Back to Journals » Open Access Emergency Medicine » Volume 9
Jugular bulb oxygen saturation correlates with Full Outline of Responsiveness score in severe traumatic brain injury patients
Authors Senapathi TG ![]() , Wiryana M, Sinardja K, Nada KW, Sutawan IB, Ryalino C, Alphonso A
, Wiryana M, Sinardja K, Nada KW, Sutawan IB, Ryalino C, Alphonso A
Received 23 June 2017
Accepted for publication 7 August 2017
Published 28 August 2017 Volume 2017:9 Pages 69—72
DOI https://doi.org/10.2147/OAEM.S144722
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Tjokorda Gde Agung Senapathi, Made Wiryana, Ketut Sinardja, Ketut Wibawa Nada, Ida Bagus Krisna Jaya Sutawan, Christopher Ryalino, Aloysius Alphonso
Department of Anesthesiology and Intensive Care, Udayana University, Sanglah General Hospital, Denpasar, Bali, Indonesia
Background: Maintaining brain oxygenation status is the main goal of treatment in severe traumatic brain injury (TBI). Jugular venous oxygen saturation (SjvO2) monitoring is a technique to estimate global balance between cerebral oxygen supply and its metabolic requirement. Full Outline of Responsiveness (FOUR) score, a new consciousness measurement scoring, is expected to become an alternative for Glasgow Coma Scale (GCS) in evaluating neurologic status of patients with severe traumatic head injury, especially for those under mechanical ventilation.
Methods: A total of 63 patients with severe TBI admitted to emergency department (ED) were included in this study. SjvO2 sampling was taken every 24 hours, until 72 hours after arrival. The assessment of FOUR score was conducted directly after each blood sample for SjvO2 was taken. Spearman’s rank correlation was used to determine the correlation between SjvO2 and FOUR score. Regression analysis was used to determine mortality predictors.
Results: From the 63 patients, a weak positive correlation between SjvO2 and FOUR score (r=0.246, p=0.052) was found upon admission. Meanwhile, strong and moderate negative correlation values were found in 48 hours (r=-0.751, p<0.001) and 72 hours (r=-0.49, p=0.002) after admission. Both FOUR score (p<0.001) and SjvO2 (p=0.04) were found to be independent mortality predictors in severe TBI.
Conclusion: There was a negative correlation between the value of SjvO2 and FOUR score at 48 and 72 hours after admission. Both SjvO2 and FOUR score are independent mortality predictors in severe TBI.
Keywords: jugular vein, unconsciousness, Full Outline of Responsiveness, mortality predictor
Introduction
Traumatic brain injury (TBI) is one of the commonest cases in the emergency department (ED). It is one leading cause of mortality in productive age, where the incidence is significantly increased with the increased use of motor vehicles.1,2 The efforts to minimize secondary brain injury in TBIs is the key for intervention in neuroanesthesia and intensive care.3 The primary goal is to maintain the adequacy of tissue oxygenation. Thus, the ability to do early detection of hypoxia is very essential in critical care, since ischemia and hypoxemia have a vital contribution to the brain damage.1,3
Jugular venous oxygen saturation (SjvO2) is one of the techniques that can be used to estimate the balance between cerebral oxygen delivery and demand.4–6
For >40 years, Glasgow Coma Scale (GCS) is the most common method used by clinicians all over the world in assessing consciousness level and neurological condition. Its main features are that it is simple, easy to perform, and does not require any special diagnostic tools.7 This scale has several limitations such as the interobserver variability and the inability to examine the verbal (V) component in intubated patients.4 GCS also fails to explore brain stem reflexes, changes in breathing patterns, and the need for mechanical ventilation, which may explain the severity of unconsciousness.4,5,8
Full Outline of Responsiveness (FOUR) score is a new scale for consciousness that was developed by a group of doctors at Mayo Clinic in 2005.4 This scale includes the examination of eye, motor, brain stem reflexes, and respiration.4,5 The FOUR score provides greater neurological detail than the GCS, recognizes a locked-in syndrome, and is superior to the GCS due to the availability of brainstem reflexes, breathing patterns, and the ability to recognize different stages of herniation.4 By expanding the neurological assessment with measurable evaluation, the hope is that FOUR score may provide an innovative and detailed way in assessing level of consciousness in critically ill patients.
Methods
The aims of this study were to determine the correlation between SjvO2 and FOUR score and to assess whether they act as independent mortality predictors in TBI cases. This study was held from January to March 2017 at ED and intensive care unit (ICU) of Sanglah General Hospital in Denpasar, Indonesia. This study was approved by the research ethics committee of Sanglah General Hospital and Udayana University. All the patients or their guardians have provided written informed consent to be included in this study.
Patients aged from 10 to 70 years with severe traumatic head injury who were admitted to ED were enrolled in this study. Those with cyanotic heart disease, chronic obstructive pulmonary disease, brain stem death upon admission, and contraindication conditions to single-lumen catheter insertion were excluded from the study. SjvO2 sampling was taken from single-lumen catheter in the unilateral side of the brain’s pathological process and was taken upon admission, 24 hours, 48 hours, and 72 hours after arrival. After the blood sample was taken, the observer assessed the FOUR score. Patients who were sedated for brain resuscitation purpose were excluded from the study.
Kolmogorov–Smirnov test was used to evaluate data normality. Correlation between SjvO2 and FOUR score was evaluated by Spearman’s correlation test. A p-value ≤0.05 was considered as statistically significant.
Results
A total of 63 eligible patients were enrolled in this study. The characteristics of subjects is shown are Table 1. The median age was 32 years with 44 (69.8%) patients male and the remaining 19 (17.9%) patients female. Out of these 63 patients, 50 (79.4%) were treated with surgical procedure and the others (20.6%) were treated conservatively in the ICU. In all, 44 patients (68.8%) were alive and discharged and the remaining 19 (30.2%) patients died under the treatment in ICU.
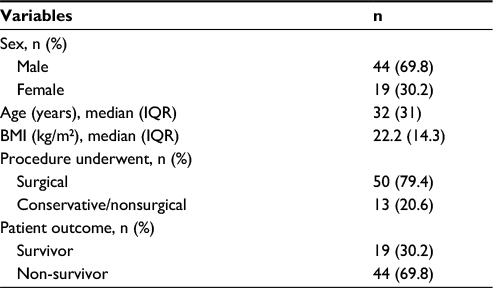 | Table 1 Sample characteristics Abbreviations: IQR, interquartile range; BMI, body mass index. |
Weak positive correlation (r=0.246, p=0.052) between SjvO2 and FOUR score was found upon patients’ arrival. On 24 hours post admission, the correlation between the two was r=0.481 (p=0.082). These two correlations were taken as not significant due to their respective p-value (>0.05).
Significant negative correlations were found on 48 and 72 hours post admission, with r=-0.751 (p<0.001) and r=–0.49 (p=0.002), respectively, as shown in Table 2. These indicate strong correlation at 48 hours and moderate correlation at 72 hours post admission.
 | Table 2 Spearman’s correlation between SjvO2 and FOUR score Notes: r, Spearman’s correlation; *statistically significant. Abbreviations: SjvO2, jugular venous oxygen saturation; FOUR, Full Outline of Responsiveness. |
In linear regression analysis, we looked for variables with statistically significant mortality predictor. Table 3 shows that SjvO2 (p=0.04) and FOUR score (p<0.001) are statistically significant variables as mortality predictors.
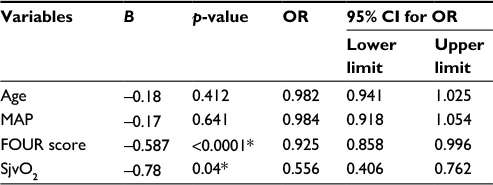 | Table 3 Regression analysis results to detect mortality predictor Note: *Statistically significant. Abbreviations: MAP, mean arterial pressure; OR, odds ratio; CI, confidence interval; FOUR, Full Outline of Responsiveness; SjvO2, jugular venous oxygen saturation. |
Discussion
SjvO2 measurement provides information about the balance between supply and demand of brain oxygen status.3,5 Unused oxygen in the brain will be delivered to the systemic circulation via internal jugular vein, and therefore, SjvO2 measurement can help to determine the balance between cerebral blood flow (CBF) and cerebral metabolic requirement of oxygen (CMRO2).3
Normal value of SjvO2 is 55–75%. The value <55% means patients have inadequate CBF due to various causes (hyperventilation, reduced cerebral perfusion pressure, and vasospasm) or increased CMRO2. While the value of >75% can be caused by hyperemia condition, decreased cerebral metabolism requirement (due to cell death or mitochondrial dysfunction), and microvascular shunting due to oxygen extraction and diffusion disturbance on the damaged brain tissue. These conditions have a poor neurological prognosis.3,5
FOUR score, a new consciousness scale, has an important advantage for patients treated at ICU as can help evaluate neurological status of intubated patients. Unlike GCS, it does not include verbal component on the examination.4,5,8 The FOUR scale includes the examination of eye, motor, brain stem reflexes, and respiration.4,5 FOUR score may be a promising method to evaluate consciousness in intubated patients in the intensive care setting.
This study was conducted to determine the correlation between SjvO2 and FOUR score. Weak positive correlation values were found at the admission and 24 hours post admission. However, they were not statistically significant, most likely due to patients being sedated in this period to assist brain resuscitation.
Meanwhile, moderate-to-strong negative correlation values were found at 48 and 72 hours post-arrival period. These results were consistent with the study of Sharf and El-Gebali,9 which reported a strong positive correlation between SjvO2 and GCS in all cases (r=0.85 and p<0.001) and in survived patients (r=0.74, p<0.001). The study also reported a strong negative correlation on 48 and 72 post-arrival periods. These findings show that FOUR score and GCS possess similar features in terms of their relationship with SjvO2.
Gopinath et al10 reported a correlation between desaturation in SjvO2 and final neurological prognosis in brain injury case. Poor final neurological prognosis was obtained in 90% of patients with recurrent SjvO2 desaturation events. In patients who did not have SjvO2 desaturation events, poor neurological prognosis was found only in 55% of these patients. Cormio et al11 reported that in 450 severe head injury patients treated at the intensive neurosurgical care unit, 25.6% of patients’ with increased SjvO2 got a better outcome (good recovery, moderate disability), 25.6% recovered with severe disability, and 48.8% died or turned into vegetative state. The two studies suggest that SjvO2 should be in optimal range, not lower or higher than its normal range.
Both SjvO2 and FOUR score were found to be significant predictors to mortality. Sharf and El-Gebali9 also reported that GCS (p=0.008) and SjvO2 (p<0.001) were significant mortality predictors.
The limitation of this study is the sample size that was relatively small. A similar research with a larger sample size can provide more information on the relationship between the two variables.
Conclusion
SjvO2 is significantly correlated with FOUR score at 48 and 72 hours after patient’s arrival. Both SjvO2 and FOUR score are significant mortality predictors. Further research may be needed to get more information about correlation between SjvO2 and FOUR score and to assess their relationship with long-term neurological outcomes such as Extended Glasgow Outcome Scale.
Disclosure
The authors report no conflicts of interest in this work.
References
Maloney-Wilensky E, Gracias V, Itkin A, et al. Brain tissue oxygen and outcome after severe traumatic brain injury: a systematic review. Crit Care Med. 2009;37(6):2057–2063. | ||
Menon DK, Schwab K, Wright DW, et al; Demographics and Clinical Assessment Working Group of the International and Interagency Initiative toward Common Data Elements for Research on Traumatic Brain Injury and Psychological Health. Position statement: definition of traumatic brain injury. Arch Phys Med Rehabil. 2010;91(11):1637–1640. | ||
Bhardwaj A, Bhagat H, Grover VK. Jugular venous oximetry. J Neuroanaesthesiol Crit Care. 2015;2:225–231. | ||
Wijdicks EF, Bamlet WR, Maramattom BV, Manno EM, McClelland RL. Validation of a new coma scale: The FOUR score. Ann Neurol. 2015;58:585–593. | ||
Haddad SH, dan Arabi YM. Critical care management of severe traumatic brain injury in adults. Scand J Trauma Resuc Emerg Med. 2012;20:12. | ||
Schell RM, Cole DJ. Cerebral monitoring: jugular venous oximetry. Anesth Analg. 2000;90(3):559–566. | ||
Senapathi TG, Wiryana M, Aribawa IG, Ryalino C. Bispectral index value correlates with Glasgow Coma Scale in traumatic brain injury patients. Open Access Emerg Med. 2017;9:43–46. | ||
Jalali R, Rezaei M. A comparison of the Glasgow Coma Scale score with Full Outline of Unresponsiveness Scale to predict patients’ traumatic brain injury outcomes in intensive care units. Crit Care Res Pract. 2014;2014:4. Article ID 289803. | ||
Sharf MS, El-Gebali MA. Correlation between Glasgow Coma Scale and jugular venous oxygen saturation in severe traumatic brain injury. Egypt J Anesth. 2013;29(3):267–272. | ||
Gopinath SP, Robertson CS, Contant CF, et al. Jugular venous desaturation and outcome after head injury. J Neurol Neurosurg Psychiatry. 1994;57(6):717–723. | ||
Cormio M, Valadka AB, Robertson CS. Elevated jugular venous oxygen saturation after severe head injury. J Neurosurg. 1999;90(1):9–15. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.