011.tb00014.x
3. Parks J, Svendsen D, Singer P, Foti ME, Mauer B. Morbidity and mortality in people with serious mental illness. Alexandria, VA Natl Assoc State Ment Heal Progr Dir Med Dir Counc. 2006;25(4):1–87.
4. Mitchell AJ, Malone D, Doebbeling CC. Quality of medical care for people with and without comorbid mental illness and substance misuse: systematic review of comparative studies. Br J Psychiatry. 2009;194(6):491–499. doi:10.1192/bjp.bp.107.045732
5. Lawrence D, Kisely S. Inequalities in healthcare provision for people with severe mental illness. J Psychopharmacol. 2010;24(4_suppl):61–68. doi:10.1177/1359786810382058
6. Leucht S, Burkard T, Henderson J, Maj M, Sartorius N. Physical illness and schizophrenia: a review of the literature. Acta Psychiatr Scand. 2007;116(5):317–333. doi:10.1111/j.1600-0447.2007.01095.x
7. Lawrence D, Jablensky A. Preventable physical illness in people with mental illness. 2001.
8. Saraceno B, Levav I, Kohn R. The public mental health significance of research on socio-economic factors in schizophrenia and major depression. World Psychiatry. 2005;4(3):181.
9. Green MF, Horan WP, Lee J, McCleery A, Reddy LF, Wynn JK. Social disconnection in schizophrenia and the general community. Schizophr Bull. 2018;44(2):242–249. doi:10.1093/schbul/sbx082
10. Thornicroft G, Brohan E, Rose D, Sartorius N, Leese M, Group IS. Global pattern of experienced and anticipated discrimination against people with schizophrenia: a cross-sectional survey. Lancet. 2009;373(9661):408–415. doi:10.1016/S0140-6736(08)61817-6
11. Saxena S, Maj M. Physical health of people with severe mental disorders: leave no one behind. World Psychiatry. 2017;16(1):1. doi:10.1002/wps.20403
12. Odlaug BL, Gual A, DeCourcy J, et al. Alcohol dependence, co-occurring conditions and attributable burden. Alcohol Alcohol. 2016;51(2):201–209. doi:10.1093/alcalc/agv088
13. Roerecke M, Rehm J. Alcohol use disorders and mortality: a systematic review and meta‐analysis. Addiction. 2013;108(9):1562–1578. doi:10.1111/add.12231
14. Dixon L, Medoff DR, Wohlheiter K, et al. Correlates of severity of smoking among persons with severe mental illness. Am J Addict. 2007;16(2):101–110. doi:10.1080/10550490601184415
15. Saavedra J, López M, González S, Arias S, Crawford P. Cognitive and social functioning correlates of employment among people with severe mental illness. Community Ment Health J. 2016;52(7):851–858. doi:10.1007/s10597-015-9874-4
16. Nicaise P, Giacco D, Soltmann B, et al. Healthcare system performance in continuity of care for patients with severe mental illness: a comparison of five European countries. Health Policy (New York). 2020;124(1):25–36. doi:10.1016/j.healthpol.2019.11.004
17. Ghebreyesus TA. Addressing mental health needs: an integral part of COVID‐19 response. World Psychiatry. 2020;19(2):129. doi:10.1002/wps.20768
18. Li J, Yang Z, Qiu H, et al. Anxiety and depression among general population in China at the peak of the COVID‐19 epidemic. World Psychiatry. 2020;19(2):249. doi:10.1002/wps.20758
19. Yao H, Chen JH, Xu YF. Patients with mental health disorders in the COVID-19 epidemic. Lancet Psychiatry. 2020;7(4):e21. doi:10.1016/S2215-0366(20)30090-0
20. Kozloff N, Mulsant BH, Stergiopoulos V, Voineskos AN. The COVID-19 global pandemic: implications for people with schizophrenia and related disorders. Schizophr Bull. 2020;46(4):752–757. doi:10.1093/schbul/sbaa051
21. Shinn AK, Viron M. Perspectives on the COVID-19 pandemic and individuals with serious mental illness. J Clin Psychiatry. 2020;81(3). doi:10.4088/JCP.20com13412
22. de Lusignan S, Dorward J, Correa A, et al. Risk factors for SARS-CoV-2 among patients in the Oxford Royal college of general practitioners research and Surveillance Centre primary care network: a cross-sectional study. Lancet Infect Dis. 2020;20(9):1034–1042. doi:10.1016/S1473-3099(20)30371-6
23. Wang Q, Xu R, Volkow ND. Increased risk of COVID‐19 infection and mortality in people with mental disorders: analysis from electronic health records in the United States. World Psychiatry.
24. Sheffield JM, Karcher NR, Barch DM. Cognitive deficits in psychotic disorders: a lifespan perspective. Neuropsychol Rev. 2018;28(4):509–533.
25. Le Berre A, Fama R, Sullivan EV. Executive functions, memory, and social cognitive deficits and recovery in chronic alcoholism: a critical review to inform future research. Alcohol Clin Exp Res. 2017;41(8):1432–1443. doi:10.1111/acer.13431
26. Hakulinen C, Elovainio M, Arffman M, et al. Employment status and personal income before and after onset of a severe mental disorder: a case-control study. Psychiatr Serv. 2020;71(3):250–255. doi:10.1176/appi.ps.201900239
27. Jones L, Bates G, McCoy E, Bellis MA. Relationship between alcohol-attributable disease and socioeconomic status, and the role of alcohol consumption in this relationship: a systematic review and meta-analysis. BMC Public Health. 2015;15(1):400.
28. Tempelaar WM, Termorshuizen F, MacCabe JH, Boks MPM, Kahn RS. Educational achievement in psychiatric patients and their siblings: a register-based study in 30 000 individuals in the Netherlands. Psychol Med. 2017;47(4):776–784. doi:10.1017/S0033291716002877
29. Crum RM, Helzer JE, Anthony JC. Level of education and alcohol abuse and dependence in adulthood: a further inquiry. Am J Public Health. 1993;83(6):830–837. doi:10.2105/AJPH.83.6.830
30. Kim S-W, Park W-Y, Jhon M, et al. Physical health literacy and health-related behaviors in patients with psychosis. Clin Psychopharmacol Neurosci. 2019;17(2):279. doi:10.9758/cpn.2019.17.2.279
31. Lincoln A, Paasche‐Orlow MK, Cheng DM, et al. Impact of health literacy on depressive symptoms and mental health‐related: quality of life among adults with addiction. J Gen Intern Med. 2006;21(8):818–822. doi:10.1111/j.1525-1497.2006.00533.x
32. WHO. Munich Security Conference. 2020. Available from: https://www.who.int/dg/speeches/detail/munich-security-conference.
33. Sc M, Peto R, Karim QA, et al. Repurposed antiviral drugs for COVID-19 – interim WHO SOLIDARITY trial results. 2020;15.
34. World Health Organization. Coronavirus Disease (COVID-19) Pandemic. 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus–2019.
35. Kissler SM, Tedijanto C, Goldstein E, Grad YH, Lipsitch M. Projecting the transmission dynamics of SARS-CoV-2 through the postpandemic period. Science (80-). 2020;368(6493):860–868. doi:10.1126/science.abb5793
36. Moore KA, Lipsitch M, Barry JM, Osterholm MT COVID‐19: the CIDRAP Viewpoint: part 1: the Future of the COVID‐19 Pandemic: lessons Learned from Pandemic Influenza. CIDRAP Univ Minnesota April 30th. 2020:8.
37. World Medical Association. Declaration of Helsinki, Ethical Principles for Scientific Requirements and Research Protocols. World Med Assoc. 2013:29–32. Avialable from: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/.
38. Vosoughi S, Roy D, Aral S. The spread of true and false news online. Science (80-). 2018;359(6380):1146–1151. doi:10.1126/science.aap9559
39. Bai Y, Yao L, Wei T, et al. Presumed asymptomatic carrier transmission of COVID-19. JAMA. 2020;323(14):1406–1407. doi:10.1001/jama.2020.2565
40. Lewis T. Seeking health information on the internet: lifestyle choice or bad attack of cyberchondria? Media Cult Soc. 2006;28(4):521–539. doi:10.1177/0163443706065027
41. Allcott H, Gentzkow M. Social media and fake news in the 2016 election. J Econ Perspect. 2017;31(2):211–236. doi:10.1257/jep.31.2.211
42. Kata A. A postmodern Pandora’s box: anti-vaccination misinformation on the Internet. Vaccine. 2010;28(7):1709–1716. doi:10.1016/j.vaccine.2009.12.022
43. Sommerlad J Coronavirus: china’s disinformation campaign costing lives and hindering global response, MPs warn. The Independent. Available from: https://www.independent.co.uk/news/uk/politics/coronavirus-china-disinformation-commons-foreign-affairs-report-russia-iran-a9448241.html.
44. Stavro K, Pelletier J, Potvin S. Widespread and sustained cognitive deficits in alcoholism: a meta‐analysis. Addict Biol. 2013;18(2):203–213. doi:10.1111/j.1369-1600.2011.00418.x
45. Guess A, Nagler J, Tucker J. Less than you think: prevalence and predictors of fake news dissemination on Facebook. Sci Adv. 2019;5(1):eaau4586. doi:10.1126/sciadv.aau4586
46. Puveendrakumaran P, Fervaha G, Caravaggio F, Remington G. Assessing analytic and intuitive reasoning using the cognitive reflection test in young patients with schizophrenia. Psychiatry Res. 2020;284:112683. doi:10.1016/j.psychres.2019.112683
47. van Prooijen J, Staman J, Krouwel APM. Increased conspiracy beliefs among ethnic and Muslim minorities. Appl Cogn Psychol. 2018;32(5):661–667. doi:10.1002/acp.3442
48. Hatashita-Wong M, Smith TE, Silverstein SM, Hull JW, Willson DF. Cognitive functioning and social problem-solving skills in schizophrenia. Cogn Neuropsychiatry. 2002;7(2):81–95. doi:10.1080/13546800143000168
49. Schmidt T, Roser P, Juckel G, Brüne M, Suchan B, Thoma P. Social cognition and social problem solving abilities in individuals with alcohol use disorder. J Clin Exp Neuropsychol. 2016;38(9):974–990. doi:10.1080/13803395.2016.1180346
50. Peters E, Västfjäll D, Slovic P, Mertz CK, Mazzocco K, Dickert S. Numeracy and decision making. Psychol Sci. 2006;17(5):407–413. doi:10.1111/j.1467-9280.2006.01720.x
51. Bago B, Rand DG, Pennycook G. Fake news, fast and slow: deliberation reduces belief in false (but not true) news headlines. J Exp Psychol Gen. 2020;149(8):1608–1613. doi:10.1037/xge0000729
52. Roets A. ‘Fake news’: incorrect, but hard to correct. The role of cognitive ability on the impact of false information on social impressions. Intelligence. 2017;65:107–110. doi:10.1016/j.intell.2017.10.005
53. Dryhurst S, Schneider CR, Kerr J, et al. Risk perceptions of COVID-19 around the world. J Risk Res. 2020;1–13.
54. van der Bles AM, van der Linden S, Freeman ALJ, et al. Communicating uncertainty about facts, numbers and science. R Soc Open Sci. 2019;6(5):181870. doi:10.1098/rsos.181870
55. Roozenbeek J, Schneider CR, Dryhurst S, et al. Susceptibility to misinformation about COVID-19 around the world. R Soc Open Sci. 2020;7(10):201199. doi:10.1098/rsos.201199
56. Sani G, Janiri D, Di Nicola M, Janiri L, Ferretti S, Chieffo D. Mental health during and after the COVID-19 emergency in Italy. Psychiatry Clin Neurosci. 2020;74(6):372. doi:10.1111/pcn.13004
57. Moccia L, Janiri D, Pepe M, et al. Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: an early report on the Italian general population. Brain Behav Immun. 2020;87(April):75–79. doi:10.1016/j.bbi.2020.04.048
58. Fiorillo A, Gorwood P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur Psychiatry. 2020;63:1. doi:10.1192/j.eurpsy.2020.35
59. Shore JH, Hilty HMP, et al. Emergency management guidelines for telepsychiatry B.. 2007;29:199–206. doi:10.1016/j.genhosppsych.2007.01.013
60. Liu S, Yang L, Zhang C, et al. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry. 2020;7(4):e17–e18. doi:10.1016/S2215-0366(20)30077-8
61. Deslich S, Stec B, Tomblin S, Coustasse A. Telepsychiatry in the 21(st) century: transforming healthcare with technology. Perspect Health Inf Manag. 2013;10.
62. Amerio A, Odone A, Marzano L, et al. Covid-19: the last call for telepsychiatry. Acta Biomed. 2020;91(3):1–2. doi:10.23750/abm.v91i3.10337
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.