Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 6
Knowledge about human immunodeficiency virus infection and sexual behavior among drug users: a cross sectional study in Pokhara submetropolitan city, Nepal
Authors Neupane SR, Mishra SR
Received 7 November 2013
Accepted for publication 10 December 2013
Published 12 February 2014 Volume 2014:6 Pages 1—7
DOI https://doi.org/10.2147/HIV.S57176
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Sanjeev Raj Neupane, Shiva Raj Mishra
Maharajgunj Medical Campus, Institute of Medicine, Kathmandu, Nepal
Abstract: Drug abuse is one of the public health problems in Nepal. Only limited research has been done to explore knowledge and sexual behaviors of injection drug users in Nepal. The objective of this research was to explore knowledge about human immunodeficiency virus (HIV) infection and sexual behavior among drug users in Nepal. More than 90% of participants had heard of HIV. Almost all participants who had heard of HIV knew that HIV is transmitted through unsafe sexual intercourse and through syringe use. In comparison to that, a small percentage of participants knew of infected blood and mother to child as modes of transmission of HIV. Injection drug users were less likely to use condoms during sexual intercourse with their wives. Awareness programs and behavior-change communication to alert drug users to the risks of sharing syringes need to be conducted, in addition to promoting the use of condoms during sexual intercourse with other women as well as with their wives.
Keywords: drug use, HIV, Nepal, sexual behavior
Background
Drug abuse is a public health problem in Nepal, like in other developed and developing countries. It is very difficult to say from when exactly the drug-abuse problem started in Nepal. Some drugs, such as cannabis and alcohol, have been traditionally used in Nepal for centuries. Use of cannabis derivatives such as marijuana (locally referred to as ganja) and bhang (an infusion of cannabis) is often justified in connection with religious festivals because of the presumed predilection by one of the principal figures of the Hindu pantheon, the lord Shiva, for the drug.1 Drug use began to be noticed as a problem since the 1960s in Nepal. With the influx of large numbers of hippies from Western world, the sporadic use of drugs later shifted from cannabis to synthetic opiates and sedatives. Being traditionally used in certain religious contexts and easy availability of heroin are some of the reasons responsible for such change. The mode of drug administration also changed from smoking or ingesting to injecting.2,3
According to the 2008 World Drug Report, approximately 208 million people or 4.9% of the world’s population aged 15–64 years had used drugs at least once in the previous 12 months. The proportion of drug users in the world population aged 15–64 years has remained basically stable since the 1990s. The prevalence of drug users in the late 1990s was 4.8%, and in 2008 it was 4.9%, a slight increase from the 1990s level.4 Approximately 16 million people worldwide inject drugs, with 3 million infected with human immunodeficiency virus (HIV). High levels of HIV infection among injection-drug users (IDUs) are observed in South and Southeast Asia, Eastern Europe, and Latin America.4–6
Estimating the number of IDUs in Nepal is a challenge, because of a lack of credible data and the hidden nature of the target population. The estimates done in the 1990s estimated the number of IDUs in Nepal in the range of 2,500–4,000, of whom 2,000 were said to be in Kathmandu Valley and 1,200 in Pokhara. Just as there is a wide variation in estimations of number of IDUs, the same is the case with HIV prevalence among IDUs. Up to 1995, the HIV prevalence among male IDUs in Nepal was less than 2%, and this figure increased substantially to 40% in 1999. In 2007, new data disseminated by the National Centre for AIDS and STD Control, New Era Nepal, and Family Health International showed that 34.7% of IDUs in Kathmandu, 6.7% in Pokhara, 17.1% in Eastern Terai, and 11% in West-Far-West Terai were HIV-positive.7
IDUs are at high risk of blood-borne infections, including HIV, hepatitis B, and hepatitis C through sharing of needles, syringes, and other injection paraphernalia.8 Amidst this scenario, there is very limited research on HIV knowledge and sexual behaviors of IDUs in Nepal. The objective of this research was to explore knowledge about HIV infection and sexual behavior among drug users in Nepal.
Materials and methods
Study setting
This study was conducted among drug users in Pokhara submetropolitan city in Kaski District of Nepal. Kaski District of the Western Region of Nepal has a population of 492,098 people, of which 53% (264,991) are living in Pokhara.9 It is estimated that 5,500 drug users in total, including 700 IDUs, live in Pokhara. The Integrated Biological and Behavioral Surveillance Survey (IBBS) in 2009 reported that the IDUs in Pokhara were mostly young, including 88% below 30 years of age and 61% younger than 25 years. They represented diverse caste/ethnic groups residing in the valley. The Tibeto-Burman communities (Tamang, Lama, Magar, Gurung, Rai, Newar) make up the largest proportion of IDUs (58.5%), followed by the Brahmin and Chhetri/Thakuri communities (27.1%). IDUs had a 3.4% prevalence of HIV infection.10 This study took place with the support of Naulo Ghumti Nepal. Established in 2002, this organization provides drug-counseling, treatment, and rehabilitation services in Pokhara.11
Study design and sampling
A cross-sectional survey was conducted among drug users of Pokhara in 2009. The sample size was calculated through Epi Info (version 3.5; Centers for Disease Control and Prevention, Atlanta, GA, USA). Based on a prevalence of 20% at a 95% confidence interval and 20% nonresponse rate, a sample of 448 was calculated. Of these, 412 gave consent to participate in the study. From those, eight questionnaires were incomplete and not included in the analysis. Finally, there were 404 participants in the study. The final sample size was higher than the expected, due to the high response rate (92%).
In partnership with a local nongovernmental organization (Naulo Ghumti Nepal), social mapping of Pokhara was done. Pokhara submetropolitan city was divided into six different clusters. A list of IDUs in each cluster was prepared with the help of service registers of community mobilizers and outreach workers working in Naulo Ghumti Nepal, who themselves were recovering IDUs. From each cluster, IDUs were drawn randomly according to their proportion from total samples. The researcher then traced the selected samples with the help of community mobilizers and outreach educators. The randomly selected IDUs were approached up to three times if they were not available at their place of residence during the first visit. If not available after three visits or if the randomly selected IDU refused to give consent, they were replaced by the next IDU on the list. There was no record of oral drug users (ODUs), so they were selected through the “snowball” technique with the help of community mobilizers and outreach educators. Drug users who had not used any drugs in the previous 6 months and IDUs who started directly with injection were excluded from the study.
The questionnaire used in this study was adapted from the 2007 IBBS study in Nepal. Pretesting of the tool was done in the Lekhnath municipality of Kaski District to ensure cultural adaptability. Altogether, 20 drug users (ten IDUs and ten ODUs) were interviewed with the questionnaire for pretesting. These respondents were not selected in data collection.
Research ethics
This study obtained ethical approval from the Department of Community Medicine and Public Health. The objectives and benefit of the research to the participants were clearly explained before starting the interview. Written or thumbprint consent was taken from each participant before starting the interview, and participants were given the right to leave the interview or skip any particular question if they found difficulty in answering.
Data processing and analysis
The structured questionnaires were edited on the evening of the day of data collection. Data entry was done in Epi Info 3.5. The database was then exported to SPSS 13.0 (SPSS Inc., Chicago, IL, USA) for analysis. Descriptive analysis was done. A χ2 test was done, and odds ratios were calculated for certain variables in the analysis.
Age, age at first drug use, occupation, ethnicity, educational status, marital status, and age at first marriage were expressed as frequencies and percentages after descriptive analysis. Awareness of HIV, knowledge about HIV transmission, HIV prevention, sexual behaviors, age at first sexual intercourse, and motivating factors for drug use were analyzed against demographic characteristics using χ2 tests and odds ratios.
Defining variables
The variables used in the descriptive analysis were age, gender, education level, age at initiation of drug use, injection practice of sexual partner, and sexual behavior. The IDUs included those who had started taking drugs through noninjection routes and ultimately changed their route of drug administration to the injection route. Drug users who were taking drugs through routes other than injection were defined as ODUs in this study.
Results
General characteristics of drug users
Most of the study participants were in their twenties, and 61% of them were unmarried. Among those who were married, 21% had married before the age of 19 years. The majority of the participants were unemployed. People from all ethnic groups were represented in this study. Brahmin and Chhetri together comprised 28% of the participants. The largest percentage was Gurung/Rai/Pun (37%). Nearly half the participants had completed a secondary level of education (47.5%), and 6.7% were illiterate (Table 1).
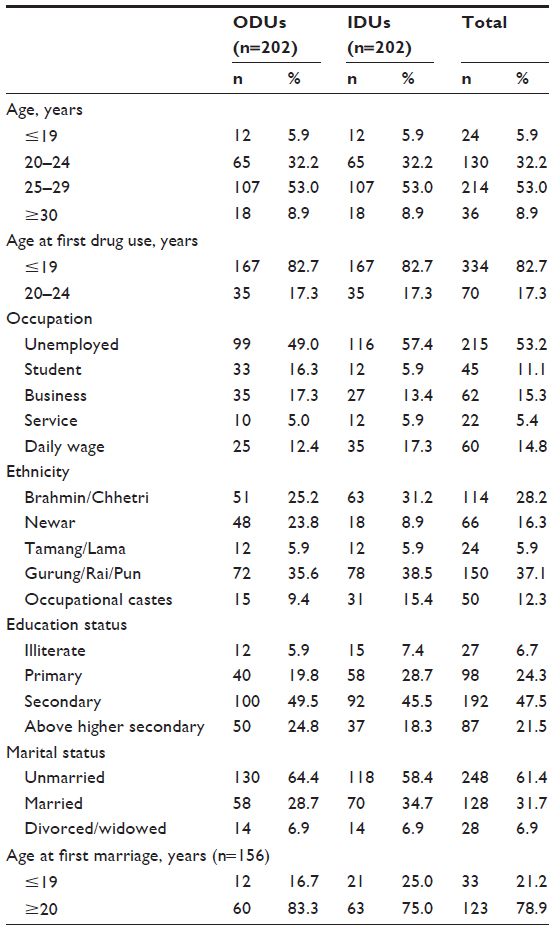 | Table 1 General characteristics of the participants |
Knowledge of HIV
The majority of the participants had heard of HIV: 90% of ODUs and 94% of IDUs. Though the majority of the participants responded that they had heard of HIV, when they were asked further about the modes of transmission of HIV, they could not list them all. Almost all of the ODUs and IDUs who had heard of HIV knew that HIV is transmitted through unsafe sexual intercourse and through syringe use. However, among ODUs, only 79% knew that HIV is transmitted through infected blood and 68% knew that HIV is transmitted from mother to child. Similarly, among IDUs, 85% knew that HIV is transmitted through infected blood and 73% knew that HIV is transmitted from mother to child (Tables 2–4). When cross-tabulated with the education level of the participants, almost all with both primary and below and secondary and above level of education said unsafe sexual intercourse and syringe use were modes of transmission of HIV.
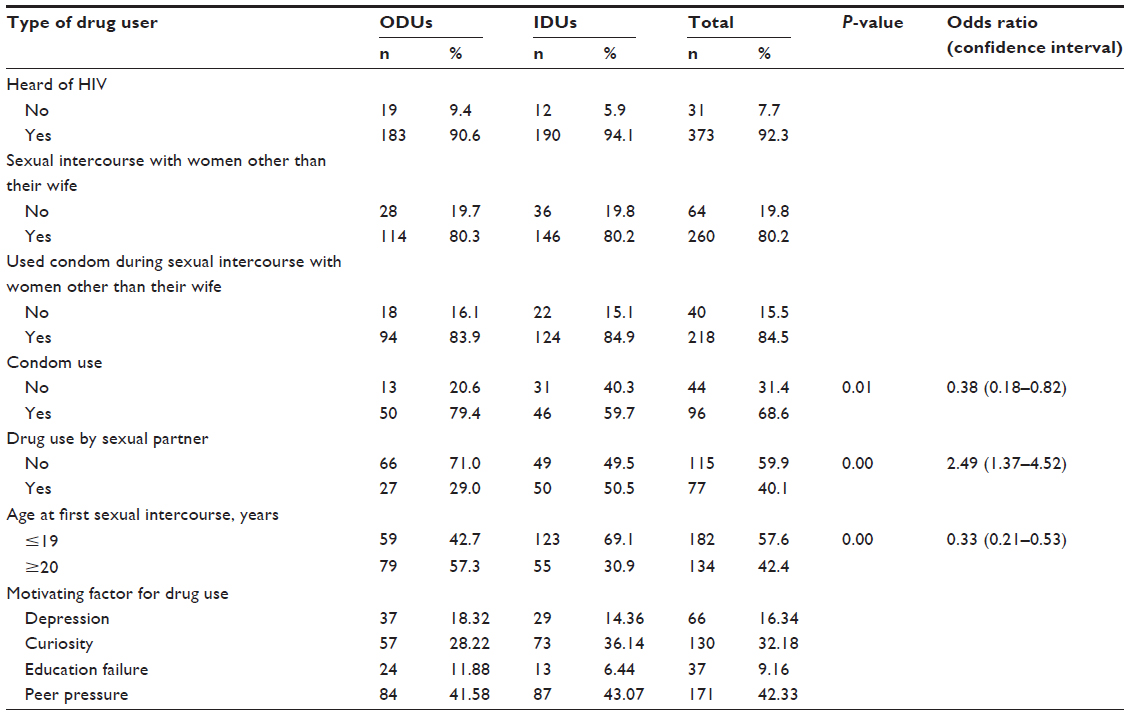 | Table 2 Oral and injection-drug use by knowledge, and sexual behaviors |
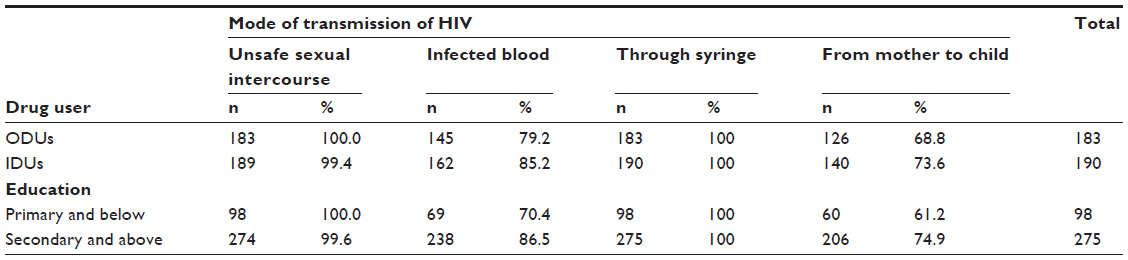 | Table 3 Knowledge about mode of transmission of human immunodeficiency virus (HIV) by type of drug user, and educational status (multiple responses) |
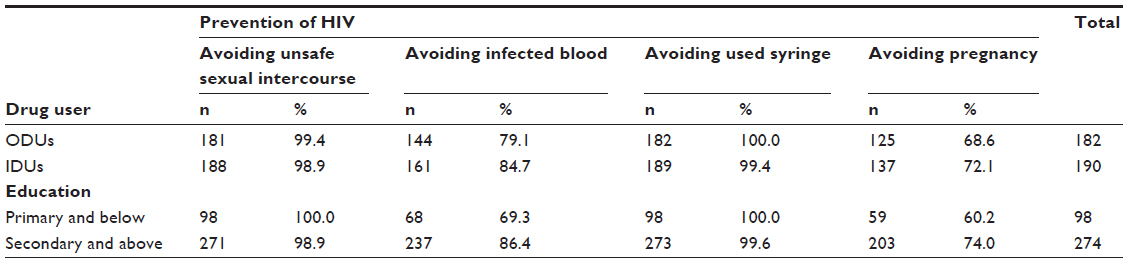 | Table 4 Knowledge about prevention of human immunodeficiency virus (HIV) by type of drug user (multiple responses) |
Almost all IDUs and ODUs suggested avoiding unsafe sexual intercourse and avoiding used syringes as methods of prevention of HIV. However, among ODUs, only 79% knew that avoiding infected blood could prevent HIV, and 68% knew that avoiding pregnancy in an infected mother could prevent transmission of HIV. Similarly, among IDUs, 84% knew that avoiding infected blood could prevent HIV, and 72% knew that avoiding pregnancy could prevent transmission of HIV.
Respondents with an education level of secondary and above had more comprehensive knowledge in comparison to the respondents with an education level of primary and below (Table 3).
Sexual behaviors of drug users
Of both ODUs and IDUs, 20% had not had sexual intercourse with other women except for their wife, and 80% had had sexual intercourse with women other than their wife (Table 2). Among ODUs, 16% did not use a condom and 84% used a condom during sexual intercourse with other women (Table 2). Similarly, among IDUs, 15% did not use a condom and 85% used a condom during their most recent sexual intercourse with other women. More than half (58%) of the drug users had sexual intercourse for the first time when they were 19 years old or less, and 42% of the participants had sexual intercourse for the first time when they were 20 or more years of age (Table 2). Of ODUs, 80% used a condom during sexual intercourse with their wife, and among IDUs, 60% used a condom during sexual intercourse with their wife (Table 2). The mean age at first sexual intercourse of ODUs and IDUs was 19.64 years (standard deviation 2.74 years) and 18.57 years (standard deviation 2.53 years), respectively.
Drug use by sexual partner
Among ODUs, 29% of their sexual partners also used drugs, and 71% of their sexual partners did not use drugs. Similarly, among IDUs, 49% had sexual partners who also took drugs, and 50% of their sexual partners did not take drugs (Table 2).
For both IDUs and ODUs, peer pressure was the main motivating factor to initiate drug use. Around 42% of the participants started to take drugs because of peer pressure, followed by curiosity (32%), depression (16%), and education failure (9.16%) (Table 2).
There was a statistically significant association between the type of drug user and use of condoms during sexual intercourse with their wife. IDUs were less likely to use a condom during sexual intercourse with their wife in comparison to ODUs (odds ratio 0.38, confidence interval 0.18–0.82) (Table 2). There was a statistically significant association between the type of drug user and their age at first sexual intercourse, as well. IDUs were three times more likely to have sexual intercourse at less than 19 years of age than ODUs. There was a statistically significant difference on mean age at first sexual intercourse (t=–3.589, P=0.00) (Table 2). There was a statistically significant association (P<0.05) between the type of drug user and drug use by sexual partner. IDUs were 2.49 times more likely to have a sexual partner who also uses drugs than the ODUs.
Discussion
Though the majority of respondents said that they had heard of HIV, comprehensive knowledge on HIV was poor. Having sexual intercourse with women other than their wife was found among both IDUs and ODUs. More than one in ten drugs users did not use a condom during their last sexual intercourse. More than half of the drug users had sexual intercourse for the first time when they were 19 years of age or below. Given the increased risk of transmission of HIV from drug users to the low-risk general population, findings from this study highlight the importance of targeted prevention intervention for drug users.
Compared to the majority of the drug users who had heard of HIV in this study, the 2007 IBBS done in Pokhara showed 100% of IDUs had heard of HIV. When those who said that they had heard of HIV were asked further about modes of transmission and prevention methods of HIV to assess their comprehensive knowledge on HIV, they could not list all the modes of transmission of HIV. In the 2007 IBBS, 91.1% said abstinence from sexual contact, 95.3% said having only one sexual partner, and 99% said using a condom every time could prevent them from contracting HIV. In total, 86.9% of IDUs were aware of all three.12
The findings on comprehensive knowledge of the respondents on HIV from this study are also similar to that of a previous IBBS.12 In this study, 99% said avoiding unsafe sexual intercourse, 85% said avoiding infected blood, 99% said avoiding used syringes, and 72% said avoiding pregnancy were methods of prevention of HIV. Though most of the respondents knew that avoiding unsafe sexual intercourse and avoiding used syringes were means of HIV prevention, knowledge on the other two methods, ie, avoiding infected blood and avoiding pregnancy in a positive mother, was poor. This might be because prevention programs launching awareness programs for drug users might have focused mainly on two modes of transmission of HIV – the sharing of syringes and unsafe sexual intercourse – because these are the high-risk behaviors that drug users are most likely to practice.
This research reported a high percentage of drug users had sexual intercourse with other women other than their wife. Within the scenario where not all drug users used condoms during their last sexual intercourse, these findings should be looked at carefully. Unprotected sexual intercourse with other women increases the risk of transmission of HIV and other sexually transmitted diseases to the low-risk general population.13 More than half of the drug users had sexual intercourse for the first time when they were 19 years of age or less. This shows early sexual initiation among drug users, and is of particular importance to public health programs. Young drug users are often not targeted in HIV-prevention programs. Harm-reduction programs that intend to reduce the risk of drug use through needle exchange, drug replacement, and awareness need to focus on young drug users as well.
We found drug-using habits (oral or injection) among sexual partners of drug users. Drug users often use drugs while having sexual intercourse; this further elevates the risk of HIV transmission.14 For both IDUs and ODUs, peer pressure was the main motivating factor to initiate drug use. This was followed by curiosity, depression, and education failure. Therefore, partner tracing of IDUs in harm-reduction programs and voluntary counseling should be given importance.
IDUs were less likely (P<0.05) to use condoms during sexual intercourse with their wife in comparison to ODUs. The reasons for IDUs not to use condoms during sexual intercourse with their wife might be that they may not have felt it necessary. IDUs are sharing syringes, having sexual intercourse with other women without using condoms, and also having sexual intercourse with their wives without using condoms, and this might be acting as a bridge in transmitting the HIV virus from the pool of IDUs to wives of IDUs.15,16
IDUs are one of the key affected populations for HIV in Nepal. They have high HIV prevalence compared to other key affected groups.7,8,12 Within this scenario, where not all drug users have heard of HIV, not all have comprehensive information of HIV, and not all are using condoms during sexual intercourse, the risk of HIV transmission among drug users themselves, and transmission to their wives and other female sexual partners or unprotected sexual contacts can increase.
Comprehensive information about HIV needs to be provided to drug users through awareness activities. Promotion of the use of condoms during sexual intercourse with other women and with wives through these awareness activities is necessary. These awareness activities should also target young drug users. Carried out among small populations of drug users, this could limit the generalizability of study findings to drug user populations in other parts of Nepal. Further research could focus on factors affecting transition from non-IDUs to IDUs among a large sample population. With the very limited evidence about knowledge of HIV and sexual behavior of drug users in Nepal, this study will help program planners and policy makers in designing and delivering targeted prevention intervention for drug users. The HIV-prevention program needs to focus on young drug users. Partners of drug users need to be traced, and voluntary counseling offered to drug users.
Conclusion
Though the majority of respondents said that they had heard of HIV, comprehensive knowledge regarding HIV was poor. IDUs were less likely to use a condom during sexual intercourse with their wife. This may act as a bridge in transmitting HIV from the pool of drug users and sex workers to wives of IDUs. Awareness programs and behavior-change communication to alert drug users to the risks of sharing syringes need to be conducted, in addition to promoting the use of condoms during sexual intercourse with other women and with wives.
Acknowledgment
The authors express their thanks to all participants in this research, and the community mobilizers and outreach educators of Naulo Ghumti who helped us with data collection. Also, we would like especially to thank Mr Amit Dhungel, Dr Laxmi Bilas Acharya, Mr Mahesh Shrestha, and Mr Dipak Karki.
Disclosure
The authors report no conflicts of interest in this work.
References
Jutkowitz JM, Spielmann H, Koehler U, Lohani J, Pande A. Drug use in Nepal: the view from the street. Subst Use Misuse. 1997;32:987–1004. | |
Shrestha NM. Alcohol and drug abuse in Nepal. Br J Addict. 1992;87:1241–1248. | |
Chatterjee A, Uprety I, Chapagain M, Kafle K. Drug abuse in Nepal, a rapid assessment study. 1996. Available from: http://www.unodc.org/unodc/en/data-and-analysis/bulletin/bulletin_1996-01-01_1_page003.html. Accessed December 13, 2013. | |
United Nations Office on Drugs and Crime. 2008 World Drug Report. Vienna: UNODC; 2008. | |
Mathers BM, Degenhardt L, Phillips B, et al. Global epidemiology of injecting drug use and HIV among people who inject drugs: a systematic review. Lancet. 2008;372:1733–1745. | |
Arasteh K, Jarlais DC. Injecting drug use, HIV and what to do about it. Lancet. 2008;372:1709–1710. | |
National Centre for AIDS and STD Control. National Estimates of HIV Infections: 2007 Nepal. Kathmandu: NCASC; 2007. | |
Henderson LA, Vlahov D, Celentano DD, Strathdee SA. Readiness for cessation of drug use among recent attenders and nonattenders of a needle exchange program. J Acquir Immune Defic Syndr. 2003;32:229–237. | |
Central Bureau of Statistics (CBS). Area and population. National Population and Housing Census 2011. Available from: http://cbs.gov.np/wp-content/uploads/2012/11/National%20Report.pdf. Accessed August 7, 2013. | |
Family Health International. Integrated Biological and Behavioral Surveillance Survey (IBBS) among injecting drug users in Pokhara Valley: round IV – 2009. 2009. Available from: http://www.fhi360.org/sites/default/files/media/documents/Integrated%20Biological%20and%20Behavioral%20Surveillance%20Survey%20%28IBBS%29%20among%20Injecting%20Drug%20Users%20in%20Pokhara%20Valley%20%28Round%20IV%202009%29.pdf. Accessed December 13, 2013. | |
Naulo Ghumti [website on the Internet]. Available from: http://www.ngn.org.np. Accessed October 23, 2013. | |
Family Health International. Integrated Bio-behavioral Survey (IBBS) among injecting drug users in Pokhara Valley – 2007. 2008. Available from: http://ncasc.gov.np/ncasc/Reports/Integrated%20Bio-Behavioral%20Surveys-%20Nepal/IDUs/Pokhara/2007/Full%20Report_IBBS%20IDU%20POKHARA%202007%20Final%20edited.pdf. Accessed December 13, 2013. | |
Mishra SR, Khanal V. Sexual behaviors among men who have sex with men: a quantitative cross sectional study in Kathmandu Valley, Nepal. HIV/AIDS (Auckl). 2013;5:81–88. | |
Cheng WS, Garfein RS, Semple SJ, Strathdee SA, Zians JK, Patterson TL. Increased drug use and STI risk with injection drug use among HIV-seronegative heterosexual methamphetamine users. J Psychoactive Drugs. 2010;42:11–18. | |
Wodak A, Ali R, Farrell M. HIV in injecting drug users in Asian countries. BMJ. 2004;329:697–698. | |
Toussova O, Shcherbakova I, Volkova G, Niccolai L, Heimer R, Kozlov A. Potential bridges of heterosexual HIV transmission from drug users to the general population in St. Petersburg, Russia: is it easy to be a young female? J Urban Health. 2009;86 Suppl 1:121–130. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.