Back to Journals » Clinical Ophthalmology » Volume 13
Keratoconus Screening Among Myopic Children
Authors Omar IAN
Received 1 August 2019
Accepted for publication 12 September 2019
Published 25 September 2019 Volume 2019:13 Pages 1909—1912
DOI https://doi.org/10.2147/OPTH.S225326
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ismail Ahmed Nagib Omar
Ophthalmology Department, Faculty of Medicine, Minia University, El-Minya, Egypt
Correspondence: Ismail Ahmed Nagib Omar
Ophthalmology Department, Faculty of Medicine, Minia University, El-Minya 61111, Egypt
Tel +20 100 255 4116
Email [email protected]
Aim: To assess the topographic corneal changes and the incidence of keratoconus among children with high myopia.
Settings: It is a prospective study, in which 174 eyes of children with high myopia were studied in the period between August 2015 and June 2018.
Methods: All patients were examined to assess the refractive error and corneal examination using Scheimpflug camera to evaluate different corneal parameters.
Results: Studied children aged between 6 and 14 years (11.05±1.98). Males represented 54% of the cases (n=94). The mean spherical error was −7.75±2.97 ranging from −6 to −13.50D. The mean cylindrical error was −4.12±1.78D (−1 to −8). Regarding corneal examination, data recorded were those about maximum K reading (kmax), thinnest location, highest anterior and posterior elevation in 4mm zone, and higher-order corneal aberrations. Analysis of the obtained data revealed 16 eyes (9.2%) with keratoconus. These eyes were considered as a separate group and compared with the remaining eyes. There was significant difference in kmax (p= 0.03), anterior elevation, and posterior elevation (p=0.01 for both). Regarding myopia or astigmatism, there were no significant differences when compared with normal eyes. But high myopia with low astigmatism were found in five eyes of them (31.2%). The main statistically different aberrations were vertical coma (−2.04±0.99) (p=0.01) and spherical aberrations (−0.9±0.78) (p=0.02). Regarding gender, there were 11 eyes in boys (68.7%), and this was statistically significant (p=0.01). Vernal keratoconjunctivitis with frequent eye rubbing was found in 6 eyes (37.5%).
Conclusion: Children with high myopia irrespective of the degree of astigmatism may have corneal abnormalities which are more pronounced in cases with vernal keratoconjunctivitis. Corneal examination should be performed for highly myopic children to detect any corneal abnormality and to treat it as early as possible.
Keywords: myopia, keratoconus, children
Introduction
Myopia has an important concern in children as it may affect their visual development. In contrast to adults, corneal abnormalities in children are usually discovered late, after the progression of the disease because of late diagnosis.1
High myopia is frequently reported among Egyptian children and it represents a health problem as it affects school achievement of affected children when not properly managed.2
The new corneal examination techniques gave us more detailed data about corneal abnormalities and hence early management. Scheimpflug camera as an examination tool increased our ability to investigate corneal curvature, front and back elevation changes, multiple point pachymetry, and many other parameters and indices which added to our knowledge about the examined cornea.3
Keratoconus is a progressive, frequently asymmetric, non-inflammatory corneal thinning disorder characterized by changes in the structure and organization of corneal collagen.4 Formerly, keratoconus was believed as a disease of adolescence, but nowadays it is being diagnosed more commonly.5
In paediatric patients, keratoconus is often more advanced at the time of diagnosis and the progression of the disease is more frequent and has a very rapid course.6
Therefore, early detection of the disease is necessary to prevent severe visual impairment and decreases the need for corneal transplantation in children.7
Often keratoconus is an isolated disease; however, it may be associated with other diseases, the most frequent of them are vernal keratoconjunctivitis, atopy, Down syndrome, and retinitis pigmentosa.8
The aim of this study was to assess the topographic corneal changes and the incidence of keratoconus among children with high myopia in an attempt to highlight the importance of corneal examination among those children.
Subjects And Methods
This study was a prospective study which was conducted on children with high myopia above 6 D who were studied in the period between August 2015 and June 2018. The study design was explained to the parents or their legal guardians and all of them provided written informed consent. The study was designed respecting the expected ethical aspects. It was performed according to the Declaration of Helsinki 1964, as revised in 2008 and approved by the Institutional Review Board and Medical Ethics Committee of Minia University Hospital. The study registration number is UMIN000037273.
Inclusion criteria were as follows: age less than 14 years old, clear cornea, clear lens, and myopia more than 6D with or without astigmatism. Exclusion criteria were corneal opacity, cataract, previous ocular surgery, previous trauma, recent use of contact lenses, any ocular abnormalities which may affect the corneal curvature like upper lid ptosis, and retinal or systemic diseases which may be associated with keratoconus.
For each subject included in the study, complete history was taken focusing on allergic conjunctivitis or frequent eye rubbing and family history of keratoconus. Full ophthalmic examination was performed using slit-lamp bio-microscopy, cycloplegic refraction using autorefractometer, and fundoscopy.
The corneal surfaces were then examined using the Pentacam rotating Scheimpflug imaging system (Oculus Optikgerate GmbH, Wetzlar, Germany). The items studied were sagittal corneal curvature, thickness of the thinnest location, anterior maximal elevation (more than 15 µm considered abnormal within 4 mm zone), and posterior maximal elevation (more than 20 µm considered abnormal within 4 mm zone) on best fit sphere (BFS) 9 mm. Higher-order aberrations were studied too. Three readings were collected for each examined eye, and the best quality reading with good centration was recorded.
Diagnosis of keratoconus was based on slit lamp findings and/or corneal images obtained by Pentacam. Then, participants were grouped according to having keratoconus or not, where eyes with keratoconus were considered as cases and remaining normal eyes were considered as controls.
Statistical Analysis
All data were analysed using SPSS (Statistical Package for Social Sciences) software version 20 to describe the demographic and clinical characteristics, and variables were summarized using means, standard deviations (SD), and ranges. Categorical variables were summarized using frequencies and percentages. Probability (p) was considered significant if < 0.05.
Results
The total eyes included in this study were 174 eyes from 87 children with high myopia. They aged between 6 and 14 years old with a mean of 11.05±1.98 years. Male gender represented 54% and 46% were female.
Table 1 shows the data studied for all children participated in the study. All patients had myopia with varying grades and the same for astigmatism. Regarding sagittal curvature, the maximum k reading was recorded (kmax). The recorded pachymetry was the thinnest location which was less than 500 µm in 21 (12.09%) eyes. Regarding elevation either anterior or posterior, it was recorded from the highest reading in the 4mm zone which represented the highest elevation in this zone. Also, higher-order aberrations were studied, and the recoded data were those concerning spherical aberrations, horizontal coma, and vertical coma as they are frequently affected with keratoconus.
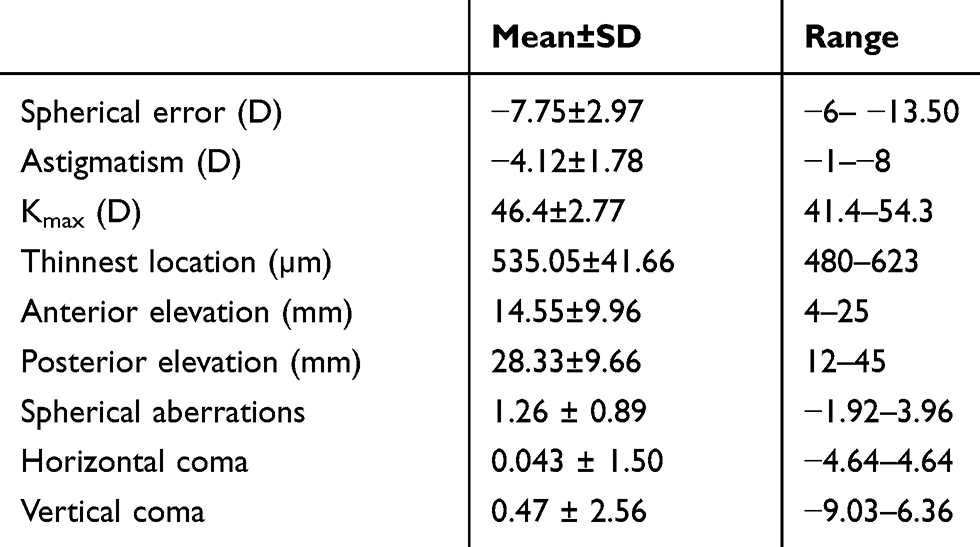 |
Table 1 Data Of All Studied Patients |
Analysis of the obtained data revealed that keratoconus was diagnosed with variable grades in 16 eyes (9.2%) of the studied eyes. These eyes were further studied for their topographic and refractive characteristics as shown in Table 2. When compared with the remaining topographically normal eyes (158 eyes) which were considered as controls, there was a significant difference regarding maximum k reading (p= 0.03), anterior and posterior elevation (p=0.01 for both). Regarding myopia or astigmatism, there were no significant differences when compared with normal eyes. But high myopia with low astigmatism were found in five eyes of them (31.2%).
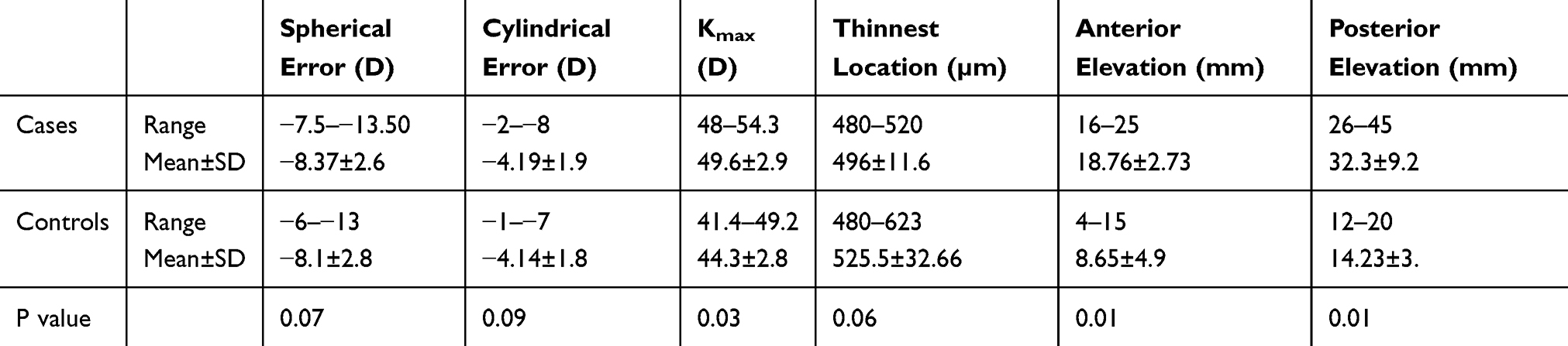 |
Table 2 Topographic Parameters And Refractive Errors Of Keratoconus Children Versus Controls |
The main statistically different aberrations were vertical coma (−2.04±0.99) (p=0.01) and spherical aberrations (−0.9±0.78) (p=0.02). Regarding gender, there were 11 eyes in boys (68.7%), and this was statistically significant (p=0.01). Vernal keratoconjunctivitis with frequent eye rubbing was found in 6 eyes (37.5%). And positive family history of keratoconus was found in the eyes of two patients (12.9%), but no family history of keratoconus was reported among patients with normal eyes.
Discussion
This study was conducted in children with high myopia to investigate corneal abnormalities among them and hence early detection of keratoconus. This was to avoid late diagnosis and management of corneal ectasia.
In a study done in Riyadh (Saudi Arabia), they found keratoconus prevalence of 4.79% among pediatric patients.9 In another study carried out on 92 Lebanese students, 4.4% prevalence of keratoconus was found among them.10
The current study showed more than double these percentages which may be attributed to focusing on only highly myopic children in the present study, while former studies collected data from children regardless of their refractive state.
Keratoconus was found to be more frequent among male cases which was also previously reported by Léoni-Mesplié S and her colleagues.6,11
Vernal keratoconjunctivitis was reported in 37.5% of the keratoconus eyes and they had the most severe form of corneal abnormalities. The association between allergic conjunctivitis and KC was controversial with studies reporting an association ranging from 7% to 35%, while others did not show any relationship. However, most studies had proven that there was a definite association between allergy with eye rubbing and keratoconus.12–15
However, in 2016, Caputo and his colleagues reported lower incidences of keratoconus with vernal keratoconjunctivitis in the paediatric population of 0.61%, as compared to previously documented.16 Their results were dissimilar to our results and this could be attributed to large sample size, different age groups, different ethnic groups and different refractive errors in contrast to our study which targeted myopic children.
Keratoconus results in visual impairment by inducing myopia and astigmatism and decreases the quality of life of the affected individuals.17 One third of the diagnosed keratoconus cases in the current study had high myopia but with low astigmatism. That is why high myopia alone can be considered as an alarming sign for further corneal examination to exclude any corneal abnormalities.
Corneal thinning is a common finding in corneas with keratoconus.18 In this study, the thickness of the thinnest location was not statistically different between eyes with keratoconus and normal eyes. This can be explained that corneal thinning takes some time to develop and that is why it was not evident in children.
Corneal distortion and scarring induced by keratoconus affect image quality by inducing higher-order aberrations. In addition, corneal thinning causes marked shape changes and hence higher-order aberration which is different from that found in normal eyes.19
On measuring higher-order aberrations in the current study, it was found that vertical coma and spherical aberrations were significantly higher among keratoconus eyes, but Bühren et al in 2007 found vertical coma was the only aberration affected.20
It can be concluded that children with high myopia irrespective of the degree of astigmatism may have corneal abnormalities which are more pronounced in cases with vernal keratoconjunctivitis. Corneal examination should be performed for high myopic children to detect any corneal abnormality and to treat it as early as possible.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Reeves SW, Stinnett S, Adelman RA, Afshari NA. Risk factors for progression to penetrating keratoplasty in patients with keratoconus. Am J Ophthalmol. 2005;140(4):607–611. doi:10.1016/j.ajo.2005.05.029
2. El-Bayoumy BM, Saad A, Choudhury AH. Prevalence of refractive error and low vision among schoolchildren in Cairo. East Mediterr Health J. 2007;13:575–579.
3. Vazquez PR, Delrivo M, Bonthoux FF, Pfortner T, Chiaradia P, Galletti J. Subclinical keratoconus detection based on Pentacam Scheimpflug tomography indices. Invest Ophthalmol Vis Sci. 2013;54(15):534.
4. Vazirani J, Basu S. Keratoconus: current perspectives. Clin Ophthalmol. 2013;7:2019–2030. doi:10.2147/OPTH.S50119
5. El Rami H, Chelala E, Dirani A, et al. An update on the safety and efficacy of corneal collagen cross-linking in pediatric keratoconus. Biomed Res Int. 2015;2015:257927.
6. Leoni-Mesplie S, Mortemosque B, Touboul D, et al. Scalability and severity of keratoconus in children. Am J Ophthalmol. 2012;154:156–162. doi:10.1016/j.ajo.2012.03.014
7. McAnena L, O’Keefe M. Corneal collagen crosslinking in children with keratoconus. J Aapos. 2015;19:228–232. doi:10.1016/j.jaapos.2015.02.010
8. Gordon Shaag A, Millodot M, Shneor E, et al. The genetic and environmental factors for keratoconus. Biomed Res Int. 2015;2015:795738.
9. Torres Netto EA, Al-Otaibi WM, Hafezi NL, et al. Prevalence of keratoconus in paediatric patients in Riyadh, Saudi Arabia. Br J Ophthalmol. 2018;102(10):1436–1441. doi:10.1136/bjophthalmol-2017-311391
10. Wakend N, Fayad AM, Fadlallah A, et al. Keratoconus screening in Lebanese students’ population. J Fr Ophthalmol. 2012;35(1):23–29.
11. Godefrooij DA, de Wit GA, Uiterwaal CS, Imhof SM, Wisse RPL. Age-specific incidence and prevalence of keratoconus: a nationwide registration study. Am J Ophthalmol. 2017;175:169–172. doi:10.1016/j.ajo.2016.12.015
12. Krachmer JH, Feder RS, Belin MW. Keratoconus and related noninflammatory corneal thinning disorders. Surv Ophthalmol. 1984;28:293–322.
13. Yeniad B, Alparslan N, Akarcay K. Eye rubbing as an apparent cause of recurrent keratoconus. Cornea. 2009;28(4):477–479. doi:10.1097/ICO.0b013e31818d37fa
14. Lapid-Gortzak R, Rosen S, Weitzman S, Lifshitz T. Videokeratography findings in children with vernal keratoconjunctivitis versus those of healthy children. Ophthalmology. 2002;109(11):2018–2023. doi:10.1016/s0161-6420(02)01218-6
15. Bawazeer AM, Hodge WG, Lorimer B. Atopy and keratoconus: a multivariate analysis. Br J Ophthalmol. 2000;84:834–836. doi:10.1136/bjo.84.8.834
16. Caputo R, Versaci F, Pucci N, et al. Very low prevalence of keratoconus in a large series of vernal keratoconjunctivitis patients. Am J Ophthalmol. 2016;172:64–71. doi:10.1016/j.ajo.2016.09.009
17. Aydin Kurna S, Altun A, Gencaga T, Akkaya S, Sengor T. Vision related quality of life in patients with keratoconus. J Ophthalmol. 2014;2014:7. doi:10.1155/2014/694542
18. Brautaset R, Nilsson M, Miller W, et al. Central and peripheral corneal thinning in keratoconus. Cornea. 2013;32(3):257–261.
19. Jinabhai A, Radhakrishnan H, o’donnell C. Higher-order aberrations in keratoconus: a review. Optometry Pract. 2009;10:141–160.
20. Bühren J, Kühne C, Kohnen T. Defining subclinical keratoconus using corneal first-surface higher-order aberrations. Am J Ophthalmol. 2007;143:381–389. doi:10.1016/j.ajo.2006.11.062
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.