Back to Journals » International Medical Case Reports Journal » Volume 19
Keratinizing Penile Squamous Cell Carcinoma Arising from Chronic Balanoposthitis in an Uncircumcised Diabetic Man: A Case Report from a Rural Tertiary Hospital in Uganda
Authors Chris-Uchendu HC ![]() , Charles T, Nek AJ
, Charles T, Nek AJ ![]() , Olwit G
, Olwit G ![]() , Okecho S
, Okecho S ![]() , Rhonah K, Kaheru SA
, Rhonah K, Kaheru SA ![]()
Received 10 April 2026
Accepted for publication 12 June 2026
Published 15 June 2026 Volume 2026:19 615878
DOI https://doi.org/10.2147/IMCRJ.S615878
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Hans Chinomso Chris-Uchendu,1 Tumwesige Charles,1 Arthur Jonathan Nek,1 Gerald Olwit,2 Stanley Okecho,1 Kwikiriza Rhonah,1 Sean Arthur Kaheru1
1Department of Surgery, School of Medicine, Kabale University, Kabale, Uganda; 2Department of Internal Medicine, School of Medicine, Kabale University, Kabale, Uganda
Correspondence: Hans Chinomso Chris-Uchendu, Department of Surgery, School of Medicine, Kabale University, P.O. Box 317, Kabale, Uganda, Tel +256 766607269, Email [email protected]
Background: Penile squamous cell carcinoma (SCC) primarily develops through two distinct etiopathogenic routes: human papillomavirus (HPV)-mediated and non-viral, chronic inflammation-driven pathways. In low-resource settings, long-standing phimosis and recurrent balanoposthitis present significant public health challenges that accelerate tissue transformation.
Case Presentation: We report a case of an uncircumcised 75-year-old African man presenting to a tertiary facility in Southwestern Uganda with a 2-year history of a progressive, painful, exophytic penile mass associated with chronic balanoposthitis and a 7-year history of Type 2 Diabetes Mellitus. Clinical examination revealed a 4.0 cm × 5.0 cm ulcerated, necrotic tumor involving the glans penis and distal shaft, along with bilateral 1.5 cm palpable inguinal lymph nodes. Due to resource constraints at our center, molecular screening (p16 immunohistochemistry and HPV DNA PCR) and staging node biopsies were unavailable. Histopathological examination of the partial penectomy specimen confirmed a well-differentiated, keratinizing squamous cell carcinoma (pT2 cN0 M0). The patient experienced an uneventful postoperative recovery and was transitioned to a structured clinical surveillance program.
Discussion: This case highlights the role of chronic balanoposthitis, diabetes mellitus, and poor foreskin ventilation in promoting a sustained inflammatory microenvironment that may predispose to malignant transformation of penile epithelium. It underscores the diagnostic challenge posed by inflammatory penile lesions that mimic benign disease and the consequences of delayed medical evaluation.
Conclusion: This case provides a descriptive illustration of penile carcinoma emerging in a background of chronic inflammation, highlighting the clinical realities of managing advanced disease in a resource-limited environment. It underscores the critical need for localized screening, early surgical intervention for phimosis, and improved access to molecular diagnostics in sub-Saharan Africa.
Keywords: penile squamous cell carcinoma, chronic balanoposthitis, penile cancer, diabetes mellitus, chronic inflammation
Introduction
Penile cancer is a rare but aggressive malignancy, accounting for less than 1% of male cancers in high-income nations, yet it represents a disproportionate public health burden in low- and middle-income regions (LMICs) across Africa, Asia, and South America.1–3 Squamous cell carcinoma (SCC) comprises over 95% of these malignancies, typically originating from the glans penis, prepuce, or coronal sulcus.2,4 Despite its relative rarity, penile SCC carries profound physical and psychosexual morbidity, particularly when diagnostic delays necessitate radical surgical intervention.2,4
The etiology of penile SCC is multifactorial, historically categorized into HPV-associated and HPV-independent pathways. Established risk factors include a lack of neonatal circumcision, poor genital hygiene, phimosis, tobacco use, and immunosuppression.1,2,5 Among these, chronic balanoposthitis, a persistent inflammatory insult to the glans and foreskin, is increasingly recognized as a critical precursor in the HPV-independent inflammatory carcinogenic pathway.2,4
Chronic balanoposthitis is fueled by recurrent tissue injury secondary to smegma accumulation, tight phimosis, and systemic metabolic derangements, most notably Diabetes Mellitus. This persistent inflammation establishes a pro-tumorigenic microenvironment characterized by chronic oxidative stress and dysregulated cytokine release.6,7 The resulting cycles of epithelial damage and aberrant repair promote genomic instability and DNA damage, bypassing viral oncogenic mechanisms to drive malignant transformation.6–8 Phimosis further exacerbates this “smoldering” milieu by facilitating bacterial colonization and preventing mechanical clearance of carcinogens.5,9
Clinically, the transition from chronic inflammation to invasive SCC is often insidious, as early-stage malignant lesions frequently mimic benign dermatoses. This diagnostic overlap is a primary driver of late-stage presentation in resource-limited settings, where patients often seek care only after the onset of ulceration, foul discharge, or mechanical urethral obstruction.10,11 While partial penectomy remains the oncological standard for localized disease, the requirement for such radical surgery underscores a systemic failure in the early recognition of pre-malignant states.12,13
In sub-Saharan Africa, penile cancer presents a distinct epidemiological profile, often linked to low neonatal circumcision rates, high visual-diagnostic delays, and limited access to specialized urological care.1,2 Regional data from East Africa indicates that squamous cell carcinoma remains the dominant histological subtype, frequently presenting at advanced stages (T2 or higher) due to socioeconomic barriers and initial reliance on traditional medicine.2,14 Reporting cases from regional tertiary settings like Southwestern Uganda is essential to document the localized clinical burdens and highlight structural gaps in diagnostic infrastructure.2,14
This report presents a descriptive case of keratinizing penile SCC emerging within a background of chronic balanoposthitis in an uncircumcised patient with a 7-year history of Type 2 Diabetes Mellitus. Due to systemic resource limitations in our clinical setting, molecular profiling, specifically p16 immunohistochemistry, HPV DNA PCR testing, and glycated hemoglobin (HbA1c) measurements, could not be performed. While a definitive non-viral carcinogenic pathway cannot be molecularly confirmed, the case provides a highly instructive clinical illustration of long-standing, inflammation-driven epithelial transformation within a low-resource environment.
Case Presentation
Presenting Complaint
The patient came with complaints of “For the last 12 hours, I haven’t been able to pass urine at all. I also have a sore on my private part that has been growing for about 10 months; it smells bad and bleeds easily”.
History of Present Complaint
The patient is a 75‑year‑old man who reported that 10 months earlier he noticed a small red patch on the head of his penis and foreskin. The area gradually became a pale, yellowish ulcer that never healed. Over the last 4 months his urinary stream had become noticeably weaker, he had to push to start and dribbled after finishing, and he felt that his bladder never emptied completely. Twelve hours before arrival he became completely unable to pass urine. The sore had been constantly moist, discharged a foul‑smelling yellow fluid, and bled when touched. He also described itching and swelling of the penis and had noticed lumps in both groins. He denied any pain from the ulcer initially, although there had been a brief period of burning with intercourse that later subsided even as the ulcer grew. He had experienced repeated episodes of foreskin redness, moisture, and cheesy material (smegma) behind a tight foreskin for many years.
Past Medical and Surgical History
The patient’s medical history is significant for Type 2 Diabetes Mellitus, managed for seven years. He had been taking metformin monotherapy for the entire duration, though recent glycated haemoglobin levels were unavailable. He is HIV-seronegative and has no history of hypertension or systemic malignancy.
Sexual, Social, and Family History
The patient initiated sexual activity in early adulthood and reported multiple lifetime female partners with inconsistent barrier protection. He denied any history of syphilis, genital warts, or HPV-related pathologies. Despite painful ejaculation, erectile function remained preserved until surgical intervention.
Social history was negative for tobacco use but positive for moderate weekly alcohol consumption. Environmental risk factors included a lack of neonatal circumcision and infrequent hygiene of the preputial sac. Family history was non-contributory for genitourinary malignancies or hereditary syndromes.
Physical Examination on Admission
General
Alert, afebrile, BP 128/74 mmHg, HR 72 bpm, SpO2 92% on room air. No pallor, icterus, or peripheral oedema.
Abdomen
Soft, non‑tender; a distended, dull bladder was percussed to 4 cm above the pubic symphysis.
Genitalia
Uncircumcised phallus with a completely non‑retractable, oedematous foreskin (acquired phimosis). A foul‑smelling, purulent discharge could be expressed from the preputial opening. The glans could not be visualised.
Post-Dorsal Slit Examination
Exposure revealed a 3×2.5 cm ulcerated, fungating mass with everted, indurated edges and a necrotic base involving the entire glans and inner prepuce. The mass partially occluded the external urethral meatus.
Lymphatic
Bilateral, firm, mobile, slightly tender inguinal lymph nodes (1.5 cm) in diameter were palpable. The bilateral palpable inguinal lymph nodes (1.5 cm) were clinically assessed as reactive hyperplasia secondary to the severe, chronic inflammation and bacterial superinfection of the foul-smelling, necrotic primary penile tumor. Due to severe local resource constraints and the lack of immediate cytopathology infrastructure at our center, fine-needle aspiration cytology (FNAC) or staging inguinal lymphadenectomy was not performed at admission. Advanced imaging and node sampling were deferred in favor of immediate primary tumor control, representing a necessary deviation from international guidelines (EAU/NCCN) dictated by our low-resource setting. The nodal status was therefore classified strictly under clinical staging as cN0.
Examination After Emergency Dorsal Slit
Release of the phimotic band exposed an ulcerated, fungating mass involving the entire glans and the inner aspect of the prepuce. The lesion measured approximately 3×2.5 cm, had heaped‑up, indurated, everted edges, and a pale‑yellow necrotic base. The external urethral meatus was partially covered by tumour, making catheterisation impossible. The dorsal slit wound was clean. No scrotal abnormality was found (See Figure 1).
 |
Figure 1 Gross clinical appearance of the penis after an emergency dorsal slit, showing an ulcerated, exophytic mass with irregular, indurated margins involving the glans penis and distal shaft. The image illustrates how preputial constriction can obscure early penile pathology and contribute to delayed presentation. |
Differential Diagnosis
At presentation, the differential diagnosis for this massive, ulcerated penile lesion included Buschke-Löwenstein tumor (giant condyloma acuminatum), syphilitic gumma, chancroid, and deep fungal infections. Giant condyloma acuminatum was considered due to the extensive, exophytic, cauliflower-like growth pattern, but it typically lacks the destructive, deep infiltrative invasion and extensive central necrosis seen in this patient. Granulomatous venereal diseases, such as tertiary syphilis (gumma) or chronic chancroid ulcers, were effectively excluded based on the negative serological screens for Treponema pallidum (VDRL/TPHA), the absence of painless induration typical of primary lesions, and the poor clinical response to initial empirical broad-spectrum antibiotic therapies. Definitive differentiation was established via histopathological evaluation of the incisional wedge biopsy, which demonstrated clear cytological features of malignant epithelial transformation, including cellular atypia, prominent mitotic figures, and infiltrating keratin pearls, ruling out benign infectious or hyperplastic mimickers.
Investigations
Initial laboratory evaluation revealed largely normal hematologic and biochemical parameters, with significant elevations in serum PSA and GGT, alongside hypercholesterolemia (Table 1).
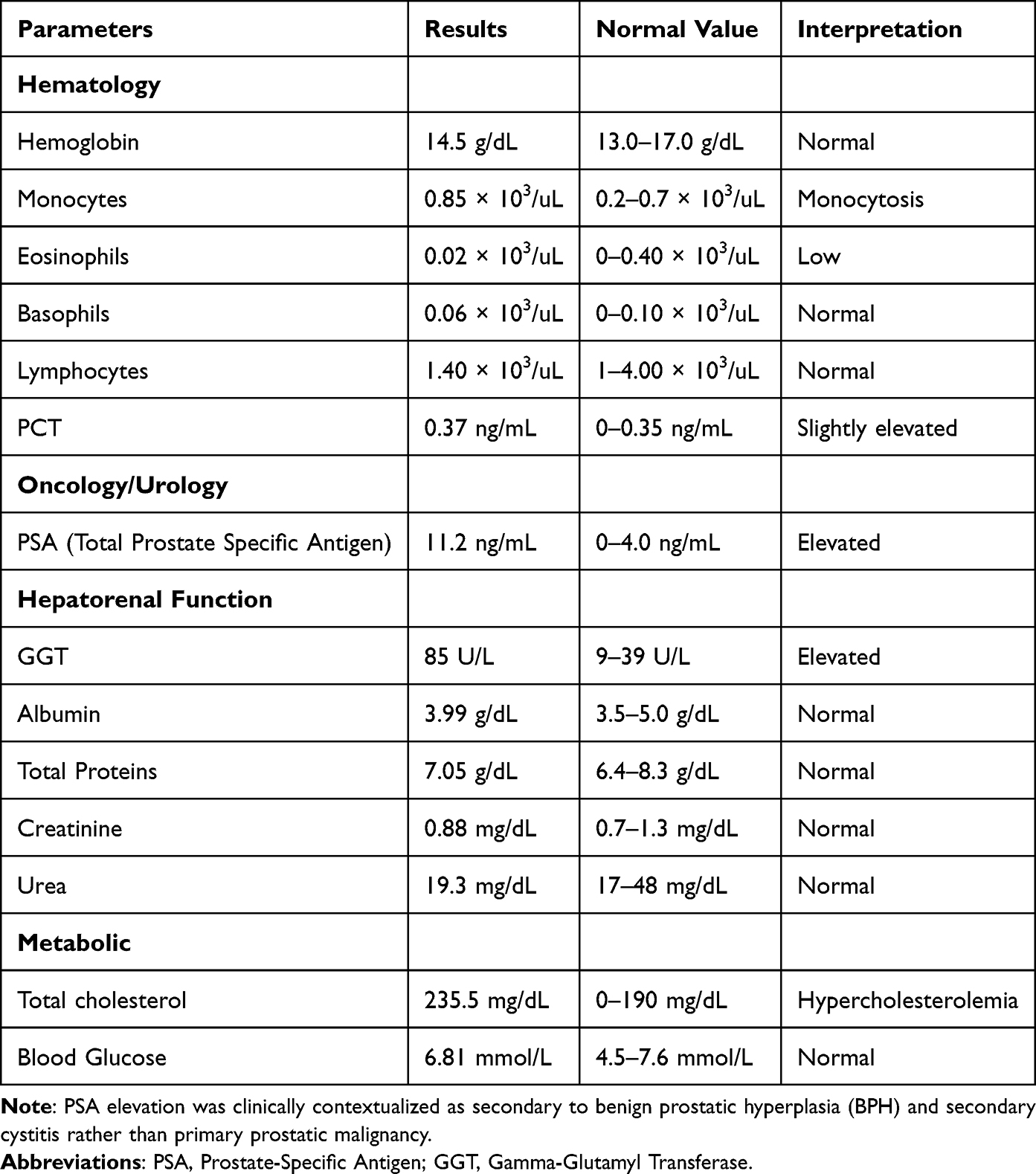 |
Table 1 Admission Laboratory Investigations: Hematological, Biochemical, and Metabolic Profile |
This isolated random blood glucose reading, though within the normal range, does not reflect long‑term glycaemic control, for which glycated haemoglobin was unavailable.
Imaging
Ultrasonographic imaging of the abdomen and pelvis confirmed prostatic enlargement and secondary cystitis, also with bladder outlet obstruction (Table 2).
 |
Table 2 Radiographic and Ultrasonographic Findings |
Histopathological analysis of the penile biopsy and resected specimen confirmed squamous cell carcinoma of the penis, arising in the background of chronic balanoposthitis. The tumor was as N0, M0 (pT2 cN0 M0 (Stage II)) (Figure 2). No inguinal lymph node dissection was performed, and no metastatic disease was identified.
 |
Figure 2 Intraoperative photograph showing the surgical excision of a biopsy specimen from the inner surface of the prepuce. This critical diagnostic step provided the representative tissue necessary to establish the definitive histopathological diagnosis of penile malignancy. |
Given the diagnostic confirmation of invasive squamous cell carcinoma against a background of chronic, obstructive preputial stenosis and elevated inflammatory markers (Table 1), conservative management was deemed insufficient. Consequently, the patient was optimized for definitive surgical intervention to address both the oncological pathology and the underlying metabolic risks associated with his diabetic state.
Treatment and Outcome
Initial urological management was necessitated by failed urethral catheterization due to meatal obstruction. Emergency intervention involved a dorsal slit and a localized meatotomy to relieve the AUR, during which extensive involvement of the glans penis was visualized. A wedge biopsy of the preputial lesion was performed simultaneously. Histopathological analysis subsequently confirmed invasive squamous cell carcinoma, prompting a partial penectomy as a definitive management three weeks later.
Intraoperative examination revealed extensive ulcerative and infiltrative lesions on the inner surface of the prepuce that extended toward and partially obstructed the external urethral meatus (Figure 3). Deep corporal invasion beyond the glans was confirmed, consistent with clinical stage T2 disease (Figure 4). Negative surgical margins were verified by frozen section, ensuring oncological radicality while preserving sufficient urethral length for standing micturition.
 |
Figure 3 Clinical photograph of the retracted prepuce revealing multiple ulcerated, proliferative lesions with indurated margins overlying the glans penis. The lesions can be seen extending toward and partially occluding the external urethral meatus, illustrating the mechanical mechanism behind the patient’s urinary obstruction. |
 |
Figure 4 Intraoperative photograph showing extensive infiltrative ulceration extending from the inner prepuce into the glans penis and proximal shaft. This documented deep extension dictated the necessity of a definitive partial penectomy to achieve adequate oncological control. |
Postoperative histopathology confirmed a keratinizing squamous cell carcinoma, staged as N0, M0 (pT2 cN0 M0 (Stage II)), with clear margins. Perioperative care comprised intravenous fluids, prophylactic ceftriaxone, analgesia with paracetamol and tramadol, and glycaemic monitoring. A Foley catheter remained in situ for four weeks. The patient reported minor bleeding on the first postoperative day only, and no subsequent wound complications occurred.
At four‑week follow‑up, the surgical site had healed by primary intention (Figure 5). Following catheter removal, the patient voided normally without leakage or dribbling. Pain had resolved, and there was no discharge or clinical evidence of infection. No adjuvant chemotherapy or radiotherapy was recommended. The patient remained compliant with follow‑up and expressed concern regarding long‑term sexual function and cancer recurrence.
 |
Figure 5 Postoperative clinical photograph four weeks following partial penectomy, showing satisfactory healing and complete epithelization of the remaining penile shaft. The reconstructed urethral opening is patent with no early signs of wound complications. |
Discussion
Penile squamous cell carcinoma (SCC) is an uncommon malignancy globally but remains a significant health burden in low- and middle-income settings, where delayed presentation, limited awareness, and persistent inflammatory genital conditions are prevalent.2,4 This case highlights the malignant transformation of chronic balanoposthitis into invasive penile SCC, complicated by progressive urethral obstruction, and illustrates several well-established but under-recognized pathogenic pathways linking chronic inflammation, metabolic disease, local microenvironmental factors, and carcinogenesis.
Chronic Balanoposthitis as a Carcinogenic Milieu
Chronic balanoposthitis is increasingly recognized as a premalignant inflammatory condition, particularly when prolonged and inadequately treated. Persistent inflammation leads to repeated epithelial injury and regeneration, creating a microenvironment conducive to malignant transformation. Inflammatory infiltrates generate reactive oxygen and nitrogen species, which induce DNA damage, genomic instability, and epigenetic alterations in squamous epithelial cells. Over time, these changes may promote dysplasia and eventual progression to invasive SCC.6,7
Role of Poor Foreskin Ventilation and Uncircumcised Status
The patient’s uncircumcised status likely played a significant role in disease pathogenesis. An intact foreskin can create a closed, warm, and humid subpreputial environment, impairing ventilation and facilitating microbial overgrowth. Such conditions promote chronic irritation, smegma retention, and persistent inflammation of the glans and inner prepuce.5,9
Epidemiological studies have consistently demonstrated a lower incidence of penile SCC among circumcised males, particularly when circumcision is performed in infancy or early childhood.15
In uncircumcised individuals, long-standing phimosis traps desquamated epithelial cells, skin oils, and moisture, creating an enclosed environment prone to recurrent bacterial superinfections.5,9 Modern oncological consensus has discarded the historical notion that smegma acts as a direct chemical carcinogen.5 Instead, current evidence indicates that smegma retention serves as a mechanical lattice that promotes continuous, long-term irritation of the glans and inner prepuce.9 This constant physical microtrauma and subsequent chronic balanoposthitis trigger cellular proliferation pathways, setting the stage for malignant epithelial transformation over several decades.5,9
Diabetes Mellitus and Impaired Local Immune Defense
Diabetes mellitus is an important systemic risk modifier in penile carcinogenesis. Chronic hyperglycemia impairs both innate and adaptive immune responses, including neutrophil chemotaxis, phagocytosis, and complement activation, leading to increased susceptibility to infections and delayed resolution of inflammation, a phenomenon documented across multiple immune cell types in diabetic individuals.16–18 Moreover, urogenital infections such as balanitis and balanoposthitis occur more frequently in diabetic patients compared with non-diabetic cohorts, with a high proportion of balanoposthitis patients found to have underlying diabetes mellitus. These immune and inflammatory alterations contribute to recurrent and refractory genital inflammation, providing a pro-carcinogenic microenvironment in susceptible individuals.10,11,19
At the molecular level, chronic hyperglycemia in diabetes is associated with increased oxidative stress, which generates reactive oxygen species that damage DNA and disrupt normal repair mechanisms, thereby contributing to carcinogenesis.7,20 Hyperglycemia also induces microvascular and endothelial dysfunction, resulting in impaired tissue perfusion and persistent inflammation, further potentiating a pro-carcinogenic microenvironment.20,21 Additionally, diabetes is linked to multiple aspects of immune dysfunction, including impaired neutrophil chemotaxis and phagocytosis, which can delay the resolution of chronic inflammation and reduce effective immune surveillance against emerging malignant clones.19,21,22 Collectively, these systemic derangements synergize with localized chronic inflammation, such as chronic balanoposthitis, to enhance epithelial DNA damage and promote malignant transformation in susceptible tissues, as observed in this patient.
Chronic Inflammation and Squamous Cell Carcinogenesis
The link between chronic inflammation and SCC is well established across multiple organ systems, including the skin, esophagus, and cervix.8,23 At the cellular level, long-standing chronic inflammation induces a state of persistent oxidative stress, releasing reactive oxygen species (ROS) and pro-inflammatory cytokines within the penile microenvironment.6,7 In literature, these factors are well-documented to activate transcription factors such as nuclear factor kappa B (NF – κB) and signal transducer and activator of transcription 3 STAT3, which upregulates cyclooxygenase-2 (COX-2) expression.8,23 While molecular profiling was unavailable to map these specific pathways in our patient due to diagnostic limitations, this established inflammatory cascade represents the most plausible theoretical mechanism linking his decades of chronic balanoposthitis to subsequent keratinizing epithelial malignancy.6,23
Within the penile epithelium, chronic inflammatory dermatoses, including balanoposthitis, lichen sclerosus, and chronic infectious states, are well-recognized precancerous conditions that markedly increase the risk of progression to invasive penile squamous cell carcinoma.24–28
The patient’s lesion demonstrated classic high-risk features associated with malignant transformation: non-healing ulceration, indurated and everted edges, progressive enlargement, foul discharge, and eventual urethral involvement. These features align with established clinical descriptors of invasive penile SCC arising from chronic inflammatory disease. Histologically, the tumour was a keratinising squamous cell carcinoma, the variant most frequently associated with HPV‑negative status and with precursor conditions such as lichen sclerosus and chronic balanoposthitis.4,28,29
Delay in Presentation and Disease Progression
A notable feature of this case is the delay in seeking medical care, attributed to the patient’s expectation that the lesion would resolve spontaneously. Delayed presentation is a common and critical factor in penile cancer outcomes, often resulting in more advanced local disease and increased morbidity.12,13 By the time of presentation, the tumor had progressed to Stage II disease N0, M0 (pT2 cN0 M0 (Stage II)) with urethral involvement, necessitating partial penectomy.
This case highlights the critical clinical significance of early recognition and timely management of chronic inflammatory penile conditions. In the present patient, prolonged untreated balanoposthitis in the setting of diabetes mellitus and an uncircumcised foreskin culminated in progressive ulceration, urethral obstruction, and eventual malignant transformation. Persistent, non-healing penile ulcers, particularly when painless, indurated, or associated with foul discharge, should prompt a high index of suspicion for underlying malignancy and warrant early biopsy. Delayed presentation, as observed in this case, remains a recurring challenge in resource-limited settings and underscores the need for improved patient education regarding genital hygiene, symptom recognition, and the oncologic risks of deferring care.
Interpretation of Incidental Laboratory Findings
The serum PSA of 11.2 ng/mL, in the context of a 35.9 cc prostate, acute urinary retention, and cystitis, is most consistent with benign prostatic hyperplasia and inflammation rather than prostatic carcinoma; repeat measurement after decompression is planned. The isolated GGT elevation (85 U/L) with normal transaminases and ultrasonographic fatty liver is attributable to the patient’s alcohol intake and underlying metabolic syndrome. The resting SpO2 of 92% was recorded during acute distress and may reflect diabetic pulmonary microvasculopathy; no respiratory intervention was required, but this finding warrants outpatient re‑evaluation.Organ-sparing treatment modalities, such as local tumor excision, laser ablation, or topical therapies, were bypassed in this case due to the advanced stage at clinical presentation. The tumor had already caused extensive, deep destruction of the glans penis and exhibited infiltration into the corpus cavernosum and corpus spongiosum (T2 disease). Attempting an organ-preserving approach would have carried an unacceptably high risk of positive surgical margins and local recurrence, necessitating a definitive partial penectomy to achieve safe oncological control.
Following his discharge, the patient was enrolled in a standard, rigorous 2-year post-treatment surveillance schedule in accordance with adapted regional guidelines.13 This program dictates clinical follow-up evaluations every 3 months for the first year, and every 6 months during the second year. Each visit entails a meticulous clinical palpation of the penile stump to monitor for local recurrence, alongside a thorough physical examination of both inguinal basins to identify emerging regional lymphadenopathy early.
Limitation
This report is primarily limited by the absence of diagnostic molecular confirmation. Due to resource constraints at our facility, p16/p53 immunohistochemistry, HPV DNA testing, and baseline HbA1c levels were unavailable. Furthermore, pathological staging of the inguinal lymph nodes via biopsy or FNAC was not performed, leaving the nodal evaluation restricted to clinical examination (cN0). Regarding the tissue specimen, the formalin-fixed paraffin-embedded (FFPE) tissue block remains securely archived within the Kabale University pathology repository; however, immunohistochemical scanning capabilities for p16 are currently unavailable at our institution. Lastly, our current follow-up data is limited to the early post-operative period. Despite these limitations, the classic keratinizing morphology of the tumor, its direct emergence from a field of severe chronic balanoposthitis, and the patient’s long-standing phimosis collectively offer a robust, descriptive clinical window into probable inflammation-associated penile carcinogenesis.
Conclusion
Chronic balanoposthitis can serve as a direct, HPV‑independent precursor to penile squamous cell carcinoma, particularly in uncircumcised diabetic men in whom persistent smegma accumulation, phimosis, and hyperglycaemia‑driven immune impairment create a sustained pro‑carcinogenic microenvironment. Persistent, non‑healing penile ulcers warrant early biopsy, and refractory balanoposthitis should be managed aggressively to prevent progression to invasive disease. This case reinforces the need for heightened clinical suspicion and targeted preventive education in high‑risk populations.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
Institutional approval for single-case reports is waived by the Kabale University School of Medicine Research Ethics Committee, provided that strict anonymity is maintained and explicit patient consent is secured. This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying clinical images.
Acknowledgments
The authors would like to acknowledge the Departments of Surgery of Kabale University School of Medicine for their academic support. We are particularly grateful to Dr. Mugarura Timothy and Dr. Colin Meghoo for their mentorship, guidance, and valuable insights during the preparation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We declare that no funding, financial support, or grants were received from any institutional, private, or corporate source.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Douglawi A, Masterson TA. Updates on the epidemiology and risk factors for penile cancer. Transl Androl Urol. 2017;6(5):785–11. PubMed PMID: 29184774; PubMed Central PMCID: PMC5673812. doi:10.21037/tau.2017.05.19
2. Thomas A, Necchi A, Muneer A, et al. Penile cancer. Nat Rev Dis Primer. 2021;7(1):11. doi:10.1038/s41572-021-00246-5
3. Coelho RWP, Pinho JD, Moreno JS, et al. Penile cancer in Maranhão, Northeast Brazil: the highest incidence globally? BMC Urol. 2018;18:50. PubMed PMID: 29843769; PubMed Central PMCID: PMC5975591. doi:10.1186/s12894-018-0365-0
4. Amicuzi U, Grillo M, Stizzo M, et al. Exploring the multifactorial landscape of penile cancer: a comprehensive analysis of risk factors. Diagnostics. 2024;14(16):1790. doi:10.3390/diagnostics14161790
5. Larke NL, Thomas SL, Dos Santos Silva I, Weiss HA. Male circumcision and penile cancer: a systematic review and meta-analysis. Cancer Causes Control. 2011;22(8):1097–1110. doi:10.1007/s10552-011-9785-9
6. Balkwill FR, Mantovani A. Cancer-related inflammation: common themes and therapeutic opportunities. Semin Cancer Biol. 2012;22(1):33–40. doi:10.1016/j.semcancer.2011.12.005
7. Reuter S, Gupta SC, Chaturvedi MM, Aggarwal BB. Oxidative stress, inflammation, and cancer: how are they linked? Free Radic Biol Med. 2010;49(11):1603–1616. PubMed PMID: 20840865; PubMed Central PMCID: PMC2990475. doi:10.1016/j.freeradbiomed.2010.09.006
8. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
9. Onywera H, Williamson AL, Ponomarenko J, Meiring TL. The penile microbiota in uncircumcised and circumcised men: relationships with HIV and human papillomavirus infections and cervicovaginal microbiota. Front Med. 2020;7:383. doi:10.3389/fmed.2020.00383
10. Jain M, Ansari F, Agarwal N, Mittal AK. Morphological patterns of balanoposthitis and their correlation with final etiological diagnosis. Indian Dermatol Online J. 2023;14(2):187–194. PubMed PMID: 37089850; PubMed Central PMCID: PMC10115317. doi:10.4103/idoj.idoj_197_22
11. La Vignera S, Condorelli RA, Cannarella R, et al. Urogenital infections in patients with diabetes mellitus: beyond the conventional aspects. Int J Immunopathol Pharmacol. 2019;33:2058738419866582. PubMed PMID: 32031031; PubMed Central PMCID: PMC6728654. doi:10.1177/2058738419866582
12. Stecca C, Alt M, Jiang D, et al. Recent advances in the of penile cancer: a contemporary review of the literature. Oncol Ther. 2021;9:21–39. doi:10.1007/s40487-020-00135-z
13. Hakenberg OW, Comperat EM, Minhas S, Necchi A, Protzel C, Watkin N. EAU guidelines on penile cancer: 2014 update. Eur Urol. 2015;67(1):142–150. doi:10.1016/j.eururo.2014.10.017
14. Onywera H, Williamson AL, Ponomarenko J, Meiring TL. Management guidelines of penile cancer - a contemporary review of the sub-Saharan African literature. Transl Oncol BMC Syst. 2020;7(1):383–395. doi:10.1186/s13027-020-00293-9
15. Morris BJ, Gray RH, Castellsague X, et al. The strong protective effect of circumcision against cancer of the penis. Adv Urol. 2011;2011(1):812368. doi:10.1155/2011/812368
16. Kim T, Choi SH. Diabetes mellitus and infectious diseases: current evidence and clinical implications. Diabetes Metab J. 2025;49(5):915–933. PubMed PMID: 40859782; PubMed Central PMCID: PMC12436038. doi:10.4093/dmj.2025.0508
17. Toniolo A, Cassani G, Puggioni A, et al. The diabetes pandemic and associated infections: suggestions for clinical microbiology. Rev Res Med Microbiol. 2019;30(1):1. doi:10.1097/MRM.0000000000000155
18. Berbudi A, Rahmadika N, Tjahjadi AI, Ruslami R. Type 2 diabetes and its impact on the immune system. Curr Diabetes Rev. 2020;16(5):442–449. PubMed PMID: 31657690; PubMed Central PMCID: PMC7475801. doi:10.2174/1573399815666191024085838
19. Forbes JM, Cooper ME. Mechanisms of diabetic complications. Physiol Rev. 2013;93(1):137–188. doi:10.1152/physrev.00045.2011
20. Brownlee M. Biochemistry and molecular cell biology of diabetic complications. Nature. 2001;414(6865):813–820. doi:10.1038/414813a
21. Geerlings SE, Hoepelman AIM. Immune dysfunction in patients with diabetes mellitus (DM). FEMS Immunol Med Microbiol. 1999;26(3–4):259–265. doi:10.1111/j.1574-695X.1999.tb01397.x
22. Vigneri P, Frasca F, Sciacca L, Pandini G, Vigneri R. Diabetes and cancer. Endocr Relat Cancer. 2009;16(4):1103–1123. doi:10.1677/ERC-09-0087
23. Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–867. PubMed PMID: 12490959; PubMed Central PMCID: PMC2803035. doi:10.1038/nature01322
24. Gutiérrez-Pascual M, Vicente-Martín FJ, López-Estebaranz JL. Lichen sclerosus and squamous cell carcinoma. Actas Dermo-Sifiliográficas Engl Ed. 2012;103(1):21–28. doi:10.1016/j.adengl.2011.05.004
25. Schulenburg BS, Hook S, Becker M, et al. Lichen sclerosus bei klinisch relevanter Phimose: häufigkeit, Risikofaktoren und Assoziation mit Plattenepithelkarzinomen des Penis. Urol. 2024;63(5):469–473. doi:10.1007/s00120-023-02271-6
26. Velazquez EF, Cubilla AL. Lichen Sclerosus in 68 patients with squamous cell carcinoma of the penis: frequent atypias and correlation with special carcinoma variants suggests a precancerous role. Am J Surg Pathol. 2003;27(11):1448.
27. Chaux A, Cubilla AL. Advances in the pathology of penile carcinomas. Hum Pathol. 2012;43(6):771–789. doi:10.1016/j.humpath.2012.01.014
28. Dillner J, von Krogh G, Horenblas S, Meijer CJLM. Etiology of squamous cell carcinoma of the penis. Scand J Urol Nephrol. 2000;34(205):189–193. doi:10.1080/00365590050509913
29. Cubilla AL, Velazquez EF, Amin MB, Epstein J, Berney DM, Corbishley CM. The World Health Organisation 2016 classification of penile carcinomas: a review and update from the International Society of Urological Pathology expert‐driven recommendations. Histopathology. 2018;72(6):893–904. doi:10.1111/his.13429
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.