Back to Journals » International Medical Case Reports Journal » Volume 18
Isolated Colorectal Involvement in Klippel-Trenaunay Syndrome: A Case of Extensive Vascular Malformation
Authors Ilyassov N ![]() , Shayakhmetov Y, Abdikarimov A, Nurgaliev E, Saberbekov S, Aralbayev R, Tokusheva A, Kalina V
, Shayakhmetov Y, Abdikarimov A, Nurgaliev E, Saberbekov S, Aralbayev R, Tokusheva A, Kalina V
Received 7 May 2025
Accepted for publication 24 July 2025
Published 7 August 2025 Volume 2025:18 Pages 997—1002
DOI https://doi.org/10.2147/IMCRJ.S535985
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Nurbek Ilyassov,1 Yerzhan Shayakhmetov,2 Anuar Abdikarimov,1 Erlan Nurgaliev,1 Saken Saberbekov,1 Rakymzhan Aralbayev,1 Aiman Tokusheva,1 Vitaliy Kalina1
1JSC National Scientific Medical Center, Astana, Kazakhstan; 2International Oncological Tomotherapy Center “YMIT”, Astana, Kazakhstan
Correspondence: Vitaliy Kalina, JSC National Scientific Medical Center, 42 Abylai Khan Avenue, Astana, 010009, Kazakhstan, Tel +7 705 136 1399, Email [email protected]
Background: Rectal vascular malformations associated with Klippel-Trenaunay syndrome are exceedingly rare. While their diagnosis may be straightforward when characteristic features are present, such cases remain of significant educational value due to their unusual presentation and potential for misdiagnosis.
Case Presentation: Our study aimed to describe a clinical case of a 45-year old female patient. There were complaints of pain in the perianal area and periodic bleeding during/after defecation, prolapse of hemorrhoids, general weakness. Colonoscopy revealed varicose veins of the rectum, hemangioma of the rectal mucosa, and chronic internal hemorrhoids. Multislice computed tomography of the pelvic organs with intravenous bolus contrast was performed. The preliminary clinical diagnosis was hemangioma of the rectal mucosa, and vascular malformation of the rectum was considered operable. In our clinic, the patient underwent several-stage surgery: (1) implantation of a temporary vena cava filter into the inferior vena cava, (2) two weeks later laparoscopic-assisted anterior resection of the rectum with preventive transverse colostomy and demucosation of the rectal mucosa, (3) after 7 months following discharge, the closure of transverse colostomy. Pathological examination of the gross specimen revealed that mucous membrane of the colon in a section extending 12.0 cm up to the distal edge of the resection is compacted, coarsely lumpy, grayish-bluish in color, with multiple blood-filled cavities. The postoperative period proceeded smoothly. Oral nutrition and patient’s activity began on the 1st day. Primary healing of postoperative wounds was occurred. The patient was discharged in satisfactory condition on the 6th day post-surgery.
Conclusion: This clinical case is a case-of-interest due to its rare localization, asymptomatic course for a long time with a fairly large size of an excessively vascularized abnormal vascular formation. The appropriate approach to this pathology is laparoscopic surgery, which can be useful for both diagnostic and radical treatment of vascular malformations of the rectum.
Keywords: case report, hemangioma, Klippel-Trenaunay syndrome, rectum, vascular malformation
Introduction
Vascular anomalies occur in diverse clinical presentations. To facilitate their diagnostics, a systematic nomenclature for vascular anomalies has been developed by Mulliken and Glowacki in 1982.1 Later, in 1996, the classification was evolved by taking into account both histological features and hemodynamic responses,2 with further recent update in 2017.3 According to the nomenclature, the vascular anomalies are divided into vasoproliferative neoplasms (highly proliferative in the endothelial cells) and vascular malformations (minimally proliferative endothelium). The groups are also distinct by their structural features and functional responses to altered hemodynamics.3 For example, vascular anomalies have distinct structural defects in venous, lymphatic, capillary, or arteriolar vessels.4 The diversity of clinical representation of vascular malformations that can have different pathophysiological origins strongly impacts the quality and correctness of diagnostics and corresponding curative treatments.
Congenital vascular malformations of the rectum are very rare in Klippel-Trenaunay syndrome while if present, the characteristic features can facilitate associating them to the syndrome.5–8 Thus, the isolated malformations in superficial vena occur more commonly in the syndrome, as well as the common clinical representation includes portwine coloring, ectatic superficial veins that have normal or absent deep veins, and limb hypertrophy.9 In extremely rare cases, the syndrome can involve also genitourinary and pelvic vascular system.10,11 Generally, the hypertrophy of unilateral lower limb or, more seldom, bilateral lower limbs is presented;12–14 however, the remarkably expressed undergrowth of the affected limb has also been reported.14 At the same time, it is extremely rare that the Klippel-Trenaunay syndrome is not accompanied by clinically, morphologically, or functionally discernible abnormalities in the limbs.
This case report describes an unusual presentation of Klippel-Trenaunay syndrome with isolated rectal involvement but without the typical limb abnormalities. The results of multislice computed tomography (MSCT) with intravenous contrast of the pelvis allowed us to interpret the vascular malformation of the rectum, as well as the complete picture of the pelvis. The peculiarity of the clinical case is that this pathology occurs very rarely and it has appeared for the first time in the practice of our clinic.
Case Presentation
The patient was a woman aged 45 years, Caucasian. There were complaints to the pain in the perianal area during defecation, periodic bleeding after defecation, prolapse of hemorrhoids, general weakness, and malaise. From the medical history it was revealed that the patient considers herself sick since childhood, when she was diagnosed with “chronic hemorrhoids” and hemorrhoidectomy was performed. Subsequently, the patient did not seek medical help, was not treated or examined. Subsequent exacerbation in the form of intestinal bleeding and identification of hemorrhoidal problems, including a suspected rectal hemangioma, required emergent medical care and blood transfusion therapy. In June 2022, she was urgently hospitalized with an intestinal bleeding. Haemoglobin level was 45 g/l. Colonoscopy examination revealed an increase in the vascular pattern at 10.0 cm from the anus, with the expansion of the vein trunks to 0.5–0.6 cm (Figure 1A). There was a polyp-like formation on a wide stalk at 7.0 cm from the anus, above one of the trunks, 0.5–0.5 cm in size, bluish in color, circular-like narrowing of the rectal hole (Figure 1B). The colonoscopy conclusions were as follows: dolichocolon, internal hemorrhoids (degree II), rectal hemangioma(?). Colonoscopic examination revealed not only vascular pathology, but also other changes in the structure of the rectum, which required a more detailed diagnostic and therapeutic approach. In September 2023, the patient contacted JSC National Scientific Medical Center (JSC NSMC) and was hospitalized in the department of general and thoracic surgery. The colonoscopy protocol concluded that starting from the anal ring, the vascular patterns are pronounced to 10 cm, injected in places, hemangiomas with a diameter of up to 0.8–1.0 cm are detected, with smooth surfaces, which are easily injured and can be accompanied by heavy bleeding that is difficult to stop. At the exit, upon retroflexion of the rectal ampulla in typical places, the hemorrhoids are not enlarged and sized to 0.9 cm, the mucous membrane above them is pink and thickened. The diagnosis was varicose veins of the rectum, hemangioma of the rectal mucosa, and chronic internal hemorrhoids (Figure 1).
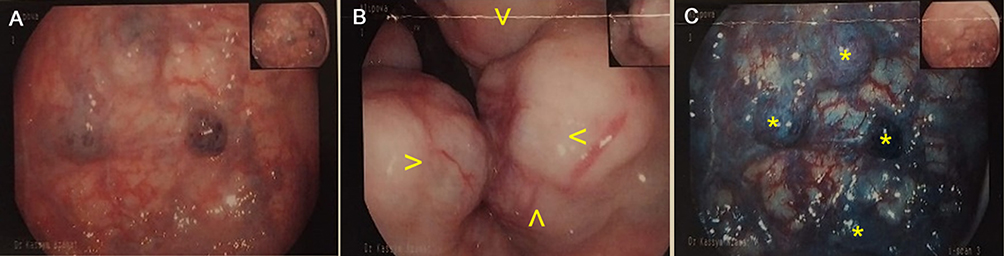 |
Figure 1 Colonoscopy images. (A) A general view of the rectum showing an increase in the vascular pattern with expansion of the vein trunks in the submucosal layer. (B) A polyp-like formation on a wide stalk in the rectum, with circular-like narrowing of the rectal hole as indicated by the yellow arrowheads. (C) Intravenous bolus contrast in the arterial and venous phases shows uneven accumulation of the contrast agent in this formation of the rectum, with signs of blood supply from the pararectal and parametrial vessels (shown by yellow asterisks). |
MSCT of the pelvic organs revealed that in the projection of the rectum, a formation (obstructing the intestinal lumen) is visualized, irregularly shaped, measuring 73×53 mm, with clear and uneven internal contours, density up to +23H, inhomogeneous structure due to foci of calcification. With intravenous bolus contrast in the arterial and venous phases, uneven accumulation of the contrast agent was observed in this formation of the rectum, with a density from +95H to +279H, with signs of blood supply from the pararectal and parametrial vessels (Figure 1C). Single defects of varicose veins of the uterus are differentiated due to thrombosis. It was concluded that there is a CT picture of rectal formation (hemangioma or cancer) with chronic cystitis (Figure 2, shown by arrowheads in panels B, C, and F).
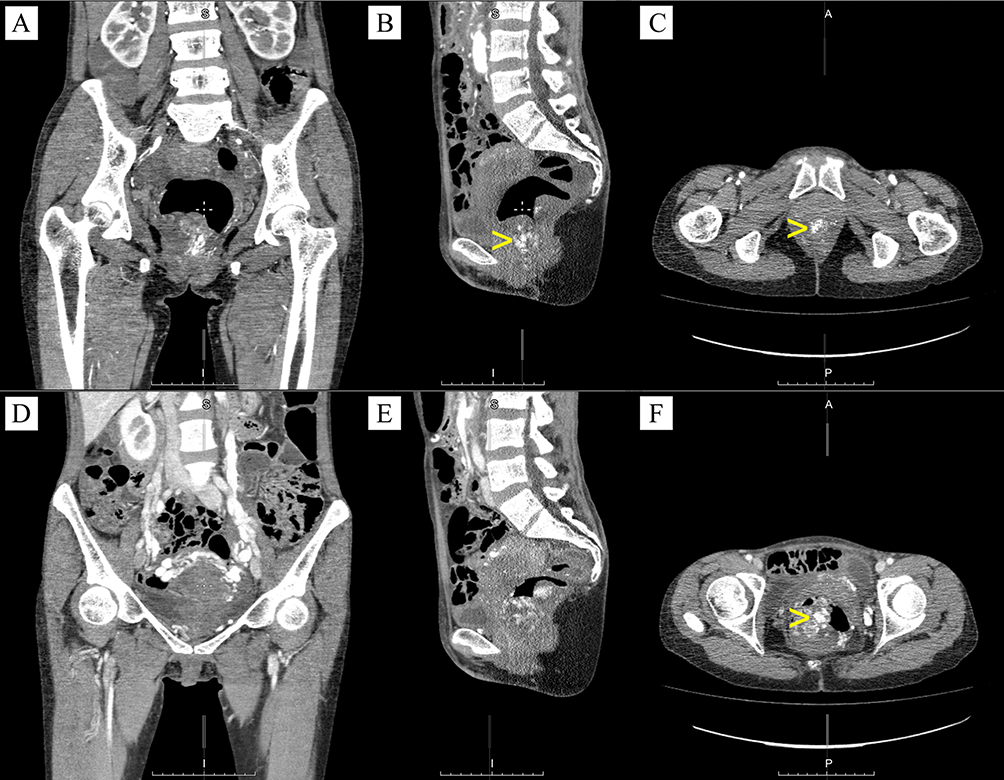 |
Figure 2 Multislice computed tomography of the pelvic organs with intravenous bolus contrast in the arterial and venous phases. Uneven accumulation of the contrast agent is observed in the formation of the rectum (shown by yellow arrowheads in panels B, C, and F), and single defects of varicose veins of the uterus are differentiated. Top panels: arterial phase – anterior view (A), lateral view (B), dorsal view (C). Bottom panels: venous phase – anterior view (D), lateral view (E), dorsal view (F). |
The preliminary clinical diagnosis was hemangioma of the rectal mucosa. In this case, vascular malformation of the rectum was considered resectable According to MSCT data of the pelvic organs, there are varicose veins of the uterus due to thrombosis with a high risk of rupture, which can lead to pulmonary embolism, and therefore it was decided to perform several stages of surgery on the patient. The first stage was the implantation of a temporary vena cava filter into the inferior vena cava. Two weeks later, laparoscopically-assisted anterior resection of the rectum with preventive transverse colostomy and demucosation of the rectal mucosa were performed as the second stage. Seven months later, the closure of the transverse colostomy was performed as the third stage.
During examination of the gross specimen, it was revealed that mucous membrane of the colon in a section extending 12.0 cm up to the distal edge of the resection is compacted, coarsely lumpy, grayish-bluish in color (Figure 3A), with multiple blood-filled cavities in the section (Figure 3B). A neoplasm within the mucous and submucosal layers was observed, represented by compactly located cavities of the vascular type with a flattened endothelial lining, containing thrombotic masses, with multiple hemorrhages along the periphery.
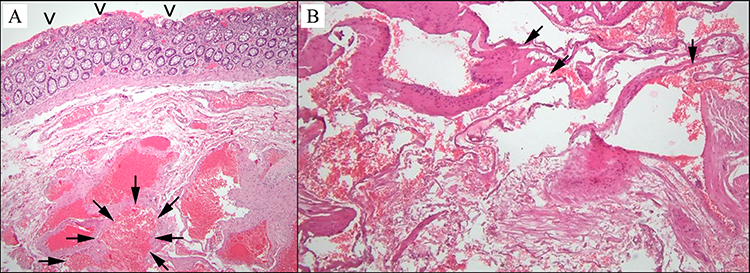 |
Figure 3 Microscopic views of preparations of the rectum. A neoplasm within the mucous and submucosal layers is observed, represented by compactly located cavities of the vascular type with a flattened endothelial lining, containing thrombotic masses, with multiple hemorrhages along the periphery. (A) The upper part of the image is the mucous layer of the colon (shown by arrowheads), in the central part there is a formation located in the submucosal layer (shown surrounded by arrows), represented by capillary-type vessels of different calibers with a flattened endothelial lining. (B) Multiple vessels in the form of cavities are observed (as shown by arrows). |
The postoperative period proceeded normally. Oral nutrition and patient’s activity began on the 1st day. No infusion adjustment was required. Primary healing of postoperative wounds was occurred. The patient was discharged in satisfactory condition on the 6th day after surgery. After 7 months, the third stage of the operation – the closure of the transverse colostomy – was performed. The follow-up of the patient for physical observation and assessment of long-term changes was not available because of inaccessibility of the patients (living in a distant region).
Discussion
The characteristic triad of features for Klippel-Trenaunay Syndrome includes capillary malformation with port-wine stain, venous malformations, and limb overgrowth.9,12–14 The hypotrophic limb can also occur but much rarely.14 The syndrome can affect other organs and systems, eg genitourinary, gastrointestinal, and pelvic vasculature, but the incidence for these cases is low.9–11 However, in extremely rare cases, the multi-organ lesions can also be observed.9 Vascular malformations of the rectum are very rare complications observed in Klippel-Trenaunay Syndrome; however, several published reports are available.15–17
To date, there is no unified strategy for treating patients with this pathology, but surgical treatment is the only radical method.5 Our case emphasizes the importance of promptly consulting a doctor in case of any unpleasant or suspicious symptoms, especially with chronic diseases. In turn, the diagnostic approach must be carefully selected prior to the choice of treatment.18 In our case, we used multi-slice computed tomography with intravenous bolus contrast in combination to colonoscopy to verify the rectal vascular lesions. Others reported similar approaches, including colonoscopy, visceral angiography (venography), and magnetic resonance imaging.5,15–17 An integrated approach to the diagnosis and treatment of vascular malformations of the rectum requires high qualifications and modern equipment, which is available in specialized medical institutions.18 In some circumstances, the lack of experienced personnel or specialized facility prevents surgical treatment, leaving only the option for conservative treatment.17 In addition, such patients may require long-term follow-up even if they demonstrated positive short-term post-operative outcome.
The presented clinical case is of a special interest due to its rare localization and asymptomatic course for a long time with fairly large size of an excessively vascularized abnormal lesion. Our decisive criterion for diagnosing hemorrhoids according to Klippel-Trenaunay Syndrome (and not just “ordinary” chronic hemorrhoids) was the pathomorphological confirmation of excessive development of cavernous tissue of the venous plexuses of the rectum, with pronounced angiomatous transformation and arteriovenous shunts. The following factors also reinforced our decision: ineffectiveness of standard methods (sclerotherapy, ligation), recurrent massive bleeding, angiomatous structure of the nodes as revealed by histology after surgery and biopsy, and angiography-confirmed presence of pathological vascular plexuses. This case highlights the importance of regular medical monitoring, even in asymptomatic patients, and adherence to specialist recommendations to perform early diagnosis, prevent complications, and improve the quality of life of patients.
Conclusions
Rectal vascular malformations in Klippel-Trenaunay Syndrome are rare and therefore may have strong negative outcomes in case if diagnosed improperly or not treated timely. The correct approach to the treatment of vascular malformations of the rectum is laparoscopic surgery, which can be useful for both diagnostic and radical treatment of vascular malformations of the rectum. The data of histological examination totally confirmed the diagnosis.
Patient’s Perspective
In the described case, the patient was provided with high-tech medical care. The patient agreed with the treatment plan before the surgery, was satisfied with all the treatments, had no complications, and did not express any complaints in regards to the treatment-related financial costs.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study has received ethical approval of a local ethical board of the National Scientific Medical Center. The institutional consent form for participation in publication was approved by the local ethical board. All methods and treatments were performed in accordance with the relevant guidelines and regulations.
Consent for Publication
Written informed consent for publication was obtained from the patient.
Acknowledgments
Authors thank Dr. Oleg Lookin (JSC National Scientific Medical Center) for his help with preparation and editing of the manuscript. This paper is available as a preprint on Heliyon at: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4953482.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any funding.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Mulliken JB, Glowacki J. Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg. 1982;69(3):412–422. doi:10.1097/00006534-198203000-00002
2. Mulligan PR, Prajapati HJ, Martin LG, Patel TH. Vascular anomalies: classification, imaging characteristics and implications for interventional radiology treatment approaches. Br J Radiol. 2014;87(1035):20130392. doi:10.1259/bjr.20130392
3. Steiner JE, Drolet BA. Classification of Vascular Anomalies: an Update. Semin Intervent Radiol. 2017;34(3):225–232. doi:10.1055/s-0037-1604295
4. Fernandez-Flores A, Cassarino D, Colmenero I. Vascular malformations: a histopathologic and conceptual appraisal. Actas Dermosifiliogr. 2023;114(3):213–228. doi:10.1016/j.ad.2022.10.035
5. Wang H, Lin W, Xie C, Yang W, Zhou J, Guo Z. Gastrointestinal involvement in Klippel-Trénaunay syndrome: pathophysiology, evaluation, and management. Orphanet J Rare Dis. 2023;18(1):288. doi:10.1186/s13023-023-02857-5
6. Wang H, Lin W, Guo Z. Klippel-Trenaunay syndrome with gastrointestinal involvement and portal hypertension-evaluation and management. Dig Liver Dis. 2022;54(10):1455–1457. doi:10.1016/j.dld.2022.04.005
7. Wang H, Lin W, Guo Z. Klippel-Trenaunay syndrome with anorectum involvement and portal hypertension. Pediatr Int. 2022;64(1):e15165. doi:10.1111/ped.15165
8. Han L, Chen S, Jiang S. Gastrointestinal bleeding with Klippel-Trenaunay syndrome: a case report. BMC Gastroenterol. 2021;21(1):315. doi:10.1186/s12876-021-01891-6
9. Wang Z, Wang X, Zhao Q, et al. Klippel-Trenaunay syndrome with multiorgan vascular involvement and gastrointestinal bleeding: a case report and literature review. Medicine. 2025;104(8):e41634. doi:10.1097/MD.0000000000041634
10. Shaikh OH, Kumbhar US, Jain A, Chakkalakkoombil SV. Klippel-Trenaunay syndrome in a young patient with the involvement of gastrointestinal and genitourinary tracts: an unusual and rare presentation. BMJ Case Rep. 2021;14(3):e239420. doi:10.1136/bcr-2020-239420
11. Wang H, Xie C, Lin W, Zhou J, Yang W, Guo Z. Internal iliac vein reflux: an underrecognized pathophysiology in Klippel-Trénaunay syndrome with pelvis involvement. Cureus. 2022;14(1):e21472. doi:10.7759/cureus.21472
12. Karmacharya RM, Vaidya S, Bhatt S, et al. Klippel-Trenaunay syndrome: case series from a university hospital of Nepal. Ann Med Surg. 2022;78:103732. doi:10.1016/j.amsu.2022.103732
13. Arasu A, Khalil-Khan A, G KI, Raju E, Gunasekaran L, Sathiamoorthy R. A rare case of Klippel-Trénaunay syndrome. Cureus. 2022;14(10):e30128. doi:10.7759/cureus.30128
14. Brandigi E, Torino G, Messina M, et al. Combined capillary-venous-lymphatic malformations without overgrowth in patients with Klippel-Trénaunay syndrome. J Vasc Surg Venous Lymphat Disord. 2018;6(2):230–236. doi:10.1016/j.jvsv.2017.09.011
15. Cheon SH, Lee SH, Park EB. Rectal Involvement of Klippel-Trenaunay syndrome. J Korean Soc Coloproctol. 2009;25(1):52–55. doi:10.3393/jksc.2009.25.1.52
16. Kim HY, Chang YW, Lee DH. Rectal and splenic vascular malformation in Klippel-Trenaunay-Weber syndrome: a case report. J Korean Soc Radiol. 2012;67(4):289–292. doi:10.3348/jksr.2012.67.4.289
17. Pranta TA. A case of Klippel-Trenaunay syndrome with gastrointestinal hemorrhage and splenomegaly. Cureus. 2024;16(11):e74371. doi:10.7759/cureus.74371
18. Asghar F, Aqeel R, Farooque U, Haq A, Taimur M. Presentation and management of Klippel-Trenaunay syndrome: a review of available data. Cureus. 2020;12(5):e8023. doi:10.7759/cureus.8023
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.