Back to Journals » International Medical Case Reports Journal » Volume 18
“Keep HIT in Mind and Take Care”. Multiple Tips From a Single Patient
Authors Bevilacqua S ![]() , Stefàno P, Ranfagni V, Ammannati B, Codecasa R, Gori AM, Cesari F, Titherington LM, Del Pace S, Rogolino A, Marcucci R
, Stefàno P, Ranfagni V, Ammannati B, Codecasa R, Gori AM, Cesari F, Titherington LM, Del Pace S, Rogolino A, Marcucci R
Received 19 October 2024
Accepted for publication 22 January 2025
Published 18 February 2025 Volume 2025:18 Pages 265—271
DOI https://doi.org/10.2147/IMCRJ.S500148
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Keep HIT in mind and take care – Video Abstract [500148]
Views: 75
Sergio Bevilacqua,1 Pierluigi Stefàno,2 Viola Ranfagni,1 Bianca Ammannati,1 Riccardo Codecasa,2 Anna Maria Gori,3 Francesca Cesari,3 Lara Mary Titherington,1 Stefano Del Pace,2 Angela Rogolino,3 Rossella Marcucci3
1Department of Anesthesia and Intensive Care. University Hospital Careggi, Florence, Italy; 2Department of Cardiothoracic and Vascular Surgery. University Hospital Careggi, Florence, Italy; 3Department of Experimental and Clinical Medicine. Atherothrombotic Diseases Center. University Hospital Careggi, Florence, Italy
Correspondence: Sergio Bevilacqua, Department of Anesthesia and Intensive Care. University Hospital Careggi, viale Morgagni 85, Firenze, 50134, Italy, Tel +390557945162, Email [email protected]
Introduction: Heparin-induced thrombocytopenia (HIT) is a relatively rare condition burdened by a high rate of complications and mortality. Cardiac surgery is a high risk setting for this condition. But in this area, some particularities can make both diagnosis and treatment difficult. Warfarin is often needed after valvular surgery but may be dangerous if HIT is ongoing. Danaparoid is the only anticoagulant whose mechanism of action has been demonstrated to counteract the pathogenesis of HIT. However, the 24-hour half-life challenges its use after surgery.
Case Presentation: Here, we present a case in which HIT occurred six days after cardiac surgery. Warfarin was initiated two days after surgery but was stopped five days later, given the high risk of bleeding due to concomitant thrombocytopenia. HIT probability was initially underestimated, because a misleading diagnosis of endocarditis was made. When redo surgery was performed, no infectious masses were found, but a large thrombus was removed from the left atrium. Bivalirudin and danaparoid were used as alternative anticoagulants during the subsequent postoperative course.
Conclusion: HIT should always be kept in mind after cardiac surgery, even if a more plausible cause of thrombocytopenia is present. Discontinuation of warfarin could lead to catastrophic consequences if an unrecognized HIT is ongoing, and an alternative anticoagulant is not started. Bivalirudin and danaparoid were used after the diagnosis of HIT, adapting anticoagulant therapy to the needs of recent surgery.
Keywords: thrombocytopenia, heparin, danaparoid, warfarin, endocarditis, bacterial, embolism and thrombosis, mitral valve annuloplasty, echocardiography
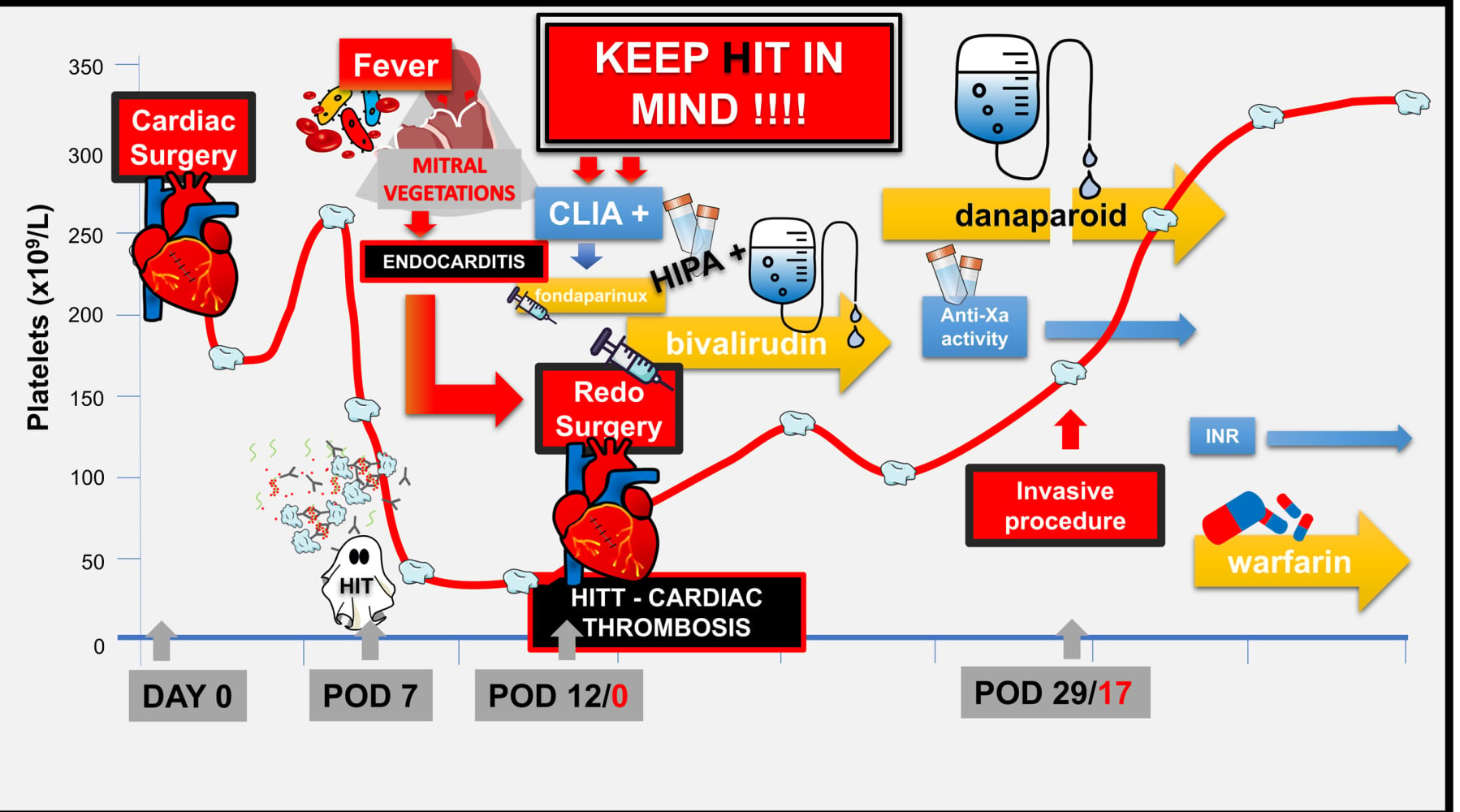
Graphical Abstract:
Introduction
Cardiac surgery is considered a high-risk setting for heparin-induced thrombocytopenia (HIT).1 In a recent study,2 we reported that as many as 16 patients with acute HIT, in whom HIT was diagnosed more than five days after the initiation of vitamin K antagonist (VKA) therapy, did not experience new thromboembolic complications although VKA was neither discontinued nor reversed, as current guidelines would advise.3,4 We hypothesized that this result could be ascribed to the early initiation of oral anticoagulation at our institution in patients in whom VKA was indicated. In fact, since antibodies are typically formed more than five days after heparin exposure, by that time warfarin anticoagulation may have already been balanced in favor of the inhibition of procoagulant factors.
Here, we describe a case of HIT complicated by thrombosis, from which we can draw some key tips on the real-world management of HIT in cardiac surgery.
Case Presentation
We describe the case of a 52-year-old Caucasian female patient. Her cardiovascular risk factors were dyslipidemia and that she was overweight. She had no previous surgeries. She reported two full-term pregnancies and one abortion and had a negative family history of thrombophilia.
She had suffered an ischemic stroke three years prior to the admission, due to atrial fibrillation. On that occasion, transthoracic echocardiography revealed moderate/severe mitral regurgitation. Amiodarone-induced hyperthyroidism also occurred. In the following months, while presenting progressive and complete neurologic recovery she had a rapid progression of mitral regurgitation and dyspnea such that surgery was indicated.
Medications prior to admission included warfarin, tapazole, furosemide, potassium canrenoate and bisoprolol.
The surgical procedure consisted of mitral valve repair with a Carpentier-Edwards Physio II annuloplasty ring, tricuspid valve repair with a Medtronic Contour 3D annuloplasty ring and left atrial appendage exclusion with atriclip pro device, performed via right mini-thoracotomy access.
The immediate postoperative course was regular. The patient was discharged from the intensive care unit on postoperative day (POD) 2 in excellent clinical condition.
In accordance with our anticoagulation protocol, 5000 IU of subcutaneous UFH three times a day was reintroduced on POD 1, while oral warfarin was also started on POD 2 aiming for a target international normalized ratio (INR) between 2 and 3.
On POD 6, subcutaneous heparin was discontinued because the INR was already within the therapeutic range (2.5). On the same day a fever occurred. Consequently, the central venous catheter was removed, and the tip and blood samples were collected for culture. A transthoracic echo ruled out endocarditis. A few days later, two blood cultures tested positive for staphylococcus epidermidis.
On POD 7, the patient had thrombocytopenia (34 × 109/L from 267 × 109/L on POD 5), and a 1 mg/dl decrease in her Hb level. Therefore, since the INR was already 2.6, warfarin was suspended, and vitamin K was administered (5 mg).
On POD 9, a floating mass on the mitral annulus became visible on both transthoracic and transesophageal echocardiography while PLT count reached the nadir of 21 × 109/L (Figure 1 and Supplemental videos 1 and 2).
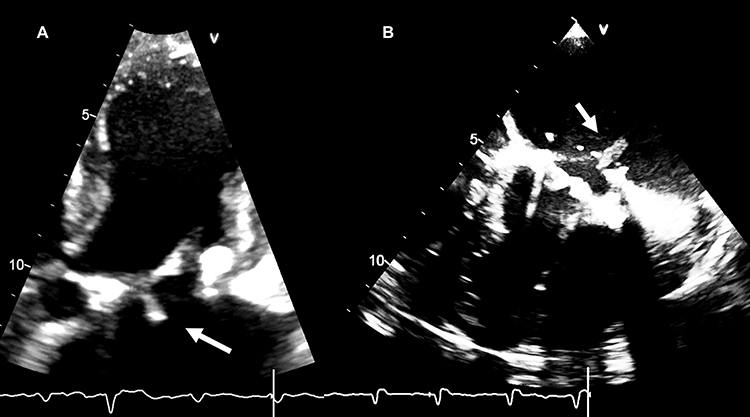 |
Figure 1 TTE and TEE images of the mitral valve. Abbreviations: TTE, transthoracic echocardiography; TEE, transesophageal echocardiography. Notes: (A) transthoracic parasternal view. (B) Transesophageal four chambers view. Vegetating mass (arrows) mimicking endocarditis. |
The urgent indication for redo surgery was decided upon. While antibiotics were started (piperacillin/tazobactam and vancomycin), HIT suspicion also arose because of a 4T score of 5 (Figure 2).
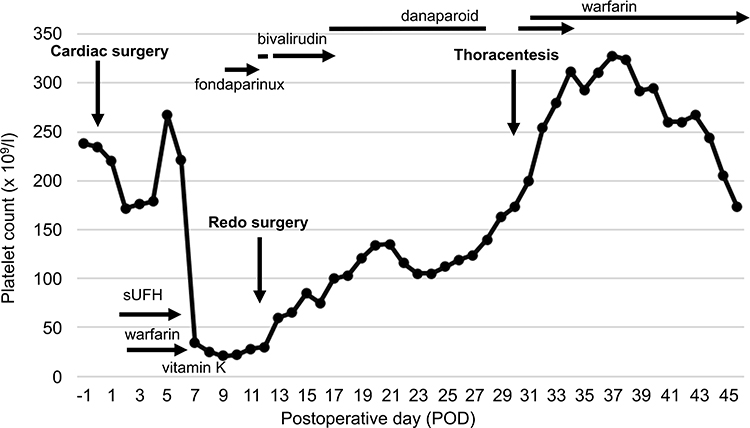 |
Figure 2 Platelet count, clinical events, and treatment during hospitalization. Notes: Platelet count during hospitalization (dotted line). Clinical events are indicated by vertical arrows. Anticoagulation management and duration is indicated by horizontal arrows. |
Therefore, an immunoglobulin (Ig)G-specific anti-PF4–heparin chemiluminescent immunoassay (CLIA) was ordered, and the alternative anticoagulant fondaparinux (7.5 mg once a day) was initiated and maintained until the day before surgery. CLIA test resulted positive for PF4/heparin antibodies (8.9 U/mL), and the heparin-induced platelet activation assay (HIPA) confirmed HIT diagnosis on POD 10.
Redo operation was performed on POD 12. Bivalirudin was the anticoagulant of choice for cardiopulmonary bypass, as had been successfully done in the past in similar cases.5 Unexpectedly, a voluminous thrombotic mass (Figure 3) was removed from the patient’s left atrium (further confirmed as a thrombus by histologic examination and by a negative culture exam). The diagnosis of HIT with thrombosis (HITT) was therefore clear, and alternative anticoagulation therapy with bivalirudin at therapeutic dose was resumed in the postoperative period as soon as bleeding became negligible.
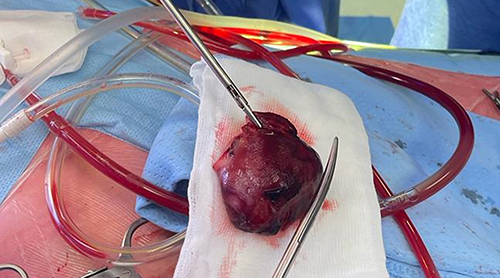 |
Figure 3 Atrial thrombus after removal. |
The patient was weaned from the ventilator on POD 2. On POD 4, after removal of the chest tubes, bivalirudin was discontinued, and danaparoid was initiated. Two subcutaneous (750 U) doses were administered first; thereafter, endovenous infusion was started at 396 U/h for the first 4 hours, 297 U/h for the next 4 hours and then 198 U/h. Danaparoid was monitored daily through its plasmatic anti-Xa activity (Figure 4).
 |
Figure 4 Danaparoid infusion, anti-Xa activity monitoring to perform thoracentesis and switch to VKA. Abbreviations: VK, vitamin K antagonist (warfarin); INR, international normalized ratio. Notes: The first two danaparoid doses were administered subcutaneously (orange dots). Danaparoid infusion rate (orange line; U/h), anti-Xa activity monitoring (blue line; U/mL), predicted anti-Xa activity after stopping danaparoid, considering 25 h half-time (gray line; U/mL). VKA oral administrations (red dot). |
On POD 15, a right pleural effusion occurred, which was drained in the following days. Therefore, planning thoracentesis, danaparoid was temporarily discontinued. Danaparoid anti-Xa activity was monitored every 12 hours until it reached the prophylactic range target (0.1–0.2 U/mL).
Thoracentesis was performed on POD 17, 38 hours after danaparoid suspension when anti-Xa activity was 0.14 U/mL. The drug was resumed 2 hours after the uncomplicated procedure (180 U/h and 162 U/h the following day) once procedural complications were excluded. The anti-Xa activity target was then set at the lowest level of the therapeutic range (0.45 U/mL).
On POD 18, when the anti-Xa activity was 0.39 U/mL, and the platelet (PLT) count had substantially recovered (160 × 109/L), the switch from danaparoid to vitamin K antagonist (VKA) was initiated. The first warfarin dose (5 mg) was administered starting from an INR 1.1. Over the next five days, the INR and the administered warfarin dose were as follows: 1.2 and 6.25 mg, 1.4 and 6.25 mg, 1.9 and 6.25 mg, 2.1 and 6.25 mg, and 2.8 and 3.75 mg, respectively.
On POD 20, after 66 hours from warfarin initiation, danaparoid infusion was stopped while plasma anti-Xa activity was 0.54 U/mL. Two days after discontinuation, the measured danaparoid activity was 0.09, while INR was 2.8.
The patient was successfully discharged from the hospital on postoperative day 35 (POD 48 from the first operation) in good clinical condition. The PLT count was then 173 × 109/L. The INR was 3.2. The serum creatinine concentration was 0.64 mg/dl.
Discussion
In this report, we discuss a case of HITT, that provides important guidance in these complex scenarios, which is worthy of being pointed out.
- HIT typically occurred on POD 6, but it was initially underestimated, as endocarditis appeared as a much more plausible cause of thrombocytopenia. However, 4T score was 5 (PLT decrease: > 50%, PLT nadir ≥ 20 × 109/L and onset time of PLT fall 5–10 days, and another plausible cause of thrombocytopenia was present). Moreover, a classic biphasic pattern of PLT count could be recognized (Figure 2). Therefore, we should have considered an intermediate risk of HIT, even though everything seemed to point to the diagnosis of endocarditis (Figure 1 and Supplementary videos 1 and 2).
- In this regard, the ultrasound appearance of a vegetation can be very similar to that of a thrombotic mass, but the two conditions can also coexist.6 Therefore, any thrombocytopenia after cardiac surgery if 4T score is ≥4, must be considered and treated as heparin-induced until proven otherwise, especially if characterized by a biphasic pattern,7 even if an infection or another cause of thrombocytopenia is highly suspected or even documented.
- Additionally, in this case, warfarin was introduced early, as in the other 16 cases described in our previous report.2 However, VKA was not discontinued because of HIT but for the elevated risk of bleeding due to concomitant thrombocytopenia. This was the reason why it was not replaced with any alternative anticoagulant. Of note, thrombosis did not occur whilst the warfarin was being administered to an appropriate INR, but abruptly appeared as soon as warfarin was discontinued, not being replaced by an alternative anticoagulant. Although warfarin can be extremely dangerous if started when acute HIT is ongoing,8 a unique condition can take place in the cardiac surgery setting. In fact, when HIT occurs, the patient may be already full anticoagulated, being on VKA for more than 5 days with heparin already suspended.2 Thrombocytopenia is also common after surgery and the risk of bleeding becomes important if patient is being treated with warfarin. Therefore, HIT should be carefully excluded before discontinuing VKA in thrombocytopenic patients. If therapeutic, VKA suspension could lead to life-threatening consequences if an unrecognized HIT is ongoing, and an alternative anticoagulant is not introduced.
- Danaparoid, is the only anticoagulant whose mechanism of action has been demonstrated to inhibit HIT pathogenesis.9 However, experience with danaparoid is still limited, especially in cardiac surgery.10 Danaparoid consists of a mixture of heparan, dermatan and chondroitin sulfates, with high anti-factor Xa to anti-factor IIa (thrombin) activity ratio (>20:1).11 Pharmacokinetic studies indicate a half-life of 19.2–24.5 hours for anti-Xa activity of danaparoid, while that of anti-IIa activity is much shorter (1.8 to 4.3 hours). Because of the long half-life of the anti-Xa component, and the lack of an antidote, it would not be the ideal anticoagulant after cardiac surgery, where patients are at elevated risk of bleeding and frequently need to undergo invasive procedures. Consequently, we preferred bivalirudin both for CPB management and anticoagulation in the immediate postoperative period due to its short and predictable half-life (25 min).12 Only some days later, bivalirudin was replaced by danaparoid, considering that the PLT count was struggling to recover. Given both the limited experience with danaparoid in cardiac surgery and the complexity of the case, we overlapped it with bivalirudin, administering two subcutaneous doses before starting the infusion, and we also monitored its anti-Xa activity daily. Anti-Xa activity provides an estimate of the amount of circulating danaparoid especially during continuous infusion.11 In this case, danaparoid showed remarkable anticoagulant stability (Figure 4). Moreover, after that danaparoid was initiated, we were faced with two challenges: performing an invasive procedure (thoracentesis) in an anticoagulated patient and switching from danaparoid to VKA. To do both things safely we did them at separate times, strictly monitoring the anti-Xa activity level. First, we discontinued danaparoid, until anti-Xa activity was in the prophylactic range (0.1–0.2 U/mL). Only in that narrow time window, we conducted thoracentesis with lower risk of bleeding and then, once complications had been excluded, we resumed danaparoid infusion. Danaparoid anti-Xa activity half-life was almost 19 hours in this patient. After thoracentesis, danaparoid infusion was resumed until the PLT count recovered. At that time, the transition to VKA could begin. Approximately five days were needed to achieve stable anticoagulation with VKA. Keeping in mind the danaparoid decay curve that had been recently tested in the same patient, we continued danaparoid infusion for 66 hours after the first warfarin dose. When danaparoid was suspended, its half-life was like the previous one and anti-Xa activity was below 0.1 U/mL in 42 hours. At that time, almost 5 days after the reintroduction of warfarin had passed, and INR was 2.8 (Figure 4). Therefore, switching from danaparoid to VKA was successfully done in absence of new thrombotic complications, but without overlapping the anticoagulant effects of the two drugs.
The main limitation of this report is that it describes a single case in a specific surgical setting, which limits the generalizability of the results to a broader population or different settings. Furthermore, the patient described in this case had normal renal function. The half-life of danaparoid may be less predictable in cases of impaired renal function.
Conclusion
Four tips can be suggested or highlighted by this case report:
- Always “keep HIT in mind” in a thrombocytopenic patient who is or has been treated with heparin if the 4T score is ≥4. Although rare, HIT is a catastrophic prothrombotic clinical condition, burdened by high mortality.
- Always “keep HIT in mind” even if a more plausible cause of thrombocytopenia seems to be present, such as a documented infective endocarditis. This may in fact be thrombosis and thrombocytopenia may be induced by heparin.
- Always “keep HIT in mind” when warfarin is therapeutic and about to be discontinued in a thrombocytopenic patient whose vitamin k-dependent procoagulant factors are stably inhibited. Warfarin suspension may precipitate life-threatening thrombosis if unrecognized HIT is ongoing, and an alternative anticoagulant is not initiated at therapeutic intensity.
- The long half-life of danaparoid may limit its use after cardiac surgery. However, its effect can be adapted to clinical needs even in this setting, by monitoring anti-Xa activity.
Data Sharing Statement
All the data generated or analyzed during this study are included in this publication. Further inquiries can be directed to the corresponding author.
Ethics Statement
Written informed consent was provided by the patient to have the case details and any accompanying images and video published. All data used was anonymized. The presented case report was performed according to the declaration of Helsinki. No official institutional approval was required by the internal ethics committee to publish the details of the case report.
Acknowledgments
We gratefully acknowledge Francesco Bevilacqua, Careggi University Hospital, for his valuable help in the development of the mathematical model applied to the decay curve of the danaparoid. The first version of this article has been posted in the research square preprint server: https://doi.org/10.21203/rs.3.rs-4638457/v1.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no competing interests, or other interests that might be perceived to influence the results and/or discussion reported in this paper.
References
1. Warkentin TE, Greinacher A. Heparin-induced thrombocytopenia and cardiac surgery. Ann Thorac Surg. 2003;76:2121–2131. doi:10.1016/j.athoracsur.2003.09.034
2. Bevilacqua S, Stefàno P, Berteotti M, et al. Heparin induced thrombocytopenia after cardiac surgery. A single-center, retrospective cohort study. Res Pract Thromb Haemost. 2024;8:102465. doi:10.1016/j.rpth.2024.102465
3. Linkins LA, Dans AL, Moores LK, et al. Treatment and prevention of heparin-induced thrombocytopenia: antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e495S–e530S. doi:10.1378/chest.11-2303
4. Cuker A, Arepally GM, Chong BH, et al. American society of hematology 2018 guidelines for management of venous thromboembolism: heparin-induced thrombocytopenia. Blood Adv. 2018;2:3360–3392. doi:10.1182/bloodadvances.2018024489
5. Caciolli S, Prisco D, Stefano P. Bivalirudin and cardiac surgery: two case reports. G Ital Cardiol. 2008;9:372–374.
6. Delgado V, Ajmone Marsan N, de Waha S, ESC Scientific Document Group, et al. 2023 ESC guidelines for the management of endocarditis. Eur Heart J. 44;2023:3948–4042. doi:10.1093/eurheartj/ehad193
7. Pouplard C, May MA, Regina S, et al. Changes in platelet count after cardiac surgery can effectively predict the development of pathogenic heparin-dependent antibodies. Br J Haematol. 2005;128:837–841. doi:10.1111/j.1365-2141.2005.05381.x
8. Dhawan N. Beware of warfarin-induced skin necrosis in the setting of heparin-induced thrombocytopenia. Cureus. 2020;12:e8857. doi:10.7759/cureus.8857
9. Krauel K, Fürll B, Warkentin TE, et al. Heparin-induced thrombocytopenia-therapeutic concentrations of danaparoid, unlike fondaparinux and direct thrombin inhibitors, inhibit formation of platelet factor 4-heparin complexes. J Thromb Haemost. 2008;6:2160–2167. doi:10.1111/j.1538-7836.2008.03171.x
10. Magnani HN, Gallus A. Heparin-induced thrombocytopenia (HIT). A report of 1478 clinical outcomes of patients treated with danaparoid (Orgaran) from 1982 to mid-2004. Thromb Haemost. 2006;95:967–981. doi:10.1160/TH05-07-0489
11. Wilde MI, Markham A. Danaparoid: a review of its pharmacology and clinical use in the management of heparin-induced thrombocytopenia. Drugs. 1997;54:903–924. doi:10.2165/00003495-199754060-00008
12. Shammas NW. Bivalirudin: pharmacology and clinical applications. Cardiovasc Drug Rev. 2005;23:345–360. doi:10.1111/j.1527-3466.2005.tb00177.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.