Back to Journals » Patient Preference and Adherence » Volume 10
Is it appropriate regarding patient preference to take Myrtol standardized enteric-coated soft capsules after a meal rather than at fasted state? A food–drug pharmacokinetic interaction study in healthy Chinese volunteers
Authors Zhao TT, Zhu LL, Chen M, Zhou Q ![]()
Received 9 July 2016
Accepted for publication 13 September 2016
Published 3 October 2016 Volume 2016:10 Pages 2031—2037
DOI https://doi.org/10.2147/PPA.S116823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Ting-Ting Zhao,1 Ling-Ling Zhu,2 Meng Chen,1 Quan Zhou1
1Department of Pharmacy, 2VIP Care Ward, Division of Nursing, The Second Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang Province, People’s Republic of China
Background: According to prescribing information for Myrtol standardized enteric-coated soft capsules, the medicine should be taken on an empty stomach. Some patients may experience stomach discomfort after oral administration in fasted state and would prefer to take the medicine after a meal. However, there is no literature addressing the effect of meal on absorption of this drug; therefore, it is desirable to explore the feasibility of taking the capsule after a meal from pharmacokinetic perspective.
Methods: A gas chromatography coupled with triple quadruples mass spectrometry assay was established and validated for determining plasma concentrations of eucalyptol, a target component of Myrtol standardized capsules. A self-control clinical study was carried out in healthy male volunteers in fasted and fed states after a single oral dose of 300 mg capsules. Comparison of pharmacokinetic parameters in the two phases and bioequivalence evaluation were performed.
Results: The specificity, sensitivity, accuracy, and precision of the assay satisfied the requirements for biopharmaceutical analysis. Pharmacokinetic parameters of eucalyptol (fasted vs fed) were as follows: maximal plasma concentrations (Cmax) (167.60±114.69 vs 518.89±314.47 ng·mL-1), time of maximum concentration (Tmax) (3.7±1.1 vs 4.8±0.7 h), elimination half-life (T1/2) (3.2±1.4 vs 2.6±0.7 h), area under the plasma concentration–time curve (AUC0–t) (584.91±369.90 vs 1,271.61±605.82 ng·h·mL-1), and AUC0–∞ (690.36±467.26 vs 1,458.02±720.21 ng·h·mL-1). There was statistically significant difference in Cmax, AUC0–t, and AUC0–∞ between the two dosing methods (P<0.05). Pharmacokinetic parameters of eucalyptol given in fasted state in Chinese were comparable to those in Germany population. The 90% confidence intervals for the ratio of Cmax (18.4%~64.7%), AUC0–t (28.9%~68.5%), and AUC0–∞ (31.1%~68.4%) values for the test (fasted) and reference (fed) were beyond the Food and Drug Administration’s acceptable range of 80%~125%. In addition, significant difference was obtained in Tmax (P<0.05).
Conclusion: Compared with dosing at fasted state, taking Myrtol standardized capsules after a meal achieves a delayed absorption rate and an increased absorption extent. The two dosing methods were not bioequivalent in this small study and, thus, not interchangeable. Patient preference and pharmacokinetic food–drug interaction issue should be balanced. Further clinical study is necessary to explore the clinical outcome of oral administration of Myrtol standardized capsules after or with meal.
Keywords: dosing method, eucalyptol, food-drug interaction, gas chromatography mass spectrometry, GC-MS, patient preference, bioequivalence, herb
Introduction
Administration of medicines at mealtimes may result in food–drug interactions. Physicians and patients should be aware of the potential consequences of toxicity or decreased efficacy that might result from medication administration regardless of the effect of food or variations in diet.1–3 According to Joint Commission International (JCI) Accreditation Standards for Hospitals (5th Edition), hospitals should use standardized materials and processes in educating patients on potential interactions between prescribed medications and other medications or food. Also, actual or potential interaction between the medications and food is one of the elements in appropriateness review of medication prescriptions or orders prior to dispensing.4
Myrtol standardized (Gelomyrtol forte) is a phytotherapeutic extract indicated for the treatment of acute and chronic bronchitis and sinusitis.5,6 It enhances mucociliar clearance and has muco-secretolytic activity. Also, it has additional anti-inflammatory and antioxidation effects on alveolar macrophages in patients with chronic obstructive pulmonary disease.7 According to prescribing information for Myrtol standardized capsules, the drug should be taken half an hour before mealtime without chewing.8 However, there is no literature addressing the effect of meal on absorption of this drug. Gelomyrtol forte is of large size, and some patients may experience stomach discomfort after oral administration in fasted state and would prefer to take the medicine after a meal. However, there is no literature addressing the effect of meal on absorption of this drug; therefore, it is desirable to explore the feasibility of taking capsules after a meal from pharmacokinetic perspective.
Myrtol standardized mainly consists of three monoterpenes: eucalyptol (also named as 1,8-cineole), d-limonene, and (+)alpha-pinene, the relative content of each component being 46.35%, 36.83%, and 14.70%, respectively.9 A pharmacokinetic food–drug interaction study was conducted in Chinese subjects, and alternations in eucalyptol pharmacokinetics as a marker of indicating the effect of meal on the bioavailability of Myrtol standardized enteric-coated soft capsules was analyzed. A gas chromatography coupled with triple quadruples mass spectrometry (GC/MS/MS) technology was developed and utilized to determine eucalyptol plasma concentrations.
Materials and methods
Chemicals and solutions
Reference eucalyptol (lot number 110788-201105) was purchased from Beijing Jiuhe Pharmaceutical Co., Ltd. (Beijing, People’s Republic of China). Internal standard (IS) was linalool (lot number 1503-200001, National Institute for the Control of Pharmaceutical and Biological Products, Beijing, People’s Republic of China). Chemical structures of eucalyptol and IS were illustrated in Figure 1. Myrtol standardized enteric-coated soft capsules (lot number 238794; G Pohl-Boskamp GmbH & Co. KG, Schleswig-Holstein, Germany) were provided by The Second Affiliated Hospital, School of Medicine, Zhejiang University. Blank human plasma was obtained from volunteers at the Blood Center of Zhejiang Province (Hangzhou, People’s Republic of China). All other chemicals and reagents were of analytical grade and were used without further purification.
 | Figure 1 Chemical structures of eucalyptol and linalool (internal standard). |
The standard substances were dissolved in hexane, and stock solutions were prepared. The concentrations of stock solutions of eucalyptol and IS were 8.11 and 14.2 mg/mL, respectively. Working standard solutions of eucalyptol (10 μg/mL) and IS (10 μg/mL) were prepared by dilution in hexane.
GC/MS/MS
GC/MS/MS was performed on an Agilent 7890B gas chromatograph equipped with a multimode inlet, an HP-5MS capillary column (30 m, 0.25 mm, df 0.25 μm) and an Agilent 7000C Triple Quadrupole GC/MS (Agilent Technologies Inc., Santa Clara, CA, USA). The carrier gas was high-purity helium (99.999%) at a constant rate of 1.0 mL/min. An amount of 1 μL was injected in split mode with injector temperature at 200°C and a 20:1 split ratio. The transfer line to the ion source was held at 280°C. Mass spectrometric analysis was performed in the electron ionization mode at 70 eV and multiple reaction monitoring (MRM) acquisition mode which monitored the transitions of the precursors to the product ions as follows: m/z 154→84 for eucalyptol and m/z 136→121 for the IS.
Sample preparation
Plasma eucalyptol concentrations were determined by GC/MS/MS. Briefly, plasma samples (100 μL) were placed in Eppendorf tube, mixed with 10 μL of the working solution of the IS (10 μg/mL) and 100 μL of hexane. The samples were shaken and centrifuged at 735 × g at 4°C for 10 min. The supernatant was directly taken for the GC/MS/MS analysis.
Clinical study design
This was a two-period self-control clinical study, with a 1-week washout period between each study phase. The study conformed to the guidelines of the Declaration of Helsinki – Tokyo for humans. The protocol was approved by the Ethics Committee of the Second Affiliated Hospital of Zhejiang University (Zhejiang, People’s Republic of China) and Chinese Clinical Trial Register (registration number: ChiCTR-IPR-15005849).
Subjects
Twelve healthy male Chinese volunteers took part in this study. The demographic characteristics of the participants were as follows: body weight (63.8±7.3 kg), height (172.8±5.9 cm), body mass index (21.4±1.5 kg/m2), and age (26.6±3.4 years). As mentioned in our previous paper/earlier study,10 all the volunteers gave their written informed consent. They were judged to be healthy through medical history inquiry, physical examination, electrocardiographic examination, and laboratory tests (eg, complete blood count, blood biochemistry testing, and urinalysis) before enrolling in the study. Participants were excluded for the following reasons: any significant medical history; history of any localized or systemic infections within 4 weeks before admission; use of prescription or over-the-counter medication or alcohol within 2 weeks before enrollment; history of smoking, alcohol or drug abuse; and donation of blood within the past 2 months.
Sample collection
All the volunteers were not allowed to take any medications, coffee, and food rich in flavonoids 2 weeks before and during the entire study period. Period 1 (fasted treatment): after a l0-h overnight fast, each volunteer received a single oral dose of Myrtol standardized capsule 300 mg (one capsule) with 200 mL of water. No food was permitted until 4 h after administration of the medication. Water intake was allowed after 2 h of dose; water, lunch, and dinner were given according to a time schedule. A high-fat and high-calorie diet made of protein (about 150 calories), carbohydrates (250 calories), and fat (500–600 calories) was provided and was treated as a standardized meal for food–effect bioavailability study. All the volunteers were under medical supervision at the study site. Blood samples (5 mL) were drawn into Vacutainer™ tubes with K2EDTA from an indwelling catheter in the forearm vein before drug intake and at 0.5, 1, 1.5, 2, 2.5, 3, 3.5, 4, 4.5, 5, 6, 8, 12 h after the administration of medication. Blood samples were immediately placed on ice bath and centrifuged at 3,000 × g at 4°C for 10 min. Plasma separation from blood was stored in polypropylene tube at −80°C until assay. After 1-week washout, the participants fasted for the same amount of time (10 h) for period 2 (fed treatment) as they did for period 1. Each participant consumed identical and standardized meal within 30 min and then received a single oral dose of Myrtol standardized capsule 300 mg (one capsule) with 200 mL of water 30 min after the meal began. The blood sample collection method in the second phase was identical to that in the first phase. Post-study, electrocardiogram, and biochemical and hematological laboratory tests were carried out to identify any clinical abnormalities.
Statistics
As mentioned in our previous study,10 pharmacokinetic parameters were calculated by using drug and statistics software (version 2.1.1, Mathematical Pharmacology Professional Committee, Shanghai, People’s Republic of China) with noncompartmental method. Maximal plasma concentrations (Cmax) and the times at which they occurred (Tmax) were determined by inspection of the plasma concentration–time profile. The terminal elimination rate constant (λz) was determined by linear regression of the terminal portion of the log concentration–time profile. The elimination half-life (T1/2) was calculated as 0.693/λz. Area under the plasma concentration–time curve (AUC) was determined by trapezoidal rule and was extrapolated to infinity by using the calculation of Ct/λz. F = [AUC0–t (fasted)/AUC0–t (fed)] ×100%. Log transformed, Cmax, AUC0–t, and AUC0–∞ were analyzed using analysis of variance analysis and Schuirmann two one-sided t-test. Tmax was analyzed by the nonparametric test, Wilcoxon’s test. If eucalyptol in the two phases was bioequivalent, 90% confidence interval (CI) value for test (fasted)/reference (fed) ratios of Cmax, AUC should fall within the range of 75%–133% and 80%–125%, respectively. The pharmacokinetics of eucalyptol between the two phases were compared to each other using a paired two-sample t-test (two-tailed). Data were presented as mean ± standard deviation. A P-value of <0.05 was judged to be statistically significant.
Results
Validation of GC/MS/MS assay
The assay method was specific. Determination of eucalyptol and IS was not interfered by endogenous chemicals. Retention times for eucalyptol and IS were 3.3 and 4.3 min, respectively. The total analysis time was 7 min. The MRM chromatograms were illustrated in Figure 2. The calibration curves were linear in the range of 1~1,000 ng/mL, with the lowest limit of quantitation (LLOQ) of 1 ng/mL (n=5, relative standard deviation =10.8%). The within- and between-day coefficient of variation of quality control (QC) samples at high (500 ng/mL), medium (100 ng/mL), and low (10 ng/mL) concentrations were all <10%. The average method recoveries for low, medium, and high concentrations were 109.0%±4.2%, 102.4%±2.62%, and 98.4%±1.0%. The average absolute recoveries for low, medium, and high concentrations were 94.0%±4.11%, 93.3%±3.36%, and 96.4%±3.75%, respectively. The stability of eucalyptol in plasma was confirmed by three studies (20 days stability at −20°C, three freeze-thaw cycles, and 24 h autosampler stability of QC samples), with recoveries being 90.7%–94.3%, 90.34%–99.86%, and 88.8%–92.2%. The specificity, sensitivity, accuracy, precision, and stability all satisfied the requirement of the pharmacokinetic study.
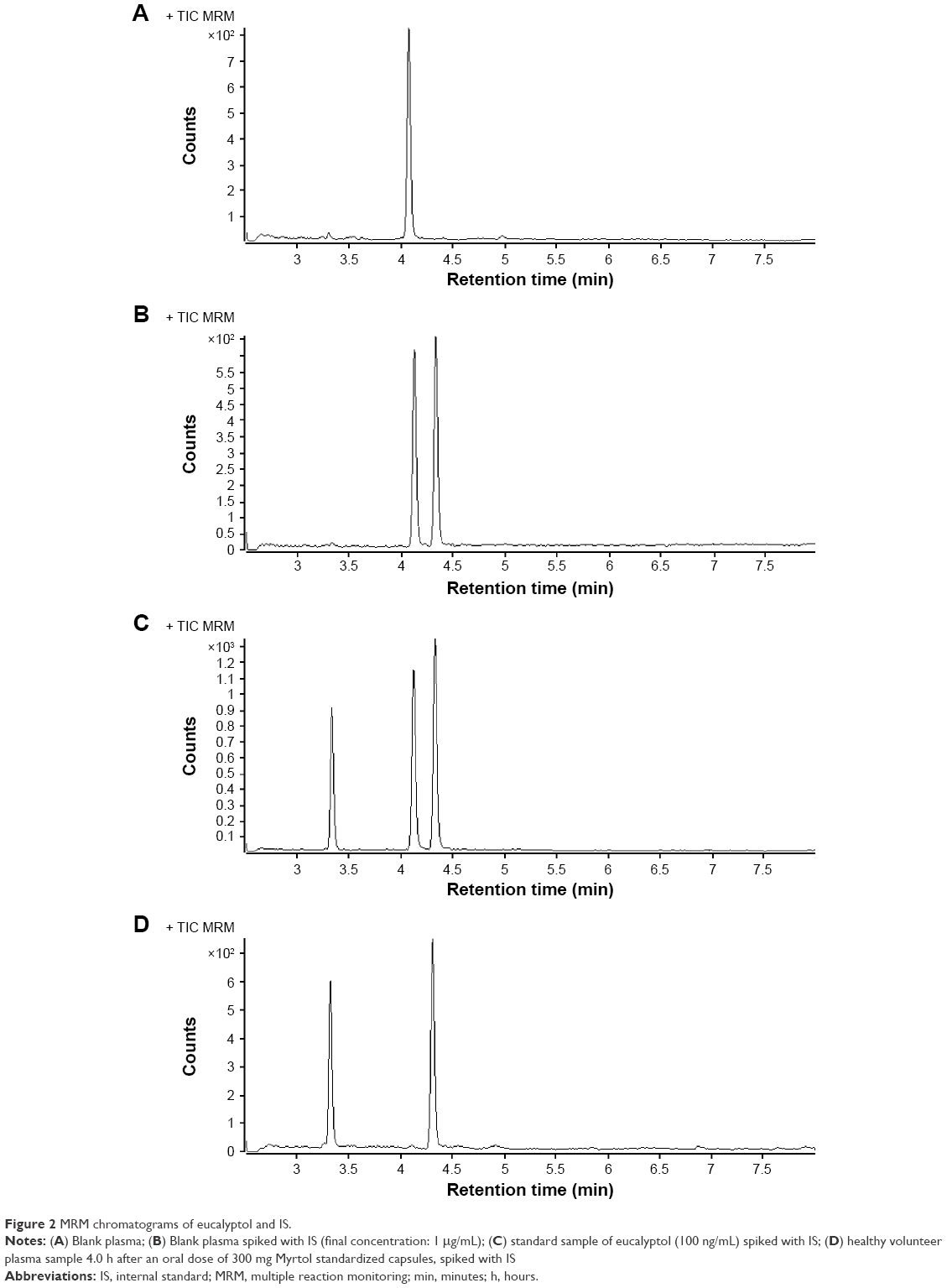 | Figure 2 MRM chromatograms of eucalyptol and IS. |
Concentration–time curves and pharmacokinetics of eucalyptol
The average concentration–time curves were illustrated in Figure 3. The pharmacokinetic parameters of dosing conditions (fasted vs after a meal) were as follows (Table 1): Cmax (167.6±114.69 vs 518.89±314.47 ng·mL−1), Tmax (3.7±1.1 vs 4.8±0.7 h), T1/2 (3.2±1.4 vs 2.6±0.7 h), AUC0–t (584.91±369.90 vs 1271.61±605.82 ng·h·mL−1), and AUC0–∞ (690.36±467.26 vs 1458.02±720.21 ng·h·mL−1). Statistically significant difference was observed in Cmax, AUC0–t, and AUC0–∞ between two dosing methods (P<0.05).
 | Figure 3 Concentration–time curves of eucalyptol after a single oral dose (300 mg) of Myrtol standardized capsules taken at fasted and fed states in 11 Chinese volunteers (mean ± standard deviation). |
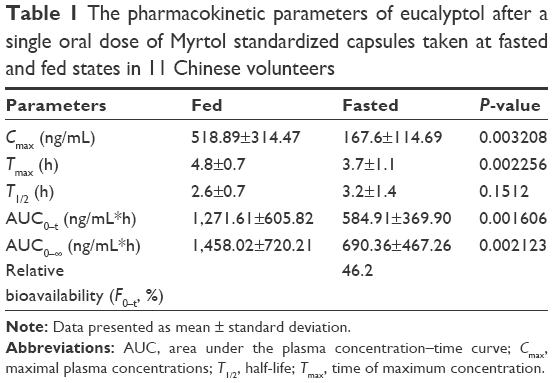 | Table 1 The pharmacokinetic parameters of eucalyptol after a single oral dose of Myrtol standardized capsules taken at fasted and fed states in 11 Chinese volunteers |
Bioequivalence evaluation
The variation sources of P-values and 90% CIs for the parameter ratios were listed in Table 2. Statistically significant formulation (pretreatment) effect was identified, with P<0.05. No statistically significant subject or period effect was encountered. The 90% CI for the ratio of Cmax (18.4%~64.7%), AUC0–t (28.9%~68.5%), and AUC0–∞ (31.1%~68.4%) values for the test (fasted) and reference (after a meal) were beyond the Food and Drug Administration’s acceptable range of 80%~125%. Additionally, Tmax value between two phases exhibited significant difference (P<0.05). The data indicated that eucalyptol was not bioequivalent in the two pretreatment phases.
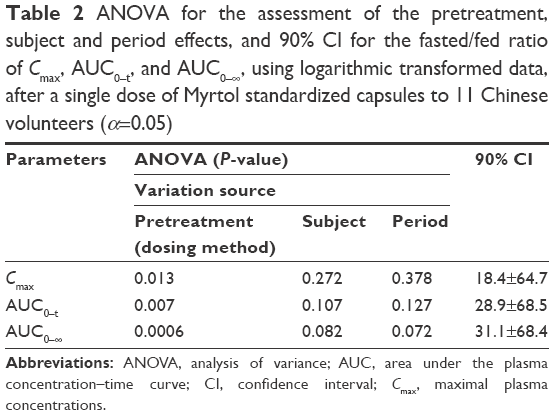 | Table 2 ANOVA for the assessment of the pretreatment, subject and period effects, and 90% CI for the fasted/fed ratio of Cmax, AUC0–t, and AUC0–∞, using logarithmic transformed data, after a single dose of Myrtol standardized capsules to 11 Chinese volunteers (α=0.05) |
Safety
The two dosing methods were well tolerated by the volunteers. No subject experienced any of the expected adverse events at either time period. Also, there was no unexpected incident that could have influenced the outcome of the study. However, one volunteer dropped out at the end of the first phase due to fear of blood samples being drawn. Eleven volunteers completed the trial, and their post-study clinical laboratory tests were normal.
Discussion
Eucalyptol, d-limonene, and (+)alpha-pinene are main active ingredients of Myrtol standardized. The reason to not include the latter two ingredients into our food–drug interaction study may be that eucalyptol was the main active ingredient in plasma, that is, the Cmax values of d-limonene and (+)alpha-pinene were about one-fifth of the value of eucalyptol (30 vs 153.4 ng/mL).11 Horst et al quantified eucalyptol in human blood and urine (LOQ: 2 ng/mL) by solid phase microextraction gas chromatography-ion trap tandem mass spectrometry using stable isotope dilution assays (SIDA-SPME-GC/MS).12 Isotope dilution is classified as a method of internal standardization, and among chemistry measurement methods, it is regarded as the highest metrological standing. However, this technology is unavailable in our laboratory. Zimmermann et al used a gas chromatography with hydrogen flame ionization detector (GC-FID) to determine eucalyptol plasma concentrations in volunteers and observed that median Cmax was 153.4 ng/mL after a single dose of 300 mg Myrtol standardized capsules.11 However, the present study failed to sensitively quantify eucalyptol using the GC-FID assay. GC/MS/MS is a robust, specific, and sensitive assay for the quantification of volatile and semi volatile compounds at trace levels. To the best of our knowledge, the method that was established and validated in this study was the first GC/MS/MS analysis applied in determining human plasma levels of eucalyptol. During the development of the GC/MS/MS, it was observed that MRM mode was more sensitive for eucalyptol than the mode of selected ion monitorings. This analytical method is simpler and more sensitive than the SIDA-SPME-GC/MS assay in terms of LLOQ, time consumed in sample preparation, and isotopically labeled synthesis.
The bioavailability of uncrushed versus crushed Myrtol standardized capsule has been investigated in German population;11 however, the effect of meal on bioavailability of Myrtol standardized has not been addressed. Pharmacokinetic parameters (eg, Cmax, AUC0–t, and AUC0–∞) of eucalyptol given in the fasted state in Zimmermann et al’s study were comparable to the data of present study.11 Moreover, this study first revealed the nonbioequivalence of eucalyptol derived from two different dosing methods (ie, fed and fasted). There was a significant food–drug interaction of Myrtol standard capsules. Meal intake slowed down the absorption rate of eucalyptol but increased the absorption extent (ie, AUC0–t and Cmax values derived from administration at fed state were 2.17 and 3.1 times the values at fasted state). Generally, meals with high total calories and high fat content are more likely to have an impact on the gastrointestinal physiology and could bring a larger effect on the bioavailability of a medicine. Food can alter the bioavailability of a drug substance through various ways (eg, delay gastric emptying, stimulate bile flow and splanchnic blood flow, change gastrointestinal pH and luminal metabolism, physicochemically interact with the dosage formulation or drug ingredients).13 Eucalyptol is part of a large group of aromatic, fat-soluble phytochemicals called terpenes. High-fat (~50% of total caloric content of the meal) meal may enhance the absorption of fat-soluble drugs due to increase in food-induced drug solubility (eg, the solubilization effect by bile micelles).14
Clinicians and patients should be cautious if oral intake of Myrtol standardized enteric-coated soft capsules at empty stomach is switched to oral administration after a meal. If such switch is necessary (eg, patients are uncomfortable after ingestion of the capsules at empty stomach), patients might experience potential augmented drug effects. According to package insert, Myrtol standardized capsules are well tolerant, with very little adverse reactions even in the use of large doses. Adverse drug reactions were as follows: hypersensitivity reactions, gastrointestinal disturbances such as stomach pain or complaints in the upper abdomen, taste alteration, headache, or possible movement of existing kidney stones and gallstones.8 It is worthy to conduct a comparative study to confirm whether non bioequivalence between the two dosing methods would result clinically significant difference in efficacy and safety of Myrtol standardized enteric-coated soft capsules.
Limitations
The present study has some limitations. First, the sample size is not large enough although it meets the China Food and Drug Administration’s requirements on food–drug interaction study, that is, number of subjects should be 10–12 according to Guideline for Pharmacokinetics Study of Chemical Drugs. Second, only the interaction study in the manner of two-period self-control was conducted rather than randomized crossover design. Third, only eucalyptol was treated as target compound in our interaction study despite that it was the main active ingredient of Myrtol standardized in human body. However, this pilot study has attempted to explore the feasibility of taking Myrtol standardized enteric-coated soft capsules after a meal to promote patient adherence as well as enhancing drug efficacy.
Conclusion
Compared with dosing at fasted state, taking Myrtol standardized capsules at fed state could achieve a delayed absorption rate and an increased absorption extent. The two dosing methods were not bioequivalent in this small study and, thus, not interchangeable. Patient preference and pharmacokinetic food–drug interaction issue should be balanced. Further clinical study is necessary to explore the clinical outcome of oral administration of Myrtol standardized capsules after or with meal.
Acknowledgments
This work was supported by Zhejiang Provincial Bureau of Traditional Chinese Medicine (grant 2011ZB075) and Zhejiang Provincial Bureau of Education (grant N20140209). Also, the authors would like to thank Professor Xiao-dan Wu and Professor Ya-er Zhu from Analysis and Testing Center at Zhejiang University, and Professor Jin-liang Chen from Division of Clinical Pharmacol at The Second Affiliated Hospital of Zhejiang University for their kind help with technical support.
Disclosure
The authors report no conflicts of interest in this work.
References
Koch KM, Reddy NJ, Cohen RB, et al. Effects of food on the relative bioavailability of lapatinib in cancer patients. J Clin Oncol. 2009;27:1191–1196. | ||
Ötles S, Senturk A. Food and drug interactions: a general review. Acta Sci Pol Technol Aliment. 2014;13:89–102. | ||
Fleisher D, Li C, Zhou Y, Pao LH, Karim A. Drug, meal and formulation interactions influencing drug absorption after oral administration. Clinical implications. Clin Pharmacokinet. 1999;36:233–254. | ||
Joint Commission International Accreditation Standards for Hospitals. 5th edition. Oak Brook, IL: Joint Commission Resources; 2013. | ||
Matthys H, de Mey C, Carls C, Ryś A, Geib A, Wittig T. Efficacy and tolerability of myrtol standardized in acute bronchitis. A multi-centre, randomised, double-blind, placebo-controlled parallel group clinical trial vs. cefuroxime and ambroxol. Arzneimittelforschung. 2000;50:700–711. | ||
Federspil P, Wulkow R, Zimmermann T. Wirkung von Myrtol standardisiert* bei der Therapie der akuten Sinusitis – Ergebnisse einer doppelblinden, randomisierten Multicenterstudie gegen Plazebo. [Effects of standardized Myrtol in therapy of acute sinusitis – results of a double-blind, randomized multicenter study compared with placebo]. Laryngorhinootologie. 1997;76:23–27. German. | ||
Rantzsch U, Vacca G, Dück R, Gillissen A. Anti-inflammatory effects of Myrtol standardized and other essential oils on alveolar macrophages from patients with chronic obstructive pulmonary disease. Eur J Med Res. 2009;14(Suppl 4):205–209. | ||
GeloMyrtol 300 mg. Available from: http://www.gelomyrtol.ca/pdf/gelomyrtol_patient_information.pdf. Accessed June 12, 2016. | ||
Lou QZ. Chemical constituents analysis of Myrtol standardized by GC-FTIR. Spectrosc Spect Anal. 2007;27:925–927. | ||
Zhou Q, Ye Z, Ruan Z, Zeng S. Investigation on modulation of human P-gp by multiple doses of Radix Astragali extract granules using fexofenadine as a phenotyping probe. J Ethnopharmacol. 2013;146:744–749. | ||
Zimmermann T, Seiberling M, Thomann P, et al. Untersuchungen zur relativen bioverfügbarkeit und zur pharmakokinetik von Myrtol standardisiert. [The relative bioavailability and pharmacokinetics of standardized myrtol]. Arzneimittelforschung. 1995;45:1198–1201. German. | ||
Horst K, Rychlik M. Quantification of 1,8-cineole and of its metabolites in humans using stable isotope dilution assays. Mol Nutr Food Res. 2010;54:1515–1529. | ||
U.S. Department of Health and Human Services. Food and Drug Administration. Center for Drug Evaluation and Research. Food-effect bioavailability and fed bioequivalence studies; December 2002. Available from: http://www.fda.gov/downloads/RegulatoryInformation/Guidances/UCM126833.pdf. Accessed June 12, 2016. | ||
Kawai Y, Fujii Y, Tabata F, et al. Profiling and trend analysis of food effects on oral drug absorption considering micelle interaction and solubilization by bile micelles. Drug Metab Pharmacokinet. 2011;26:180–191. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.