Back to Journals » Patient Preference and Adherence » Volume 20
Knowledge, Attitudes, and Practices Toward Insomnia Among Insomnia Patients
Authors Fang Y, Wang S, Li G, Deng J, Tian Y, Wan Z, Yang D, Wang Q
Received 21 November 2025
Accepted for publication 14 February 2026
Published 13 March 2026 Volume 2026:20 583503
DOI https://doi.org/10.2147/PPA.S583503
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yu Fang,1,* Shumin Wang,1,* Guiyan Li,1 Jie Deng,2 Yanyan Tian,1 Ziyi Wan,1 Dongdong Yang,1 Qiaoling Wang1
1Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 2Jinniu District Hospital of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiaoling Wang, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China, Tel +86-13708007503, Email [email protected]
Purpose: This study aimed to investigate the knowledge, attitudes, and practices (KAP) toward insomnia among patients.
Patients and Methods: A cross-sectional survey was conducted from May 20, 2023, to March 25, 2024, in the Neurology Outpatient Department at the Affiliated Hospital of Chengdu University of Traditional Chinese Medicine. Data were collected through the distribution of questionnaires.
Results: A total of 568 valid questionnaires were analyzed. Of these respondents, 368 (64.79%) were female. Notably, 156 (27.46%) exhibited symptoms of anxiety, and 103 (18.13%) were found to be experiencing depressive symptoms. The mean knowledge, attitude, and practice scores were 5.50± 2.20 (possible range: 0– 9), 24.53± 3.21 (possible range: 8– 40), and 28.55± 4.28 (possible range: 8– 40), respectively. The results of pathway analysis showed that knowledge was directly associated with both attitude (β=0.240, P=0.010) and practice (β=− 0.128, P=0.013), and attitude was associated with practice (β=0.179, P=0.010). Furthermore, an indirect association was observed between knowledge and practice through attitude (β=0.043, P=0.010).
Conclusion: The study found patients’ insomnia knowledge and attitudes are poor, yet their practices are proactive. Since knowledge and attitudes were associated with practice, clinical programs should consider implementing educational interventions to improve understanding and foster positive attitudes toward insomnia management.
Keywords: knowledge, attitude, practice, insomnia, cross-sectional study
Introduction
Insomnia, a significant public health issue, is characterized by difficulty falling asleep (initial insomnia), maintaining sleep (middle insomnia), and premature waking (terminal insomnia). These sleep disturbances not only compromise daytime functionality but also lead to fatigue, depression, anxiety, and other adverse symptoms.1,2 The condition’s prevalence ranges between 10–20%, with about 50% of these cases being chronic, defined as experiencing symptoms at least three nights a week for more than a month.3
In China, approximately 15% of the population suffers from insomnia.4 Epidemiological data indicate that insomnia rates are higher among women and increase with age.5,6 Additionally, sleep disturbances are closely linked to psychological disorders such as depression and anxiety.7 A study highlights that nearly 30% of people are affected by psychological disorders resulting from high-pressure jobs and hectic lifestyles, with many suffering from varying degrees of insomnia.8,9
Cognitive Behavioral Therapy for Insomnia (CBT-I) is advocated as the primary treatment approach. However, pharmacologic interventions are frequently employed to manage this disorder.10 The pharmacological arsenal includes various drug classes such as benzodiazepines (BZD), non-benzodiazepine GABA-A modulators, dual orexin receptor antagonists (DORAs), melatonin receptor agonists, and histamine antagonists, all of which have been approved for treating insomnia.11
The Knowledge, Attitude, and Practice (KAP) model suggests that individual behaviors are shaped by one’s knowledge and attitudes, which is a fundamental concept in public health.12 This model emphasizes the importance of understanding health-related behaviors through assessments of knowledge, attitudes, and behavioral practices, often conducted via KAP surveys.13 By exploring these elements, researchers can identify gaps in knowledge, misconceptions, and potential resistance to treatment among patients. These insights enable the development of more effective personalized treatment plans and educational interventions that enhance self-management capabilities and, consequently, improve quality of life.
Given the close association between insomnia and various psychological and physical ailments, such as depression, anxiety, and cardiovascular diseases, a deep understanding of KAP in insomnia patients is crucial not only for managing insomnia but also for preventing these related health issues. Previous research has indicated that insomnia patients frequently experience frustration and misconceptions, which may stem from a disparity between patients’ and healthcare professionals’ perceptions of insomnia and its treatment. Additionally, the subjective experiences of patients with insomnia are often overlooked.14 Despite its relevance, there is a notable scarcity of research focusing on the KAP related to insomnia. Therefore, this study aimed to investigate the KAP related to insomnia among patients suffering from this condition.
Materials and Methods
Study Design and Participants
This cross-sectional study was conducted between May 20, 2023, and March 25, 2024, at the Neurology Outpatient Department of the Affiliated Hospital of Chengdu University of Traditional Chinese Medicine. The participants were patients presenting with insomnia. Ethical approval for this study was granted by the Ethics Committee of the Hospital of Chengdu University of Traditional Chinese Medicine, and informed consent was obtained from all participants.
Inclusion criteria: 1) Patients primarily presenting with insomnia or sleep disorders; 2) Aged 18 years or older; 3) Meeting the diagnostic criteria for sleep disorders as outlined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), published by the American Psychiatric Association in 2013; 4) Willing and able to provide informed consent. Exclusion criteria: 1) Patients unable to complete the questionnaire due to severe hearing impairments, illiteracy, or similar conditions.
Questionnaire Introduction
The questionnaire design was designed with reference to the Chinese Adult Insomnia Diagnosis and Treatment Guidelines, Expert Guidance on the Management of Pandemic Stress Insomnia, the Chinese Diagnosis and Treatment Guidelines for Insomnia Disorders, and the American Academy of Sleep Medicine,15–17 Clinical Practice Guideline on Behavioral and Psychological Treatments for Chronic Insomnia Disorder in Adults.18 Key content from these guidelines, including insomnia symptoms, risk factors, treatment approaches (both pharmacological and non-pharmacological), and self-management strategies, were extracted and adapted into questionnaire items. Technical terminology was simplified to ensure comprehensibility for patients. Prior to formal data collection, the questionnaire was pilot-tested with 40 insomnia patients to assess understandability, completion time, and identify potential ambiguities. Based on feedback from the pilot test, minor modifications were made to improve clarity and readability.
The final questionnaire was administered in Chinese and comprised four sections: basic demographic information (such as gender, age, education level, occupation type, and self-reported anxiety and depressive symptoms); a knowledge section with nine questions; an attitudes section with eight items; and a practices section, also with eight questions; an attitudes section with eight items; and a practices section, also with eight questions. In the statistical analysis, responses were scored according to the number of options per item. For the knowledge section, correct answers received 1 point, and incorrect or unclear answers received 0 points, allowing for a total score ranging from 0 to 9. The attitudes section utilized a five-point Likert scale, from very positive (5 points) to very negative (1 point), with total scores ranging from 8 to 40 points. Similarly, the practices section employed a five-point Likert scale, with total scores ranging from 8 to 40 points. The practices section mainly assessed patients’ engagement in insomnia-related self-management behaviors, including sleep hygiene habits, pre-sleep routines, and daily lifestyle practices. In this study, “proactive practice” referred to a higher level of self-reported adoption of these behaviors, which are generally recommended in clinical guidelines for insomnia management, particularly those related to sleep hygiene and behavioral interventions. Scores exceeding 70% of the maximum possible in each section were considered indicative of adequate knowledge, a positive attitude, and proactive practice.19
Construct validity of the questionnaire was examined using confirmatory factor analysis (CFA) based on the hypothesized three-factor structure (knowledge, attitude, and practice). The CFA was performed using AMOS 26.0. The model fit indices indicated an acceptable fit to the data, with a χ2/df (CMIN/DF) of 2.183, RMSEA of 0.046, IFI of 0.883, TLI of 0.850, and CFI of 0.880. Standardized factor loadings of most items were statistically significant (P < 0.05), supporting the construct validity of the questionnaire. The CFA model is presented in Supplementary Figure S1, and detailed factor loadings and model fit indices are shown in Supplementary Tables 1 and 2.
The questionnaire was distributed to participants in both online and paper formats. Older participants typically completed the paper version and were provided with assistance in reading, understanding, and completing the questionnaire (See Supplementary Questionnaire).
Statistical Analysis
Statistical analyses were conducted using SPSS 27.0 (IBM, Armonk, NY, USA) and AMOS 26.0 (IBM, Armonk, NY, USA). Continuous variables underwent a normality test, with the t-test for normally distributed data and the Wilcoxon Mann–Whitney test for non-normally distributed data when comparing two groups. For three or more groups with normally distributed continuous variables and uniform variance, ANOVA was used for comparisons, while the Kruskal–Wallis test was employed for non-normally distributed data. Univariate and multivariate logistic regression analyses were performed to explore the risk factors associated with proactive practice, with a threshold set at 70% of the maximum possible score. Path analysis was employed to explore the relationships between the KAP. A two-sided P-value of less than 0.05 was considered statistically significant.
Results
Initially, a total of 600 samples were collected for this study. The following cases were excluded: 1) 8 participants were under 18 years of age; 2) 4 participants had abnormal height values; 3) 6 participants selected both “no other underlying diseases” and other underlying diseases in the basic disease variable simultaneously; 4) 14 participants selected “unclear” for all questions in the knowledge section. In the end, 568 valid questionnaires were obtained. The mean age of the 568 insomnia patients was 40.84 ± 15.93 years. Among them, 368 (64.79%) were female, 322 (56.69%) had a BMI in the normal range, 405 (71.30%) lived in urban areas, 188 (33.10%) had a monthly per capita household income of 2000–5000 Yuan, 156 (27.46%) self-reported anxiety symptoms, and 103 (18.13%) self-reported depressive symptoms. The mean scores for knowledge, attitude, and practice were 5.50 ± 2.20, 24.53 ± 3.21, and 28.55 ± 4.28, respectively.
Analyses of demographic characteristics found significant variations in knowledge scores among patients with different residences (P < 0.001), education levels (P < 0.001), occupations (P < 0.001), monthly per capita household incomes (P = 0.003), marital statuses (P < 0.001), diabetes statuses (P < 0.001), hypertension statuses (P < 0.001), and anxiety statuses (P = 0.013). For attitude scores, differences were noted among patients with different residences (P = 0.012), anxiety statuses (P = 0.014), and depression statuses (P = 0.009). Differences in practice scores were found among patients with different genders (P = 0.008), BMIs (P = 0.002), education levels (P < 0.001), occupations (P = 0.021), marital statuses (P < 0.001), hypertension statuses (P = 0.001), and anxiety statuses (P = 0.007) (Table 1).
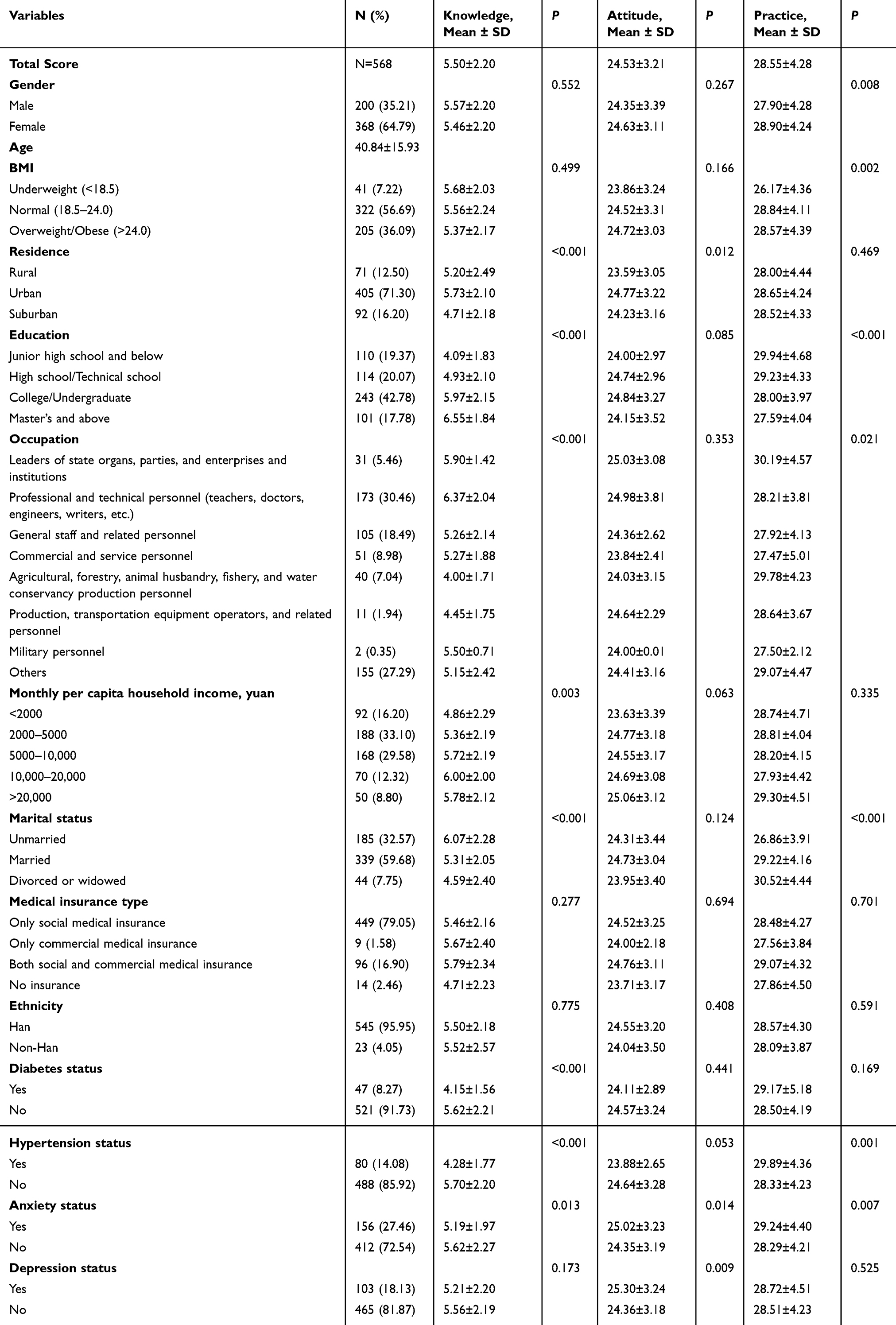 |
Table 1 Patient Baseline Characteristics and KAP Scores |
The distribution of responses in the knowledge dimension revealed that the three items with the lowest correctness rates were: “Melatonin can be used as a hypnotic agent” (K9) with 29.05%, “Chronic insomnia patients who have already received drug therapy do not need additional psychological treatment” (K7) with 38.38%, and “For patients with chronic insomnia, cognitive-behavioral therapy should be the preferred treatment in addition to establishing good sleep hygiene habits” (K6) with 47.54% (Supplementary Table 3).
In the attitude dimension, 20.6% of participants were bothered by insomnia but were not ready to take significant measures (A1), and 36.97% were fearful of insomnia, often feeling nervous near bedtime and worrying about not sleeping well (A2). Regarding factors related to insomnia, 34.86% and 36.97% of participants believed that life stress (A8.1) and psychological state (A8.2) were very highly correlated with insomnia, respectively (Supplementary Table 4).
When it comes to related practices, 24.82% reported that they often engaging in mentally stimulating activities or watching stimulating books, magazines, or TV programs within 1 hour before bedtime. (P2), 17.43% occasionally keep a regular schedule (P3), and 44.01% never drink warm milk before bedtime (P6) (Supplementary Table 5).
Multivariate logistic regression showed that knowledge score (OR = 0.898, 95% CI: [0.819–0.985], P = 0.022), attitude score (OR = 1.114, 95% CI: [1.050–1.182], P < 0.001), age (OR = 1.035, 95% CI: [1.015–1.056], P < 0.001) were independently associated with proactive practice (Table 2).
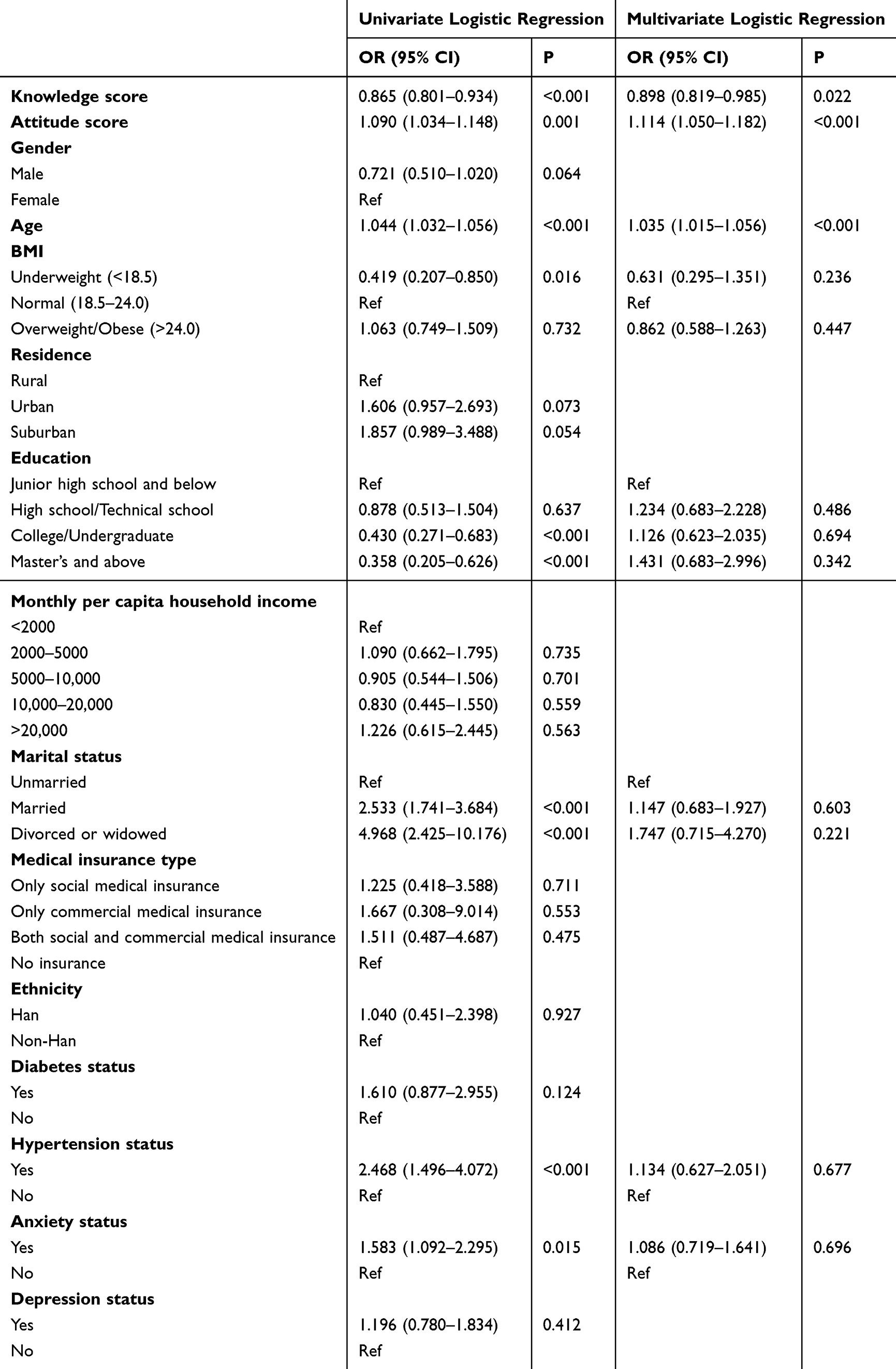 |
Table 2 Factors Influencing Proactive Practice |
The results of pathway analysis showed that knowledge was significantly associated with attitude (β = 0.240, P = 0.010) and practice (β = −0.128, P = 0.013), and attitude was significantly associated with practice (β = 0.179, P = 0.010). In addition, an indirect association was observed between knowledge and practice through attitude (β = 0.043, P = 0.010) (Table 3). The overall model demonstrated an acceptable fit to the data, with χ2/df (CMIN/DF) = 2.183, RMSEA = 0.046, IFI = 0.883, TLI = 0.850, and CFI = 0.880, indicating adequate goodness-of-fit of the pathway model.
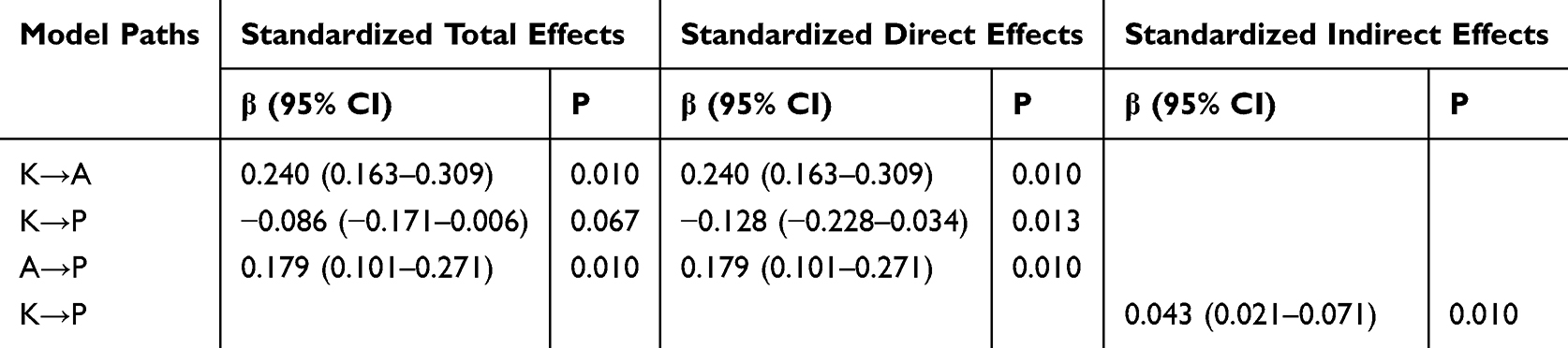 |
Table 3 Results of Pathway Analysis |
Discussion
The study revealed that patients generally possess inadequate knowledge and hold negative attitudes towards insomnia, yet they tend to engage in proactive practices. Here, proactive practices mainly referred to patients’ self-reported engagement in behaviors commonly emphasized in evidence-based insomnia management, such as maintaining sleep hygiene and adopting behavioral strategies. Clinical interventions in similar clinical settings should prioritize enhancing patient education to improve knowledge about insomnia, as better understanding is positively associated with attitudes and practices. Tailoring educational programs to address specific misconceptions and foster positive attitudes may help enhance the effectiveness of patient self-management strategies for insomnia.
This study highlights several important findings regarding the knowledge, attitudes, and practices of insomnia patients. Notably, significant differences in KAP scores were observed across various demographic and socio-economic variables. For instance, educational level significantly influenced knowledge scores, with higher education correlating with better knowledge about insomnia. This trend is consistent with literature indicating that higher education levels can enhance health literacy, thereby improving both understanding and attitudes towards health issues.20,21 Furthermore, marital status significantly influenced practice scores, with married individuals demonstrating more proactive practices, potentially due to increased social support, which has been shown to enhance engagement in health-promoting behaviors.22,23
Interestingly, while gender did not significantly affect knowledge or attitude scores, practice scores differed significantly between males and females, with females showing more proactive practices. This could be attributed to gender differences in health consciousness, as women experience higher rates of insomnia compared to men.6 Moreover, the multivariate logistic regression supports these findings, indicating an association between gender and practice scores, reinforcing the need for targeted interventions that consider gender-specific preferences and challenges in insomnia management.
The relationship between KAP was further elucidated through multivariate logistic regression and SEM, revealing that higher knowledge scores were associated with more positive attitudes and better practices. This association suggests that interventions aimed at improving knowledge may be associated with enhanced practical engagement through improved attitudes, as indicated by pathway analysis results showing both direct and indirect associations between knowledge and practice through attitude.24,25 These findings highlight the potential importance of comprehensive educational strategies in insomnia management.
The survey results on knowledge about insomnia reveal mixed levels of understanding among patients. A significant number of patients are aware of the basic symptoms and classification of insomnia, but there are gaps, particularly regarding the progression of short-term to chronic insomnia and the use of melatonin as a hypnotic agent. Notably, less than half correctly identified cognitive-behavioral therapy as a preferred treatment for chronic insomnia. To address these gaps, targeted educational programs could be developed, focusing on the importance and effectiveness of cognitive-behavioral therapy as a front-line treatment option. Moreover, incorporating detailed sessions on the safe use of melatonin and transitioning from short-term to chronic insomnia into routine patient education could help improve understanding significantly.26,27
Attitudes toward insomnia management present a complex picture. While a majority recognize the seriousness of insomnia and trust their doctors, there is a notable reluctance to engage with certain treatments, particularly concerning the use of sleeping pills and traditional Chinese medicine. This reluctance is often based on fears of side effects or doubts about effectiveness, aligning with findings from other contexts where patients expressed similar concerns.28,29 To improve attitudes, it would be beneficial to enhance doctor-patient communication, allowing for more personalized discussions that address specific fears and misconceptions. Additionally, creating patient-centered informational campaigns that clearly outline the benefits and risks of various treatment options, including empirical evidence of their safety and efficacy, could help mitigate these concerns.30,31
Practices regarding the management of insomnia show that while some good habits are well-adopted, such as maintaining a comfortable and quiet sleep environment, other beneficial practices are less frequently observed. Given that this study was conducted in a hospital of traditional Chinese medicine, the findings also have implications for culturally relevant educational and behavioral interventions. Practical education programs could integrate sleep hygiene guidance with traditional Chinese medicine–based approaches commonly accepted by patients, such as lifestyle regulation, emotional management, and non-pharmacological therapies. For example, structured sleep hygiene programs, combined with education on appropriate use of traditional Chinese medicine modalities, may help patients better understand insomnia management and encourage more consistent engagement in healthy sleep-related behaviors. Such culturally adapted interventions may be particularly suitable for clinical settings similar to ours. Particularly, the low frequency of engagement in pre-sleep rituals such as drinking warm milk or soaking feet in hot water suggests a lack of routine in bedtime practices, which is crucial for managing insomnia effectively. To encourage better practices, it might be useful to introduce structured behavioral therapy programs that include sleep hygiene training and establish regular follow-ups to reinforce these practices. Educational materials that provide practical tips on establishing a bedtime routine could also be distributed during clinic visits. Programs that offer demonstrations on relaxation techniques, such as guided imagery or progressive muscle relaxation, could further support individuals in adopting more effective sleep practices.32–34
This study has several limitations that should be considered when interpreting the results. First, the cross-sectional design restricts our ability to establish causal relationships between knowledge, attitudes, and practices regarding insomnia. Second, the sample was drawn exclusively from patients attending a single center in Chengdu, which may limit the generalizability of the findings to other regions and broader populations. Finally, the reliance on self-reported data could introduce response bias, potentially affecting the accuracy of the reported attitudes and practices. Anxiety and depressive symptoms were not assessed using validated instruments.
Conclusion
In conclusion, in this single-center sample, patients demonstrated inadequate knowledge, negative attitudes, and proactive practices towards insomnia. These findings underscore the need for targeted educational interventions in similar clinical populations aimed at improving knowledge about insomnia. Enhancing patient understanding of insomnia may be associated with more positive attitudes and proactive self-management practices.
Data Sharing Statement
All data generated or analyzed during this study are included in this article and supplementary information files.
Ethics Approval and Informed Consent
This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. This study was approved by the Ethic Committee of the Hospital of Chengdu University of Traditional Chinese Medicine (2023KL-031), and all participants provided written informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
“Xinglin Scholars” Discipline Talent Scientific Research Promotion Plan Fund of Chengdu University of TCM (MPRC2021042). The Natural Science Foundation of Sichuan Province (Nos.2024NSFSC1824). Sichuan Provincial Administration of Traditional Chinese Medicine (2023MS132). Chengdu Municipal Health and Family Planning Commission (2023431). Joint Innovation Fund of Health Commission of Chengdu and Chengdu University of Traditional Chinese Medicine” (WXLH202403223 and WXLH202403044).
Disclosure
The authors declare that they have no competing interests.
References
1. Asarnow LD, Mirchandaney R. Sleep and mood disorders among youth. Child Adolesc Psychiatr Clin N Am. 2021;30(1):251–10. doi:10.1016/j.chc.2020.09.003
2. Buysse DJ. Insomnia. JAMA. 2013;309(7):706–716. doi:10.1001/jama.2013.193
3. Bianchi MT. Chronic insomnia. Semin Neurol. 2017;37(4):433–438. doi:10.1055/s-0037-1605344
4. Cao XL, Wang SB, Zhong BL, et al. The prevalence of insomnia in the general population in China: a meta-analysis. PLoS One. 2017;12(2):e0170772. doi:10.1371/journal.pone.0170772
5. Brewster GS, Riegel B, Gehrman PR. Insomnia in the older adult. Sleep Med Clin. 2018;13(1):13–19. doi:10.1016/j.jsmc.2017.09.002
6. Mong JA, Cusmano DM. Sex differences in sleep: impact of biological sex and sex steroids. Philos Trans R Soc Lond B Biol Sci. 2016;371(1688):20150110. doi:10.1098/rstb.2015.0110
7. Cox RC, Olatunji BO. A systematic review of sleep disturbance in anxiety and related disorders. J Anxiety Disord. 2016;37:104–129. doi:10.1016/j.janxdis.2015.12.001
8. Barry V, Stout ME, Lynch ME, et al. The effect of psychological distress on health outcomes: a systematic review and meta-analysis of prospective studies. J Health Psychol. 2020;25(2):227–239. doi:10.1177/1359105319842931
9. Kobayashi Y, Kondo N. Organizational justice, psychological distress, and stress-related behaviors by occupational class in female Japanese employees. PLoS One. 2019;14(4):e0214393. doi:10.1371/journal.pone.0214393
10. Qaseem A, Kansagara D, Forciea MA, Cooke M, Denberg TD. Management of chronic insomnia disorder in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2016;165(2):125–133. doi:10.7326/m15-2175
11. Rosenberg R, Citrome L, Drake CL. Advances in the treatment of chronic insomnia: a narrative review of new nonpharmacologic and pharmacologic therapies. Neuropsychiatr Dis Treat. 2021;17:2549–2566. doi:10.2147/ndt.S297504
12. Shi X, Shi Y, Wang J, Wang H, Li Y. Knowledge, attitude, and practice toward sleep disorders and sleep hygiene among perimenopausal women. Sci Rep. 2024;14(1):11663. doi:10.1038/s41598-024-62502-4
13. Wang J, Chen L, Yu M, He J. Impact of knowledge, attitude, and practice (KAP)-based rehabilitation education on the KAP of patients with intervertebral disc herniation. Ann Palliat Med. 2020;9(2):388–393. doi:10.21037/apm.2020.03.01
14. Araújo T, Jarrin DC, Leanza Y, Vallières A, Morin CM. Qualitative studies of insomnia: current state of knowledge in the field. Sleep Med Rev. 2017;31:58–69. doi:10.1016/j.smrv.2016.01.003
15. Sleep Disorders Group NB, Chinese Medical Association. Diagnosis and treatment guidelines for insomnia in Chinese adults. Chin J Neurol. 2012;45(7):7.
16. Medicine. PMBotCSoTC. Expert guidance on the management of epidemic stress insomnia. Chin J Clin Phys. 2022;10:50.
17. Gu P, He JC, Liu YJ, et al. Chinese guidelines for the diagnosis and treatment of insomnia disorders [C]. Beijing Sleep Disease Diagnosis and Standardized Treatment Summit Forum; 2024.
18. Edinger JD, Arnedt JT, Bertisch SM, et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2021;17(2):255–262. doi:10.5664/jcsm.8986
19. Lee F, Suryohusodo AA. Knowledge, attitude, and practice assessment toward COVID-19 among communities in East Nusa Tenggara, Indonesia: a cross-sectional study. Front Public Health. 2022;10:957630. doi:10.3389/fpubh.2022.957630
20. Negesa LB, Magarey J, Rasmussen P, Hendriks JML. Patients’ knowledge on cardiovascular risk factors and associated lifestyle behaviour in Ethiopia in 2018: a cross-sectional study. PLoS One. 2020;15(6):e0234198. doi:10.1371/journal.pone.0234198
21. O’Rourke T, Dale R, Humer E, Probst T, Plener P, Pieh C. Health behaviors in austrian apprentices and school students during the COVID-19 pandemic. Int J Environ Res Public Health. 2022;19(3). doi:10.3390/ijerph19031049
22. Antabe R, Kansanga M, Sano Y, Kyeremeh E, Galaa Y. Utilization of breast cancer screening in Kenya: what are the determinants? BMC Health Serv Res. 2020;20(1):228. doi:10.1186/s12913-020-5073-2
23. McNaughton SA, Pendergast FJ, Worsley A, Leech RM. Eating occasion situational factors and sugar-sweetened beverage consumption in young adults. Int J Behav Nutr Phys Act. 2020;17(1):71. doi:10.1186/s12966-020-00975-y
24. Liang X, Fu Y, Cao WT, et al. Gut microbiome, cognitive function and brain structure: a multi-omics integration analysis. Transl Neurodegen. 2022;11(1):49. doi:10.1186/s40035-022-00323-z
25. Kustiningsih H, Sudarnika E, Basri C, Sudarwanto M. Dairy farmers’ knowledge, attitudes, and practices regarding the brucellosis surveillance and control program in Bogor, Indonesia. Vet World. 2023;16(1):126–133. doi:10.14202/vetworld.2023.126-133
26. Brownlow JA, Miller KE, Gehrman PR. Insomnia and cognitive performance. Sleep Med Clin. 2020;15(1):71–76. doi:10.1016/j.jsmc.2019.10.002
27. Riemann D, Espie CA, Altena E, et al. The European insomnia guideline: an update on the diagnosis and treatment of insomnia 2023. J Sleep Res. 2023;32(6):e14035. doi:10.1111/jsr.14035
28. Lee M, Miao E, Rapkin B, Halmos B, Shankar V, Goel S. Prevalence and assessment of factors associated with COVID-19 vaccine hesitancy in an ethnic minority oncology patient population. Vaccines. 2022;10(10). doi:10.3390/vaccines10101711
29. Pawlicka MA, Filip A. Can genistein be a potential agent against skin side effects associated with the treatment of breast cancer? Postepy Dermatol Alergol. 2022;39(1):7–12. doi:10.5114/ada.2022.113800
30. Azzez SS, Abdulah DM, Piro RS, Miho Alhakem SS. Sleep severity and fatigue manifestations in relation to the doctor-patient relationship. Sleep Med. 2019;58:13–17. doi:10.1016/j.sleep.2019.02.015
31. Klingman KJ, Williams NJ, Perlis ML, Grandner MA. Doctor-patient sleep discussions for US adults: results from the SHADES study. Sleep Health. 2019;5(6):658–665. doi:10.1016/j.sleh.2019.07.004
32. Chung KF, Lee CT, Yeung WF, Chan MS, Chung EW, Lin WL. Sleep hygiene education as a treatment of insomnia: a systematic review and meta-analysis. Fam Pract. 2018;35(4):365–375. doi:10.1093/fampra/cmx122
33. Espie CA, Emsley R, Kyle SD, et al. Effect of digital cognitive behavioral therapy for insomnia on health, psychological well-being, and sleep-related quality of life: a randomized clinical trial. JAMA Psychiatry. 2019;76(1):21–30. doi:10.1001/jamapsychiatry.2018.2745
34. Kalmbach DA, Cheng P, Arnedt JT, et al. Treating insomnia improves depression, maladaptive thinking, and hyperarousal in postmenopausal women: comparing cognitive-behavioral therapy for insomnia (CBTI), sleep restriction therapy, and sleep hygiene education. Sleep Med. 2019;55:124–134. doi:10.1016/j.sleep.2018.11.019
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.