Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Knowledge, Attitude and Practice Regarding Ramadan Fasting and Related Determinants in Patients with Type 2 Diabetes at a Saudi Diabetes Clinic
Authors Alsunni AA ![]() , Albaker WI, Almansour AH
, Albaker WI, Almansour AH ![]() , Alenazi AS
, Alenazi AS ![]() , Alaftan MS
, Alaftan MS ![]() , Badar A
, Badar A ![]()
Received 8 December 2019
Accepted for publication 9 January 2020
Published 21 January 2020 Volume 2020:13 Pages 151—159
DOI https://doi.org/10.2147/DMSO.S241496
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Ahmed Abdulrahman Alsunni, 1 Waleed Ibrahim Albaker, 2 Abdulelah Hassan Almansour, 3 Abdulaziz Saud Alenazi, 4 Mohammed S Alaftan, 5 Ahmed Badar 1
1Department of Physiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia; 2Department of Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia; 3Department of Family & Community Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia; 4Department of Otorhinolaryngology-Head and Neck Surgery, King Fahad Hospital of the University, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia; 5Department of Radiology, King Fahad Hospital of the University, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia
Correspondence: Ahmed Abdulrahman Alsunni
Department of Physiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia
Email [email protected]
Objective: This study was carried out in type 2 diabetes mellitus (T2DM) patients to assess their knowledge, attitude and practice about fasting during Ramadan and to identify the sociodemographic determinants of the knowledge, attitude and practice.
Methods: A total of 107 T2DM patients were interviewed at a diabetes clinic in the Eastern Saudi Arabia. A questionnaire containing knowledge, attitude and practice questions about fasting during Ramadan was used to collect data. Data about age, gender, city of residence, nationality, level of education, and history of diabetes in family were also collected. Descriptive and inferential statistics were carried out using IBM-SPSS Version 21.
Results: The mean total score for knowledge, attitude and practice was 16.5 ± 3.72 (out of 27). The individual scores for knowledge, attitude and practice were: 9.67± 2.53 (out of 16), 4.10± 1.28 (out of 6), and 2.77± 1.08 (out of 5), respectively. Gender (OR: 4.08, 95% CI: 1.05,15.79 and p< 0.041), education (OR: 0.068, 95% CI: 0.008,0.594, p< 0.015) and family history (OR: 5.086, 95% CI: 1.095, 23.630 p< 0.038) were identified as independent determinants of the total score.
Conclusion: Gender, Family history of diabetes and Education are determinants of knowledge, attitude and practice regarding fasting during Ramadan in the T2DM patients. A significant knowledge practice gap exists that necessitates further strengthening of the Pre-Ramadan education program for T2DM patients.
Keywords: type 2 diabetes mellitus, fasting, ramadan, knowledge, attitude, practice
Introduction
Type 2 diabetes mellitus (T2DM) is one of the most common non-communicable disease in the world and its prevalence is continuously increasing among developing countries.1 In the last decade, there has been an extraordinary increase in the prevalence of T2DM, mostly among young people related to obesity, unhealthy dietary habits and a sedentary life style.2 In Saudi Arabia, the prevalence of diabetes soared from 4.3% in 1986 to 25.4% in 2014.3 This made Saudi Arabia a country with the third largest prevalence of diabetes in the world.4
Ramadan occurs during the ninth month of the Islamic calendar. All adult Muslim men and women must fast from pre-dawn to dusk except those who are either sick or travelers, who can fast later or can compensate by feeding a needy person.5 The time duration between pre-dawn and sunset varies considerably based upon the geographical location and the season. This makes it very important that the patients are properly guided about diet and medication adjustments during Ramadan. Failing this can cause serious complications in patients with diabetes.6,7
The International Diabetes Federation (IDF) and Diabetes and Ramadan International Alliance (DAR) have together developed comprehensive guidelines for diabetes patients intending to fast during Ramadan. These guidelines cover evaluation of risk, adjustment of medicines and guidance about diet.8 Patient education and pre-Ramadan adjustments have been reported to have beneficial effects.9 The pre-Ramadan evaluation must include evaluation for any risks, develop a patient-specific medication adjustment plan and educate the patient about self-management during Ramadan.8 Most research concerning diabetes and fasting during Ramadan originates from Muslim countries; however, due to sociodemographic and geographical differences, different countries have developed their own guidelines for diabetes patients who intend to fast during Ramadan.10
Diabetes self-management behaviors are necessary to ensure optimum glycemic control during Ramadan. A number of sociodemographic factors might affect the knowledge, attitude and practice with regard to Ramadan in patients with type 2 diabetes. Identification of these factors is important to devise appropriate strategies for Ramadan-focused patient education about fasting. This in turn reduces the chance of complications related to diabetes during fasting.6 A study of determinants of knowledge related to diabetes in Kuwaiti adults with T2DM found that illiteracy, limited family income and lack of self-care were the major predictors of a lower level of knowledge about diabetes.11 Likewise, Murata et al and Walker et al reported that socioeconomic, demographic and psychosocial factors in addition to attending a clinic or a group class had an effect on knowledge about diabetes.12–14
No prior study has examined in detail the knowledge, attitude, practice and related determinants regarding Ramadan fasting in patients with T2DM in Saudi Arabia. Therefore, the purpose of this study was to assess knowledge, attitude, practice and related determinants of patients with T2DM attending a diabetes clinic at our hospital with regard to their self-care and management of diabetes during the holy month of Ramadan.
Subjects, Material and Methods
This cross-sectional (descriptive) study was conducted at the Diabetes clinic of King Fahad Hospital of Imam Abdulrahman Bin Faisal University, Alkhobar, Saudi Arabia. Approval of the study was received from the institutional review board (IRB). This clinic has 2243 registered patients with T2DM. We calculated a sample size of 107 using 95% confidence level, 10% accepted margin of error and 50% response distribution. In order to decrease the recall bias, we decided to collect data by “Purposive sampling” during the fasting month (Ramadan) so that the answers were truly reflective of knowledge, attitude and practice. We did not include new patients; we only included patients that were already registered as having T2DM and visited the clinic at least two times over the last six months. Patients who were unable to respond to the questions due to physical or psychological problems were excluded. Participation was voluntary and the purpose of the study was explained to all participants. Written informed consent was received after explaining the protocol and objective of the study. The patients were reassured about proper use and security of data. All the procedures in this study as well as the article written based upon it adhered to the 1964 Helsinki statement and the amendments made to it subsequently.
An Arabic language questionnaire was indigenously developed with the help of University of Michigan Diabetes Research and Training Center Knowledge tests15 and a questionnaire used by a study carried out in Malaysia in 2007.16 The first part of the questionnaire included demographic data that is gender, nationality and duration of disease and family history. This was followed by questions about knowledge (16 items), attitude (6 items) and practice (5 items). The questionnaire was validated by two experts familiar with patient awareness programs. This was followed by pilot testing and reliability analysis. The data from subjects used in pilot testing (n=10) were not included in the results.
The knowledge component consisted of 16 questions. The first 12 were ”General Questions” that the research team felt were essential for successful management of diabetes in patients who intended to fast during Ramadan. The remaining four questions were Ramadan specific. A blend of true and false statements was prepared so that the patients would carefully answer the questions and not just recite the “correct” answer. The patients were told that there was a mix of correct and incorrect statements.
All the questions about knowledge (Table 1), attitude (Table 2) and practice (Table 3) had three choices to choose from: “correct”, “wrong” and “do not know”. Each response was then manually marked correct or incorrect. For the analysis and future planning of patient education, the answer “do not know” was considered an incorrect answer.
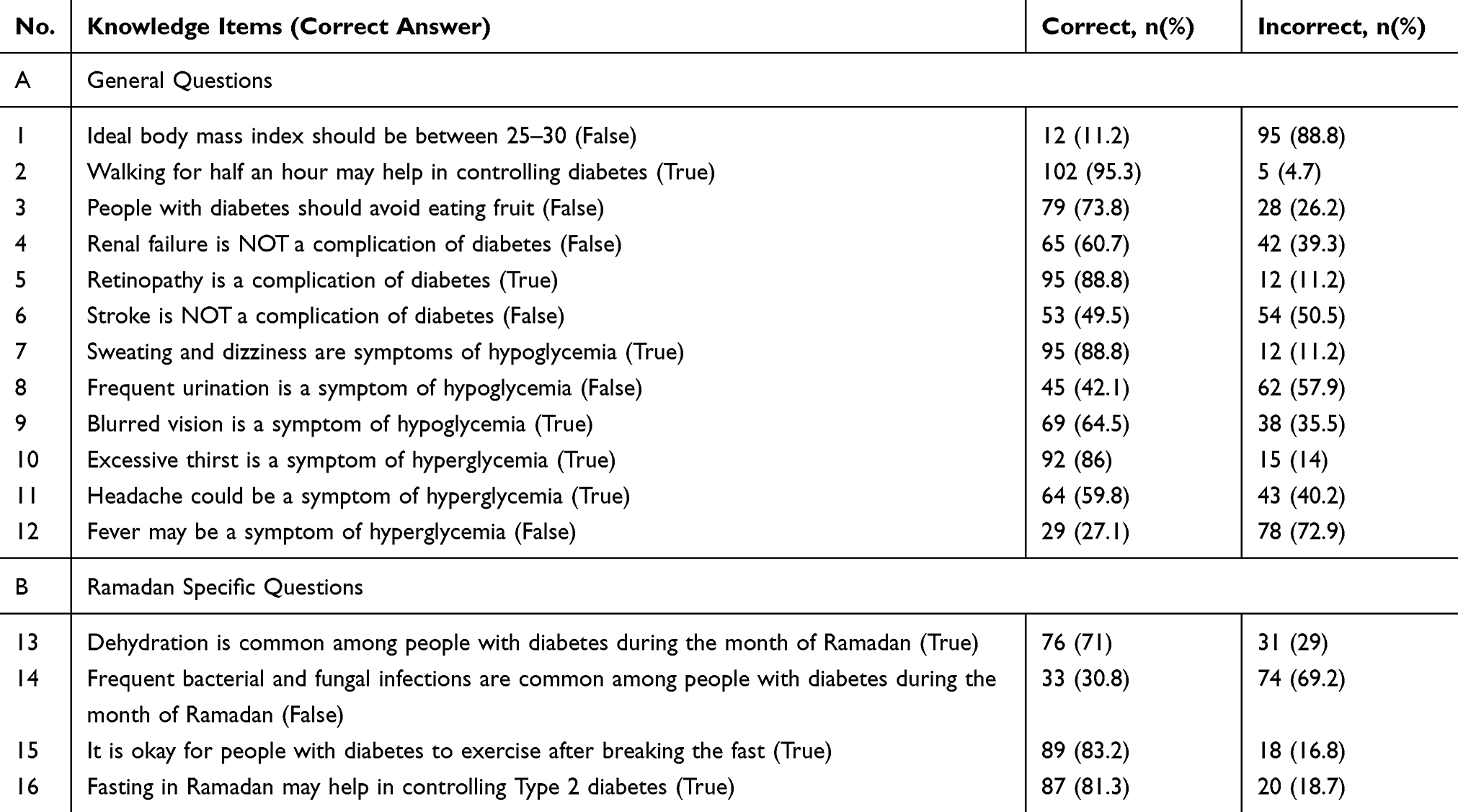 |
Table 1 Knowledge of T2DM in Patients: About Their Disease in General and Fasting During Ramadan (n=107) |
 |
Table 2 Attitude of T2DM Patients About Their Disease in Relation to Fasting During Ramadan (n=107) |
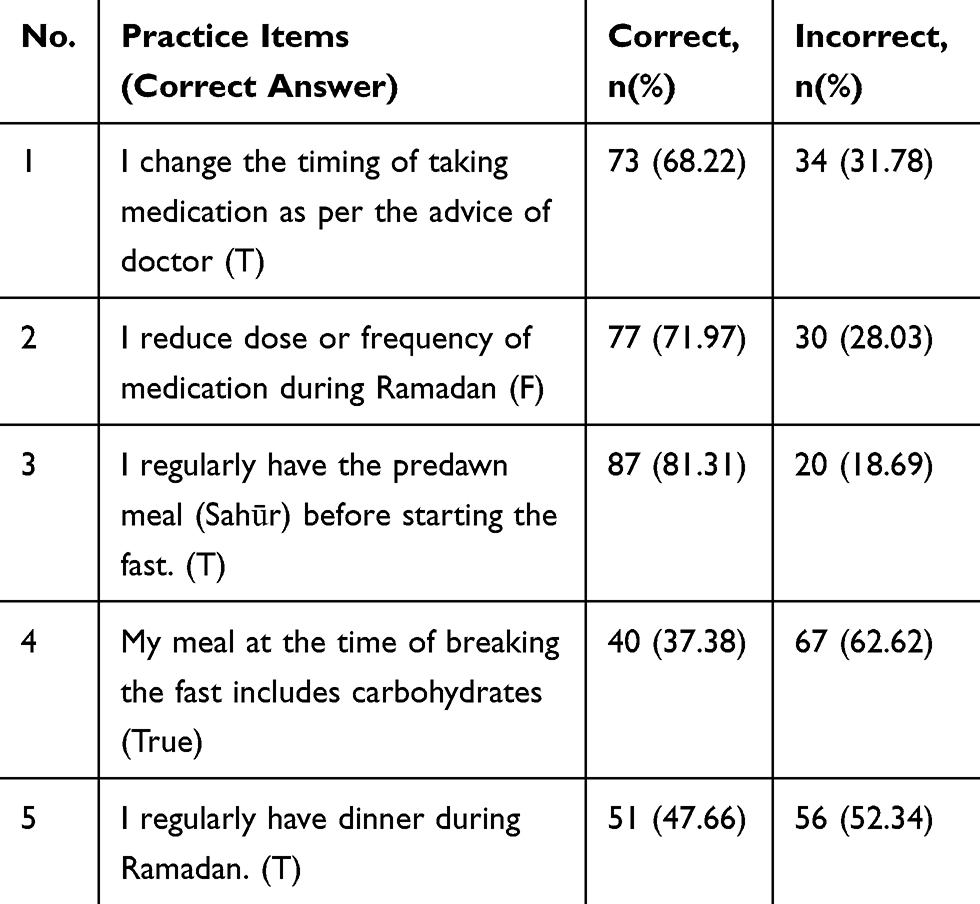 |
Table 3 Practice of T2DM Patients with Regard to Control and Care of Their Disease in Relation to Fasting During Ramadan (n=107) |
The Statistical Package for Social Sciences (SPSS, version 25.0, SPSS Inc., Chicago, IL, USA) was used for data entry and analysis. The correct answers were counted to get the scores. The scores for each individual component were calculated. In addition, the total score was calculated for all the 27 items taken together.
For the descriptive statistics, the mean, standard deviation and frequency tables were computed. For inferential statistics, the chi-square test was used to relate knowledge with gender, nationality, duration of disease, and family history. The independent sample “t” test was used to test the mean difference in the scores of knowledge, attitude and practice between gender, nationality and family history of diabetes; while analysis of variance (ANOVA) was used for the duration of disease, city of residence and level of education. Tukey’s HSD test (post hoc) was used to identify the groups showing significant differences.
Logistic-regression analysis was carried out to determine the association between a binary (potential) predictor and a binary outcome. The independent variables were organized as binary, Gender (Male, Female), Education (Less than secondary, Secondary or more), Family History (Positive, negative) and Duration (up to 5 years, More than 5 years). Likewise, the data were converted into binary for the dependent variables that is Total score (Low: 1–13, Good: 14–27), Knowledge score (Low: 1–8, Good: 9–16), Attitude score (Low: 1–3, Good: 4–6), and Practice Score (Low: 1–3, Good: 4–5). The analysis results were reported as β, SE, Expected β (adjusted Odd’s ratio) and 95% confidence interval (CI). A p value of <0.05 was considered statistically significant.
Results
The results are based upon analysis of 107 qualifying questionnaires. The mean age of patients was 52.94 (±11.63), ranging from 25 to 90 years. The number of male participants was 68 (63.6%) and females were 39 (36.4%). Saudis accounted for 93 (86.91%) while non-Saudis 14 (13.08%). Out of 107 participants, 27 (25.2%) were illiterate or could hardly read and write, 49 (48.5%) had education up to the secondary level and 31 (29%) were educated up to diploma or degree level. Participants were asked about the duration of diabetes and family history. Among 107 patients, 37 (34.57%) had diabetes for less than 5 years, 26 (24.3%) between 6 and 10 years and 44 (41.1%) had diabetes for more than 10 years. Furthermore, a large proportion of the patients (76.6%) had a family history of diabetes. Mean (±SD) scores for knowledge, Attitude and Practice as well as total score are presented in Table 4.
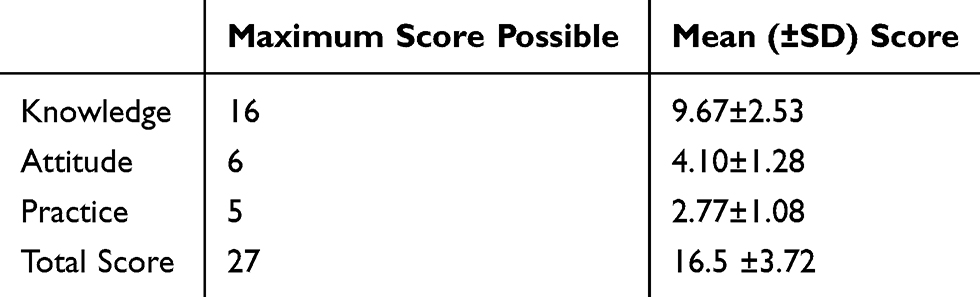 |
Table 4 Mean Scores for Knowledge, Attitude and Practice (n=107) |
The mean score of participants for the knowledge section was 9.67(±2.53) out of the maximum possible score of 16. The frequency of item wise responses is presented in Table 1. The mean score for knowledge was significantly better in males as compared with the females (p-value 0.006). ANOVA test reflected significant (p=0.045) difference of knowledge score due to education, and post hoc Tukey’s HSD identified knowledge score of Diploma, Bachelors, Masters & Doctorate group to be significantly (P=0.034) better than illiterate/just able to read and write participants. The difference in knowledge scores was not significant when tested for the variables: nationality, duration of disease, family history, and city of residence (Table 5).
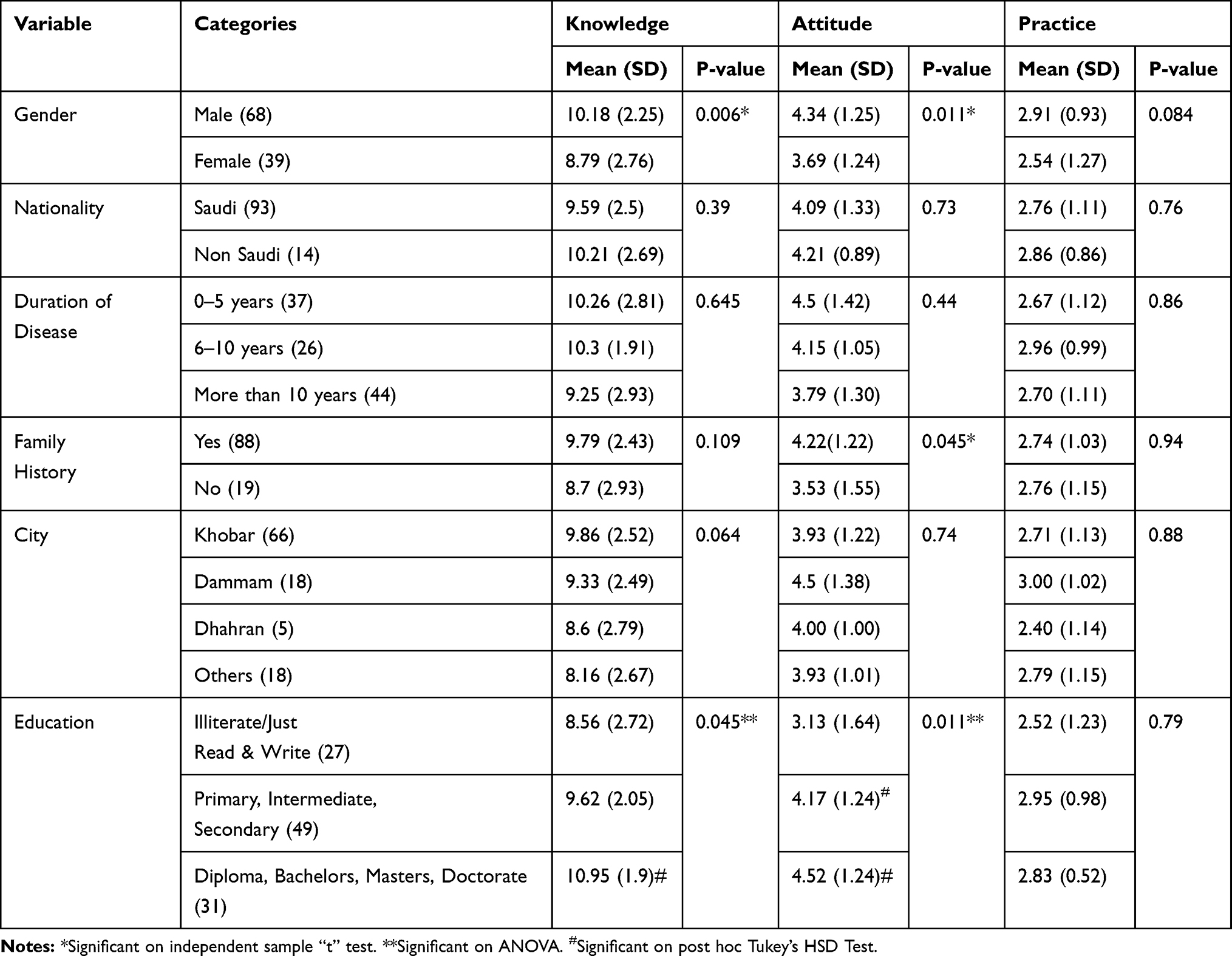 |
Table 5 Relation of Knowledge, Attitude and Practice Score with Demographic Variables |
The mean score for attitude was 4.1(±1.28) out of the maximum possible score of six. The item-wise responses are shown in Table 2. The mean score for attitude was significantly different between male and female (P=0.011) participants and those with a family history of the disease (P=0.045). ANOVA test reflected significant (p=0.011) difference of attitude score due to education, and post hoc Tukey’s HSD identified score of both primary, intermediate, secondary as well as Diploma, Bachelors, Masters, Doctorate group to be significantly (P=0.042 and P=0.036, respectively) better than illiterate/just able to read and write participants. However, the difference was not significant between primary, intermediate, secondary and Diploma, Bachelors, Masters, Doctorate subjects on Tukey’s HSD test. The difference of attitude scores was not significant when tested for the variables: nationality, duration of disease, and city of residence (Table 5).
The mean score for practice questions was 2.77(±1.08) out of a maximum of possible five. The item-wise responses are presented in Table 3. The mean score was not statistically different between any of the variables: gender, nationality, duration of disease, family history, city of residence or level of education (Table 5).
The maximum possible total KAP score was 27. The mean total score was 16.5 (±3.72). The mean total KAP score was significantly lower in the female patients (p=0.020, on independent sample “t” test) and illiterate/just able to read and write patients (as compared with the other education groups on post hoc Tukey’s HSD test). The mean KAP score was not statistically different between nationality, duration of disease, family history or city of residence.
Using logistic-regression analyses, we identified the independent determinants of the total score, as well as individual scores of knowledge, attitude and practice (Table 6). Gender (OR: 4.08, 95% CI: 1.05,15.79 and p<0.041), education (OR: 0.068, 95% CI: 0.008,0.594, p<0.015) and family history (OR: 5.086, 95% CI: 1.095, 23.630 p<0.038) were found to be independent determinants of total score. Education (OR: 0.248, 95% CI: 0.088, 0.702 p<0.009) was determined to be the only independent determinant of knowledge score.
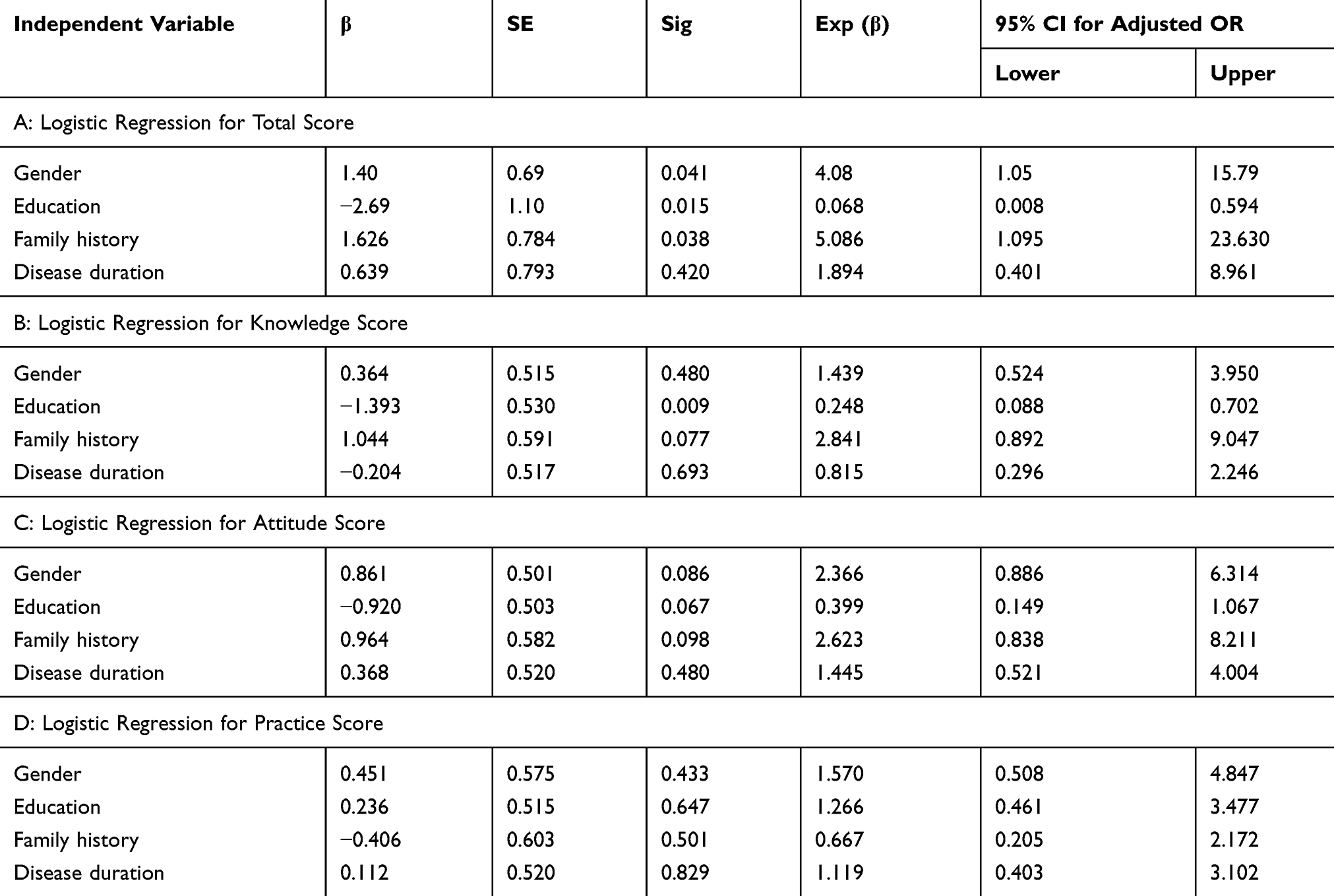 |
Table 6 Logistic Regression Analysis of the Determinants of Knowledge, Attitude and Practice Regarding Ramadan Fasting in T2DM Patients |
Discussion
This study was carried out on T2DM patients attending a diabetes clinic in Eastern Saudi Arabia. The goal of this study was to assess knowledge, attitude and practice about fasting during the Muslim holy month of Ramadan. In addition, sociodemographic factors associated with knowledge, attitude and practice with regard to fasting during Ramadan were evaluated.
The subjects in this study answered most of the Ramadan specific knowledge questions correctly, except that most (69.2%) thought that infections are common in diabetes patients who fast during Ramadan. The results show that although most participants believed that Ramadan fasting helps with the control of type-2 diabetes, yet many were unaware of the potential complications during fasting. The responses of our study population to the general questions about diabetes were overall encouraging; most participants correctly answered about the importance of walking for half an hour, fruit consumption in a controlled manner, complications of diabetes as well as symptoms of increased and decreased blood glucose levels. Surprisingly, in a country with an obesity epidemic, very few (11.2%) participants had correct knowledge about the normal BMI range. Likewise, most (57.9%) wrongly believed that frequent urination accompanies low blood glucose. Similarly, most (72.9%) thought that fever can accompany an increased blood glucose level.
The results of this study showed that male gender, family history of diabetes and education, up to secondary school or more, were associated with a significantly better overall knowledge, practice and attitude score about fasting during Ramadan. In addition, education up to secondary school or more was a significant determinant of knowledge score as well. A study from Singapore reported that young patients and those having at least a secondary school education scored better in knowledge about management of DM while fasting during Ramadan.17 Reports of the relationship between knowledge about DM and gender in non-Ramadan studies are contradictory. Some studies found the knowledge score to be higher in women with diabetes,12,18 while others found scores in women to be worse than among the men.19 A study carried out in Kuwait categorically stated that gender was not associated with the Knowledge score.11 The same study reported that T2DM patients with lower educational levels and negative family history of diabetes had significantly lower knowledge scores.11 Murata et al found that age, years of schooling, duration of treatment, cognitive function, gender and level of depression were independent determinants of the knowledge score.12
The right attitude is very important in the successful management of T2DM as it influences an individual’s choice of action and responses to challenges. The mean score of our subjects for attitude was reasonably good (4.1±1.28 out of total 6). Male gender and education more than secondary school were found to be positively associated with the right attitude. A study reported by Fatima et al showed that age, level of education and previous experience of fasting were important factors in determining the attitude of T2DM patients.20 The impact of presence of diabetes in family on knowledge, attitude and practice of diabetes patients has been noted by many non-Ramadan studies as well. It has been suggested that having a close relative with chronic disease may be a good source of health information.21,22 However, at the same time correct or incorrect knowledge as well as practice might be transferred from that family member or members. Patients with the right attitude are capable of making their own decisions to break or skip fasting in the event of any untoward symptoms.20 Amongst the non-Ramadan studies on T2DM, a study from Taiwan reported that Self-care behavior scores were significantly influenced by gender, education level, economic status, and religious beliefs of older diabetes patients.23 However, a study by Wang et al24 and another by Toljamo and Hentinen25 determined that gender does not influence the attitude towards self-care in diabetes patients. Chen et al observed that T2DM patients with a high level of education had a better attitude towards their disease than those with a low level of education.26
Correct practice is the most important aspect in self-control of diabetes. A sound knowledge or a positive attitude are neutralized if practice is not correct. The answers to questions about practice during Ramadan fasting reflected a significant proportion of incorrect practices. Around 32% admitted to adjustment of the timing of medicine without a doctor’s advice. Likewise, 28% confessed to decreasing the dose or frequency of medicine on their own. Both could have potentially disastrous results, especially as the duration of fasting and the window when eating and drinking that is permissible differs based upon the season and geographical location.7 Around 19% skipped the predawn meal, while an astonishing 52% did not have dinner regularly during Ramadan. A majority (62.62%) avoided carbohydrates at the time of breaking the fast. There is clearly a knowledge-practice gap that might result in unsafe self-management during fasting. Despite the clear knowledge practice gap, none of the sociodemographic factors evaluated in this study were associated with practice.
This type of knowledge-practice gap has been reported by recent studies from Turkey and Singapore. In the Turkish study despite good knowledge about fasting during Ramadan 83.5% of their T2DM subjects did not visit their physician during Ramadan, while 65.8% did not ask advice for fasting from their health professional.27 In the Singapore study, 58.8% of the diabetes patients (89.1% T2DM) had correct general knowledge about DM and 75.9% with regard to fasting knowledge. In those 71.4% of the diabetes patients consulted their physicians before Ramadan, yet 37.3% did not monitor their blood glucose levels. The result was that 47.0% had hypoglycemic episodes, and despite that 10.8% continued to fast.17 A study from France reported that more than half of the patients decided to fast during Ramadan against the advice of their physicians.28
Sound knowledge, the right attitude and correct practices are the backbone of self-control in T2DM patients. Social learning interventions, guidance about diet and “self-efficacy-focused” patient education is known to be helpful for the effective management of diabetes patients.29 Fasting during Ramadan is a potential challenge to self-control. The major risks for the patients with diabetes who fast during Ramadan have been identified as hypoglycemia or hyperglycemia,30 Ketoacidosis,31 dehydration and thrombosis.32
Practice of fasting leads to changes in the timing and frequency of eating meals and taking medications. Thus, diabetes patients should be educated about how to take care of their dietary habits and medication.7 Skipping the dawn or dusk meals, irregularity in taking medicine and overeating at the time of breaking the fast may cause problems for diabetes patients. It is important to be aware of the need for adjustments of medicines during Ramadan. The main therapeutic adjustments are reduction in insulin dose and glucose-lowering agents.30 This must be done under the supervision of the treating physician.
It has been suggested that Ramadan-focused education in diabetes motivates the patients to alter their lifestyle during Ramadan, which in turn decreases the risk of hypoglycemic events and prevents weight gain leading to proper metabolic control.6 Humans tend to forget, that means the learned behaviors change over time.33 Therefore, there is a need to arrange pre-Ramadan educational sessions and not rely on the memory of patients. In a recent Saudi study, a group (n=140) of T2DM patients on insulin who received a Ramadan Focused Education Program (RFEP) was compared with a group (n=122) who did not receive such education. Most subjects of the RFEP group approached the physicians for readjustment of insulin dosage while the patients in the other group did not. In addition, the hypoglycemia score in the RFEP group was lower.9 However, some factors are very deeply inculcated and need extensive education and cooperation by the subjects. Like a recent study from Morocco that investigated the determinants that drive diabetic people to fast reported that the religious beliefs and practices as well as presence of complications influenced the number of total fasting days significantly (P<0.001).34
This study has limitations and they include the following. The study was conducted at a single center, university teaching hospital and therefore generalization of results showed should be carried out with caution. Patients with T2DM visiting primary health care centers might have less or even no access to Ramadan-focused education and therefore have low knowledge and perhaps the wrong ideas about practice. In addition, a cross-sectional design was used, this might have hindered the ability to pinpoint cause-and-effect relationships between variables.
Conclusions
We conclude that male gender, positive family history of diabetes and education more than secondary school are determinants of knowledge, attitude and practice regarding fasting during Ramadan in the T2DM patients. We found a significant knowledge practice gap that needs attention. We recommend further strengthening of the Pre-Ramadan education programs by making them more inclusive especially for female patients, the less educated and those with a negative family history of diabetes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cho NH, Shaw JE, Karuranga S, et al. IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
2. Haddad JA, Haddad AN. The past decade in type 2 diabetes and future challenges. Hormones (Athens). 2018;17(4):451–459. doi:10.1007/s42000-018-0080-y
3. Al-Rubeaan K. National surveillance for type 1, type 2 diabetes and prediabetes among children and adolescents: a population-based study (SAUDI-DM). J Epidemiol Community Health. 2015;69(11):1045–1051. doi:10.1136/jech-2015-205710
4. International diabetes federation. IDF diabetes atlas (Eighth); 2017. Available From https://diabetesatlas.org/across-the-globe.html.
5. Alquran, Chapter-2 (The Cow) Verses. Madinah, Saudi Arabia: King Fahd Complex for the printing of the Holy Quran; 2018:183–184.
6. Bravis V, Hui E, Salih S, Mehar S, Hassanein M, Devendra D. Ramadan education and awareness in diabetes (READ) programme for Muslims with type 2 diabetes who fast during Ramadan. Diabetic Med. 2010;27(3):327–331. doi:10.1111/dme.2010.27.issue-3
7. Zainudin SB, Abu Bakar KN, Abdullah SB, Hussain AB. Diabetes education and medication adjustment in Ramadan (DEAR) program prepares for self-management during fasting with tele-health support from pre-Ramadan to post-Ramadan. Ther Adv Endocrinol Metab. 2018;9(8):231–240. doi:10.1177/2042018818781669
8. Hassanein M, Al-Arouj M, Hamdy O, et al. International diabetes federation (IDF), in collaboration with the diabetes and ramadan (DAR) international alliance. Diabetes and Ramadan: Practical Guidelines. Diabetes Res Clin Pract. 2017;126:303–316.
9. Tourkmani AM, Alharbi TJ, Bin Rsheed AM, et al. Impact of Ramadan focused education program on medications adjustment for patients with type 2 diabetes in a primary health care institution in Saudi Arabia. Diabetes Metab Syndr. 2019;13(1):161–165. doi:10.1016/j.dsx.2018.07.012
10. Bajaj HS, Abouhassan T, Ahsan MR, et al. Diabetes Canada position statement for people with types 1 and 2 diabetes who fast during Ramadan. Can J Diabetes. 2019;43(1):3–12. doi:10.1016/j.jcjd.2018.04.007
11. Al-Adsani AM, Moussa MA, Al-Jasem LI, Abdella NA, Al-Hamad NM. The level and determinants of diabetes knowledge in Kuwaiti adults with type 2 diabetes. Diabetes Metab. 2009;35(2):121–128. doi:10.1016/j.diabet.2008.09.005
12. Murata GH, Shah JH, Adam KD, et al. Factors affecting diabetes knowledge in Type 2 diabetic veterans. Diabetologia. 2003;46(8):1170–1178.
13. Walker RJ, Gebregziabher M, Martin-Harris B, Egede LE. Independent effects of socioeconomic and psychological social determinants of health on self-care and outcomes in Type 2 diabetes. Gen Hosp Psychiatry. 2014;36(6):662–668. doi:10.1016/j.genhosppsych.2014.06.011
14. Walker RJ, Smalls BL, Egede LE. Social determinants of health in adults with type 2 diabetes—contribution of mutable and immutable factors. Diabetes Res Clin Pract. 2015;110(2):193–201. doi:10.1016/j.diabres.2015.09.007
15. Hess GE, Davis WK. The validation of a diabetes patient knowledge test. Diabetes Care. 1983;6(6):591–596. doi:10.2337/diacare.6.6.591
16. Yaacob NA, Ismail AAS, Bebakar WMW. Knowledge, attitude and practice of type 2 diabetes mellitus patients on Ramadan fasting at Hospital Universiti Sains Malaysia. JIMA. 2007;39:6–12.
17. Zainudin SB, Ang DY, Soh AW. Knowledge of diabetes mellitus and safe practices during Ramadan fasting among Muslim patients with diabetes mellitus in Singapore. Singapore Med J. 2017;58(5):246–252. doi:10.11622/smedj.2016085
18. Rhee MK, Cook CB, El-Kebbi I, et al. Barriers to diabetes education in urban patients: perceptions, patterns, and associated factors. Diabetes Educ. 2005;31:410–417. doi:10.1177/0145721705277022
19. Hawthorne K, Tomlinson S. Pakistani Moslems with type 2 diabetes mellitus: effect of sex, literacy skills, known diabetic complications and place of care on diabetic knowledge, reported self-monitoring management and glycaemic control. Diabet Med. 1999;16:591–597. doi:10.1046/j.1464-5491.1999.00102.x
20. Fatima J, Karoli R, Chandra A, Naqvi N. Attitudinal determinants of fasting in type 2 diabetes mellitus patients during Ramadan. J Assoc Phys India. 2011;59:630–634.
21. Harrison TA, Hindorff LA, Kim H, et al. Family history of diabetes as a potential public health tool. Am J Prev Med. 2003;24:152–159. doi:10.1016/S0749-3797(02)00588-3
22. Ezenwaka CE, Offiah NV. Patients’ health education and diabetes control in a developing country. Acta Diabetol. 2003;40:173–175. doi:10.1007/s00592-003-0107-x
23. Bai YL, Chiou CP, Chang YY. Self-care behaviour and related factors in older people with Type 2 diabetes. J Clin Nurs. 2009;18(23):3308–3315. doi:10.1111/j.1365-2702.2009.02992.x
24. Wang CY, Fenske MM. Self-care of adults with non-insulin-dependent diabetes mellitus: influence of family and friends. Diabetes Educ. 1996;22(5):465–470. doi:10.1177/014572179602200506
25. Toljamo M, Hentinen M. Adherence to self-care and glycaemic control among people with insulin‐dependent diabetes mellitus. J Adv Nurs. 2001;34(6):780–786. doi:10.1046/j.1365-2648.2001.01808.x
26. Chen YM, Liao KM, Shu YH, Wu MH, Wang SH, Tsai HC. Relationships between personal perceptions and healthy behaviors of middle-aged diabetic patients. J Chin Med Sci. 2001;2:315–324.
27. Savaş E. Attitudinal determinants of Turkish diabetic patients and physicians about Ramadan fasting. J Relig Health. 2018;57(1):47–56. doi:10.1007/s10943-016-0327-3
28. Gaborit B, Dutour O, Ronsin O, et al. Ramadan fasting with diabetes: an interview study of inpatients’ and general practitioners’ attitudes in the South of France. Diabetes Metab. 2011;37:395–402. doi:10.1016/j.diabet.2010.12.010
29. Jiang X, Wang J, Lu Y, Jiang H, Li M. Self-efficacy-focused education in persons with diabetes: a systematic review and meta-analysis. Psychol Res Behav Manag. 2019;29(12):67–79. doi:10.2147/PRBM.S192571
30. Malek R, Hannat S, Nechadi A, Mekideche FZ, Kaabeche M. Diabetes and Ramadan:a multicenter study in Algerian population. Diabetes Res Clin Pract. 2019;150:322–330.
31. Abdelgadir EI, Hafidh K, Basheir AM, Afandi BO, Alawadi F, Rashid F. Comparison of incidences, hospital stay and precipitating factors of diabetic ketoacidosis in Ramadan and the following month in three major hospitals in United Arab Emirates. A prospective observational study. J Diabetes Metab. 2015;6(514):2.
32. Babineaux SM, Toaima D, Boye KS, et al. Multi-country retrospective observational study of the management and outcomes of patients with Type 2 diabetes during Ramadan in 2010 (CREED). Diabetic Med. 2015;32(6):819–828. doi:10.1111/dme.2015.32.issue-6
33. Dube L, Van den Broucke S, Housiaux M, Dhoore W, Rendall-Mkosi K. Type 2 diabetes self-management education programs in high and low mortality developing countries: a systematic review. Diabetes Educ. 2015;41(1):69–85. doi:10.1177/0145721714558305
34. Al-Balhan E, Khabbache H, Laaziz A, et al. To fast or not to fast during the month of Ramadan? A comprehensive survey on religious beliefs and practices among Moroccan diabetic patients. Diabetes Metab Syndr Obes. 2018;11:633. doi:10.2147/DMSO.S171990
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.