Back to Journals » Nursing: Research and Reviews » Volume 11
Knowledge, Attitude and Associated Factors Towards Heart Failure Management Among Nurses Working in the Cardiac Unit of Selected Government Hospitals in Addis Ababa, Ethiopia: A Cross-Sectional Study
Authors Demissie BM, Bekele DM, Habte T, Wake AD ![]()
Received 16 July 2021
Accepted for publication 1 December 2021
Published 10 December 2021 Volume 2021:11 Pages 41—53
DOI https://doi.org/10.2147/NRR.S329363
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Betelhem Mesfin Demissie,1 Daniel Mengistu Bekele,2 Teshome Habte,2 Addisu Dabi Wake3
1Nursing Department, College of Health Sciences, Woldiya University, Wollo, Amhara Regional State, Ethiopia; 2School of Nursing and Midwifery, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 3Nursing Department, College of Health Sciences, Arsi University, Asella, Oromia Regional State, Ethiopia
Correspondence: Addisu Dabi Wake
Nursing Department, College of Health Sciences, Arsi University, P.O. Box: 193/04, Asella, Oromia Regional State, Ethiopia
Tel +251 910 2867 66
Email [email protected]
Background: Heart failure (HF) is a global pandemic affecting individuals globally and is rising in magnitude. Despite the advancement of treatment for HF, the problem continues to cause substantial hospitalization, economic costs, disability, morbidity, and mortality. However, knowledge, attitude, and associated factors towards HF management in Ethiopia were unknown.
Objective: To assess knowledge, attitude, and associated factors towards HF management of nurses working in the cardiac unit.
Methods: An institution-based cross-sectional survey was conducted on 180 nurses working in a cardiac unit at selected government hospitals in Addis Ababa, Ethiopia. The data were collected from March to April 2020 by self-administered questionnaire. The data were analyzed by using SPSS version 24.0 software.
Results: A total of 180 nurses were enrolled into the study with a response rate of 95%. The mean age of the participants was 31 years. The majority (105; 58.3%) were females. About 108 (60%) of them were married and 34 (18.9%) of them were qualified with a MSc in nursing. More than two-thirds (134; 74.4%) of them had ≤ 6 years of work experience. The majority (131; 72.8%) of them have not taken training on the management of HF. The level of a good knowledge and positive attitude towards the management of HF were 30.56% (n = 55; 95% CI: 24.20– 37.50) and 94.4% (n = 170; 95% CI: 90.6– 97.8), respectively. Having a monthly income of > 6700 Ethiopian birr (AOR = 3.20, 95% CI: 2.87– 9.58), master’s degree in nursing (AOR = 4.35, 95% CI: 3.42– 14.36), having > 6 years of working experience (AOR = 5.21, 95% CI: 4.41– 15.72), and having training about HF management (AOR = 6.18, 95% CI: 4.76, 15.95) were factors significantly associated with knowledge towards HF management.
Conclusion: The level of good knowledge towards HF management was very low, while the level of positive attitude towards HF management was satisfactory. Educational programs and comprehensive training are recommended to take place to improve them.
Keywords: knowledge, attitude, heart failure management, heart failure, nurse
Background
HF is a syndrome manifested by characteristic symptoms and signs, where none of them are specific1 and it results from any structural or functional loss of ventricular filling or ejection of blood.2 Multiple comorbidities, a complex therapeutic regimen, frequent hospitalizations, poor quality of life, and high mortality were its features.3 Ischemic heart disease, hypertension, obesity, diabetes, and smoking have been identified as predictors of both the incidence of HF as well as its severity.4 Hypertensive HF, rheumatic heart disease, dilated cardiomyopathy, pericardial diseases, and HIV-associated cardiomyopathy are the common risk factors for HF.5 Besides, age, male sex, hypertension, hypertrophy, myocardial infarction, diabetes mellitus, valve disease, overweight, excessive alcohol consumption, cigarette smoking, dyslipidemia, renal insufficiency, low physical activity, low socioeconomic status and coffee consumption.6
Non-communicable diseases (NCDs) are one of the leading causes of death worldwide.7 Cardiovascular diseases (CVDs) are accountable for about one-third of deaths globally, and that number will surely rise.8 It is a major cause of lost health in the USA9 and is accountable for the high morbidity and mortality and hospital admissions in Latin America.10 HF is the global epidemic of the 21st century, with significant morbidity and mortality.11 HF is affecting at least 26 million individuals globally.12 HF is an overwhelming clinical and public health problem.13
HF is a worldwide community health concern with inconsistent morbidity and mortality impact in low- and middle-income countries.14 It is an increasing problem in Sub-Saharan Africa (SSA).15 HF is linked to high morbidity and mortality, frequent hospitalization and high economic cost.5 The rise in the prevalence of HF, its associated high mortality, and frequent hospital admissions leads to a considerable economic burden on western healthcare systems.16 The burden of NCDs are rising in Ethiopia,17,18 and CVDs are highly prevalent and cause a high magnitude of morbidity and mortality.19
HF is a burden to subjects, their careers, and health systems.20 HF is also a major societal and governmental challenge.21 It puts a heavy burden not only on subjects and their families but also on society.22 It became a rising frequent reason for hospitalisation and admission during the last two decades.23 Systolic dysfunction is frequently existing in individuals without recognized HF and related to a marked rise in all-cause mortality in the community.24 To prevent the cost of HF health economics, unplanned hospital readmissions are the most significant for consideration.25 The significant predictors of quality of life of patients with HF were identified as age, duration of HF, physical symptoms, and depression.26 The evidence indicated that most HF patients are not examined and treated as per the guidelines. Besides, the barriers for effective HF management are found to be complex in general practice.27
Since HF is found to affect the quality of life of patients,28 those with more severe HF require the option of palliative care just as cancer patients do.29 Care for patients with chronic HF is challenging, due to the progressive nature of the condition.30 The urgent interventions shall be prioritized and scaled up for targeting the cause of HF and preventing its onset and deterioration.31 There is a requirement to develop subject teaching materials and a program.32 There are various socio-demographic and clinical factors associated with self-care among patients with HF.33 Those subjects receiving more intensive education understand more about their HF condition.34 It is advised to provide health educational programs about lifestyle recommendations, complications, and how to deal with their disease for HF patients.28 Patient education is a vital element in the management of patients with HF and nurses are progressively involved in this area.35 Nurses and healthcare professionals have to understand the outcome of low health literacy.36
Nurses working in general practice have a significant role to play in supporting patients with HF to manage their situations.37 Readmission of patients with HF can be decreased through augmented nurses’ knowledge about HF.38 It is significant to identify nurses’ knowledge gaps regarding self-management principles of HF.39 Nurses have a principal role in the HF team because of their outstanding clinical assessment, communication skills, and their ability to work closely with the patients.40 Nurses in many countries give services for individuals with both acute and chronic HF.41 They have a significant role to play in meeting the health and social care challenges at the fore of worldwide health concerns.42 Their management can improve functioning and reduce the hospitalizations of HF patients.43 Care provided by specialist nurses has been revealed to improve outcomes for patients with chronic HF, substantially decreasing mortality, hospital costs, the number of unplanned readmissions, and length of hospital stay.44 There is an improvement in outcome for patients followed up by a multidisciplinary care team in which a nurse was a key player. Such level of care is now recognised in international guidelines.45 They are fundamental to give a patient education about HF.46
Even though the burden of HF is alarmingly increasing globally, there is a lack of studies that have addressed knowledge, attitude, and associated factors towards HF management among nurses working in the cardiac unit of selected government hospitals, in the study area and even in our country, Ethiopia. Therefore, the present study was aimed to determine the knowledge, attitude, and associated factors towards HF management among nurses working in the cardiac unit. The findings from the present study would alert the hospitals, nurses, government, stakeholders, and researchers to manage and control the critical burden of this HF.
Objectives
General Objective
To assess knowledge, attitude, and associated factors towards heart failure management among nurses working in a cardiac unit in selected governmental hospitals in Addis Ababa, Ethiopia.
Specific Objectives
- To determine the level of knowledge towards heart failure management among nurses working in a cardiac unit of selected government hospitals in Addis Ababa, Ethiopia.
- To assess the level of attitude towards the management of heart failure among nurses working in a cardiac unit of selected government hospitals in Addis Ababa, Ethiopia.
- To identify factors associated with knowledge towards heart failure management among nurses working in a cardiac unit of selected government hospitals in Addis Ababa, Ethiopia.
- To identify factors associated with attitudes towards heart failure management among nurses working in a cardiac unit of selected government hospitals in Addis Ababa, Ethiopia.
- To identify factors that are barriers to provide effective heart failure management among nurses working in a cardiac unit of selected government hospitals in Addis Ababa, Ethiopia.
Methods
Study Area and Study Period
The present study was conducted in Addis Ababa, the capital city of Ethiopia. Addis Ababa is home for almost all ethnic groups in Ethiopia with an estimated 6.6 million people in 2017, with about 14 government hospitals. From 14 government hospitals, only 3 hospitals were included in the study. They were Tikur Anbessa Specialized Hospital, Saint Paul Hospital Millennium Medical College, and Saint Peters Specialized Hospital. The present study was conducted from March to April 2020.
Study Design
An institution-based cross-sectional survey was conducted among nurses working in a cardiac unit of selected government hospitals in Addis Ababa.
Source Population
All nurses work in a cardiac unit of selected government hospitals in Addis Ababa.
Study Population
All nurses who are working in a cardiac unit of selected government hospitals and who fulfilled the inclusion criteria.
Eligibility Criteria
Inclusion Criteria
Nurses who have work experience of at least six months in the cardiac unit and willing to participate in the study.
Exclusion Criteria
Nurses who are off duty during the data collection period.
Sample Size Determination
Complete survey was conducted among the selected three government hospitals by census method. Since complete survey was undertaken, all nurses working in a cardiac unit of selected government hospitals were included in the study. The final sample size was 180.
Sampling Technique and Sampling Procedure
Primary purposive sampling technique was employed to select the three government hospitals based on the availability of a cardiac unit. During the survey, the duration of work experience of the nurses was considered for inclusion into the present study. Afterwards, all staff nurses who were present on the day of the survey and who had work experience of at least six months in a cardiac unit and who were willing to participate in the survey were included in the present study.
Study Variables
Dependent Variables
Knowledge towards HF management and Attitude towards HF management.
Independent Variables
Socio-demographic factors: age, gender, marital status, monthly income, in-service training, educational status, and years of work experience.
Operational Definitions
Knowledge of HF management: In the present study, it means that the nurses’ level of understanding about HF management.
Good knowledge: when nurses scored ≥85% based on the 20 items, questions raised on nurse’s knowledge towards HF management survey.47
Poor knowledge: when nurses scored <85% based on the 20 items, questions raised on nurse’s knowledge towards HF management survey.47
Attitude towards HF management: In the present study, it means the nurses’ feelings and approach towards HF management.
Positive attitude: when nurses scored a mean value and above on attitude-related questions.48,49
Negative attitude: when nurses scored less than the mean value on attitude-related questions.48,49
Barrier: In the present study, it means any situation or factor that inhibits the nurses working in a cardiac unit from providing an effective HF management. It was assessed with a dichotomized yes or no question.
Data Collection Tools and Procedures
Self-administered questionnaire was used to collect the data from study participants. It consists of four sections. These were socio-demographic characteristics of nurses, knowledge of nurses towards HF management, attitude of nurses towards HF management, and barriers that are affecting nurses from providing effective HF management. The questionnaires were adapted and developed through careful reviewing of relevant literatures with active participation of the experts. The questionnaires were adapted for knowledge assessment towards HF management in the study conducted by Albert et al. It consists of 20 items, true (yes) or false (no). The validity and reliability of questionnaires were addressed.47 The questionnaires were prepared by reviewing relevant different literatures for the attitude with adjustment fit to the local context48,49 and it consists of18 items. The reliability of the attitude scale was tested in a pilot study conducted. It showed a good level of reliability with Cronbach’s alpha coefficients of 0.798. The responses were based on a 5-point Likert scale from “strongly agree” to “strongly disagree.” These were scored from 5 to 1 respectively, and the scoring was reversed for negative statements so that higher scores indicate a more positive attitude. The questionnaire was prepared in English. Three Bachelor of Science degree (BSc) nurses were data collectors and two Master of Science degree (MSc) nurses’ supervisors were recruited for the study.
Data Quality Control
The questionnaire was pretested on 5% of the calculated sample size before data collection duration. The reliability of the questionnaire was checked by the reliability analysis and suggests a reliable tool. Data collectors and supervisors were trained for one day on the data collection instrument and data collection procedure. During the data collection period, close supervision was carried out by the principal investigator and the supervisors, and the completeness of the collected data was checked on time.
Statistical Analysis
Data were checked, coded, and entered into Epi Info Software version 3.4.5, and then it was exported to Statistical Package for the Social Sciences (SPSS) version 24.0 (IBM Corporation, North Castle Drive, Armonk, NY, USA) for statistical analysis. The presence of multicollinearity was examined using the Variance Inflation Factor and there was no multicollinearity. The outcome variable was dichotomized and coded as (poor knowledge = 0) and (good knowledge = 1), and (negative attitude = 0) and (positive attitude = 1).
Simple descriptive statistics such as mean and standard deviation were used for continuous variables and frequency with percentage distribution was used for categorical variables. Then, the descriptive statistics were summarized using tables, figures, and texts. Bivariable logistic regression and multivariable logistic regression analysis was applied to identify variables associated with knowledge. All independent variables with p-value of <0.25 in bivariable logistic regression analysis were included in the multivariable logistic regression model to identify variables associated with the knowledge. Both crude odds ratio (COR) and adjusted odds ratio (AOR) with the corresponding 95% confidence interval (CI) were calculated to display the strength of the association. Model fitness was checked by Hosmer-Lemeshow’s goodness-of-fit test for knowledge and attitude, while the result was p = 0.87 and p = 0.79, respectively, where p >0.05, and this indicates the model was fit. Finally, variables in the multivariable logistic regression with p-values <0.05 were considered as statistically significant.
Result
Socio-Demographic Characteristics of the Study Participants
A total of 180 nurses were enrolled into the study with a response rate of 95%. The mean age of the participants was (31 years, SD = 5.60) with a range of 25–51 years. The majority (105; 58.3%) of the participants were females. About 108 (60%) of the participants were married and 34 (18.9%) of the participants were qualified with a MSc in nursing. More than two-thirds (134; 74.4%) of the participants had ≤6 years of work experience. The majority (131; 72.8%) of the participants have not taken training on the management of HF (Table 1).
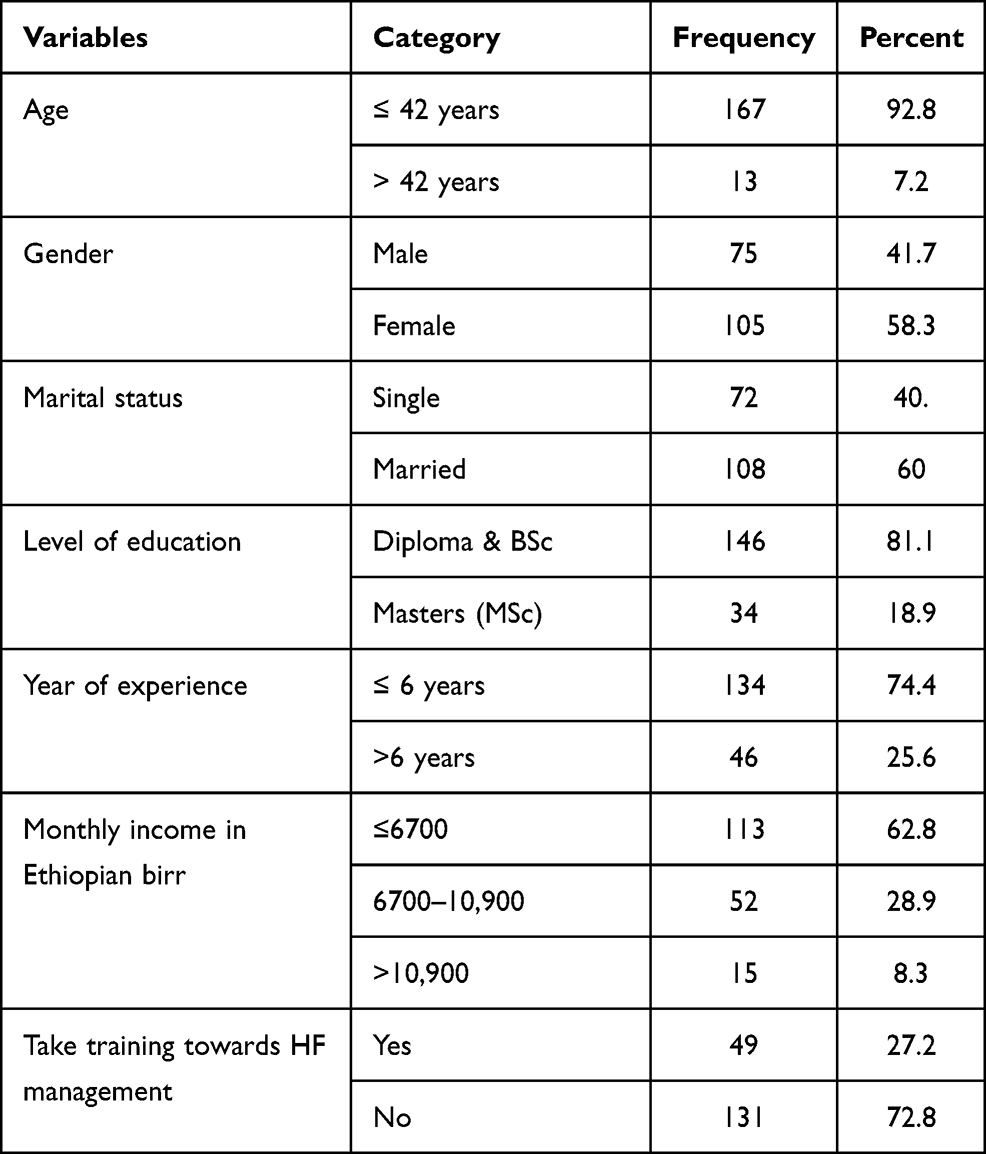 |
Table 1 Socio-Demographic Characteristics of Study Participants at Selected Government Hospitals in Addis Ababa, Ethiopia, 2020 [N= 180]. |
Level of Knowledge Towards HF Management
The participant’s level of good knowledge towards HF management was 30.56% (95% CI: 24.20– 37.50) (Figure 1).
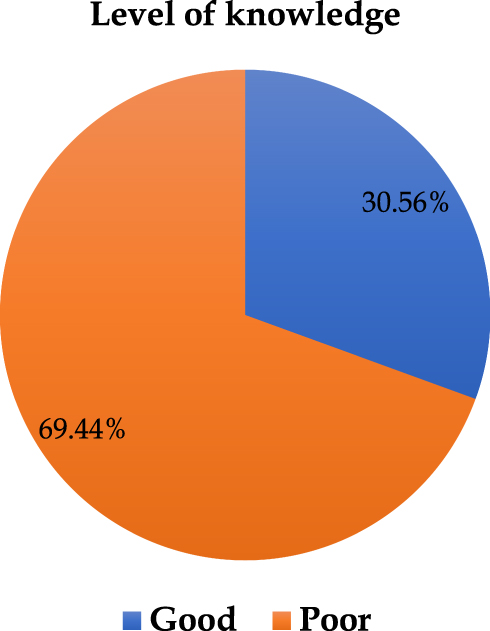 |
Figure 1 Knowledge towards heart failure management among nurses working in a cardiac unit of selected government hospitals, Addis Ababa, Ethiopia, 2020 [n= 180]. |
Knowledge Scores for Each Item Towards HF Management
The questions correctly answered by participants were questions related to fluid (70.6%), diet (80.6%), salt restriction (64.4%), symptoms (cough, nausea) (76.1%), weight (71.7%), signs (swelling of abdomen) (81.7%), ideal weight versus daily weight (53.9%) and diuretic medication (79.4%). Whereas, the questions which had low correct response were questions related to exercise (18.3%), and nonsteroidal anti-Inflammatory drugs (41.7%).
Out of 20 questions, 4 questions assessed the nurses’ knowledge regarding signs and symptoms which should be notified to the physician. Of these 4 questions, the nurses had a low correct response for 2 questions, where (43.3%) for low blood pressure without symptoms and (40%) for dizziness. While, on the rest 2 questions related to new onset of fatigue and leg weakness, they had a high correct response which were 85% and 85.6% respectively. The mean score for all study participants was 13.95 ± 3.541. The range of correct answers was 7–20 out of 20 questions. The percentage of correct responses to individual questions ranged from 18.3–85.6% (Table 2).
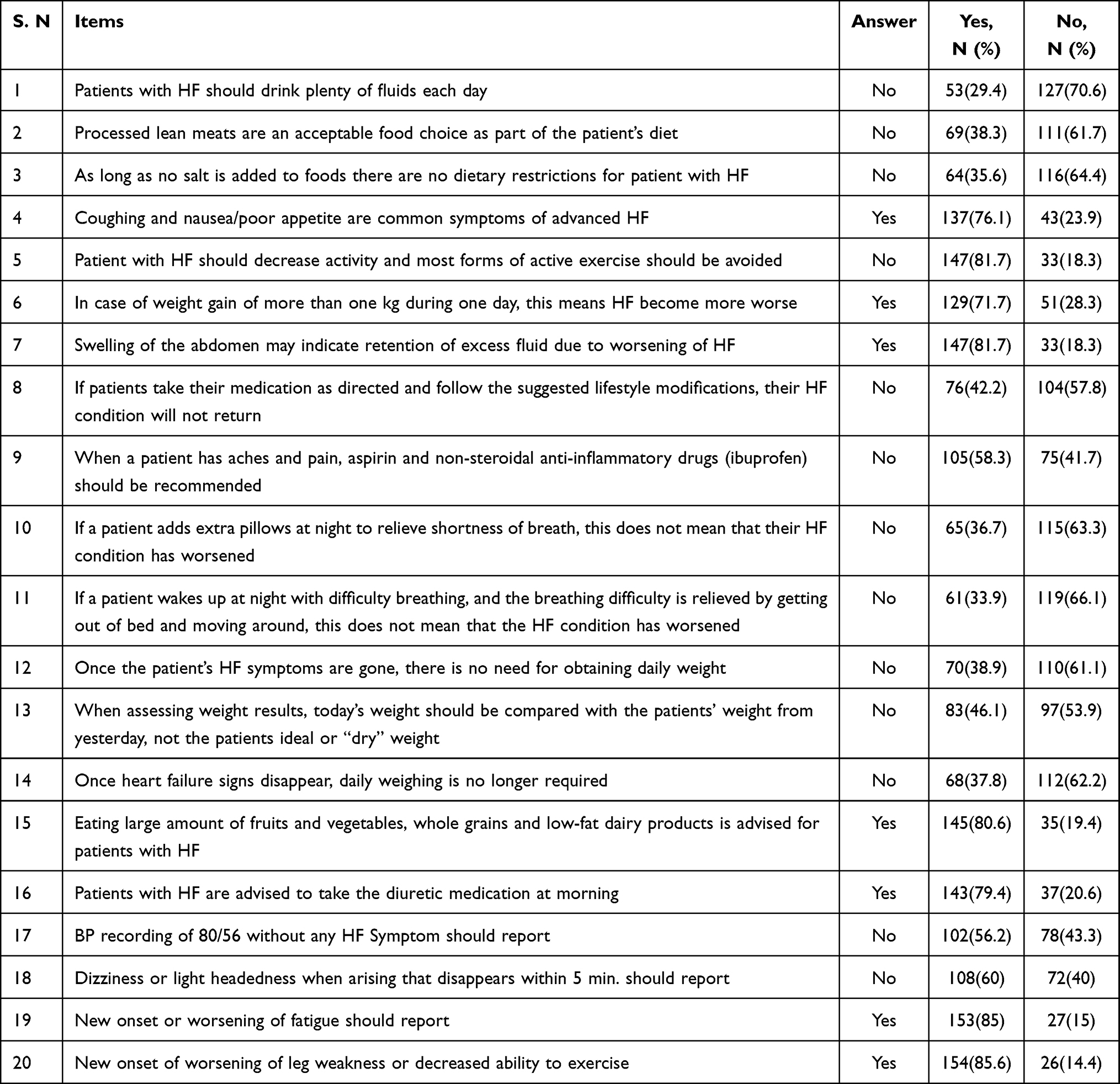 |
Table 2 Knowledge Score on Each Item Towards Heart Failure Management Among Nurses Working in Cardiac Unit of Selected Government Hospitals in Addis Ababa, Ethiopia, 2020 [n = 180]. |
Attitude Towards HF Management
The participant’s level of positive attitude towards HF management was 94.4% (95% CI: 90.6–97.8).
Factors Associated with Knowledge Towards HF Management
Age, gender, marital status, monthly income, educational level, years of working experience, and having training on HF management were factors entered into the final model. According to the results of the multivariable logistic analysis, monthly income, educational level, years of working experience, and having training about HF management were factors significantly associated with knowledge towards HF management. However, age, gender, and marital status were not significantly associated with knowledge towards HF management.
Even though age, gender, and marital status were not significantly associated with knowledge towards HF management, from the participants who were >42 years, the majority (61.5%) of them had good knowledge towards HF management. From the participants who were male, more than one-third (37.3%) of them had a good knowledge towards HF management. From the participants who were married, about 38.0% of them had a good knowledge towards HF management.
The likelihood of having a good knowledge towards HF management among participants who had a monthly income of >6700 Ethiopian birr was 3.20 times (AOR = 3.20, 95% CI: 2.87–9.58) more compared with participants who had the monthly income of ≤ 6700 Ethiopian birr. Likewise, the odds of having a good knowledge towards HF management among participants who have attended Master of degree in nursing were 4.35 times (AOR = 4.35, 95% CI: 3.42–14.36) higher than who had attended a diploma and Bachelor of Science degree in nursing.
Furthermore, those participants who had >6 years of working experience were 5.21 times (AOR = 5.21, 95% CI: 4.41–15.72) more likely to have a good knowledge towards HF management when compared with those who had ≤ 6 years of working experience. Finally, the odds of having a good knowledge towards HF management among participants who had training about HF management were 6.18 times (AOR = 6.18, 95% CI: 4.76–15.95) higher than those who had no training about HF management (Table 3).
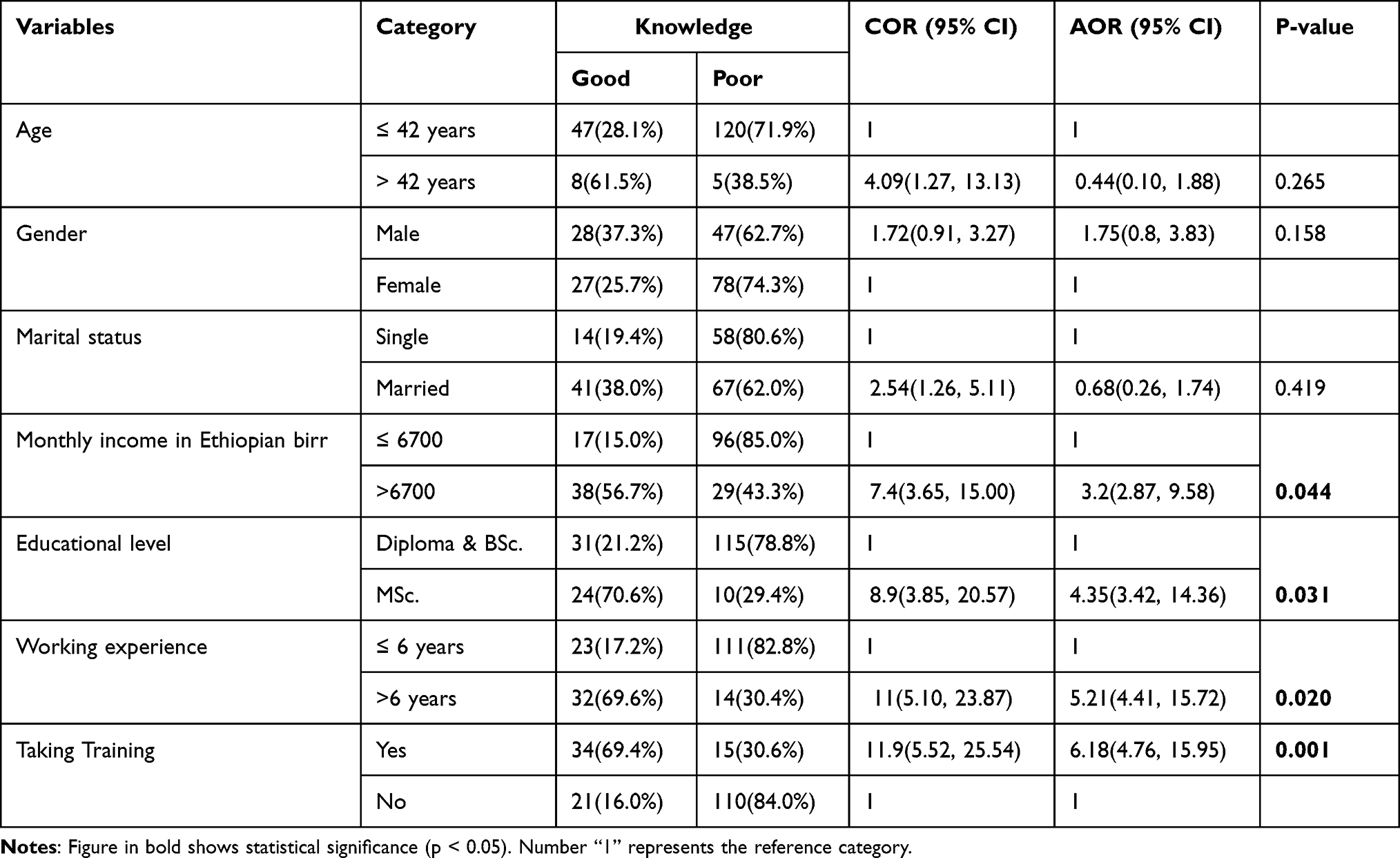 |
Table 3 Bivariate and Multivariate Analysis of Factors Associated with Knowledge Towards Heart Failure Management Among Nurses Working in Cardiac Unit of Selected Government Hospitals Addis Ababa, Ethiopia, 2020 [n = 180]. |
Factors Associated with Attitude Towards HF Management
Because the majority (94.4%) of the participants had a positive attitude towards HF management, the crosstabs results showed that all the variables age, gender, marital status, monthly income, educational level, years of working experience, training about HF management, and knowledge towards HF management violated the chi-square assumption for logistic regression. Therefore, it was impossible to run the logistic regression for attitude towards the HF management. However, the proportion of positive attitude towards the HF management was done respective to age, gender, marital status, monthly income, educational level, years of working experience, training about HF management, and knowledge towards HF management.
From the participants who were >42 years, all (100.0%) of them had a positive attitude towards HF management. From the participants who were female, the majority (96.2%) of them had a positive attitude towards HF management. From the participants who were single, 95.8% of them had a positive attitude towards HF management.
Likewise, from the participants who had a monthly income of >6700 Ethiopian birr, almost all (98.5%) of them had a positive attitude towards HF management. From the participants who were attending a Master of Science degree in nursing, all (100.0%) of them had a positive attitude towards HF management. From the participants who had >6 years working experience, all (100.0%) of them had a positive attitude towards HF management. Furthermore, from the participants who had training about HF management, all (100.0%) of them had a positive attitude towards HF management. From the participants who had a good knowledge towards HF management, the majority (94.5%) of them had a positive attitude towards HF management (Table 4).
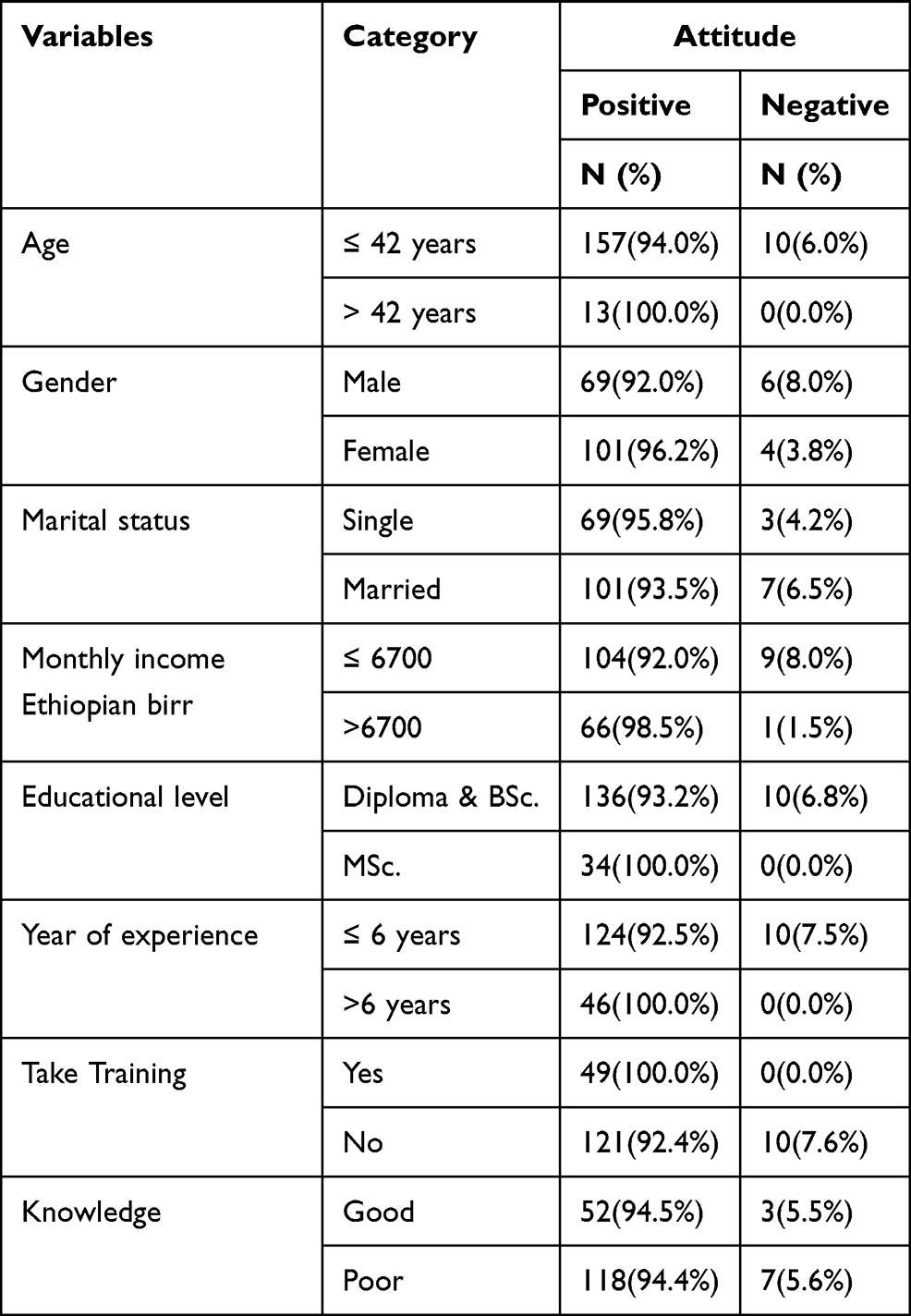 |
Table 4 The Proportion Distribution of Attitude Towards Heart Failure Management Among Nurses Working in Cardiac Unit of Selected Government Hospitals Addis Ababa, Ethiopia, 2020 [n = 180]. |
Barriers Affecting Nurse’s from Providing Effective HF Management
This section was needed to identify potential barriers for nurses’ inability to provide effective HF management. Generally, the barriers were classified as hospital and nurse-related factors. Concerning the hospital-related factors; participants were asked whether or not there was HF management guideline or the standard tools within their working unit. All 180 (100.0%) of the participants answered that there was no HF management guideline or the standard tools within their working unit. The participants were also requested whether or not they had an educational resource to educate the patient about HF management. Just under two-thirds (112; 62.2%) of them answered that they had no educational resources to educate the patient about HF management.
Furthermore, regarding nurse-related factors, the participants were asked whether or not they feel a lack of interest to participate in the education of HF patients. The majority (111; 61.7%) of them responded that they did not feel a lack of interest to participate in the education of HF patients. Finally, the participants were asked whether or not they had a shortage of time or work load to provide education for HF patients. More than half (94; 52.2%) of them responded that they had no shortage of time or work load to provide education for HF patients (Table 5).
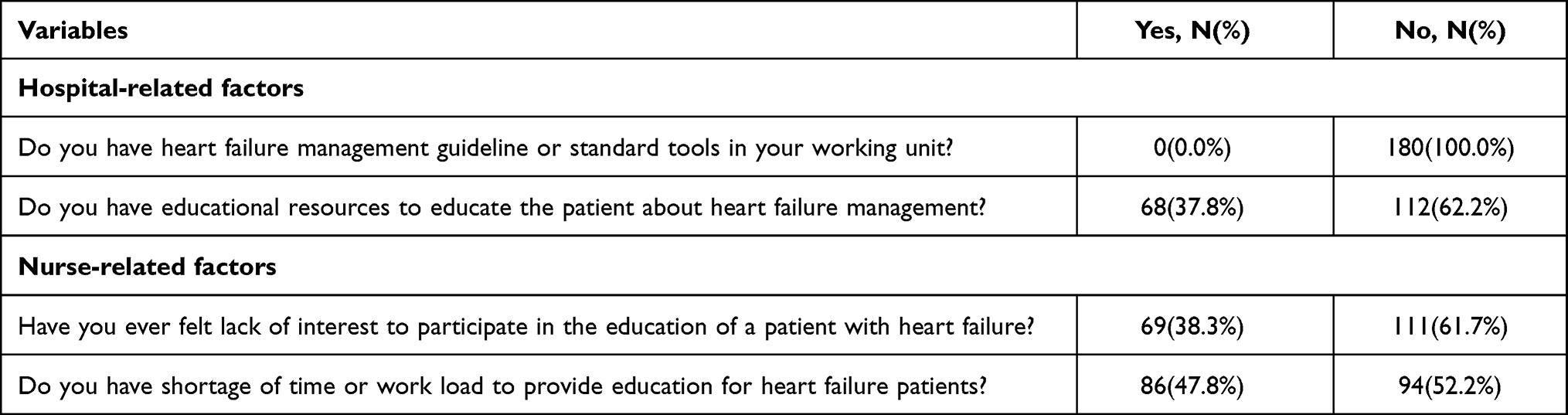 |
Table 5 Hospital and Nurse Related Barriers Affecting Nurse’s from Providing Effective Heart Failure Management Among Nurses Working in Cardiac Unit of Selected Government Hospitals in Addis Ababa, Ethiopia, 2020 [n = 180]. |
Discussion
The present study was conducted to assess the nurses’ level of knowledge, attitude, and associated factors towards HF management among nurses working in a cardiac unit. This is because knowing the level of knowledge, attitude, and associated factors towards HF management are substantial issues that have vital and significant impact on the management of heart failure to control the burden of HF because of its associated serious morbidity, mortality and hospitalization costs.
The present study showed that the level of good knowledge towards HF management was 30.56% (95% CI: 24.20–37.50). The present study finding was lower when compared with the study done in the south-eastern United States which reported the knowledge score of 79.85% towards HF self-management but the author reported it as an inadequate level of knowledge.50 The difference might be because Ethiopia is an economically developing country while the United States is an economically developed country according to the World Bank definition. The present study finding was also lower when compared with the study conducted in Seoul, South Korea, which was 48.3%. However, the authors reported it as an inadequate level of knowledge.49 The variation could be due to the difference in the tool used while the study in Seoul, South Korea, mainly focuses on the nurses’ knowledge towards palliative care for patients with HF.
The present study finding was also lower when compared with the study conducted in Connecticut, United States, which was 78.9%. However, the authors reported this as an inadequate level of knowledge.51 The difference might be because Ethiopia is an economically developing country while the United States is an economically developed country according to the World Bank definition. Besides, there was a difference in the study population, since it was conducted among home care nurses. The present study finding was also lower when compared with the study conducted in Kingdom of Bahrain which was 69.02%. However, the author reported this as an insufficient level of knowledge.48 The present study finding is also lower when compared with the study conducted in Poland which reported the nurses’ knowledge towards HF self-care principles at 63.1%. Even this score was considered as a low level.52 The variation could be due to the difference in the sample size while the study in Poland was done among 227 nurses.
The present study finding is also lower when compared with the study conducted in the northeast United States which was 80%. However, even this was not considered to be knowledgeable.53 The difference might again be because Ethiopia is an economically developing country while United States is an economically developed country according to the World Bank definition. In the present study, the participants had scores greater than 80% on 4 questions. This finding was also lower when compared with a study done in a small mid-western community hospitals where the majority (90%) of the participants answered 6 questions correctly.54 The variation could be due to the differences in socio-demographic characteristics.
The present finding was higher than the study conducted in Catalonia City, Barcelona, where the level of adequate knowledge of the participants was 16.7%.55 This variation might be due to the differences in a sample size and study period, since the study done in Catalonia City, Barcelona, was among 216 nurses in 2014. Since this is a long period of time, during this course of time there could be updated information with regard to the heart failure management strategies.
Regarding the factors associated with knowledge, age, gender, and marital status were not significantly associated with knowledge towards HF management. Even though they were not significantly associated with knowledge towards HF management, from the participants who were >42 years, the majority (61.5%) of them had good knowledge towards HF management. From the participants who were male, more than one-third (37.3%) of them had a good knowledge towards HF management. From the participants who were married, about 38.0% of them had a good knowledge towards HF management.
The likelihood of having a good knowledge towards HF management among participants who had a monthly income of >6700 Ethiopian birr was 3.20 times (AOR = 3.20, 95% CI: 2.87–9.58) more compared with participants who had a monthly income of ≤ 6700 Ethiopian birr. This might be because these nurses may be able to afford expenses for supportive materials for their profession and another source of information concerning the disease and its management approaches. Moreover, the nurse could attend the higher qualifications in private with their own fee.
The odds of having a good knowledge towards HF management among participants who have attended Master of Sciences degree in nursing were 4.35 times (AOR = 4.35, 95% CI: 3.42–14.36) higher than those who had attended a diploma and Bachelor of Science degree in nursing. This was supported by the study conducted in Poland and Barcelona, where the studies reported the association of the higher educational qualification with level of knowledge towards the HF management.52,55 This could be due to the fact that higher education provides better information about HF management and HF-related complications. The education supports to make nurses aware of the disease’s conditions, its seriousness, and its management approach.
Those participants who had >6 years of working experience were 5.21 times (AOR = 5.21, 95% CI: 4.41–15.72) more likely to have a good knowledge towards HF management when compared with those who had ≤ 6 years of working experience. The possible justification is that nurses could be mindful about the HF-related complications and its management approaches during the length of the working experience while they are expected to learn more from their daily practices and what they read.
The odds of having a good knowledge towards HF management among participants who had training about HF management were 6.18 times (AOR = 6.18, 95% CI: 4.76, 15.95) higher than those who had no training about HF management. This is consistent with the study conducted in Catalonia City, Barcelona.55 This might be due to the reason that the training would incorporate all information concerning to the HF management. In fact, this could have a significant impact on the knowledge of the nurses towards the HF management. This was supported by the quasi-experimental study findings done in Medical city at Al Najaf city reporting that the educational program was effective among nurses’ knowledge about HF management. Most (65%) participants have been failed in items in pretest, while they pass (100%) of the items in post-test after being exposed to educational sessions. This also demonstrates that there is good improvement with substantial differences for the participants between pre-and post-test, in overall items.56
Concerning the level of attitude, the present study showed that the level of positive attitude towards HF management was 94.4% (95% CI: 90.6–97.8). The present study finding was consistent with the study conducted in Kingdom of Bahrain which reported that the majority of the participants had a positive attitude.48 The present study finding was higher when compared with the study conducted in Seoul, South Korea, which was reported a low level (134.8±110.1) of participants with positive attitude.49 The variation could be due to the difference in the tool used while the study of Seoul, South Korea, mainly focuses on the nurses’ knowledge towards palliative care for patients with HF.
Furthermore, from the participants who were >42 years, all (100.0%) of them had a positive attitude towards HF management. From the participants who were female, the majority (96.2%) of them had a positive attitude towards HF management. From the participants who were single, (95.8%) of them had a positive attitude towards HF management. From the participants who had a monthly income of >6700 Ethiopian birr, almost all (98.5%) of them had a positive attitude towards HF management. Besides, from the participants who was attending Master of Science degree in nursing, all (100.0%) of them had a positive attitude towards HF management. From the participants who had >6 years work experience, all (100.0%) of them had a positive attitude towards HF management. From the participants who had training about HF management, all (100.0%) of them had a positive attitude towards HF management. From the participants who had a good knowledge towards HF management, the majority (94.5%) of them had a positive attitude towards HF management.
Finally, the potential barriers for nurses’ ability to provide effective HF management were classified as hospital and nurse-related factors. Concerning the hospital-related factors, all (100.0%) of the participants answered that there was no HF management guideline or a standard tool within their working unit. Moreover, a little bit less than two-thirds (62.2%) of them answered that they had no educational resources to educate the patient about HF management. However, the evidence recommends that guideline-based HF management in a nursing home is found to be effective. It can improve staff knowledge, prescribing, and decrease acute care utilization.57 This indicates that the critical problem was that the nurses were placed in a cardiac unit and this may have substantial effects on the knowledge of the nurses to provide the effective HF management. Furthermore, regarding nurse-related factors, the majority (61.7%) of them responded that they did not feel a lack of interest to participate in the education of HF patients. Besides, more than half (52.2%) of them responded that they had no shortage of time or work load to provide education for HF patients. Both factors have the potential to determine the clinical outcome of patients with HF. This is due to the reason that if the nurses had these factors, they could not conduct their activities accordingly and this would affect the nurse’s management for patients with HF.
Conclusions
The present study showed that the nurses’ level of knowledge towards HF management was insufficient. Whereas, the majority of nurses have a positive attitude towards HF management. The multivariable logistic regression analysis showed monthly income, educational level, years of work experience, and having training about HF management were factors significantly associated with knowledge towards HF management.
Further, the potential barriers for nurses’ ability to provide effective HF management were classified as hospital and nurse-related factors. Of which, they lack HF management guidelines or a standard tool within their working unit, and educational resources to educate a patient about HF management were hospital-related factors. Besides, feeling lack of interest to participate in the education of HF patients, and a shortage of time or work load to provide education for HF patients were nurse-related factors.
Furthermore, the present study offers a cornerstone to encourage hospitals, policymakers and implementers, the Ministry of Health, and stakeholders to consider nurses working in a cardiac unit, and it can also support them to focus on and plan methods to address these critical problems. This is because the insufficient knowledge and negative attitude towards the HF management would definitely have a harmful effect on the nurses’ effectiveness of HF management and as a result on patients’ clinical outcomes. On the other hand, if the nurse’s problem is solved, in fact they would provide effective management for the patients with HF which further improves the clinical outcome of these patients. Finally, we recommend that educational programs and comprehensive training are required in order to improve their knowledge and attitude towards HF management.
Abbreviations
HF, Heart failure; SPSS, Statistical Package for the Social Sciences; NCDs, Non-communicable diseases; CVD, Cardiovascular disease; SSA, Sub-Saharan Africa; BSc, Bachelor of Science degree; MSc, Master of Science degree; COR, crude odds ratio; AOR, adjusted odds ratio; CI, confidence interval.
Data Sharing Statement
The data used to support the findings of this study are on the hands of the corresponding author.
Ethical Approval and Consent to Participate
The study was approved by the Institutional Review Board of the Addis Ababa University (Ethics approval reference number; CHS/NSG/201/12). Then the letter was sent to Tikur Anbessa Specialized Hospital, Saint Paul Hospital Millennium Medical College and Saint Peters specialized hospital. Then, permission was obtained from those concerned bodies. The nurses were informed about the objectives and significance of the study and about the confidentiality issues prior to data collection. There were no potential risks that may cause any harm to the nurses. For the reason of privacy and confidentiality, personal identifiers were not used. The nurses were also informed that they have the right to withdraw from the study at any phase. Finally, a written informed consent was obtained from all nurses for the study.
Acknowledgments
We would like to thank the participating supervisors, data collectors, study participants, and Addis Ababa University. Furthermore, this paper was uploaded to the Addis Ababa University repository as a thesis in June 2020. See reference58: http://etd.aau.edu.et/handle/123456789/23316.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by Addis Ababa university.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Krumholz HM, Baker DW, Ashton CM, et al. Evaluating quality of care for patients with heart failure. Circulation. 2000;101(12). doi:10.1161/01.CIR.101.12.e122
2. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure. J Am Coll Cardiol. 2013;62(16):e147–e239. doi:10.1016/j.jacc.2013.05.019
3. Lindenfeld J, Albert NM, Boehmer JP. Executive summary: HFSA 2010 comprehensive heart failure practice guideline. J Card Fail. 2010;16(6):475–539. doi:10.1016/j.cardfail.2010.04.005
4. Bui AL, Horwich TB, Fonarow GC. Epidemiology and risk profile of heart failure. Nat Rev Cardiol. 2011;8(1):30–41. doi:10.1038/nrcardio.2010.165
5. Ogah OS, Adebiyi A, Sliwa K. Heart failure in Sub-Saharan Africa. Top Heart Fail Manag. 2019. doi:10.5772/intechopen.82416
6. Kenchaiah S, Narula J, Vasan RS. Risk factors for heart failure. Med Clin. 2004;88(5):1145–1172. doi:10.1016/j.mcna.2004.04.016
7. World Health Organization. Global status report on noncommunicable diseases 2010. Geneva: World Health Organization; 2011:162. Available from: https://apps.who.int/iris/bitstream/handle/10665/44579/9789240686458_eng.pdf?sequence=1.
8. Deaton C, Froelicher ES, Wu LH, Ho C, Shishani K, Jaarsma T. The global burden of cardiovascular disease. J Cardiovasc Nurs. 2011;26(4):S5–S14. doi:10.1097/JCN.0b013e318213efcf
9. Roth GA, Abate KH, Abd-Allah F, et al. The burden of cardiovascular diseases among US states, 1990–2016. JAMA Cardiol. 2018;3(5):375. doi:10.1001/jamacardio.2018.0385
10. Bocchi EA, Arias A, Verdejo H, Diez M, Gómez E, Castro P. The reality of heart failure in Latin America. J Am Coll Cardiol. 2013;62(11):949–958. doi:10.1016/j.jacc.2013.06.013
11. Luscher TF. Heart failure: the cardiovascular epidemic of the 21st century. Eur Heart J. 2015;36(7):395–397. doi:10.1093/eurheartj/ehv004
12. Savarese G, Lund LH. Global public health burden of heart failure. Card Fail Rev. 2017;03(01):7. doi:10.15420/cfr.2016:25:2
13. Roger VL. Epidemiology of Heart Failure. Circ Res. 2013;113(6):646–659. doi:10.1161/CIRCRESAHA.113.300268
14. Agbor VN, Ntusi NAB, Noubiap JJ. An overview of heart failure in low- and middle-income countries. Cardiovasc Diagn Ther. 2020;10(2):244–251. doi:10.21037/cdt.2019.08.03
15. Gallagher J, McDonald K, Ledwidge M, Watson CJ. Heart failure in Sub-Saharan Africa. Card Fail Rev. 2018;4(1):1. doi:10.15420/cfr.2018:4:1
16. Braunschweig F, Cowie MR, Auricchio A. What are the costs of heart failure? Europace. 2011;13(suppl2):ii13–ii17. doi:10.1093/europace/eur081
17. Gebremariam LW, Chiang C, Yatsuya H, et al. Non-communicable disease risk factor profile among public employees in a regional city in northern Ethiopia. Sci Rep. 2018;8(1):9298. doi:10.1038/s41598-018-27519-6
18. Shiferaw F, Letebo M, Misganaw A, et al. Non-communicable diseases in Ethiopia: disease burden, gaps in health care delivery and strategic directions. Ethiop J Health Dev. 2018;32(3). doi:10.4314/ejhd.v32i3
19. Misganaw A, Mariam DH, Ali A, Araya T. Epidemiology of major non-communicable diseases in Ethiopia: a systematic review. J Health Popul Nutr. 2014;32(1):1–13.
20. Zannad F. Rising incidence of heart failure demands action. Lancet. 2018;391(10120):518–519. doi:10.1016/S0140-6736(17)32873-8
21. Liao L, Allen LA, Whellan DJ. Economic burden of heart failure in? The elderly. PharmacoEconomics. 2008;26(6):447–462. doi:10.2165/00019053-200826060-00001
22. McMurray JJV, Stewart S. The burden of heart failure. Eur Heart J Suppl. 2002;4(suppl_D):D50–D58. doi:10.1016/S1520-765X(02)90160-4
23. Ho KKL, Pinsky JL, Kannel WB, Levy D. The epidemiology of heart failure: the Framingham study. J Am Coll Cardiol. 1993;22(4):A6–A13. doi:10.1016/0735-1097(93)90455-A
24. Redfield MM, Jacobsen SJ, Burnett JC, Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA. 2003;289(2):194. doi:10.1001/jama.289.2.194
25. Toukhsati S, Jaarsma T, Babu A, Driscoll A, Hare D. Self-care interventions that reduce hospital readmissions in patients with heart failure; towards the identification of change agents. Clin Med Insights Cardiol. 2019;13:1179546819856855. doi:10.1177/1179546819856855
26. Hwang SL, Liao WC, Huang TY. Predictors of quality of life in patients with heart failure: QOL in HF patients. Jpn J Nurs Sci. 2014;11(4):290–298. doi:10.1111/jjns.12034
27. Hickling JA, Nazareth I, Rogers S. The barriers to effective management of heart failure in general practice. Br J Gen Pract. 2001;51(469):615–618.
28. Ahmed AA, Abdalla KF. Factors affecting quality of life for patients with congestive heart failure. Med J Cairo Univ. 2016;84(1):8.
29. Bekelman DB, Rumsfeld JS, Havranek EP, et al. Symptom burden, depression, and spiritual well-being: a comparison of heart failure and advanced cancer patients. J Gen Intern Med. 2009;24(5):592–598. doi:10.1007/s11606-009-0931-y
30. Botha A. Care of patients with chronic heart failure: registered nurses’ role. Prof Nurs Today. 2020;24(3):5–10.
31. Lippi G, Sanchis-Gomar F. Global epidemiology and future trends of heart failure. AME Med J. 2020;5:15. doi:10.21037/amj.2020.03.03
32. Zeng W, Chia SY, Chan YH, Tan SC, Low EJH, Fong MK. Factors impacting heart failure patients’ knowledge of heart disease and self-care management. Proc Singap Healthc. 2017;26(1):26–34. doi:10.1177/2010105816664537
33. Koirala B, Dennison Himmelfarb CR, Budhathoki C, Davidson PM. Heart failure self-care, factors influencing self-care and the relationship with health-related quality of life: a cross-sectional observational study. Heliyon. 2020;6(2):e03412. doi:10.1016/j.heliyon.2020.e03412
34. Shaw JD, O’Neal DJ, Siddharthan K, Neugaard BI. Pilot program to improve self-management of patients with heart failure by redesigning care coordination. Nurs Res Pract. 2014;2014:1–10. doi:10.1155/2014/836921
35. Strömberg A. Educating nurses and patients to manage heart failure. Eur J Cardiovasc Nurs. 2002;1(1):33–40. doi:10.1016/S1474-5151(01)00011-1
36. Cajita MI, Cajita TR, Han HR. Health literacy and heart failure: a systematic review. J Cardiovasc Nurs. 2016;31(2):121–130. doi:10.1097/JCN.0000000000000229
37. Brady L. Chronic heart failure and the supportive role of the practice nurse. Pract Nurs. 2015;26(10):500–504. doi:10.12968/pnur.2015.26.10.500
38. Sterne PP, Grossman S, Migliardi JS, Swallow AD. Nurses’ knowledge of heart failure: implications for decreasing 30-day re-admission rates. Medsurg Nurs. 2014;23(5):321–329.
39. Hart PL, Spiva L, Kimble LP. Nurses’ knowledge of heart failure education principles survey: a psychometric study: nurses’ knowledge of heart failure. J Clin Nurs. 2011;20(21–22):3020–3028. doi:10.1111/j.1365-2702.2011.03717.x
40. Angelidou D. Caring for the heart failure patient: contemporary nursing interventions. Hosp Chron. 2010;8:22–29.
41. Riley JP, Astin F, Crespo-Leiro MG, et al. Heart Failure Association of the European Society of Cardiology heart failure nurse curriculum: heart failure nurse curriculum. Eur J Heart Fail. 2016;18(7):736–743. doi:10.1002/ejhf.568
42. Richards DA, Borglin G. Complex interventions and nursing: looking through a new lens at nursing research. Int J Nurs Stud. 2011;48(5):531–533. doi:10.1016/j.ijnurstu.2011.02.013
43. Sisk JE, Hebert PL, Horowitz CR, McLaughlin MA, Wang JJ, Chassin MR. Effects of nurse management on the quality of heart failure care in minority communities: a randomized trial. Ann Intern Med. 2006;145(4):273. doi:10.7326/0003-4819-145-4-200608150-00007
44. Grange J. The role of nurses in the management of heart failure. Heart. 2005;91(suppl_2):ii39–ii42. doi:10.1136/hrt.2005.062117
45. Riley J. The key roles for the nurse in acute heart failure management. Card Fail Rev. 2015;1(2):123. doi:10.15420/cfr.2015.1.2.123
46. Ekong J, Radovich P, Brown G. Educating home healthcare nurses about heart failure self-care. Home Healthc Now. 2016;34(9):500–506. doi:10.1097/NHH.0000000000000453
47. Albert NM, Collier S, Sumodi V, et al. Nurses’s knowledge of heart failure education principles. Heart Lung. 2002;31(2):102–112. doi:10.1067/mhl.2002.122837
48. Sanad HM. Nurses’ knowledge and attitude towards management of patients with heart failure. J Adv Pharm Educ Res. 2017;7(4):7.
49. Kim S, Hwang WJ. Palliative care for those with heart failure: nurses’ knowledge, attitude, and preparedness to practice. Eur J Cardiovasc Nurs. 2014;13(2):124–133. doi:10.1177/1474515113519521
50. Willette EW, Surrells D, Davis LL, Bush CT. Nurses’ knowledge of heart failure self-management. Prog Cardiovasc Nurs. 2007;22(4):190–195. doi:10.1111/j.0889-7204.2007.06403.x
51. Delaney C, Apostolidis B, Lachapelle L, Fortinsky R. Home care nurses’ knowledge of evidence-based education topics for management of heart failure. Heart Lung. 2011;40(4):285–292. doi:10.1016/j.hrtlng.2010.12.005
52. Jankowska-Polańska B, Brzykowska M, Uchmanowicz I, Lisiak M, Rosinczuk J. Polish nurses’ knowledge of heart failure self-care education principles. Clin Nurse Spec. 2017;31(3):E7–E13. doi:10.1097/NUR.0000000000000295
53. Fowler S. Improving community health nurses’ knowledge of heart failure education principles: a descriptive study. Home Healthc Nurse. 2012;30(2):91–99. doi:10.1097/NHH.0b013e318242c5c7
54. Washburn SC, Hornberger CA, Klutman A, Skinner L. Nurses’ knowledge of heart failure education topics as reported in a small Midwestern community hospital. J Cardiovasc Nurs. 2005;20(3):215–220. doi:10.1097/00005082-200505000-00014
55. Dalfó‐Pibernat A, Duran X, Garin O, et al. Nursing knowledge of the principles of self‐care of heart failure in primary care: a multicentre study. Scand J Caring Sci. 2020;34(3):710–718. doi:10.1111/scs.12775
56. Al-Hchaim S, Hamza R. Effectiveness of educational program on nurse’s knowledge about management of patients with heart failure. Int J Sci Res Publ. 2016;6:416–2250.
57. Heckman GA, Shamji AK, Ladha R, et al. Heart failure management in nursing homes: a scoping literature review. Can J Cardiol. 2018;34(7):871–880. doi:10.1016/j.cjca.2018.04.006
58. Mesfin B. Knowledge attitude and associated factors towards heart failure management among nurses working in cardiac unit of selected government hospitals, Addis Ababa, Ethiopia, 2020, [dissertation]. Addis Ababa: University of Addis Ababa; 2020. Available from: http://etd.aau.edu.et/handle/123456789/23316.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.