Back to Journals » Risk Management and Healthcare Policy » Volume 14
Knowledge, Attitudes, Practices, and Related Factors Towards COVID-19 Prevention Among Patients at University Medical Center Ho Chi Minh City, Vietnam
Authors Nguyen HB ![]() , Nguyen THM
, Nguyen THM ![]() , Tran TTT
, Tran TTT ![]() , Vo THN
, Vo THN ![]() , Tran VH, Do TNP, Truong QB
, Tran VH, Do TNP, Truong QB ![]() , Nguyen TH
, Nguyen TH ![]() , Ly LK
, Ly LK ![]()
Received 11 February 2021
Accepted for publication 14 April 2021
Published 24 May 2021 Volume 2021:14 Pages 2119—2132
DOI https://doi.org/10.2147/RMHP.S305959
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Hoang Bac Nguyen,1,2 Thi Hong Minh Nguyen,1 Thi Thanh Tam Tran,1 Thi Hong Nhan Vo,1 Van Hung Tran,1 Thi Nam Phuong Do,1 Quang Binh Truong,1,2 Thi Hiep Nguyen,3,4 Loan Khanh Ly3,4
1University Medical Center Ho Chi Minh City, Ho Chi Minh City, 700000, Vietnam; 2University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, 700000, Vietnam; 3Tissue Engineering and Regenerative Medicine Department, School of Biomedical Engineering, International University, Ho Chi Minh City, 700000, Vietnam; 4Vietnam National University, Ho Chi Minh City, 700000, Vietnam
Correspondence: Thi Hong Minh Nguyen Email [email protected]
Aim: This study measured the level of knowledge, attitudes and practices towards COVID-19 prevention and examined associated factors among patients at a national tertiary general hospital in Vietnam.
Methods: Adult patients admitted to University Medical Center during research period were recruited in a cross-sectional study, which employed a convenience sampling method with a 4-component questionnaire in order to examine the patients’ consciousness towards COVID-19 spreading prevention based on four aspects: demographic characteristics (10 items), knowledge (14 items), attitudes (6 items), and practices (7 items).
Results: The study involved 2769 respondents (18– 90 years) with the mean age of 38.05± 13.91 years. About two thirds of the respondents obtained diploma degree or higher (63.4%) and shared their living space with others (64.4%). The majority of patients settled in urban area (74.9%). All participants stayed informed about COVID-19, with the most commonly used channels like television (75.2%), the Internet (72.2%) and phone (69.8%). The vast majority showed sufficient knowledge (93.7%) and positive attitudes (76.3%). Just over half of participants remained good practiced of COVID-19 prevention (57.7%). On average, the factors of younger age, higher educational level, frequency and department of admission, and the number of COVID-19 informative channels were significantly associated with sufficient knowledge, positive attitudes, and good practices regarding preventive action against COVID-19 spreading. The optimistic attitude and having more undergoing chronic diseases were associated with the likelihood of well-practiced COVID-19 preventive measures (OR 3.63, 95% CI 1.54– 8.55, p=0.003 and OR 0.86, 95% CI 0.78– 0.98, p=0.02, respectively).
Conclusion: The results of this study demonstrated that the likelihood of good preventive practices in the fight against COVID-19 pandemic was influenced by attitudes and several sociodemographic factors. More drastic interventions for the prevention of COVID-19 should be widely furnished and equipped in hospitals, through various routes to maximize the efficiency and adherence to prevention practices.
Keywords: knowledge, attitudes, practices, COVID-19 prevention, patients, Vietnam
Introduction
Twenty-four days after Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was first detected in Wuhan, China in December, 2019, Vietnam identified the first active case of a patient travelled from China to Vietnam.1 Nearly one year later, on November 28, 2020, 1341 cases were confirmed in Vietnam, including entries or community transmission cases, with 1179 cases had recovered and been released from hospitals, and 35 patients died due to COVID-19, accounting for 2.6% of death rate.2,3 At that time, the whole globe recorded 62,544,800 active cases, and the death cases stood at 1,457,368.4 From these recorded data, Vietnam clearly is one of the very few countries that have achieved this remarkably low number of transmitted cases compared to the whole world, demonstrating a great success in preventing and controlling the spread of COVID-19 pandemic.5
In the fight against COVID-19, hospital is an essential place where symptom screening, early detection, and confirmed-case management activities take place. However, due to the threats of crowded populations, not excluding those at risk of being infected silently or with symptoms, close contact between patients and health practitioners, and the urge to be fully operational even during the period of social distancing, University Medical Center Ho Chi Minh City has become a more vulnerable environment for COVID-19 spreading. Evidently, during this period, there were four waves of COVID-19 outbreaks in Vietnam. Especially, nearly fifty percent of them were directly related to hospitals and the health sectors. Moreover, since the beginning of the outbreak, numerous hospitals have been suspended due to failure to meet the government’s standards of safe hospital environment for COVID-19 prevention and control.6,7 Therefore, in addition to the prevention and control of COVID-19 transmission in the community, the current national top-priority, the prevention and control of the spread of COVID-19 in hospital settings is also one of the vital keys to repel the attack and stop the spread of the COVID-19 pandemic.
It is crucial to raise knowledge, increase attitudes, and thereby promote appropriate practices for patients to control the spread of the disease while continuing to provide safe and effective health care services to the community. The fundamental measures, including medical declaration,8 limiting the change in family caregivers or suspension of patient visiting,9 are being implemented at University Medical Center Ho Chi Minh City and have demonstrated great effectiveness in controlling the pandemic spreading. They can, however, be hindered by the Eastern cultural and daily habits of patients and their relatives.10,11 Therefore, measuring the knowledge, attitudes, and practices (KAP) of patients in hospital environment would probably benefit the hospital authority in understanding the patient’s level of awareness about the pandemic, their response attitude, and preventive actions. Consequently, it is possible to develop and implement the most suitable programs to improve the KAP of patients in the hospital environment, thus, ensuring not only the safety of patients but also the quality of treatment.
Given the fact that there is an urgent need for scientific works on COVID-19 on many different population characteristics in the world and very few large-scale studies on KAP of Vietnamese patients were found. This study aims to measure the level of knowledge, attitudes, and practices towards COVID-19 prevention and examine the associated factors among patients using healthcare services to understand the KAP this specific population of the community has been equipped with. Consequently, this work would not only benefit the hospital managers and national governments to gain the latest scientific data to build municipal policies, butalso shed light on the fight against COVID-19 pandemic in general.
Methods
Study Design
This was a cross-sectional study.
Setting and Subjects
The study was carried out at one outpatient department and 14 inpatient departments at University Medical Center, Ho Chi Minh City, Vietnam from December 1, 2020 to January 5, 2021 using a convenience sampling method. Inclusion criteria: All patients aged 18 years or older, who visited and were treated at research sites during the study period and were fluent in Vietnamese. Exclusion criteria: Patients who were undergoing critical illness condition or being treated at Emergency or Intensive care unit (ICU); patients who were diagnosed with psychiatric or dementia; and those who refused to participate in the study.
Sample Size
The sample size of this study was determined by applying a sample size formula to estimate a single proportion, with a confidence level (CI) of 95%, margin of error of 2%, an average sample population of around 7400 patients per day and an estimated dropout rate of 30%, resulting in at least 2430 participants were necessary. However, the larger the sample size, the more emphasized the external validity and generalization of the research results.12,13 As a result, the original sample size calculated in this study was expanded up to 3000 participants to maximally improve its validity, representability, and generalizability.
Study Instrument
Data were collected through a self-report questionnaire developed by the authors after comprehensive reviews in compliance with Vietnam government’s guidelines and the currently available published studies,5,14–16 consisting of 2 main parts: (1) sociodemographic characteristics and (2) KAP towards COVID-19 prevention.
The first part of the survey investigated sociodemographic related information on the patients, such as gender, age, education level, living residence, religion, address of residence, and occupation. Item of medium channels through which the patient received COVID-19 information was also included as a nominal variable. Places and frequency of hospital admission were also collected. Finally, the underlying chronic disease, presented as a nominal variable, was also included in this section.
The second part of the questionnaire examined for the patient’s KAP, which was defined by three sub-components, namely knowledge, attitudes, and practices of COVID-19 precautionary measures. There were 14 yes/no questions to gather information about the respondent’s level of knowledge. Each item was counted as 1 if the patient chose the correct answer and 0 for the wrong answer, giving it a total score of 0–14. There was no inverse question included in this content. The patient’s knowledge was classified into three levels based on Bloom’s cut-off classification.17–19 Specifically, knowledge was defined as insufficient or low if the total score was ≤ 8 points, corresponding to less than 60%; moderate if the total score ranged 9–11 (60–80%); and high, good, or sufficient if the total score was ≥ 12 (80–100%).
In section 2, 6 Likert 5-scale questions were used to determine the patient’s attitude, from 1 (completely disagree) to 5 (completely agree). The total score for this section ranged from 6 to 30 with a score ≤ 17 was categorized as negative; between 18 and 24 as neutral; and ≥ 25 as positive attitudes, applying Bloom’s cut-off point.
Finally, 7 yes/no questions were employed to measure patient’s practice of prevention. The correct answer received 1 point while the wrong one received 0, resulting in a total score of 7. By referencing Bloom’s cut-off point, a threshold value of ≤ 3 was determined to categorize the patient’s practice level as poor; 4–5 as fair; and 6–7 as good practice.
The first draft version of the questionnaire was sent to three experts in scientific and nursing research to comment on its clarity, validity, succinctness, reliability and interestingness.20 Then, 20 potential respondents were asked for their opinion on whether the questionnaire was clear and understandable. Cronbach’s Alpha was calculated to evaluate the internal consistency of the three sections with the values of KAP being 0.62, 0.65, and 0.68, respectively, indicating an acceptable reliability.
Data Collection
Eligible patients at one examination department and 14 inpatient departments at University Medical Center Ho Chi Minh City were reached and informed about the research purpose and other relevant information in order to obtain their informed consent before enrolling in the investigation.
Data Analysis
Collected data were organized and analyzed using IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY, USA). The mean, standard deviation (SD), frequency, and proportion were used to display demographic characteristics. Meanwhile, statistically significant differences in KAP level when comparing among dichotomous or nominal independent variables were examined using one-way ANOVA with p<0.05 being the value of statistical significance. To identify factors related to KAP, logistic regression analysis was also employed.
Ethical Approval
The study was conducted in compliance with the Declaration of Helsinki. Official ethical approval was obtained from the Medical Ethics Committee of University Medical Center Ho Chí Minh City, Viet Nam before proceeding with data collection (Approval No.51/GCN-HĐĐĐ-UMC, 25/11/2020). Additionally, an informed consent was signed by each participant before enrolling in the study in compliance with ethical standards in scientific research. The patients responded to the questionnaire anonymously with no identifying information required.
Results
Out of 3000 patients being approached, 2791 patients met the research criteria and were enrolled in the study. Then, 2769 completely fulfilled surveys were collected and analyzed, equivalent to an overall response proportion of 92.3%. Seventeen respondents did not complete the survey and the remaining were inappropriate responses.
The Characteristics of the Study Participants
Table 1 presents the distribution of the sociodemographic characteristics of participants among 2769 patients with 54.8% female and 62.1% aged under 40 years (38.05±13.91, range 18–90 years). Most of the respondents obtained diploma degree or above (59.8%) and shared their living space with others (64.4%). While 100% of respondents were informed about COVID-19, only one-thirds stayed updated with COVID-19 news from at least five sources of information. The most common medium platforms for COVID-19 information were television (75.2%), the Internet (72.2%), and phone (69.8%). Only 36% of patients demonstrated that they kept up-to-date on disease-related news through hospital channel.
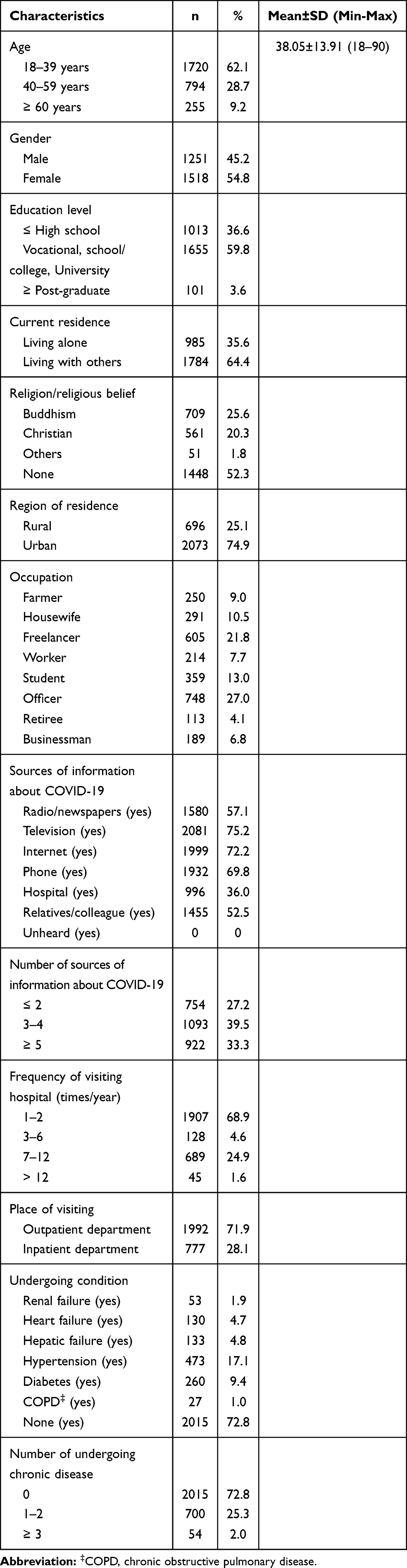 |
Table 1 Sociodemographic Characteristics of Study Subjects (n=2769) |
Knowledge
Table 2 shows the findings on the respondents’ knowledge towards COVID-19 prevention. The mean score of knowledge was 13.35±1.16, equivalent to a correction rate of 95% (13.35/14). Almost all participants had sufficient knowledge (93.7%). Additionally, there was a significantly low proportion of patients with moderate or insufficient knowledge of pandemic controlling, around 5.5% and 0.8%, respectively. Out of 14 items measuring knowledge of the participants, almost all statements had their correct response rate of at least 92%. In contrast, only 77% of participants gave the correct answer when being asked “People in close contact or eating wild animals are likely to be infected with COVID-19”.
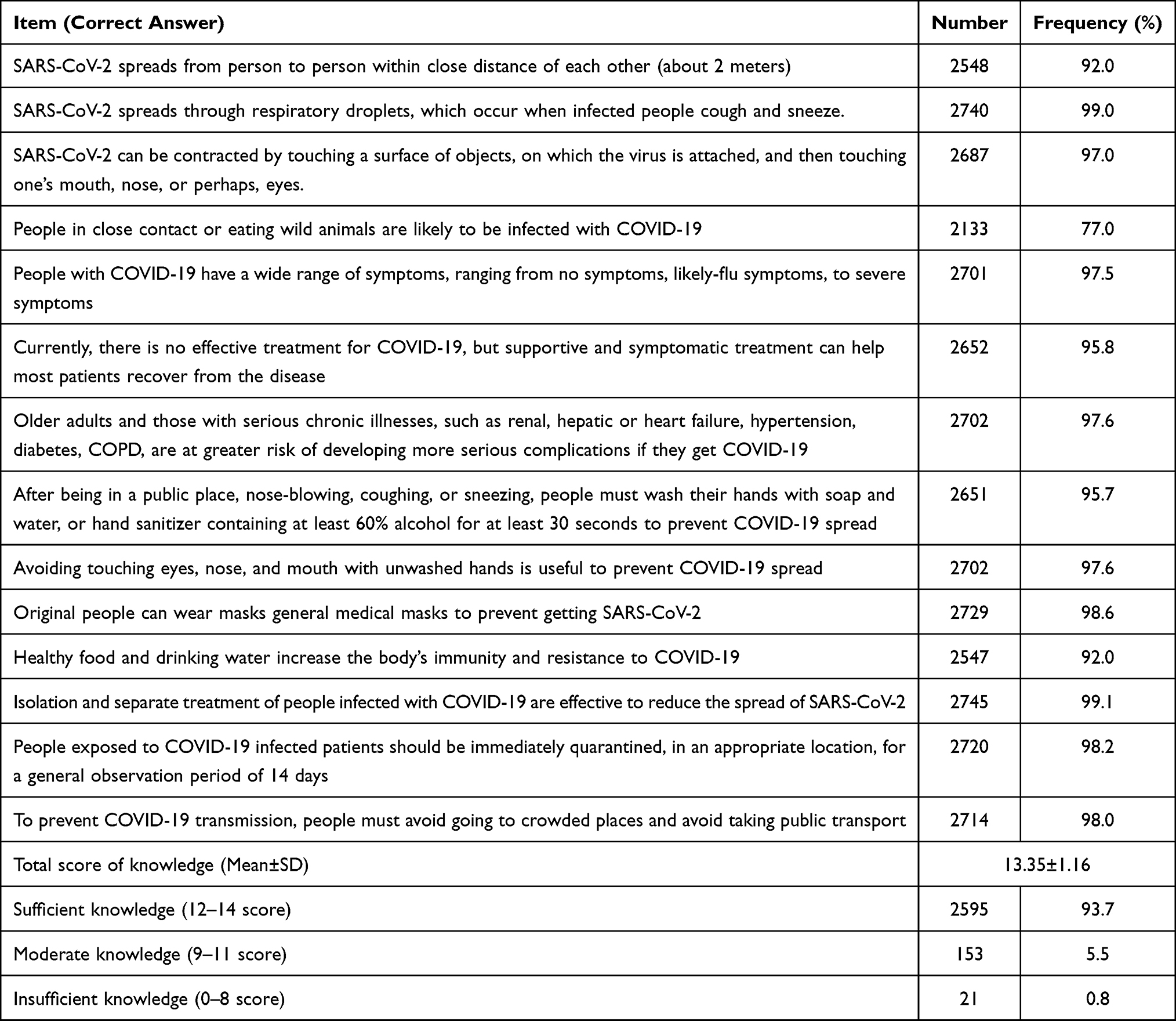 |
Table 2 Patients’ Knowledge Towards COVID-19 Prevention (n=2769) |
Attitude
The attitudes of participants towards COVID-19 prevention were presented in Table 3, using 5-point Likert scale with a total mean score of 26.6±3.48 (range 1–30). While most respondents strongly agreed on attitude statements, the mean score of item “It is necessary to wear mask during this current period” was only 3.58±1.79. The proportion of belief in successful COVID-19 controlling was 76.3%. Meanwhile, 22.6% of patients carried neutral attitude and this value for negative attitude was only 1.2%.
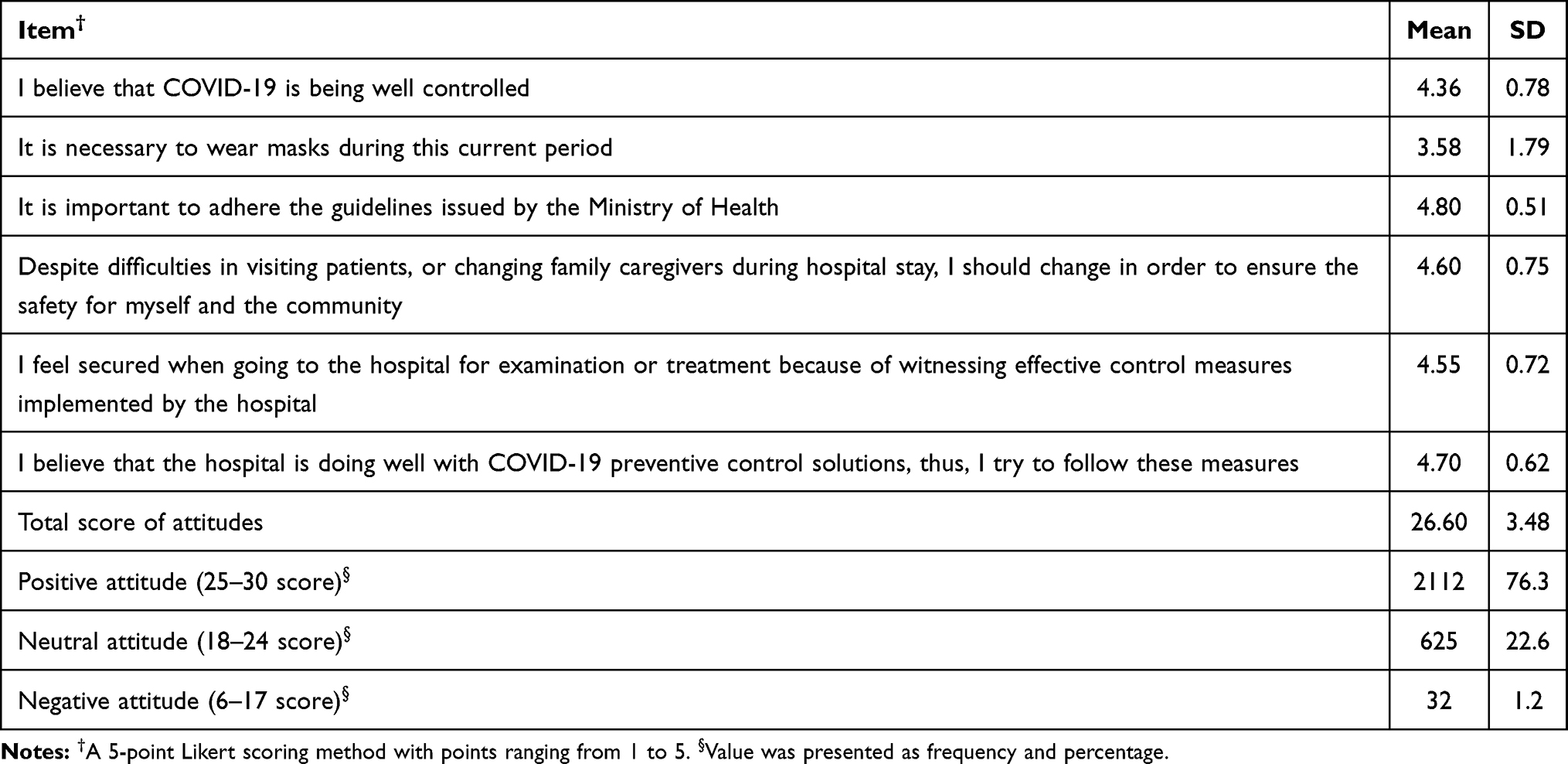 |
Table 3 Patients’ Attitudes Towards COVID-19 Prevention (n=2769) |
Practice
Table 4 shows the results regarding the patients’ practices towards COVID-19 preventive action. This section had a mean of total score was 5.39±1.49 with 57.7% of patients remained good practice towards COVID-19 prevention. There was up to 15.7% of patients chose only 0–3 correct answers out of seven, equivalent to poor practice. Furthermore, a great number of patients, 1134 out of 2769 patients (41%), purposefully bought medications without consulting their physicians when having no abnormal symptoms. Meanwhile, only approximately two-thirds of patients (63.8%) in this study reported the utility of a beneficial means of communication to consult with doctors about the demand of direct examination at hospital. The rates of keeping sanitizers containing at least 60% alcohol for frequent hand washing and active online registration to limit crowded gathering were quite uncommon, only at 71.2% and 76.2%, respectively.
 |
Table 4 Patients’ Practices Towards COVID-19 Prevention (n=2769) |
Differences on Comparison KAP Among Sociodemographic Characteristics
Table 5 compares the scores of the patients’ knowledge, attitudes, and practices in relation to their sociodemographic characteristics. Firstly, there were statistically differences in the mean score of knowledge among age groups and educational level (p<0.001). Specifically, the 18–39 aged group had the highest mean knowledge score (13.45±0.94), followed by the 40–59 and ≥ 60 aged groups that scored 13.21±1.39 and 13.09±1.55, respectively. Similarly, people holding diploma/bachelor’s degree had significantly higher score than others (13.49±0.85, p<0.001). Noticeably, the patients who lived alone tended to have significantly higher knowledge towards COVID-19 prevention than those sharing their spaces with others (13.48±0.79 as compared to 13.28±1.31 with p<0.001). There were also statistical differences in COVID-19 prevention knowledge among the patients with chronic illnesses, different occupations, location of residence, frequency and place of hospital visiting, and number of COVID-19 related information sources.
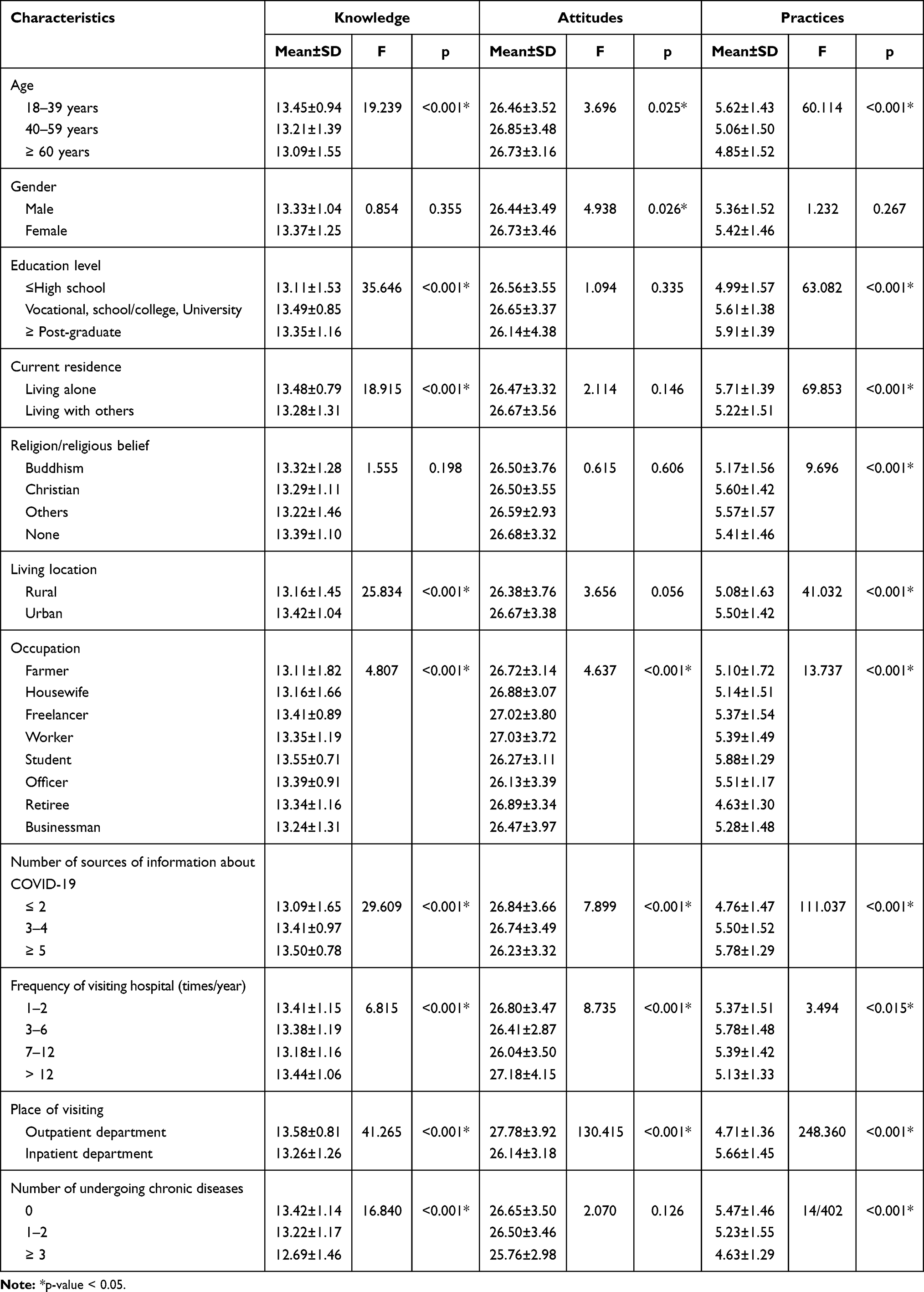 |
Table 5 Differences on Comparison Knowledge, Attitudes and Practices Among Sociodemographic Characteristics (n=2769) |
These significant differences were also witnessed when comparing the practice scores across age groups, education level, residential status, region of living, numbers of COVID-19 information sources, and the amount of their chronic diseases, with p<0.015 or p<0.001. Moreover, the practice scores were also significantly different among different religious groups and occupations (p<0.001). Interestingly, while the mean scores of knowledge and attitudes of outpatients were statistically higher than those of inpatients (p<0.001), at 4.71±1.36 and 5.66±1.45, respectively.
In terms of attitudes, significant differences were observed among multiple factors including age groups, gender, occupation, the amount of information sources, the frequency of visiting hospital, and the department of admission (p<0.001). Female respondents showed much optimistic attitude (26.73±3.46) compared to male counterparts (26.44±3.49) with p=0.026. In contrast to knowledge and practices, those who gathered information from few sources yielded a higher attitude score (p<0.001).
Associated Factors to Sufficient Knowledge, Optimistic Attitude and Good Practice Regarding COVID-19 Prevention
Table 6 reveals the factors associated with a good KAP towards COVID-19 prevention. The prevalence of sufficient knowledge was negatively associated with the following factors: aged 40–59 (OR 0.51, 95% CI 0.35–0.75, p=0.001) or older than 60 (OR 0.48, 95% CI 0.27–0.87, p=0.015), rural region (OR 0.57, 95% CI 0.40–0.82, p=0.002), visiting hospital monthly or more (OR 0.27, 95% CI 0.09–0.88, p=0.003). This, however, was positively correlated with factors, such as undergraduate degree or higher (OR 1.95, 95% CI 1.27–3.02, p=0.002), number of COVID-19 information sources (OR 1.47, 95% CI 1.31–1.66, p<0.001), and being admitted to inpatient department (OR 6.99, 95% CI 2.46–11.49, p<0.001).
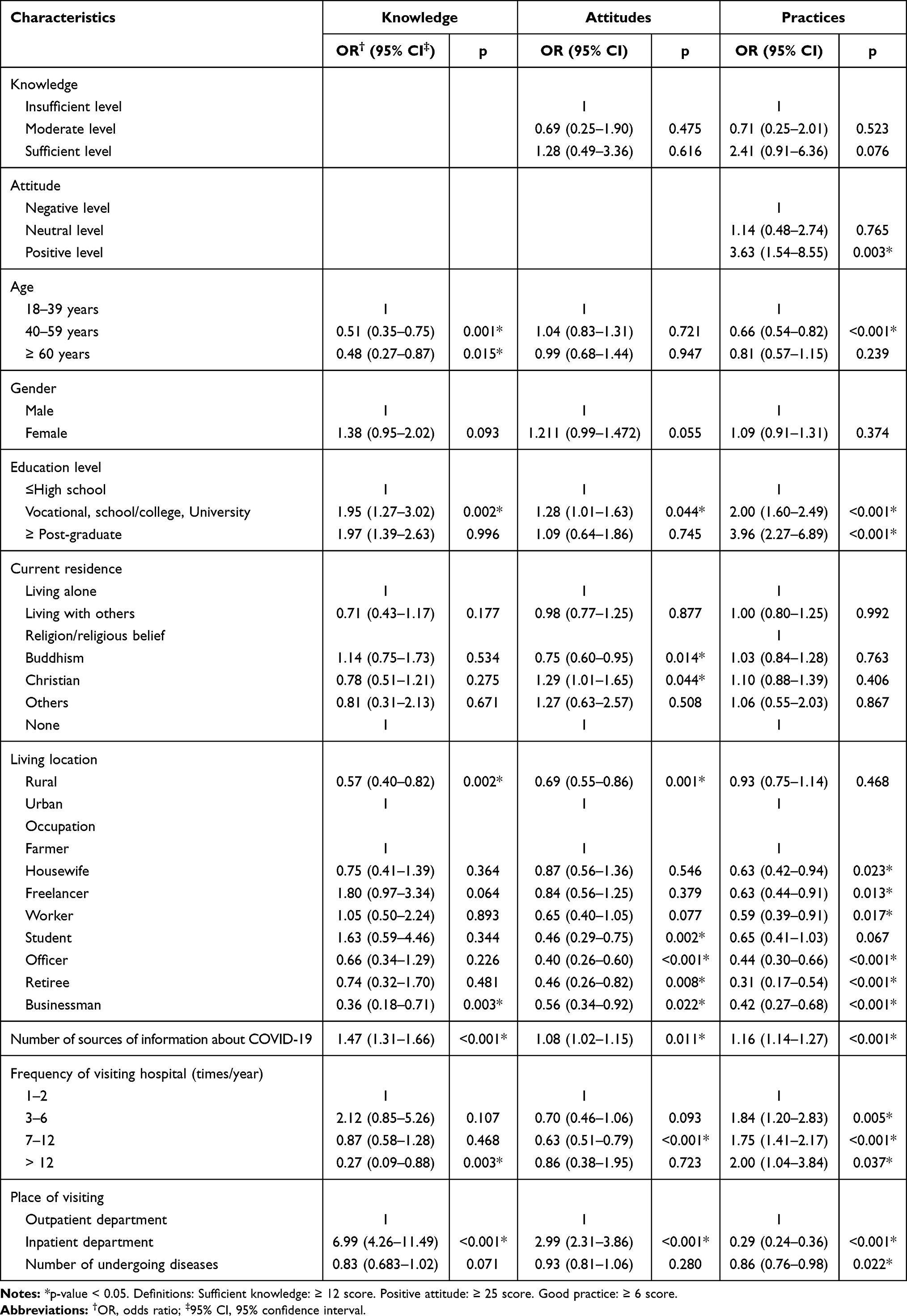 |
Table 6 Associated Factors to Sufficient Knowledge, Optimistic Attitudes and Good Practices Regarding COVID-19 Prevention (n=2769) |
There were fewer factors associated with positive attitudes likelihood, including undergraduate degree or above (OR 1.82, 95% CI 1.01–1.63, p=0.044), having Christian faith (OR 1.29, 95% CI 1.01–1.65, p=0.044) or Buddhism (OR 0.75, 95% CI 0.60–0.95, p=0.014), being in specific occupations (eg, student, officer, retiree, or businessman), visiting hospital 7–12 times per year (OR 0.63, 95% CI 0.51–0.79, p<0.001), rural residence (OR 0.69, 95% CI 0.55–0.86, p=0.001), number of COVID-19 information sources (OR 1.08, 95% CI 1.02–1.15, p=0.011), and admission to inpatient department (OR 2.99, 95% CI 2.31–3.86, p<0.001).
The prevalence of appropriate practices was associated with positive level of attitudes (OR 3.63, 95% CI 1.54–8.55, p=0.003) and almost all other variables.
Discussion
Due to the current complicated situations of the COVID-19 outbreak, KAP of patients who are especially vulnerable due to poor health conditions and their exposure to many risk factors during medical examinations and treatments, is of great importance. This study aims to measure the patients’ KAP in preventing the spread of the COVID-19 pandemic using the convenience sampling method.
From the findings of this study, the majority of participants in this study were female (54.8%) and the percentage of highly educated patients was quite high as of 63.4%. The demographic features of this study were nearly similar to those found in previous studies conducted in Ho Chi Minh City (55.7% and 61.9%, respectively)21 and in Hanoi (78.3% and 68.7%, respectively).5 In addition, this study also noticed the highest use of television and online channels of participants in obtaining COVID-19 related information and news that were consistent with the highlight of COVID-19 information sources found in other studies in Vietnam,5,21 and in other continents.22 In Vietnam, in January 2020, the Internet users proportion was 70%, while active social media users stood at 67%, accounting for around two-thirds of the whole population, with the average daily use of about 6.5 hours.23 In addition to some official sources of COVID-19 information that are hourly updated by international organizations such as Centers for Disease Control and Prevention (CDC), World Health Organization (WHO) through their websites, Vietnamese government has also been actively strengthening the community education about the pandemic through many preferred social media (eg Facebook, Instagram, YouTube and so on).24,25 Using these social media as a means of communication, all individuals currently residing in Vietnam are kept posted with newest COVID-19 information, thus noticeably improving the knowledge of the community.
Overall, most of the respondents correctly answered the items measuring their knowledge of COVID-19 prevention (95%) with 93.7% of them demonstrated adequate knowledge on this topic. This high level of knowledge was similar to the results in another study in Vietnam with 92.2% of patients holding good knowledge5 but significantly higher than studies conducted in other countries, such as Bangladesh of around 48.3%26 and 54.9%,27 and North-Central Nigeria.28 Furthermore, the overall rate of correct responses to the knowledge questions in this study was much higher than that reported in previous studies at 88.75%,22 81.64%,14 80.5%,29 and 90%.30 This can be partially explained by the characteristics of the subjects in this study. First, the participants of this study were highly educated (63.4%) and most of them were young people (62.1%) who used a variety of medium channels, especially online platforms to receive news. Besides, the majority of the participants resided in big cities, such as Hanoi and Ho Chi Minh City, allowing for spontaneous access to medical examination and treatments (74.9%). In addition, there was a fact that since the pandemic evolved in China, Vietnamese government was aware of the highly infected possibility due to geographic contiguity, therefore, has been drastically educating and informing the public about the pandemic as well as disease control and prevention. The rapid acts of Vietnamese authorities not only provide the community with accurate and updated information regarding COVID-19 pandemic but also enhance the public awareness in the most complete and effective way.
This study also revealed a great proportion of participants having positive attitudes towards successful pandemic control (76.3%) with an average score of 26.6±3.48 (range 6–30). This finding was similar to that in a community-based study in the Kingdom of Saudi Arabia14 and higher than in another work conducted in Vietnam previously.5 Interestingly, in the current study, the highest attitudes scores were found on patients’ opinions about the importance of being in compliance with the government and the Ministry of Health’s guidelines and the strong belief in health care systems and their disease control measures (at 4.8±0.51 and 4.7±0.62, respectively).
In this study, we observed that the participants acquired adequate and sufficient knowledge about the disease, which led to positive attitudes and the optimistic prospects of COVID-19 control. Despite the severity of COVID-19 in many regions around the world, Vietnam’s outstanding achievements in disease control and the development of COVID-19 vaccine may contribute to reassuring and strengthening patients’ mentality against the current global emergency of COVID-19. Moreover, hospitals have been implementing many rigorous pandemic control and prevention measures and policies including suspension of inpatient visiting, mandatory medical declaration and face-covering, widely equipped hand hygiene kits, educational information, social distancing rule, and warnings broadcasting within hospital locations. These actions play an important role in enhancing clients’ confidence and optimism about the disease in general as well as promoting their safety within hospital environments, particularly those that have been confirmed and recommended in existing work.31 However, compared to a significant percentage of knowledge (93.7%), the proportion of positive attitudes was fairly low. This could be due to the fact that major social media platforms have been continuously exaggerating about the severity and high mortality of COVID-19 disease happened in many developed countries that consequently imposed negativity on patients’ beliefs in the prospect of pandemic control.
In terms of practices, 57.7% of participants presented appropriate practices in COVID-19 control and prevention in hospital environment. Although the good practice rate in this study was lower than that in Huynh et al,21 the scale of the current study included 7 items, significantly more than the 3-item scale in the reference work.
Another considerable finding was that the restriction of visiting and family caregivers during hospital stays and required face-covering were complied with by up to 98.3% and 95.4% of respondents, respectively. The findings in this study were considerably higher than those in the previous study in Vietnam where the response rate about the necessity of wearing masks in public was only 83.3%.21 This demonstrated the proactive and compliance of patients in protecting themselves and the community from pandemics, thus promoting a safe hospital environment. Vietnam is a Southeast Asian country with Confucianism and family culture that has been deeply embedded in the community’s perception and daily life. Consequently, the culture of visits and taking care from relatives during the hospital stay are believed to have significant effects on the patient’s mental health and recovery. Despite these cultural features, the patient’s remarkably high obligation to visiting suspension reflects their timely awareness in helping to protect the community as well as the success of hospital authority in implementing the control and prevention policies. However, nearly a third of participants failed to practice some anti-epidemic measures such as keeping hand hygiene products (28.8%), using online registration provided by the hospital (23.8%) or consulting medical staff about the necessity of direct examination (36.2%). This is probably due to the widespread availability and feasibility of self-purchase medicine needless doctor prescription, which makes patients more inclined to follow the previous prescriptions rather than complying with reexamination schedule and doctor order.
As expected, a positive relationship between high academic degree and good level of knowledge was found in this study. Similarly, this study also reported a significant association between sufficient knowledge and urbanity as a region of residence. These results can be because those being young or settling in modern cities had more advantageous opportunities to stay informed with the latest information about COVID-19 controlling via various medium channels. In terms of factors associated with the KAP, a positive correlation was found between knowledge and practices but not between attitudes and practices in Huynh et al,21 this study revealed an opposite trend, in which positive attitudes were associated with the prevalence of good practices (OR 3.63, 95% CI 1.54–8.55, p=0.003), but not for knowledge factor. Correlation between attitudes and practices was also found in other studies (OR 1.43, 95% CI 1.19–1.71, p<0.001).26 A significant proportion of the patients’ positive attitudes towards pandemic corresponded to good practice level is consistent with the previously developed knowledge-attitude-behavior/practice model.32,33
Moreover, we also observed that younger people tended to gain sufficient knowledge and practices statistically better than older people (p<0.001 for both cases). The findings were in agreement with previous patient-based study that demonstrated a relation between young age and knowledge level,34 but were different from others that revealed a positive correlation between age and knowledgeable level.14,29 Although adults seem to pay more attention to their health due to the higher probability of being infected with COVID-19,14,35 younger patients were able to get immediate access to the latest and accurate news about COVID-19 through multiple social media platforms, helping them always stayed updated and had higher knowledge level. This encourages the active usage of these friendly and pervasive media in informing target audiences about COVID-19 information. On the other hand, it is not surprising to see the higher likelihood of good knowledge, positive attitudes, and appropriate practices among high educational level, urban area residents, and the number of medium channels providing COVID-19 information groups.
However, the more frequent the hospital visits, the higher the likelihood of good practices. This is thanks to the patients’ intensive exposure to the hospital’s mandatory policies during their frequent examination and treatment that enhanced their good practices towards controlling and preventing the spread of the disease. When considering the correlations between knowledge, attitudes, frequency of hospital visits, and good practices, the effectiveness of establishing compulsory prevention policies by the hospital authority for successful prevention of COVID-19 spreading has been proven.
Strengths
The study was conducted on a very large-scale population of patients who came to be examined and treated in both outpatient and inpatient departments at University Medical Center Ho Chi Minh City. It is a national tertiary general hospital with a variety of patients from many regions across the country seeking medical examination and treatment. Therefore, the subjects in this study were highly representative of the Vietnamese demographic characteristics. In addition, the questionnaire used to collect data was designed with careful and thorough referencing from not only previous studies but also actual guidelines that were issued by the Vietnamese government. This helps to maximize the accuracy and relevance of the questionnaire to the current context of COVID-19.
Limitations
Although COVID-19 topic and related scientific information have gained a great interest among scientists around the world, there is lack of studies conducted on patient population. Therefore, it is challenging to find sufficient literature serving as references for this type of study. Moreover, the questionnaire used in this study was developed based on a limited number of relevant publications available as references, resulting in a not quite high Cronbach’s alpha. Despite this, the Cronbach’s alpha higher than 0.6 is considered to be acceptable, presenting appropriate reliability for the current study. Additionally, even though the participants were fully instructed on how to respond to the questionnaire, information bias was unavoidable due to the nature of its self-answering questionnaire.
Conclusions
Knowledge, attitudes and practices of patients on COVID-19 prevention within hospital environment are relatively good, reflecting the efforts of Vietnamese government in general and University Medical Center Ho Chi Minh City in particular in preventing and controlling the spread of COVID-19 pandemic. These praiseworthy results are achieved not only by government’s rigorous and drastic measures but also by the policies set by the hospital authority, implying that pandemic prevention will be most effective if the efforts are initiated from every nuclear unit, not just from the national level. Hospitals need to comply with government guidelines and actively develop their own preventive measures in accordance with their own conditions and characteristics, as well as apply scientific and technological achievements into medical examination and treatment such as remote consultation, highlighted reminder signals of face-covering and washing hand. In addition, it is recommended that the state and hospital authorities need to develop specific measures to enhance the KAP of the patient groups that are likely to exhibit low KAP, to strengthen the community education through the most preferred mass media, and to improve the health of people. Besides, given the fact that the study participants were recruited from a hospital environment, the research findings were less likely to truly representpublic characteristics. Therefore, more future studies on subjects such as people in the community would probably be able to correct this limitation. Furthermore, the research measuring healthcare practitioners’ KAP should also be recommended.
Data Sharing Statement
The data that support the findings of this study are available within this article.
Acknowledgments
The authors sincerely thank all the patients and their relatives, physicians, and nurses in outpatient and inpatient departments at University Medical Center Ho Chi Minh City, Vietnam for their assistance in completing this study. We would also like to thank Nguyen Huu Thinh for his advice and support throughout this study. Truong Quang Binh is the founder and instructor of this research work.
Disclosure
The authors reported no conflicts of interest for this work.
References
1. World Health Organization. Coronavirus disease (COVID-19) situation report-126; 2021. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200525-covid-19-sitrep-126.pdf?sfvrsn=887dbd66_2.
2. Health Mo. Trang tin về dịch bệnh viêm đường hô hấp cấp COVID-19; 2020. Available from: https://ncov.moh.gov.vn/web/guest/dong-thoi-gian?p_p_id=com_liferay_asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_nf7Qy5mlPXqs&p_p_lifecycle=0&p_p_state=normal&p_p_mode=view&_com_liferay_asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_nf7Qy5mlPXqs_delta=10&p_r_p_resetCur=false&_com_liferay_asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_nf7Qy5mlPXqs_cur=5.
3. JohnsHopkins. Coronavirus resource center; 2020. Available from: https://coronavirus.jhu.edu/region/vietnam.
4. CoronaBoard. COVID-19 dashborad; 2020. Available from: https://coronaboard.com/global/.
5. Ha VN, Tran TTH, Nguyen TAV, Tran NQL, Truong QT. Knowledge, attitudes, and practices of the Vietnamese as key factors in controlling COVID-19. J Commun Health. 2020;45(6):1263–1269. doi:10.1007/s10900-020-00919-4
6. Health Mo. From 8:00 pm on August 19, E Hospital stopped receiving medical examination and treatment: the Ministry of Health worked overnight on the prevention of COVID-19 epidemic; 2020. Available from: https://ncov.moh.gov.vn/-/tu-20h-toi-ngay-19-8-benh-vien-e-dung-tiep-nhan-kham-chua-benh-bo-y-te-lam-viec-ngay-trong-em-ve-cong-tac-chong-dich-covid-19.
7. Duy C, Nong VM, Van Ngo A, et al. Nosocomial Coronavirus disease outbreak containment, Hanoi, Vietnam, March–April 2020. Emerg Infect Dis. 2020;27(1):10. doi:10.3201/eid2701.202656
8. University Medical Center HCMC. Sàng lọc COVID-19 tại nơi chữa bệnh; 2021. Available from: http://www.bvdaihoc.com.vn/Home/ViewDetail/2140#maincontent.
9. City UMCHCM. Bệnh viện Đại học Y Dược TPHCM quy định về việc thăm bệnh, nuôi bệnh trong mùa dịch COVID-19; 2021. Available from: http://www.bvdaihoc.com.vn/Home/ViewDetail/2166#maincontent.
10. Lipson JG, Meleis AI. Issues in health care of Middle Eastern patients. West J Med. 1983;139(6):854.
11. Oheneba-Sakyi Y, Takyi BK. African Families at the Turn of the 21st Century. Greenwood Publishing Group; 2006.
12. Cavana R, Delahaye B, Sekeran U. Applied Business Research: Qualitative and Quantitative Methods. John Wiley & Sons; 2001.
13. Faber J, Fonseca LM. How sample size influences research outcomes. Dent Press J Orthod. 2014;19(4):27–29. doi:10.1590/2176-9451.19.4.027-029.ebo
14. Al-Hanawi MK, Angawi K, Alshareef N, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a cross-sectional study. Front Public Health. 2020;8. doi:10.3389/fpubh.2020.00217
15. CDC CfDCaP. People with certain medical conditions; 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/groups-at-higher-risk.html.
16. World Health Organization. COVID-19 Strategy Update 14 April 2020; 2020. Available from: https://www.who.int/publications/m/item/covid-19-strategy-update. Accessed January 10, 2021.
17. Yimer M, Abera B, Mulu W, Bezabih B. Knowledge, attitude and practices of high risk populations on louse-borne relapsing fever in Bahir Dar city, north-west Ethiopia. Sci J Public Health. 2014;2(1):15–22. doi:10.11648/j.sjph.20140201.13
18. Koo H-C, Poh B, Ruzita A. Assessment of knowledge, attitude and practice towards whole grains among children aged 10 and 11 years in Kuala Lumpur. Int J Food Sci Nutr Diet. 2015;4(1):171–177. doi:10.19070/2326-3350-1500032
19. Seid MA, Hussen MS. Knowledge and attitude towards antimicrobial resistance among final year undergraduate paramedical students at University of Gondar, Ethiopia. BMC Infect Dis. 2018;18(1):312. doi:10.1186/s12879-018-3199-1
20. Jenn NC. Designing a questionnaire. Malay Fam Physician. 2006;1(1):32.
21. Huynh G, Nguyen MQ, Tran TT, et al. Knowledge, attitude, and practices regarding COVID-19 among chronic illness patients at outpatient departments in Ho Chi Minh City, Vietnam. Risk Manag Healthc Policy. 2020;13:1571. doi:10.2147/RMHP.S268876
22. Ejeh FE, Saidu AS, Owoicho S, et al. Knowledge, attitude, and practice among healthcare workers towards COVID-19 outbreak in Nigeria. Heliyon. 2020;6(11):e05557. doi:10.1016/j.heliyon.2020.e05557
23. Kemp S. Digital 2020 Vietnam. Datareportal; 2021. Available from: https://datareportal.com/reports/digital-2020-vietnam.
24. Tran TPT, Le TH, Nguyen TNP, Hoang VM. Rapid response to the COVID-19 pandemic: Vietnam government’s experience and preliminary success. J Glob Health. 2020;10(2). doi:10.7189/jogh.10.020502
25. La V-P, Pham T-H, Ho M-T, et al. Policy response, social media and science journalism for the sustainability of the public health system amid the COVID-19 outbreak: the Vietnam lessons. Sustainability. 2020;12(7):2931. doi:10.3390/su12072931
26. Ferdous MZ, Islam MS, Sikder MT, Mosaddek ASM, Zegarra-Valdivia J, Gozal D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: an online-based cross-sectional study. PLoS One. 2020;15(10):e0239254. doi:10.1371/journal.pone.0239254
27. Haque T, Hossain KM, Bhuiyan MMR, et al. Knowledge, attitude and practices (KAP) towards COVID-19 and assessment of risks of infection by SARS-CoV-2 among the Bangladeshi population: an online cross sectional survey. J Infect Dev Ctries. 2020.
28. Reuben RC, Danladi MM, Saleh DA, Ejembi PE, Noonan D, Simmons LA. Knowledge, attitudes and practices towards COVID-19: an epidemiological survey in North-Central Nigeria. J Commun Health. 2020;45:1–14. doi:10.1007/s10900-019-00710-0
29. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E, Tu W-J. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. doi:10.1371/journal.pone.0233668
30. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745. doi:10.7150/ijbs.45221
31. Hu VH, Watts E, Burton M, et al. Protecting yourself and your patients from COVID-19 in eye care. Commun Eye Health. 2020;33(108):S1.
32. Bettinghaus EP. Health promotion and the knowledge-attitude-behavior continuum. Prev Med. 1986;15(5):475–491. doi:10.1016/0091-7435(86)90025-3
33. Rahbar T, Garg S, Tripathi R, Gupta V, Singh M. Knowledge, attitude, behavior and practice (KABP) regarding HIV/AIDS among pregnant women attending PPTCT programme in New Delhi”. J Commun Dis. 2007;39(3):179–184.
34. Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020;13:1949. doi:10.2147/IDR.S258736
35. Spagnuolo R, Larussa T, Iannelli C, et al. COVID-19 and inflammatory bowel disease: patient knowledge and perceptions in a single center survey. Medicina. 2020;56(8):407. doi:10.3390/medicina56080407
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.