Back to Journals » International Medical Case Reports Journal » Volume 18
Isotretinoin – Induced AGEP: A Case Report
Authors Alotaibi HM ![]() , AlNasser S
, AlNasser S ![]() , Aldossari A
, Aldossari A ![]() , Alluhaybi A, Alsergani R, Alrajban W
, Alluhaybi A, Alsergani R, Alrajban W
Received 15 August 2024
Accepted for publication 22 January 2025
Published 1 February 2025 Volume 2025:18 Pages 211—215
DOI https://doi.org/10.2147/IMCRJ.S488180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Hend M Alotaibi,1 Sultan AlNasser,1 Abdulelah Aldossari,2 Abdulrahman Alluhaybi,1 Reem Alsergani,1 Waleed Alrajban1
1Department of Dermatology, College of Medicine, King Saud University and King Saud University Medical City (KSUMC), Riyadh, Saudi Arabia; 2Department of Dermatology, King Fahad Specialist Hospital, Buraydah, Saudi Arabia
Correspondence: Sultan AlNasser, Email [email protected]
Abstract: Acute Generalized Exanthematous Pustulosis (AGEP) is a relatively rare but severe dermatological adverse reaction characterized by the rapid onset of generalized erythema, coupled with numerous sterile nonfollicular pustules. Agents commonly implicated in triggering AGEP include antibiotics, antifungals, antimalarials, and diltiazem. We present a case of a isotretinoin induced AGEP in a young female patient known to have guttate psoriasis, inverse and scalp psoriasis. She was started on Isotretinoin as she had inflammatory acne as well. Three days later, she developed pruritic, erythematous lesions, some vesicles with a yellowish exudate over the armpits, upper chest, upper arms, and legs. A skin biopsy was performed, which, in conjunction with the clinical presentation, was suggestive of AGEP. In 2010, Filho et al described the first case of isotretinoin-induced AGEP in a female patient diagnosed with Hidradenitis Suppurativa. The EuroSCAR tool was utilized to assess the lesion morphology, clinical course, and histological outcomes, which validated the diagnosis. Using the same criteria, our patient was categorized as “definite AGEP”, further supporting the isotretinoin-induced AGEP hypothesis. This report highlights isotretinoin as a possible trigger for AGEP, emphasizing the crucial role of a thorough history and vigilant clinical assessment in early identification and management of such reactions.
Keywords: acute generalized exanthematous pustulosis, isotretinoin, pustular psoriasis, drug reactions
Introduction
Acute Generalized Exanthematous Pustulosis (AGEP) is a relatively rare but severe dermatological adverse reaction, with a reported incidence ranging from 1 to 5 cases per million individuals annually.1
This reaction is characterized by the rapid onset of generalized erythema, coupled with numerous sterile nonfollicular pustules. Significantly, these symptoms often begin to subside after the discontinuation of the offending agent, typically a recently introduced medication.2
Despite AGEP generally being associated with lower morbidity compared to other severe cutaneous adverse reactions, instances of systemic complications such as acute renal insufficiency and hepatitis have been documented, and a mortality rate of less than 5% has been reported.2
Agents commonly implicated in triggering AGEP include antibiotics, antifungals, antimalarials, and diltiazem, with the characteristic eruption of AGEP typically observed within three days of drug administration.1
We present a case of isotretinoin-induced AGEP in a female patient known to have guttate psoriasis.
Case Presentation
A 20-year-old female patient was being managed for guttate, inverse, and scalp psoriasis under dermatological care. The treatment regimen included topical steroids, narrow band UVB phototherapy, methotrexate, none of which showed clinical improvement. Subsequently, she commenced treatment with cyclosporine at a dose of 2.5 mg/kg/day. After one month, the patient exhibited significant clinical improvement but developed flank pain and urinary symptoms, which necessitated the discontinuation of cyclosporine.
Since the patient was also having inflammatory acne, Isotretinoin was then initiated at a dosage of 40 mg daily. Three days later, she developed pruritic, erythematous lesions and some vesicles with a yellowish exudate originating around the armpits and subsequently spreading to the upper chest, upper arms, and legs. These symptoms were accompanied by joint pain and a slight decrease in appetite. The patient denied any recent infection, fever, or development of oral or genital ulcers. There was a familial history of psoriasis in her uncle, but otherwise, no significant family medical history was noted.
Upon physical examination, the patient was vitally and clinically stable Dermatological assessment revealed numerous non follicular pustules and desquamative scales on top of erythematous and edematous plaques distributed from the upper chest to the upper arms and lateral aspects of the trunk bilaterally (Figure 1). Additionally, there were multiple erythematous papules with punctate excoriations on the legs, with sparing of the scalp, face, lower trunk, thighs, genitals, palms, and soles. No lymphadenopathy or involvement of mucous membranes was present.
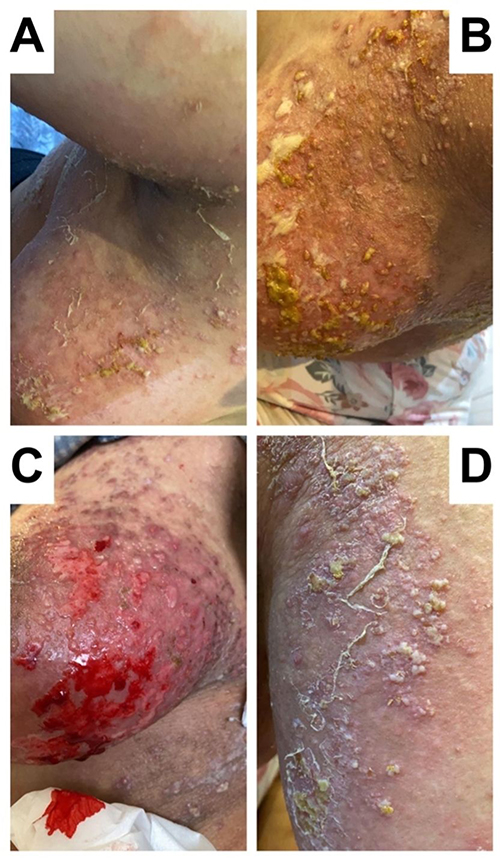 |
Figure 1 (A and B) Follicular pustules and desquamative scales with a background of erythema over the axilla and breast. (C) Eroded pustules over background of erythematous edematous plaque over the breast. (D) Same as A but over the lateral side of the upper back. |
Laboratory investigations indicated an elevated white blood cell count at 15.760 with neutrophilia and eosinophilia. Eosinophil count was 2.52×109 /L and a percentage of 16%. All other laboratory parameters were within normal ranges.
The primary diagnostic consideration was pustular psoriasis of the exanthematic type, likely precipitated by isotretinoin. Differential diagnoses included acute generalized exanthematous pustulosis (AGEP) and subcorneal pustular dermatitis. The treatment plan involved discontinuation of isotretinoin and resumption of cyclosporine at an increased dose of 3 mg/kg/day, split into two doses, along with the application of topical mometasone ointment twice daily on the affected areas for a duration of two weeks.
A skin biopsy from a lesion on the right lower abdomen was performed, which, in conjunction with the clinical presentation, was suggestive of AGEP (Figure 2). The patient’s management plan was adjusted to continue cyclosporine treatment.
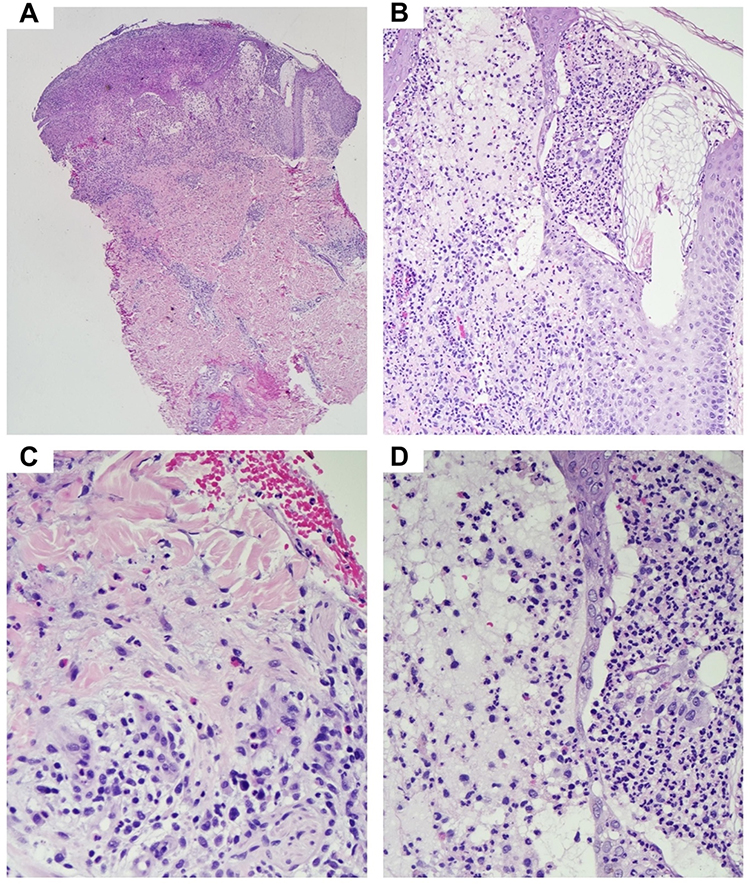 |
Figure 2 (A) At 40x, this punch biopsy clearly demonstrates an epidermal erosion, subcorneal and intraepidermal pustule. In the dermis there is evidence of perivascular infiltrate. (B) At 100x, Subcorneal and intraepidermal neutrophilic infiltrate, spongiosis, and perivascular inflammation is seen with dermal edema (upper left). (C) At 200x, an intradermal neutrophilic pustule is seen, with vacuolar interface dermatitis. A significant number of eosinophils can be seen. (D) At 200x, within the superficial dermis, the perivascular lymphoplasmacytic is appreciated along with scattered eosinophils and neutrophils. |
At the three-week follow-up, the patient presented with a complete resolution of the lesions. Residual post-inflammatory hyperpigmentation was noted on both upper extremities, with no active lesions observed (Figure 3). Eosinophil count after treatment was 0/L.
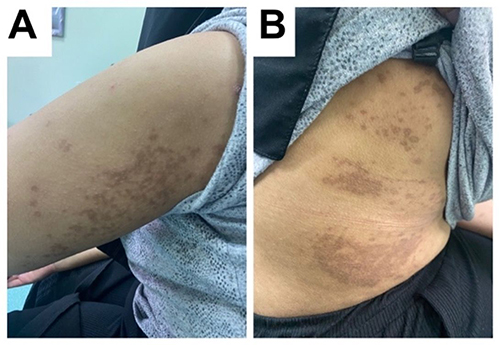 |
Figure 3 (A and B) Post inflammatory hyperpigmented macules and patches over the Upper limb and lateral side of the trunk. |
Discussion
Acute Generalized Exanthematous Pustulosis (AGEP) is primarily drug-induced, as affirmed by a substantial retrospective review of 340 patients, wherein 85% of AGEP cases were attributed to drug reactions.1 The recognized triggers encompass infections, radiocontrast media, and arachnid bites, though many cases remain idiopathic.1,3,4 Despite an exhaustive investigation, our patient did not exhibit any known AGEP etiologies, leading us to propose isotretinoin as the causative agent, a hypothesis supported by the clinical timeline and characteristic eruption.
Isotretinoin, a Vitamin A derivative, has a broad therapeutic spectrum in dermatology, notably in managing psoriasis.5 It modulates cellular differentiation and inflammatory processes, effectively attenuate keratinocyte hyperproliferation.6 While associated with reversible side effects such as xerosis and cheilitis, and serious risks like potential teratogenicity, these adverse effects generally resolve post discontinuation or treatment completion.5 Interestingly, up to this date only one study has reported isotretinoin-induced AGEP.7
In 2010, Filho et al described the first case of isotretinoin-induced AGEP in a female patient diagnosed with Hidradenitis Suppurativa, who developed eruptions after 5 days of isotretinoin initiation. The EuroSCAR tool was utilized to assess the lesion morphology, clinical course, and histological outcomes, which validated the diagnosis. Using the same criteria, our patient was categorized as “definite AGEP”, further supporting the isotretinoin-induced AGEP hypothesis.
One common differential diagnosis that can be confused with AGEP is pustular psoriasis, especially the generalized variant.8 Clinically, it may pose a challenge to differentiate between generalized pustular psoriasis and AGEP due to their overlapping and common presentations. However, laboratory tests and histological examinations can aid in distinguishing between them and confirming the diagnosis. Typically, AGEP is associated with neutrophilia and/or eosinophilia in the blood, and histologically, it presents with spongiform subcorneal and/or intraepidermal pustules, marked papillary edema, and a polymorphous perivascular infiltrate with neutrophils, and some eosinophils.2,8
Interestingly, a positive history of pustular psoriasis tends to favor a diagnosis of Generalized Pustular Psoriasis over AGEP.9 However, in our patient, despite a history of psoriasis, the laboratory tests, histological examinations, and clinical timeline confirmed the diagnosis of AGEP.
Additionally, our patient demonstrated significant peripheral eosinophilia in the blood which indicated a more severe clinical manifestation, a need to start systemic therapy, and a longer recovery time compared to patients without peripheral eosinophilia.10
In conclusion, our case highlights isotretinoin as a possible trigger for AGEP, emphasizing the crucial role of a thorough history and vigilant clinical assessment in early identification and management of such reactions. We recommend vigilant monitoring, immediate discontinuation of the offending drug, and utilizing additional tests to accurately differentiate AGEP from other conditions. This case raises awareness about the potential of isotretinoin to trigger AGEP and stresses the importance of monitoring for rash within the first two weeks of isotretinoin therapy.
Abbreviations
AGEP, Acute Generalized Exanthematous Pustulosis; UVB, Ultraviolet B.
Ethics Approval and Consent to Participate
A written informed consent has been provided by the patient to have the case details and any accompanying images published. Institutional approval was not required to publish the case details.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study did not receive any financial support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Creadore A, Desai S, Alloo A, et al. Clinical characteristics, disease course, and outcomes of patients with acute generalized exanthematous pustulosis in the US. JAMA Dermatol. 2022;158(2):176–183. doi:10.1001/JAMADERMATOL.2021.5390
2. Szatkowski J, Schwartz RA. Acute generalized exanthematous pustulosis (AGEP): a review and update. J Am Acad Dermatol. 2015;73(5):843–848. doi:10.1016/j.jaad.2015.07.017
3. Hammerbeck AA, Daniels NH, Callen JP. Ioversol-induced acute generalized exanthematous pustulosis: a case report. Arch Dermatol. 2009;145(6):683–687. doi:10.1001/ARCHDERMATOL.2009.100
4. Davidovici BB, Pavel D, Cagnano E, Rozenman D, Halevy S. Acute generalized exanthematous pustulosis following a spider bite: report of 3 cases. J Am Acad Dermatol. 2006;55(3):525–529. doi:10.1016/j.jaad.2006.05.010
5. Sbidian E, Maza A, Montaudié H, et al. Efficacy and safety of oral retinoids in different psoriasis subtypes: a systematic literature review. J Eur Acad Dermatol Venereol. 2011;25(SUPPL 2):28–33. doi:10.1111/J.1468-3083.2011.03993.X
6. Beckenbach L, Baron JM, Merk HF, Löffler H, Amann PM. Retinoid treatment of skin diseases. Eur J Dermatol. 2015;25(5):384–391. doi:10.1684/EJD.2015.2544/METRICS
7. Da Cunha Filho RR, De Almeida HL, Lorencette NA, Fillus Netto J. Acute generalized exanthematous pustulosis induced by isotretinoin. Int J Dermatol. 2010;49(9):1077–1079. doi:10.1111/j.1365-4632.2009.04327.x
8. Parisi R, Shah H, Navarini AA, et al. Acute generalized exanthematous pustulosis: clinical features, differential diagnosis, and management. Am J Clin Dermatol. 2023;24(4):557–575. doi:10.1007/S40257-023-00779-3
9. Sussman M, Napodano A, Huang S, Are A, Hsu S, Motaparthi K. Pustular psoriasis and acute generalized exanthematous pustulosis. Medicina. 2021;57(10):1004. doi:10.3390/MEDICINA57101004
10. Drago F, Cogorno L, Agnoletti AF, Ciccarese G, Parodi A. A retrospective study of cutaneous drug reactions in an outpatient population. Int J Clin Pharm. 2015;37(5):739–743. PMID: 26050251. doi:10.1007/s11096-015-0134-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.