Back to Journals » Vascular Health and Risk Management » Volume 10
Is higher body temperature beneficial in ischemic stroke patients with normal admission CT angiography of the cerebral arteries?
Authors Elnan Kvistad C, Khanevski A, Nacu A, Thomassen L, Waje-Andreassen U, Naess H
Received 4 October 2013
Accepted for publication 19 November 2013
Published 21 January 2014 Volume 2014:10 Pages 49—54
DOI https://doi.org/10.2147/VHRM.S55423
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Christopher Elnan Kvistad,1 Andrej Khanevski,1 Aliona Nacu,1 Lars Thomassen,1 Ulrike Waje-Andreassen,1 Halvor Naess1,2
1Department of Neurology, Haukeland University Hospital, Bergen, Norway; 2Centre for Age-related Medicine, Stavanger University Hospital, Stavanger, Norway
Background: Low body temperature is considered beneficial in ischemic stroke due to neuroprotective mechanisms, yet some studies suggest that higher temperatures may improve clot lysis and outcomes in stroke patients treated with tissue plasminogen activator (tPA). The effect of increased body temperature in stroke patients treated with tPA and with normal computed tomography angiography (CTA) on admission is unknown. We hypothesized a beneficial effect of higher body temperature in the absence of visible clots on CTA, possibly due to enhanced lysis of small, peripheral clots.
Methods: Patients with ischemic stroke admitted to our Stroke Unit between February 2006 and April 2013 were prospectively registered in a database (Bergen NORSTROKE Registry). Ischemic stroke patients treated with tPA with normal CTA of the cerebral arteries were included. Outcomes were assessed by the modified Rankin Scale (mRS) after 1 week. An excellent outcome was defined as mRS=0, and a favorable outcome as mRS=0–1.
Results: A total of 172 patients were included, of which 48 (27.9%) had an admission body temperature ≥37.0°C, and 124 (72.1%) had a body temperature <37.0°C. Body temperature ≥37.0°C was independently associated with excellent outcomes (odds ratio [OR]: 2.8; 95% confidence interval [CI]: 1.24–6.46; P=0.014) and favorable outcomes (OR: 2.8; 95% CI: 1.13–4.98; P=0.015) when adjusted for confounders.
Conclusion: We found an association between higher admission body temperature and improved outcome in tPA-treated stroke patients with normal admission CTA of the cerebral arteries. This may suggest a beneficial effect of higher body temperature on clot lysis in the absence of visible clots on CTA.
Keywords: acute ischemic stroke, body temperature, thrombolysis, tissue plasminogen activator
Introduction
Body temperature is an important clinical factor in ischemic stroke. Hypothermia is considered a robust neuroprotectant, and it has shown efficiency against different modalities of brain injury at an experimental level.1 In ischemic stroke, animal studies have shown a reduction of stroke volume in hypothermia and increased stroke volumes at higher temperatures.2–4 Similarly, observation studies in stroke patients have indicated an association between poor prognosis and increased body temperature within the first 12–24 hours of stroke onset.5,6 However, the role of body temperature in acute stroke patients treated with tissue plasminogen activator (tPA) is unclear. In vitro studies have shown a decrease in the fibrinolytic activity of tPA when temperature is reduced.7 In addition, several clinical studies have reported a beneficial effect of increased body temperature in ischemic stroke patients treated with tPA, suggesting an augmentation of clot lysis and recanalization at higher temperatures.8–10 In support of this theory, we recently showed an association between a low body temperature upon admission in acute ischemic stroke patients and persistent proximal middle cerebral artery (MCA) occlusion.11
A number of acute ischemic stroke patients treated with tPA present with normal computed tomography angiography (CTA) of the cerebral arteries on admission. These patients may have occluded cerebral vessels, which are too small for visualization on CTA, or they have already achieved complete recanalization at the time of admission. It is unknown whether body temperature influences outcomes in these patients. We aimed to explore this effect and hypothesized that higher body temperature has a beneficial effect on short-term outcomes in ischemic stroke patients treated with tPA with normal admission CTA of the cerebral arteries.
Methods
All patients with acute ischemic stroke admitted to the Stroke Unit, Department of Neurology, Haukeland University Hospital in Bergen, Norway, between February 2006 and April 2013 were prospectively registered in The Bergen NORSTROKE Registry, and the data were retrospectively analyzed. Ischemic stroke was defined in accordance with the Baltimore–Washington Cooperative Young Stroke Study Criteria, which were comprised of neurological deficits lasting longer than 24 hours because of ischemic lesions or transient ischemic attacks, where CT or magnetic resonance imaging showed infarctions related to the clinical findings.12
CTA was performed on admission in patients who were candidates for intravenous (IV) thrombolysis, unless contraindications to iodinated contrast agents were present (including renal insufficiency and a history of contrast agent allergy). The degree of partial or complete occlusion was assessed in the major cerebral arteries (including the MCA, anterior cerebral artery, posterior cerebral artery, basilar artery, and the intracranial part of the vertebral arteries). Total occlusion was defined as 100% occlusion, partial occlusion as 20%–50% or 50%–99% occlusion, and no occlusion as 0%–20% occlusion. The presence of an internal carotid artery (ICA) occlusion was evaluated with duplex ultrasound examination within 24 hours after admission.
Patients were included if they presented with no occlusion of the major intracranial arterial vessels on admission and without ICA occlusion on duplex ultrasound. All included patients had ischemic stroke and were treated with tPA. tPA was administered to eligible patients according to the Safe Implementation of Thrombolysis in Stroke (SITS) protocol.13 In addition, tPA was administered to patients with relative contraindications to tPA (such as age >80 years) based on a case by case evaluation.14
Body temperature was obtained on admission and measured by either an infrared tympanic device (LighTouch-LTX; Exergen Corporation, Watertown, MA, USA) or by using a temporal artery thermometer (Exergen Temporal Scanner; Exergen Corporation). The precision of both methods has been validated in several trials.15–17 Prior to temperature measurement, no temperature intervention (paracetamol or IV administration of fluids) was provided. The National Institute of Health Stroke Scale (NIHSS) was used to assess stroke severity on admission and discharge. Short-term outcomes were defined by the modified Rankin Scale (mRS) score on day 7 or at discharge, if the patient was discharged earlier. An excellent outcome was defined as an mRS score of 0, and a favorable outcome as an mRS score of 0 or 1. The study was approved by the local research ethics committee, and informed consent was obtained from all patients as part of a prospective study protocol.
Neuroimaging
Nonenhanced computed tomography (CT) and CTA sequences were performed according to a standard departmental stroke protocol with an 8- or 16-section multidetector CT scanner (LightSpeed®; GE Healthcare Bio-Sciences Corp, Piscataway, NJ, USA). Representative sample parameters were as follows: 120 kVp; 300 mA; 2-second scan time; and 5 mm section thickness. Nonenhanced CT was immediately followed by CTA. Scan delay time was determined using SmartPrep (GE Healthcare) and 80 mL of a nonionic contrast agent (Iomeron®; Bracco Imaging S.p.A., Milano, Italy) was administered at an injection rate of 2.0 mL/second through an 18-gauge intravenous catheter using a power injector (Medrad Stellant®; Medrad, Pittsburgh, PA, USA). The following parameters were used: 100 kVp; 300 mA; 1.25 mm section thickness; 0.6 mm reconstruction interval; and 1.35:1 pitch. Nonenhanced CT scans and CTA scans were reviewed by a stroke neurologist and stroke neurologist research fellow experienced in neuroimaging review (HN and CK, 15 and 4 years of neuroimaging experience, respectively).
Statistics
Included patients were dichotomized into two groups: those with an admission body temperature ≥37.0°C and those with an admission body temperature <37.0°C. Univariate analyses were performed between these two groups, where Student’s t-test, Pearson’s chi-square test, Fisher’s exact test, and the Wilcoxon rank sum test were used when appropriate. Logistic regression analyses were performed with excellent outcomes and favorable outcomes serving as the dependent variables. A post hoc analysis was performed with the NIHSS score at discharge as the dependent variable in a linear regression model. Potential confounders from the univariate analyses, such as time from symptom onset to hospital admission, prior medical history, stroke etiology, and admission parameters, were removed from the analyses by backward stepwise selection. Analyses were performed using STATA 11.0 (StataCorp LP, College Station, TX, USA).
Results
A total of 272 ischemic stroke patients were treated with tPA, of which 185 (68.0%) had CTA without partial or complete occlusion of the cerebral arteries on admission. Of this population, there were 13 (7.0%) patients with ICA occlusion. This led to the inclusion of 172 patients with normal CTA of the cerebral arteries and without ICA occlusion.
Body temperature on admission was ≥37.0°C in 48 (27.9%) of these patients, whereas 124 patients (72.1%) had a body temperature <37.0°C. The mean body temperature was 37.3°C (95% confidence interval [CI]: 37.2°C–37.4°C) in patients with an admission temperature ≥37.0°C and 36.3°C (95% CI: 36.3°C–36.4°C) in patients with an admission temperature <37.0°C.
Demography, clinical characteristics, and outcome rates are shown in Table 1. The mean age was 70.3 years in patients with body temperatures ≥37.0°C and 70.5 years in patients with body temperatures <37.0°C (P=0.460). Prior medical history and stroke etiology were similar in both groups. Median NIHSS score on admission was 6 (interquartile range: 4–10) in patients with a body temperature ≥37.0°C, and 6 (interquartile range: 4–11) in patients with a body temperature <37.0°C (P=0.673). Blood test values at admission were also similar in both groups, except for serum glucose, which was lower in patients with a body temperature ≥37°C (6.1 mmol/L versus 7.1 mmol/L, P=0.008). A total of 16 patients (33.3%) with a body temperature ≥37.0°C and 18 patients (14.5%) with a body temperature <37.0°C had excellent short-term outcomes (P=0.005). Favorable short-term outcomes were achieved in 26 patients (54.2%) with a body temperature ≥37.0°C and in 41 patients (33.1%) with a body temperature <37.0°C (P=0.011).
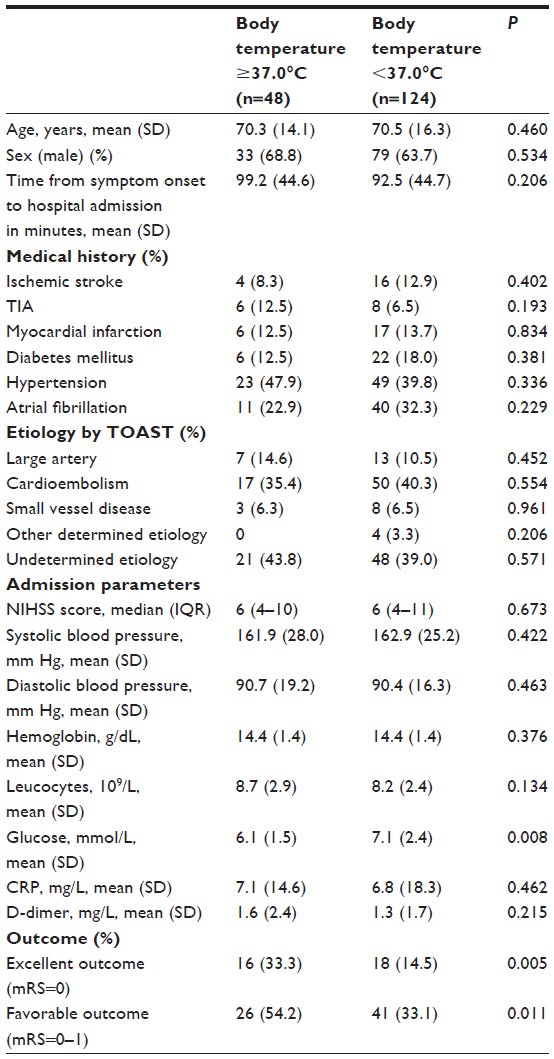 | Table 1 Univariate analyses of demography, clinical characteristics, and outcome rates among ischemic stroke patients with normal CT angiography of their cerebral arteries after treatment with tPA and with admission body temperatures ≥37.0°C versus <37.0°C |
Logistic regression analyses with excellent outcomes and favorable outcomes are illustrated in Tables 2 and 3, respectively. Body temperature ≥37.0°C was independently associated with excellent outcomes (odds ratio [OR]: 2.8; 95% CI: 1.24–6.46; P=0.014) and favorable outcomes (OR: 2.4; 95% CI: 1.13–4.98; P=0.015) when adjusted for age, sex, and NIHSS score on admission. Serum glucose was not associated with excellent outcomes (OR: 1.0; 95% CI: 0.80–1.18; P=0.798) or favorable outcomes (OR: 0.94; 95% CI: 0.81–1.11; P=0.502), and it did not affect the impact of body temperature on outcomes when implemented into the logistic regression models as an independent variable (not shown). It was, therefore, removed from the final logistic regression models.
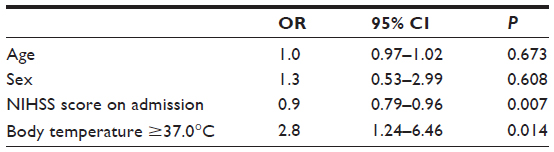 | Table 2 Logistic regression analysis with excellent outcomes (mRS=0) as the dependent variable among ischemic stroke patients with normal CT angiography of their cerebral arteries when treated with tPA |
 | Table 3 Logistic regression analysis with favorable outcomes (mRS=0–1) as the dependent variable among ischemic stroke patients with normal CT angiography of their cerebral arteries when treated with tPA |
A post-hoc analysis was performed with the NIHSS score at discharge serving as the dependent variable in a linear regression model. Increased body temperature on admission was independently associated with lower NIHSS scores at discharge when adjusted for confounders and when patients with minor stroke symptoms on admission (NIHSS score ≤1) were excluded. (P=0.029). There was no such association when patients with an admission NIHSS score ≤1 were included (P=0.104).
Discussion
Our study showed that higher body temperature on admission was associated with improved short-term outcomes in ischemic stroke patients treated with tPA and with normal angiographic findings of their cerebral arteries on admission. A recent study showed an association between higher body temperature upon admission and recanalization of the MCA prior to admission.11 Our findings suggest a beneficial effect of higher body temperature also in the absence of larger clots on admission CTA. This may be explained by an improved thrombolytic effect of tPA in smaller clots, which are not visible on angiographic imaging, resulting in a higher rate of recanalization and improved outcomes in patients with higher body temperatures. Normal CTA on admission in ischemic stroke patients may also indicate that a thrombus has already recanalized prior to the thrombolytic treatment. It is possible that an increased body temperature could have contributed to an earlier recanalization prior to admission than was achieved in patients with lower temperatures, thus resulting in improved outcomes in patients with higher temperatures. These theories remain speculative, as admission CTA was normal on admission in all patients and imaging of recanalization prior to admission is difficult to obtain.
There are other potential explanations for our findings. Patients presenting with lower body temperatures could have had worse outcomes due to more severe neurological deficits that appeared initially, thus leading to less muscle activity and lower body temperature on admission. However, neurological deficits, as measured by the NIHSS score, were similar in both groups upon admission, which makes this explanation unlikely.
Serum glucose was higher in patients with lower admission temperatures. Higher levels of glucose have been associated with worse prognosis in prior stroke studies.18,19 Consequently, patients with lower temperatures could have achieved worse short-term outcomes due to elevated glucose levels on admission. Nonetheless, higher body temperature was still associated with improved outcomes when serum glucose levels were adjusted for in the multivariate analyses.
Our results contradict the findings of prior clinical trials.5,6,20,21 These studies found an association between increased body temperatures measured beyond 6 hours after stroke onset and worse prognosis. In this study, we were primarily interested in the effect of higher body temperatures on clot lysis, and in outcomes in the very early phase following the onset of stroke symptoms. We, therefore, used body temperature measured on admission. This may explain some of the discrepancies between our findings and the findings of these studies.
Our findings are in agreement with the results of other clinical studies. A recent study, which included 647 ischemic stroke patients treated with tPA, found an association between high baseline body temperature and favorable outcomes after 3 months.8 This finding suggested an increased rate of clot lysis in patients with increased body temperatures. We recently reported an association of higher body temperature and major neurological improvement in severe ischemic stroke patients treated with tPA,22 suggesting a beneficial effect of higher body temperature on clot lysis and recanalization. In addition, a previous study including 111 patients treated with tPA found a beneficial effect of high admission body temperature on short-term outcomes.10 The authors speculated that the effect of high body temperature on clot lysis could be more important than the potential neuroprotective effect of low body temperature in stroke patients treated with tPA.
It is customary to treat elevated body temperatures with pharmacological or physical strategies in the acute phase of ischemic stroke, even though there are no randomized trials favoring such strategies. A randomized, placebo-controlled study including 1,400 patients with ischemic stroke showed no overall effect of paracetamol on outcomes, although a post hoc analysis found a beneficial effect of paracetamol in patients with increased temperatures.23 In addition, a systematic review of randomized trials could not find evidence to support the use of pharmacological or physical strategies to reduce body temperature in patients with acute ischemic stroke.24 Our study and previous findings may explain these disappointing results obtained when treating stroke patients in the acute phase with different cooling strategies.9–11 Although temperature lowering represents a potent neuroprotective therapy, this effect may be negated due to prolonged clot lysis in stroke patients treated with tPA.
Our study has some limitations. We theorized a beneficial effect of higher body temperature on clot lysis and recanalization. Although our results showed an association between higher body temperature and improved outcomes, our theory is difficult to assess due to lack of direct imaging of recanalization. This would, however, have been difficult to obtain, as CTA was normal in all patients on admission. Second, ICA occlusion was assessed by ultrasound within 24 hours after admission and not on admission CTA. It is theoretically possible that a patient with ischemic stroke due to ICA occlusion presented with normal CTA of the cerebral vessels, where the ICA occlusion recanalized after thrombolytic treatment and, therefore, was not evident on ultrasound examination the next day. Since the rate of successful recanalization in ICA occlusions is relatively low, this could only have affected a small minority of patients.25 Third, only short-term clinical outcomes were obtained, and not outcomes after 3 months. Early outcomes may, however, also be highly relevant when studying acute stroke, as it is more directed to the stroke as such, whereas patient outcomes after 3 months encompass other factors such as rehabilitation, caregiver support, recurrent strokes, and so on.26
Conclusion
In conclusion, our study showed an association between higher body temperature upon admission and improved short-term outcomes in ischemic stroke patients treated with tPA, and who presented with normal CTA of the cerebral arteries on admission. This may suggest a beneficial effect of higher body temperature on clot lysis in the absence of visible clots on CTA.
Acknowledgment
Christopher Elnan Kvistad has been supported by Helse Vest Research Fund number 911776 as a PhD research fellow.
Disclosure
The authors report no conflicts of interest in this work.
References
Yenari MA, Hemmen TM. Therapeutic hypothermia for brain ischemia: where have we come and where do we go? Stroke. 2010;41(Suppl 10):S72–S74. | |
van der Worp HB, Sena ES, Donnan GA, Howells DW, Macleod MR. Hypothermia in animal models of acute ischaemic stroke: a systematic review and meta-analysis. Brain. 2007;130(Pt 12):3063–3074. | |
Huang ZG, Xue D, Preston E, Karbalai H, Buchan AM. Biphasic opening of the blood-brain barrier following transient focal ischemia: effects of hypothermia. Can J Neurol Sci. 1999;26(4):298–304. | |
Dietrich WD, Halley M, Valdes I, Busto R. Interrelationships between increased vascular permeability and acute neuronal damage following temperature-controlled brain ischemia in rats. Acta Neuropathol. 1991;81(6):615–625. | |
Jørgensen HS, Reith J, Pedersen PM, Nakayama H, Olsen TS. Body temperature and outcome in stroke patients. Lancet. 1996; 348(9021):193. | |
Boysen G, Christensen H. Stroke severity determines body temperature in acute stroke. Stroke. 2001;32(2):413–417. | |
Yenari MA, Palmer JT, Bracci PM, Steinberg GK. Thrombolysis with tissue plasminogen activator (tPA) is temperature dependent. Thromb Res. 1995;77(5):475–481. | |
de Ridder I, den Hertog H, van Gemert M, Dippel D, van der Worp B; PAIS investigators. Increased benefit of alteplase in patients with ischemic stroke and a high body temperature. Cerebrovasc Dis. 2013;35(1):60–63. | |
Kvistad CE, Thomassen L, Waje-Andreassen U, Naess H. Low body temperature associated with severe ischemic stroke within 6 hours of onset: The Bergen NORSTROKE Study. Vasc Health Risk Manag. 2012;8:333–338. | |
Naess H, Idicula T, Lagallo N, Brogger J, Waje-Andreassen U, Thomassen L. Inverse relationship of baseline body temperature and outcome between ischemic stroke patients treated and not treated with thrombolysis: the Bergen stroke study. Acta Neurol Scand. 2010;122(6):414–417. | |
Kvistad CE, Øygarden H, Thomassen L, Waje-Andreassen U, Naess H. Persistent middle cerebral artery occlusion associated with lower body temperature on admission. Vasc Health Risk Manag. 2013;9:297–302. | |
Johnson CJ, Kittner SJ, McCarter RJ, et al. Interrater reliability of an etiologic classification of ischemic stroke. Stroke. 1995;26(1):46–51. | |
Wahlgren N, Ahmed N, Davalos A, et al. Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST): an observational study. Lancet. 2007;369:275–82. [Erratum, Lancet. 2007;369:826]. | |
Kvistad CE, Logallo N, Thomassen L, Waje-Andreassen U, Brøgger J, Naess H. Safety of off-label stroke treatment with tissue plasminogen activator. Acta Neurol Scand. 2013;128(1):48–53. | |
Summers S. Axillary, tympanic, and esophageal temperature measurement: descriptive comparisons in postanesthesia patients. J Post Anesth Nurs. 1991;6(6):420–425. | |
Lee G, Flannery-Bergey D, Randall-Rollins K, et al. Accuracy of temporal artery thermometry in neonatal intensive care infants. Adv Neonatal Care. 2011;11(1):62–70. | |
Myny D, De Waele J, Defloor T, Blot S, Colardyn F. Temporal scanner thermometry: a new method of core temperature estimation in ICU patients. Scott Med J. 2005;50(1):15–18. | |
Bruno A, Levine SR, Frankel MR, et al; NINDS rt-PA Stroke Study Group. Admission glucose level and clinical outcomes in the NINDS rt-PA Stroke Trial. Neurology. 2002;59(5):669–674. | |
Adams HP Jr, del Zoppo G, Alberts MJ, et al; American Heart Association/American Stroke Association Stroke Council; American Heart Association/American Stroke Association Clinical Cardiology Council; American Heart Association/American Stroke Association Cardiovascular Radiology and Intervention Council; American Heart Association/American Stroke Association Cardiovascular Radiology and Intervention Council; Artherosclerotic Peripheral Vascular Disease Working Group; Quality of Care Outcomes in Research Interdisciplinary Working Group. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Circulation. 2007;115(20):e478–e534. | |
Castillo J, Dávalos A, Marrugat J, Noya M. Timing for fever-related brain damage in acute ischemic stroke. Stroke. 1998;29(12):2455–2460. | |
Kammersgaard LP, Jørgensen HS, Rungby JA, et al. Admission body temperature predicts long-term mortality after acute stroke: the Copenhagen Stroke Study. Stroke. 2002;33(7):1759–1762. | |
Kvistad CE, Thomassen L, Waje-Andreassen U, Logallo N, Naess H. Body temperature and major neurological improvement in tPA-treated stroke patients. Acta Neurol Scand. Epub 2013 Sep 20. | |
den Hertog HM, van der Worp HB, van Gemert HM, et al; PAIS investigators. High-dose paracetamol in stroke: new trials are necessary and feasible. Lancet Neurol. 2009;8(8):700–701; author reply 701. | |
Den Hertog HM, van der Worp HB, Tseng MC, Dippel DW. Cooling therapy for acute stroke. Cochrane Database Syst Rev. 2009;(1):CD001247. | |
Christou I, Felberg RA, Demchuk AM, et al. Intravenous tissue plasminogen activator and flow improvement in acute ischemic stroke patients with internal carotid artery occlusion. J Neuroimaging. 2002;12(2):119–123. | |
Thomassen L, Waje-Andreassen U, Broegger J, Naess H. Acute stroke centre – the changing focus of stroke unit care. The Bergen NORSTROKE Study. Acta Neurol Scand. 2012;125(6):410–415. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.