Back to Journals » Breast Cancer: Targets and Therapy » Volume 9
Knowledge, attitudes and behaviors of primary health care nurses and midwives in breast cancer early diagnosis applications
Received 30 October 2016
Accepted for publication 20 January 2017
Published 13 March 2017 Volume 2017:9 Pages 163—169
DOI https://doi.org/10.2147/BCTT.S126124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pranela Rameshwar
Aliye Bulut,1 Aziz Bulut2
1Department of Nursing, Higher School of Health, Bingol University, 2Department of General Surgery, Bingol State Hospital, Bingol, Turkey
Purpose: The purpose of this research was to analyze the knowledge, attitudes and behaviors of the nurses and midwives about the early diagnosis of breast cancer.
Materials and methods: This cross-sectional study was carried out at 9 family medical centers (FMCs) and 1 community health center (CHC) in Bingol; the population of this research consisted of 25 midwives and 38 nurses. The protocol for this study was approved by the regional ethics committee of Bingol University. The study was performed in accordance with the principles of the Declaration of Helsinki. The purpose of this study was explained to the nurses and midwives who participated, and their written and verbal permission was obtained; great care was taken to ensure that they understood participation was voluntary. A questionnaire of 41 questions was used for the data collection.
Results: When the age distribution of nurses and midwives was examined, it was found that 96.8% of them were aged ≤39 years. A total of 92.0% of midwives and 84.2% of nurses practiced breast self-examination (BSE). A total of 56% of the married women practiced family planning, and the most frequent method was using contraceptive pills. A total of 88.9% of the women had never had hormonal treatment for any reason. The BSE knowledge level of 65% of the women, who performed clinical breast examination, was complete. Among the women who had full knowledge of BSE, 38.5% of them performed examination once every 6 months, 23.0% of them once a year and 38.5% of them once every 3 years.
Conclusion: This research showed that the deficiencies for nurses and midwives regarding the early diagnosis methods of breast cancer have been identified, and supporting these deficiencies with training is recommended.
Keywords: nurses, midwives, primary health care, breast self-examination
Introduction
Cancer is an increasing major health problem worldwide, including in Turkey. Cancer is a significant public health issue due to its frequency and high lethality.1
According to studies conducted, one-tenth of women are at risk of contracting breast cancer throughout their lifetime, and one-third of them are at risk of death due to breast cancer. Similar to many cancer types, more than one factor plays a role in the etiology of breast cancer.2–4 These factors can be personal or environmental, such as familial predisposition, hormonal changes, age and fertility characteristics. However, the fact that 20% of breast cancer patients have these risk factors and a significant proportion of these factors are impossible to keep under control increases the importance of early diagnosis in cancer protection.3,4
As it is not possible to provide primary protection in breast cancer, early diagnosis, which is the secondary protection, is essential. Due to being easily treatable and recoverable, early diagnosis and treatment of breast cancer, is effective in extending the length of life and reducing mortality.5 According to literature, 90% of breast cancer is detectable by the individuals themselves, aiding in the important early diagnosis. The methods used for early diagnosis of breast cancer are breast self-examination (BSE), physical examination carried out by the doctor and mammography. BSE is a practice that is simple and inexpensive, does not require an invasive procedure, does not have any risk and does not necessitate any kind of tools. In this regard, women should know the importance of early diagnosis and should be informed in this direction.6,7
Since diagnosing breast cancer at the early stage increases the survival rate and there is a high chance of treatment, this situation prioritizes the roles of midwives and nurses above other health care workers. Midwives and nurses, who have more contact with patients and healthy individuals, can explain the importance of breast cancer, it’s symptoms and screening methods to women by having adequate knowledge and skills about early diagnosis and treatment of cancer, and using effective communication techniques. In addition, they can motivate them by encouraging BSE, clinical breast examinations (BEs) and mammography. As women, midwives and nurses themselves should regularly perform BSEs in the correct method and have clinical BEs and regular mammograms, they can turn these controls into a routine behavior. This is required as the nurses and the midwives primarily can relate to other women with whom they are responsible to serve, and they should have a wide knowledge of the risks, symptoms and findings of breast cancer.8,9
Breast, colon and cervical cancers are included in the screening program of the Turkish Ministry of Health to assist in the prevention and early diagnosis of these diseases, and nurses and midwives undertake the most important role in these screenings. It is important for the nurses and the midwives, who are responsible of the public’s health, to care about their own health and to have their screening tests with appropriate regularity. Awareness of all health care personnel should be raised regarding protecting their own health. In order to reach this goal, the importance of protecting their own health should be emphasized to the health care professionals both before and after their graduation. In addition to this, special permissions given to the nurses and midwives by their administrators for their screenings might be encouraging.
There are a significant number of duties to be executed by nurses and midwives regarding breast cancer. Therefore, it was aimed to select midwives and nurses serving in the primary health care services as the target population of the study to determine their levels of knowledge and to increase their levels of knowledge as a priority if needed. The purpose of this research was to analyze the knowledge, attitudes and behaviors of the nurses and midwives about the early diagnosis of breast cancer.
Materials and methods
This cross-sectional study was carried out at 9 family medical centers (FMCs) and 1 community health center (CHC) in Bingol; the population of this research consisted of 25 midwives and 38 nurses (the response rate 100%). The protocol for the study was approved by the regional ethics committee of Bingol University. The study was performed in accordance with the principles of Declaration of Helsinki. All participants gave written and verbal permission to participate in this study. A questionnaire of 41 questions was used for the data collection. The questions in the survey form consisted of sociodemographic characteristics of the nurses and midwives (age, occupation, education level, marital status, total years of work, number of children, number of pregnancies, utilization of family planning), situation of having breast cancer risk factors (age of the beginning of the first menstrual cycle, status of the continuation of menstrual cycle, status of breastfeeding the children, age of the first pregnancy, the method used for family planning, status of receiving hormonal therapy, breast diseases carried, having a history of breast cancer in the family, status of having invasive procedures such as biopsy and biopsies resulting in atypical hyperplasia), information questions related to BSE, behavioral questions related to BSE, knowledge questions about clinical BE, behavioral questions related to clinical BE and behavioral questions related to mammography. The dependent variables of the study were age, marital status, education level, occupation, working time, age of the starting of the first menstrual cycle, continuation status of menstrual cycle, status of breastfeeding the children, age of the first pregnancy, the utilized method for family planning and the length of use, status of receiving hormonal therapy, breast diseases carried, having a family history of breast cancer, status of having invasive procedures such as biopsy and biopsies resulting in atypical hyperplasia. The data were analyzed using the statistical software package SPSS 17.0. Averages were given with standard deviation, and p<0.05 was identified as the level of significance. In the statistical evaluation of the data, Fisher’s chi-square test was used; however, the p-value could not be calculated because the groups were not equally distributed. The data were presented as descriptive statistics (number and percentage).
Results
In this study, questions were directed regarding the breast cancer risk factors and early diagnosis techniques of nurses and midwives working in primary health care institutions; the distribution of the sociodemographic characteristics of the nurses and midwives according to the status of their implementing BSE is presented in Table 1. In this regard, the rate of implementing BSE was 87.3%. When the age distribution of nurses and midwives was examined, it was found that 96.8% (n=61) of them were aged ≤39 years, and 92.0% of midwives and 84.2% of nurses practiced BSE. When the education levels of the nurses and midwives who participated in the study were analyzed, 91.7% of high school graduates, 87.9% of graduates of an associate degree, and all the bachelor’s degree graduates practiced BSE. All the women who participated in the study were in their premenopausal period, 61.9% of them had children and 47.6% of them had been working between 5 and 10 years. A total of 56% of the married women practiced family planning, and the most frequent method was using contraceptive pills. A total of 88.9% of the women had never had hormonal treatment for any reason.
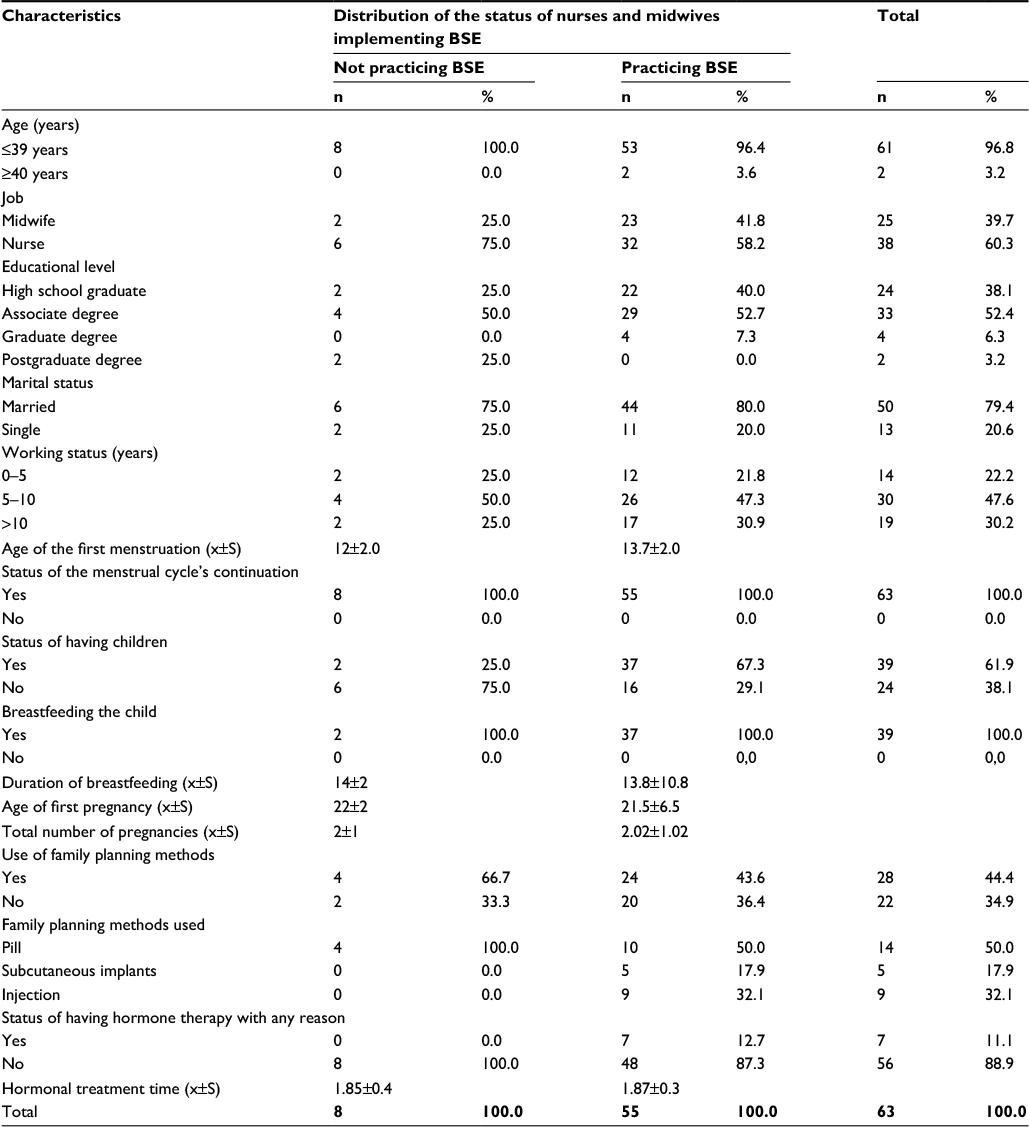 | Table 1 Distribution of the nurses and midwives regarding their sociodemographic characteristics Note: As the groups are not equally distributed, the value of chi-square has not been calculated. Abbreviations: BSE, breast self-examination; m, mean; S, standard deviation. |
The distribution of the nurses and midwives regarding their knowledge levels on BSE is presented in Table 2. According to this, 30.2% of midwives and nurses had full knowledge, 42.9% had missing knowledge, and the remainder of them did not know BSE at all. According to the education levels, 62.5% of high school graduates did not know BSE and 57.6% of associate degree graduates and all the bachelor’s degree graduates had missing knowledge. A total of 53.3% of the women who had 0–5 years of working time had missing knowledge. Of the 73.6% women who participated in the study and who had over 10 years of work experience; 36.8% of these women had full knowledge of BSE implementations, while 36.8% of these women had missing knowledge.
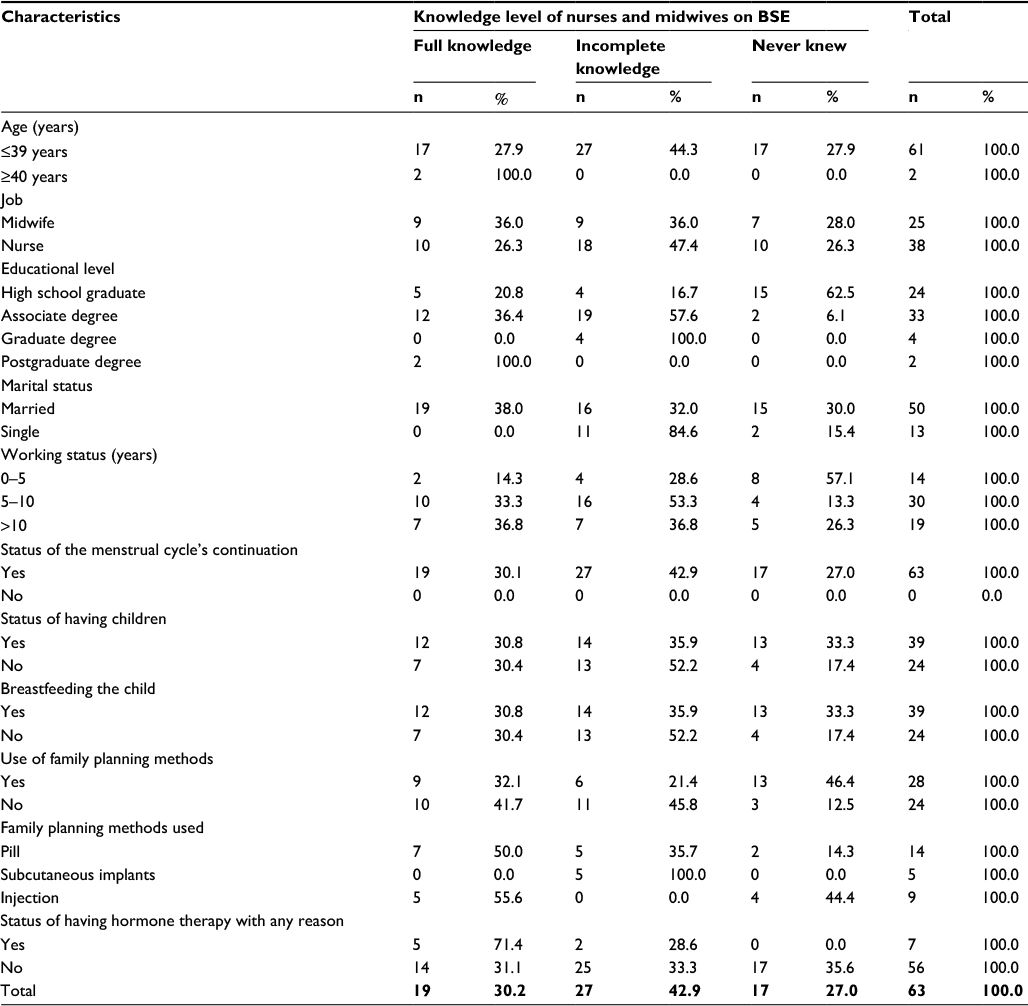 | Table 2 Distribution of characteristics regarding the knowledge level of nurses and midwives about BSE Note: As the groups are not equally distributed, the value of chi-square has not been calculated. Abbreviation: BSE, breast self-examination. |
The distribution of midwives and nurses regarding the behavior of the nurses on clinical BE is presented in Table 3. The BSE knowledge level of 65% of the women who performed clinical BE was complete. Among the women who had full knowledge of BSE, 38.5% of them performed examination once every 6 months, 23.0% of them once a year and 38.5% of them once every 3 years. A total of 77% of the women, who fully knew the subject, stated the reason for clinical BE as early diagnosis. A total of 55.6% of them, who had experienced breast diseases in the past, had full knowledge on BSE.
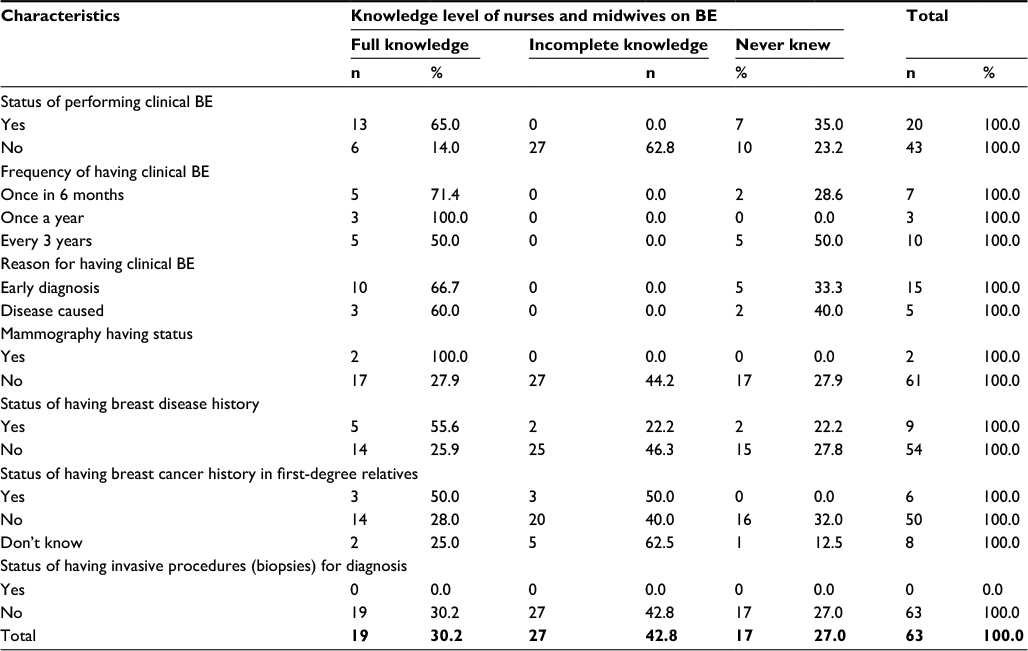 | Table 3 Behaviors of the nurses and midwives, associated with clinical BE Note: As the groups are not equally distributed, the values of chi-square and p have not been calculated. Abbreviation: BE, breast examination. |
Discussion
The most reliable way to reduce mortality of breast cancer is early diagnosis and treatment. The primary methods that are recommended for early diagnosis in breast cancer are BSE, clinical BE and mammography. With these methods, it is aimed to detect if there are any abnormalities of the breast.10 BSE, mammography and clinical BE are recommended to raise awareness for breast cancer. BSE is a simple method that is cost-effective, easy to apply, creates awareness about breast cancer and raises self-care responsibility. A total of 39.0% of participants stated that they practiced BSE regularly. In studies performed in Turkey, it was seen that the rate of practicing BSE for women varied between 32.0% and 84.1%.11,12
BSE is a simple, inexpensive, non-invasive, safe and practicable-at-home technique.13 The rate of the participants of the current study practicing BSE was 87.3%. In the study of Aydın and Işıklı,8 it was stated that 96.3% of the nurses and midwives working at preventive medicine services have been implementing the BSE; however, the rate of the women who carry out BSE regularly is 28.6%. In the study of Canbulat9 carried out in 2006, it was stated that 22.9% of midwives and 15.8% of nurses, working in the hospitals and health centers in Erzurum, have been practicing BSE regularly.
Regarding the education levels, 62.5% of high school graduates had never known the subject and 57.6% of associate degree and all bachelor’s degree graduates had incomplete information. A total of 57.1% of the women working for 0–5 years had never known the subject, 53.3% of women with 5–10 years of work experience had incomplete information and 73.7% of the women who had been working over 10 years fully knew or had missing information. In the study of Karahan et al,14 a statistically significant difference had been found between the education levels of the nurses and knowledge levels for BSE; and it was identified that 90.9% of bachelor’s degree graduates, 78.3% of medical vocational high school graduates and 79.7% of associates degree graduates have the knowledge of BSE. In the study that Orhan carried out on the general population, a statistical significance between education level and BSE knowledge level had been determined. While, 13.5% of primary school graduate women had knowledge about BSE, this rate raised up to 22.5% for the women graduated from secondary school or higher.15 When considering that the sample population consisted of health care workers, whose professional trainings included breast cancer prevention information and early diagnosis methods, and with the Ministry of Health who have been organizing in-service trainings for the health care workers periodically; it is remarkable that the rate of implementing regular (monthly) BSE for the research group was significantly low (39.0%).
Of the nurses and midwives, who implement clinical BE, 30.2% have full knowledge, 42.9% have incomplete information, and the remaining have no information about the subject. In the study of Karahan et al,14 it was stated that 93.0% of the women who implement BSE know the appropriate technique and 64.1% of them practice it even though they do not know the technique.14 In the study carried out by Çadır et al,16 the difference between the BSE implementation and average knowledge points was found to be significant, and it was expressed that 45.1% of the women practice BSE and the women who apply it have the highest average knowledge point of 19.58±7.41. The findings of these studies and the findings in our study resemble each other in terms of the higher knowledge on the technique of the BSE by the implementers among the participants.
One of the important methods for the early diagnosis of breast cancer is clinical BE. Clinical BE is a method that should be performed by the doctor once every 3 years before the age of 40 and once a year after the age of 40.1 A total of 38.5% of the nurses and the midwives who had full knowledge carried out BE once every 6 months, 23.0% of them once a year and 38.5% of them once every 3 years. In a study on determining the statuses of the knowledge and implementations of women health professionals who work at a government hospital in Turkey, for the early diagnosis methods of breast cancer, it was determined that only 2.6% of the participants had clinical BE once a year and 1.3% of them had regular mammography once a year.17 In another study that was performed outside Turkey, it was observed that 28.9% of the nurses had clinical BEs.18 Assuming that nurses and midwives should know as health professionals that a pathological situation in the breast is a factor that increases the risk of breast cancer, it is thought-provoking that nearly half of them still do not know, or have incomplete information, on the appropriate implementation of BSE, even though they have had a diagnosis of a breast disease. These findings reflect that the responsibility levels for not even the health professionals are at the desired level regarding their own health.
Conclusion and recommendations
This research showed that deficiencies for nurses and midwives regarding the early diagnosis methods of breast cancer have been identified, and supporting these deficiencies with training is recommended. In-service training for primary care health institutions should be systemized and functionalized, and this training should be provided by individuals who are experts in their subjects. Additionally, by measuring the knowledge, attitudes and behaviors at the beginning and the end of each training, the effectiveness of the training should be evaluated.
Acknowledgments
Aziz Bulut is the second author and husband of Aliye Bulut. Aziz Bulut is a general surgery specialist, the authors have also collaborated on other studies.
Disclosure
The authors report no conflicts of interest in this work.
References
Turkish Association for Cancer Research and Control. Cancer Statistics in Turkey and in the World. Available from: http://www.turkcancer.org.php. Accessed January 8, 2016. | ||
Sadler RG, Ko CM, Cohn AJ, White M, Weldon R, Wu P. Breast cancer knowledge, attitudes, and screening behaviors among African American women: the Black cosmetologists promoting health program. BMC Public Health. 2007;7:57. | ||
Fındık YÜ, Turan N. Identification of the behaviors of the women regarding the early diagnosis of breast cancer. Nursing Forum Magazine; November-December 2004:54. | ||
Gençtürk N. The risk factors in breast cancer. Nursing Forum Magazine; July-August, May-June 2006:106–112. | ||
Koç Z, Sağlam Z. Determining the knowledge and the implementations of the women regarding breast cancer, preventive measures, and breast self-examination, and the effectiveness of education. Vol. 5. Breast Health Magazine; 2009:25–33. Publication No. 1. | ||
Dolgun E, Solak Kabataş M, Ertem G. Analyzing the effectiveness of the planned trainings provided about the Breast Self-Examination for the women at and over the age of 20. Vol. 5. Breast Health Magazine; 2009. Publication No. 3. | ||
Gölbaşı Z, Çetin R, Kalkan S, Durmuş T. The Knowledge and Behaviors of the Girls Who Are University Students Regarding the Breast Cancer and Breast Self-Examination. Vol. 6. Breast Health Magazine; 2010. Publication No.2. | ||
Aydın I, Işıklı Z. The breast self-examination beliefs of nurses and midwives who work in preventive health care services. In: 3rd National Nursery Student Congress Statement Booklet. Edirne: University Publications; 2004:32. | ||
Canbulat N. Master’s Thesis for the Analysis of the Health Professionals’ Beliefs on Health Regarding Breast Cancer, Breast Self-Examination and Mammography. Erzurum: Atatürk University; 2006. | ||
Jemal A, Siegel R, Ward E, Murray T, Thun M. Cancer statistics. Cancer J Clin. 2007;57:43–66. | ||
Karayurt Ö, Coşkun A, Cerit K. The Beliefs and Application Status of the Nurses on the Breast Cancer and Breast Self-Examination. Vol. 4. Breast Health Magazine; 2008:15–20. | ||
Özaydın AN, Güllüoğlu BM, Ünalan PC, et al. The Knowledge Levels, Knowledge Sources of Breast Cancer and Implementations About Breast Health of the Women Residing in Bahçeşehir. Vol. 5. Breast Health Magazine; 2009:214–224. | ||
Çetintaş SK. In: Kayıhan E, Çetintaş SK, editors. Self-Examination and Physical Examination at Breast Cancers. Bursa: Nobel Medicine Publications; 2005:163–168. | ||
Karahan A, Topuzoğlu A, Harmancı H. The factors that affect the behaviors of the nurses regarding the breast self-examination and having mammography. In: 8th National Public Health Congress Booklet. Diyarbakır; 2002:666. | ||
Orhan S. Master’s Thesis of the Views and Behaviors of the Grown up Women Regarding Breast Cancer in the Region of the Selected Municipal Healthcare Center in Kayseri Province. Kayseri: Erciyes University; 2002. | ||
Çadır G, Eksen M, Bütüner E, et al. Determining the Knowledge and Implementation Status of the Women, Residing in the Regions of Central Muğla, Bayır, Yerkesik and Yeşilyurt Healthcare Centers, Regarding the Subjects of Breast Cancer and Breast Self-Examination. International Human Sciences Magazine; 2004:1–16.ISSN:1303-5134. | ||
Gençtürk N. The knowledge and implementation statuses of the health professionals of breast cancer early diagnosis methods. J Breast Health. 2013;9(1):5–9. | ||
Odusanya OO, Tayo OO. Breast cancer knowledge, attitudes and practice among nurses in Lagos, Nigeria. Acta Oncol. 2001;40(7):844–848. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.