Back to Journals » International Journal of Women's Health » Volume 7
Is female circumcision evolving or dissolving in Norway? A qualitative study on attitudes toward the practice among young Somalis in the Oslo area
Authors Gele A, Sagbakken M, Kumar B
Received 28 July 2015
Accepted for publication 13 September 2015
Published 26 November 2015 Volume 2015:7 Pages 933—943
DOI https://doi.org/10.2147/IJWH.S93217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Elie Al-Chaer
Abdi A Gele,1,2 Mette Sagbakken,1,2 Bernadette Kumar2
1Department of Nursing and Health Promotion, Oslo and Akershus University College of Applied Sciences, Oslo, Norway; 2Norwegian Centre for Minority Health Research, Oslo, Norway
Abstract: Female genital mutilation or female circumcision (FC) is increasingly visible on the global health and development agenda – both as a matter of social justice and equality for women and as a research priority. Norway is one of the global nations hosting a large number of immigrants from FC-practicing countries, the majority from Somalia. To help counteract this practice, Norway has adopted a multifaceted policy approach that employs one of the toughest measures against FC in the world. However, little is known about the impact of Norway’s approach on the attitudes toward the practice among traditional FC-practicing communities in Norway. Against this background, this qualitative study explores the attitudes toward FC among young Somalis between the ages of 16 to 22 living in the Oslo and Akershus regions of Norway. Findings indicate that young Somalis in the Oslo area have, to a large extent, changed their attitude toward the practice. This was shown by the participants’ support and sympathy toward criminalization of FC in Norway, which they believed was an important step toward saving young girls from the harmful consequences of FC. Most of the uncircumcised girls see their uncircumcised status as being normal, whereas they see circumcised girls as survivors of violence and injustice. Moreover, the fact that male participants prefer a marriage to uncircumcised girls is a strong condition for change, since if uncut girls are seen as marriageable then parents are unlikely to want to circumcise them. As newly arrived immigrants continue to have positive attitudes toward the practice, knowledge of FC should be integrated into introduction program classes that immigrants attend shortly after their residence permit is granted. This study adds to the knowledge of the process of the abandonment of FC among immigrants in Western countries.
Keywords: FGM, immigrants, attitude change, Somalis
Background
An estimated 100 to 125 million women alive today have undergone female circumcision (FC) worldwide, and three million girls are at risk every year.1 The vast majority of these women live in 28 countries in Africa, some areas in Asia and in Western countries that host immigrants.1 The prevalence of FC varies among practicing countries in Africa, with Somalia having the highest prevalence of FC in the world.1 Like many other Western countries, immigrants of Somali descent constitute the largest non-Western immigrant group in Norway and the largest group from any FC-practicing country.2,3 While the history of the practice in Africa indicates that FC evolves and dissolves with time and place, immigrants of Somali descent who live in Scandinavia are often perceived as a cultural society that generally supports FC.4 Nonetheless, with approximately 40,000 Somalis currently living in Norway, there are a significant number of young Somalis who are born or brought up in Norway, and to date existing literature in Scandinavia has not explored the attitudes and practices toward FC among this generation.
“Female genital mutilation” or “female circumcision”, which we use in this paper because it is a literal translation from the Somali language (gudniinka dumarka), is a traditional social practice involving the removal or injury of external female genitals for non-therapeutic reasons.5 The practice is often performed on girls between the ages of 0–9 through one of four types classified by the World Health Organization.5 Type I (sunna) involves the partial or total removal of the clitoris and/or the prepuce, while Type II involves the partial or total removal of the clitoris and labia minora. Being the most radical form, Type III (pharaonic) involves the partial or total removal of the external genitalia and a sealing of the vaginal opening, leaving only a small hole for urine and menstrual blood to pass (whether with or without cutting the clitoris). Lastly, Type IV involves all other procedures to the female genitalia for nonmedical reasons.
Independent of type, FC is a painful surgical procedure that is usually carried out without anesthesia, and which often results in psychological and medical complications for the girls.6 Girls may suffer tissue damage that may negatively affect the health of the girls over the course of their lifetime.6 Local and generalized infections, severe pain, acute hemorrhage, and even death may be short-term complications, with other possible complications including the retention of urine and difficulties in menstruation.7 A number of studies have shown associations between different adverse obstetric outcomes and FC.6,8 The psychological consequences following FC are described as post-traumatic shock and depression, as well as a loss of trust and a lack of bodily well-being.9 It is also important to highlight that the practice is a violation of the basic human rights of girls and women.
The health and human rights consequences of the practice make it imperative for societies, governments, and the entire international community to take action to put this practice to an end. Despite an international determination to end the practice, FC continues to persist in practicing countries in Africa.10 People who practice FC live in three different social environments: 1) those in which nearly everyone has their girls cut; 2) those in which no one has their girls cut; and 3) those in which some girls get cut, while others do not.11 Families who live in the latter two social environments are more likely to give up the practice through interventions as they interact with communities who do not circumcise their daughters, and hence who may inspire them to abandon the practice,12 compared to those who live in environments in which almost every girl is cut. Accordingly, after 40 years of international campaigns, the prevalence of FC remains almost stagnant in most countries where the prevalence exceeds 80%.10
FC in Somalia
There is no evidence on how and when FC came into Somalia, but older literature indicates that FC existed in Somalia as early as the 17th century.13 Somalia currently has a FC prevalence of ≥97%, which is the highest in the world.14 Each year, an estimated 70,000 to 80,000 girls between the ages of 6 to 10 face the possibility of being circumcised by traditional practitioners,15 although the medicalization of FC is also on the rise.16 While milder types of FC constitute 85% of global FC, infibulations or pharaonic are the most prevalent types in Somalia.16 Unlike other countries where the FC prevalence is ethnically dependent, and/or the disaggregation of prevalence by ethnicity is necessary, the practice equally affects all ethnic groups in Somalia.16 Similarly, literacy, sub-group membership or lifestyle does not seem to influence the prevalence of the practice, as the procedure is used by the entire spectrum of people, from urban dwellers to nomads.15 The reasons behind the practice of circumcision is primarily the belief that it is required by religion17 and a social pressure based on “do what others did”.18 After generations of infibulating girls, many Somalis presume that only an infibulated girl can be a virgin. Hence, because infibulations have become the sole certificate for virginity, its absence may create a suspicion of premarital sex, thereby questioning the moral accountability of the woman. As Mackie has stated, women may believe that men would not marry an unmutilated woman, and men may believe that an unmutilated woman may not be a faithful partner in marriage; consequently, people lock themselves in this convention, since a woman would not choose non-marriage and a man would not choose an unfaithful partner.13
FC in Norway
Following the onset of the civil war in Somalia during 1988–1991, a large influx of Somalis fled to the outside world, with many of them ending up in Western countries that host immigrants. The resettlement of Somalis to Western countries with different cultures required an extensive adjustment that has sometimes compromised their health.19 Somalis’ tradition of circumcising girls was unknown in their host countries and unacceptable internationally. This raised a discussion on how to deal with Somalis regarding their FC traditions, and as a result, many countries adopted policies against the practice, including the criminalization of FC.20
Norway has one of the toughest measures against FC in the world. The practice was criminalized in 1995, with the penalty of performing FC being “a term of imprisonment of up to 6 years”.20 In addition, a government action plan against FC was established in 2000.20 The rationale of the action plan was to prevent FC and to accomplish a behavioral change toward the practice.20 Among the different measures in the action plan was the inclusion of FC as a theme in Norway’s parental guidance program and the development of training programs for religious leaders, health personnel, school staff and students, in addition to the provision of financial support to non-governmental organizations and institutions to design and implement preventive programs against the practice.20 The first evaluation report of the government’s action plan was conducted in 2005. The report highlighted the importance of introducing strict measures, including legal punishment and deterrence in preventing FC, as well as suggesting compulsory genital checkups for the population at risk.21 Accordingly, there is a voluntary genital checkup of girls from countries where FC is practiced.
The second evaluation report on FC in Norway was presented by the Institute of Social Research in 2008.22 This report concluded that FC is not a significant problem in Norway, which was supported by ample empirical findings in Norway,2,3,23–25 as well as the latest report on FC presented by the Institute of Labor and Social Research in 2014.4 Furthermore, the Institute of Labor and Social Research report highlighted an inconsistency between the government measures, which are often based on the notion that FC is a serious problem in Norway, and the available empirical evidence indicating that FC is no longer a major problem in Norway.4 With this inconsistency existing between the current approach to FC abandonment in Norway and the available empirical findings, this study explores how FC is viewed by young Somali–Norwegian girls and boys between the ages of 16 and 22 years.
Influence of social environment in attitudes toward FC
Attitude is a learned tendency to evaluate a phenomenon in a certain way, and while they emerge from and are embedded in social interaction, attitudes are neither static nor immutable, but are spatially or temporarily variable.26 Given that attitudes are subject to modification, permutation, even transformation, it is important to understand how attitudes toward FC evolve.The primary process in influence is not the change in attitudes toward FC but rather change in the definition and meaning of the practice. When meaning changes, attitudes change accordingly. An anthropological study in Norway stated that FC, which is perceived as cleansing and a sign of womanhood in Somalia, has now been reinterpreted by Somali women in exile as “amputation and even mutilation”.23 As people gain information about FC, new altered beliefs may result as a result of that exposure. If altered or new beliefs develop, they will be followed by changed attitudes.
The place of residence is known to have a strong influence on meaning and definitions of FC and consequently the attitudes toward the practice. In Africa, urban women are less likely to support the continuation of the practice compared to rural women, and there is a discrepancy in the circumcision of girls within members of the same ethnic group given the social context in which each family lives. For instance, women from the Peulh tribe of Senegal unanimously circumcise their daughters when they live in the Matan region, where the prevalence of FC is almost universal, but FC is almost nonexistent within this ethnic group when they live in the Diourbel region, where the prevalence of FC is almost zero.10 Similarly, the type and frequency of FC in Somalia are predicted by the region of residence and not by the birthplace of the parents.27 For example, people who moved from Northern Somalia, where infibulation was common, to Southern regions, where the milder forms of FC were predominant, adopted the practice common to their new residence. The Falasha community, who used to practice FC when they were in Ethiopia, abandoned the practice when they resettled in Israel, where the practice is unknown.28
The rationale is that when people resettle to a new environment “they weigh their available choices, and they always move to the highest possible value among their available choices”.29 Accordingly, in populations where every girl is circumcised, neither those who oppose the practice nor those who do not (acting alone) have an option valued more highly than to circumcise their daughters, since neither of the two groups has an incentive to choose otherwise. The same applies to communities who move to where no girl is circumcised, as no one in that community has an option valued higher than leaving their girls untouched.30
The Padilla (1980) Model of Acculturation shows that having a “cultural awareness” that involves a proficiency in the languages of each culture and a knowledge of major historical events that have shaped the cultures are decisive in the acculturation process.31 The model holds that individuals are more acculturated if they show more knowledge of host cultures and speak the host country’s language better than the language of their original country. This raises a question of how young Somalis who are born or brought up in Norway, and who speak Norwegian as a mother tongue and Somali as their second language, see the practice of FC, which is a tradition that is common in their country of origin though unknown in their host culture. Existing theories on FC emphasize that when families live in an environment in which FC is normative, they are more likely to conform to the prevalent social norm.29 Similarly, in a social environment where the practice is unknown and illegal, people are likely to conform to the social rules and abandon the practice. Shell-Duncan and Herniund argued that in some situations, people may abandon the practice even if they personally want it to continue, eg, when they reside in an environment where there is an enforced law that forbids the practice, with a subsequent fear of prosecution for breaking the law.32 There is a large Somali community in the Oslo area, where FC is illegal. Moreover, previous studies have reported a sign of abandonment of FC among the Somali community in Norway,2,3 though none of these studies have explored how FC is viewed by young Somalis. This paper explores the attitudes toward FC among young Somalis between the ages of 16 to 22 living in the Oslo and Akershus regions of Norway.
Methods
Participants and data collection
A qualitative study including 24 young Somalis between the ages of 16 and 22 was conducted in the Oslo and Akershus regions of Norway. The participants were recruited using a maximum variation sampling aimed at diversity in terms of education, sex, age, and number of years having lived in Norway. Prior to the data collection, the participants were informed about both the objectives of the study and the expected duration of the interviews. Verbal consent was obtained from participants with the assurance that they could withdraw from the study at any time without any negative consequences. The study was evaluated and approved by the Norwegian Social Science Data Services.
Two Somali-born, bilingual research assistants (male and female) who work for the Norwegian Centre for Minority Health Research conducted the interviews in Somali and Norwegian languages. The researchers were members of the Somali community in Oslo, who previously conducted a similar data collection on female genital mutilation from Somalis in Oslo. As a result, they enjoyed trust and respect among their community. Despite the sensitivity of the research topic, as FC is illegal in Norway, the participants, given their familiarity with researchers, have never associated the researchers with authority, a superior power or the mainstream community. Hence, the participants seemed to discuss the topic openly without fear of any negative consequences or stigma. After each interview, a reward card of 250 Norwegian kroner was offered to participants for compensation for their participation. All interviews were audio-taped, with each interview lasting 30 minutes to an hour. The interview process continued until it was clear that no new information was emerging from the additional interviews; that is when saturation was achieved.
Content of the interviews
Within a Somali context, the term “female genital mutilation” refers to the “pharaonic” form and may exclude the “sunna” circumcision. In order to avoid this interpretation, we adopted the term “female circumcision”, which includes all forms of female genital mutilation and is locally used. During the interviews, participants were asked about their understanding of FC, their personal experience with FC, the advantages and disadvantages of the practice, the religious, legal and human rights aspects of the practice and their perspectives regarding the continuation or discontinuation of all forms of FC. The reasons behind the motivation for the continuation or discontinuation of the practice, as well as the factors considered decisive for the continuation or discontinuation of the practice, were explored. Furthermore, the link between marriage and FC was explored and female participants were asked if they were circumcised or not. We did not ask where the circumcision took place, however, we recorded participants’ age of arrival in Norway. As age of circumcision among Somali girls is known, it is not difficult to know whether someone is circumcised after or before arrival in Norway.
Analysis
The interviewers transcribed the interviews. The first author systematically read the transcripts, and then reread them to identify themes of importance. We used thematic analysis to identify, analyze, and report on the identified themes, with the coding process being involved in recognizing an important theme and encoding it prior to interpretation. Leininger33 suggests that themes can be identified by bringing together fragments of ideas, experiences, and beliefs that are often meaningless when viewed alone. For that reason, themes that emerged from the informants’ stories were pieced together to form a comprehensive picture of the participants’ shared experience.34 The themes that were identified through coding were divided into categories based on the participants’ common experience, knowledge, and attitude toward FC.
Results
This study included 24 young Somali–Norwegians (12 boys and 12 girls), aged 16 to 22 years, and the mean age of the study participants was 18 years. The majority of our study participants were born in Norway, with this being the case for eight out of 12 boys and five out of 12 girls. Others came to Norway within 2 years prior to the commencement of this study, and all the participants were students, who either attended a lower/upper secondary school or a university. Table 1 provides demographic details and circumcision status for the female participants in this study. Four major categories emerged from the analysis: participants’ attitudes toward the continuation or discontinuation of FC, the reasons behind the participants’ decisions in regards to continuation\discontinuation of FC, the participants’ perspectives toward the link between marriage and circumcision, and the participants’ perceptions toward circumcised and uncircumcised girls.
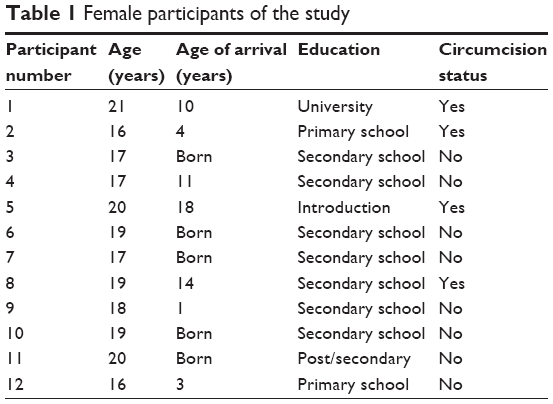 | Table 1 Female participants of the study |
Participants’ attitude toward the continuation or discontinuation of the practice
Regardless of their sex, the young Somalis who participated in the study were predominantly against the practice. Their position is partially shaped by the conviction that FC is a harmful practice subjected on girls without their consent, and that it is not required by Islam. In Somalia, both boys and girls are circumcised for the same reason. However, our participants separated male circumcision from FC. Whereas they considered the former to be both a religious duty and a symbol of good health, they saw the latter as being detrimental to the health of girls. With the exception of two boys who had lived in Norway for just over a year, the majority of the participants were negatively inclined toward FC. The arguments against the continuation of FC were similar for most of the participants, who expressed that these practices cause health problems among girls, and that FC is not a religious requirement, but instead a violation of a woman’s human rights. Participants expressed that this was especially the case because girls are subjected to this practice without their consent. Some participants iterated that their position toward FC is largely influenced by the social environment within which they live (Norway), and that it is very different from the social environment where their parents grew up (Somalia).
Female participants who were either born in Norway or came to Norway before the age of 4 reported not to be circumcised. As shown in Table 1, this was in stark contrast to those who came to Norway at a later stage in life, and this finding is in accordance with prior quantitative studies among Somalis in Oslo.
Social environment that rejects the practice
Most participants agreed that FC should be discontinued. This change was attributed to the social environment in Norway, which is supportive of change. Participants mentioned their parents, friends, media, and society in general as their source of information, in addition to motivational factors for rejecting FC.
I was brought up in another country where FC was seen as normal. When I came to Norway, I found that every person here is against it, and I agree with them because it is a harmful tradition. [Participant 8, girl]
I know my mum believes that FC is wrong. Like my friends, I am influenced by the media, such as TV and newspapers. [Participant 15, boy]
I support the discontinuation of FC because it is not religious duty. It is a tradition, and the tradition is amendable. An increased knowledge of Islam influenced my position towards FC. Secondly, it is my family and my friends who influenced me. I live in Norway, even the social environment that I live in has an influence on me. [Participant 7, girl]
One female participant clearly demonstrated the power of one’s social environment in influencing attitudes toward FC. As a young person who was brought up in Norway, she noted that she had never heard anything positive about FC, and from what she could tell, there was nothing advantageous about this practice:
I have never heard anything good about FC. The only thing I have heard about FC was that it is a harmful tradition that is forced on girls. [Participant 10, girl]
The practice is not required by religion
Apart from two boys who thought that FC was required by Islam, participants rejected the practice, as they believed that it has nothing to do with religion. Most participants were uncertain as to why circumcision was practiced at all. Girls born in Norway were more likely to ask questions, such as “Why are girls circumcised?” than giving answers themselves:
I don’t know why girls are circumcised? What do they cut? Circumcision is not for girls, if it was, Allah would have mentioned it in the Koran. Yet, when they are doing the procedure, it is not a doctor who is doing it, it is very dangerous. [Participant 3, girl]
Some participants had a clear idea about the differences between boy circumcision and FC, with the former being perceived as a religious duty, while the latter was perceived as non-Islamic:
Boy circumcision is proper, but girl circumcision is wrong. The reason is that boy circumcision is a religious duty, but girl circumcision is not. It is wrong to inflict unnecessary harm on girls. [Participant 7, girl]
Other participants rejected the practice in strong terms with the conviction that FC is not even “sunna” (optional), and it has nothing to do with Islam:
Islam doesn’t accept the mutilation of the girl body. Some people may perceive it as sunna, but I don’t believe that and I would prefer that girls are left uncut. The Koran doesn’t mention anything about cutting tissues from girls and sewing them up. [Participant 5, girl]
Islam forbids FC but there are many people who think that it is religious duty. It is not even sunna. [Participant 6, girl]
Islam doesn’t require girl circumcision as my mum told me, so it is wrong to circumcise girls. If it was sunna then religion would have given us clear instructions about it, but that doesn’t exist. [Participant 23, boy]
Girl circumcision has no place in Islam. It is an old harmful tradition. [Participant 24, boy]
The practice causes health problems
Almost all the participants associated FC with health problems, including pain, infection, bleeding, urine and menstrual retention, as well as difficulties in childbirth and sexual problems. Some participants, particularly those who were born in Norway, demonstrated some level of misunderstanding about the health problems associated with FC. For instance, one boy mentioned that women who are circumcised are unable to conceive a child. Additionally, while participants had no doubt about FC’s adverse health effects, most of the girls who were born in Norway were uncertain of the types of health problems this practice can cause:
I don’t know the problems associated with FC, but I think it is a painful procedure. Health problems may include infection. I don’t know about other health problems. [Participant 7, girl]
All I know about is urine retention and difficulties in childbirth, and possibly sexual intercourse. [Participant 10, girl]
FC has so many problems, such as infection, menstrual retention, difficulties in childbirth; I don’t know about other problems. [Participant 11, girl]
Girls who were born in Somalia and experienced FC themselves had a better and more detailed explanation about the health consequences of FC compared to those who were born in Norway:
FC is painful. The pain often comes when the woman gets married. They feel pain during child delivery, and if they are infibulated they experience menstrual retention. If a girl is circumcised using a severe form, they feel pain in urination and menstruation. I don’t know that much about the problems due to FC, but if the girl is infibulated it can lead to other problems. I was taught at school that tissues that are sexually important are removed, so girls may worry about their sexual desire and enjoyment. [Participant 8, girl]
FC is unethical and a violation of human rights
The majority of the participants were against FC as a practice because they thought that young girls are subjected to this practice without their consent. They emphasized that girls, if given a voice, would not choose to become circumcised. As previously mentioned, participants who had experienced this practice were far more likely to oppose it than girls and boys who were born in Norway, arguing that it was a human rights violation:
According to human rights, every woman has a right to say no if that is what she doesn’t want. Most of the girls didn’t decide for FC. Therefore, FC is violation of human rights. [Participant 1, girl]
They violated the human rights of girls because their tissues were cut, while girls were unable to decide on what they want to do with their own body. There are others who made the decision to cut, and it is violation of the rights of the girls. [Participant 2, girl]
Participants of both sexes who were born in Norway used the terms: “I think”, “I don’t know”, or “as I have heard from others” very frequently, which may show that they were somehow uncertain of what they were saying because they have not experienced FC themselves:
I don’t know what FC looks like, but what I know is that girls are subjected to the practice while very young and without their consent, and for that reason FC is bad. [Participant 14, boy]
What I have heard was that most of the girls don’t want to be circumcised. It is the parents who decide for the procedure to take place against the will of the girl. That is all I have heard, but it is not something I have experienced or know about. [Participant 14, boy]
The human rights law forbids FC because the practice is often forced on a [girl] child without her consent. [Participant 10, girl]
I don’t know the position of human rights on FC. But what I know is that every human being wants to feel peace and security. I think it is forbidden because it is harmful to the health of the girls. [Participant 7, girl]
FC was not performed as a wish of the girl, it was the parents who decided for her. Her rights were not respected and she might not have chosen to circumcise herself if she was asked. Since she was not happy about what they did to her body, it is violation of her personal rights. [Participant 3, girl]
The Norwegian law
Another important theme that emerged from the interviews was the participants’ knowledge and their support for the criminalization of FC in Norway. The participants overwhelmingly expressed their support and sympathy toward the Norwegian law against FC, which they believed was an important step toward saving young girls from the harmful consequences of FC:
FC is unlawful in Norway and there is the likelihood of a penalty of 5 to 8 years for those who are found performing the practice. I support this law because harm is caused to the young girl and her rights are violated. The law is meant to bring the perpetrator to justice. [Participant 2, girl]
Norwegian law doesn’t accept FC. When I came to Norway, I was told that anyone who performed FC would be arrested because it is illegal. To me, it is right that FC is illegal. [Participant 5, girl]
In Norway, FC is illegal and anyone who performs it will be arrested, which I fully agree with. I wouldn’t have supported the law against it if I knew a single advantage of FC. [Participant 6, girl]
I have heard that it is a serious crime in Norway, and I believe it is correct to outlaw this practice. [Participant 18, boy]
However, while the vast majority supported the Norwegian law against FC, some boys who were born in Norway were either not aware of the presence of such a law against this practice in Norway, or whether the law was for or against the practice:
I don’t know whether the law is against or for FC. I don’t know. [Participant 14, boy]
I don’t know what the Norwegian law says about FC. [Participant 19, boy]
Influence of circumcision on marriage
Female participants were asked if the circumcision of girls may have an effect on their future marriage, and most girls reported that FC would not have any influence on their marriage:
I am circumcised and I don’t think I will have any problem in my marriage. I am going to marry a Somali man and it will be ok. [Participant 2, girl]
I am circumcised and I don’t think this will have any negative effect on my marriage. I don’t think I am different from uncircumcised girls. It depends how my future husband sees it. [Participant 1, girl]
It depends on how my future husband sees it. If he is a Somali who knows Somali culture he may not mind it. [Participant 8, girl]
Men [Somalis] have a good knowledge on girl circumcision, or if he wants he can ask me before we get married, but in any case I don’t think men care about circumcision. [Participant 5, girl]
Boys were asked if girls’ circumcision status is an issue for their marriage and whether they prefer circumcised or uncircumcised girls as their brides. The majority of boys either did not care about a girl’s circumcision status or had never thought about it:
If a girl is circumcised I cannot say I won’t marry you because you are circumcised. That is irrational. [Participant 14, boy]
I can hardly answer the question because I am not in that situation now. But as long as I love the person, it is ok for me [regardless of their circumcision status]. [Participant 15, boy]
I will marry an uncircumcised girl because I was born in Norway. My future wife is 99% likely to be born in Norway, and girls who are born in Norway are not circumcised.[Participant 24, boy]
Perceptions toward circumcised girls
Young participants were asked about how circumcised/uncircumcised girls are seen in their community. Most of the uncircumcised girls see their uncircumcised status as being normal, whereas they see circumcised girls as survivors of violence and injustice. Moreover, they consider discussing circumcision in the presence of circumcised girls to be an offense, and they believe that it should be avoided. Nonetheless, some participants said that being circumcised in Somalia is considered as an ideal, while being uncircumcised is a totally alien concept for native Somalis. However, the opposite is true in Norway:
Being circumcised in Norway is subject to stigmatization, particularly in my generation. But in Somalia, circumcised girls are considered ideal. [Participant 1, girl]
Here in Norway, being uncircumcised has a certain status, while being circumcised is like “sorry”. For instance, as we were discussing things yesterday, one of my friends asked my family member about her circumcision status. She responded “yes I am circumcised”. Then, she asked if she has any sexual feeling. Such weird questions often come into the discussion, and it may be difficult for circumcised women to bear. [Participant 4, girl]
People cannot understand whether or not someone is circumcised, and it is not normal to ask someone about her circumcision status. Most women see uncircumcised girls as ideal women because there are more uncircumcised girls than circumcised in Norway. As most of the girls who are born here are not circumcised, un-circumcision is popular here. [Participant 2, girl]
If the girl is circumcised, she is not stigmatized. Here in Norway most of the girls are not circumcised, though the circumcised and uncircumcised are treated equally in the public’s eyes. [Participant 3, girl]
When people ask you about your circumcision status and you respond “yes”, they give you an impression of condolence “sorry for that”. They look at you as someone who survived from human tragedy. But the circumcised girl may not see herself in that way. Fifty percent of my friends are not circumcised. It is circumcised girls who often feel psychological pain. The reason is that when all your age-mates are not circumcised, the circumcised girls are looked through different eyes. Every person is saying “sorry”, was it a painful procedure? Circumcision is not something that often come to our discussions because most of my age-mates are not circumcised. [Participant 4, girl]
People look at a circumcised girl as someone who is missing an important thing, who doesn’t have any sexual feelings and is a victim of abuse. In Somalia, however, circumcised girls are seen as polite and decent girls. [Participant 8, girl]
Poor knowledge about the practice among boys
A limited amount of knowledge regarding the practice was observed among the boys born in Norway. During the interview, they talked far less than the girls about the practice because they had very little to say about FC. Here are some of the responses that the boys gave when they were asked whether they had heard about FC and where they had obtained this information:
I have heard about girl circumcision, but I haven’t seen someone who was subjected to this practice. I don’t know how they perform it either. I have only heard that there is a type of circumcision called pharaonic. I don’t know the reason, is he the one who first initiated this practice? [Participant 22, boy]
I don’t know much about girl circumcision. I know about boy circumcision. But I heard that girls are also circumcised. I heard about it from a Somali girl who was my classmate in my primary school. She travelled to Somalia with her family. When they came back to Norway, she was told to attend a genital checkup to investigate whether or not she had been subjected to girl circumcision. That was the first time I have heard about this practice. Then I asked my mum and she explained to me about it. [Participant 23, boy]
I have heard that there are African countries, including Somalia, where girls are circumcised. I travelled to Somalia in 2009. That is when I heard about it and learned that there are two types of FC. [Participant 24, boy]
Discussion
This study is the first of its kind to explore the attitudes toward FC among young Somali–Norwegian boys and girls, and it presents a unique perspective of young generations who were born or brought up in Norway. The study shows that young Somali–Norwegians see being circumcised as a symbol of injustice and a violation of human rights, while being uncircumcised is seen as the norm. Moreover, circumcised girls are seen as survivors of torture. This perception clearly contradicts the widespread perception of FC among Somalis in Somalia, where being circumcised is the norm and being uncircumcised is an alien concept. This is supported by a previous quantitative study from Oslo, which shows that almost all Somali girls who were born in Norway were not circumcised.3 The study participants’ understanding of FC is shaped by the social environment in Norway, where FC is not only a crime, but also attracts strong public opposition by both mainstream and immigrant communities. An earlier anthropological study from Norway stated that FC, which is perceived as cleansing and a sign of womanhood in Somalia, has now been reinterpreted by Somali women in exile as “amputation and even mutilation”.20 It is highly likely that where FC is not a social norm, and is not associated with social status by the majority culture, some of the social forces influencing its continuation may be eroded.29 Thus, the finding that all the female participants in this study who were born or brought up in Norway (<4 years) were not circumcised is an indication of progress toward the abandonment of FC in Norway.
Having said this, in Norway there are inconsistencies between the public discourse on FC and the available empirical evidence.4 The public discourse supports the notion that FC exists in Norway. However, the evidence, including years of genital checkups of girls and a number of empirical studies, supports the notion that FC is no longer an immense threat to Norwegian girls. Yet, there are people who believe that FC is going “underground” in Norway or possibly that Norwegian girls outside Norway are being subjected to it, a perception that might be shaped by the public media. In 2007, the Norwegian TV station (NRK) aired a report that showed that 189 Somali–Norwegian girls were circumcised in Hargeisa, Somalia within 3 years. Professor Aud Talle, who interviewed 78 circumcisers in Hargeisa, found that none of them had ever circumcised a girl from Norway or another European country.24 In 2014, a Swedish journalist published a report that 30 Somali girls who attended the same class were subjected to FC, which received immediate attention from global media. Later, the Swedish report was dismissed as being overstated and false. While such (sensational) media information gradually fades away from our minds, its adverse effect may remain within the immigrant communities with a possible stigma “as mutilators”, as well as the subsequent perceived discrimination, which may eventually hinder integration. This is of particular concern because studies show that stigmatized individuals often become unreceptive to information, are defensive, and are reluctant to accept blame for their negative behavior.35
The point worth mentioning here is the fact that boys and girls who are born in Norway demonstrated a very limited knowledge about the practice of FC, which is the same practice that 98% of Somali women have experienced. This may be because they were born in a social environment where the practice of FC does not exist, which could be the result of acculturation. According to a quantitative model of acculturation by Padilla,31 there are two major constructs that are decisive for acculturations to occur, namely cultural awareness and ethnic loyalty. Cultural awareness involves individuals’ implicit knowledge of their cultures of origin, as well as that of their host community. Proficiency in the languages of each culture and knowledge of important historical events that have shaped the cultures are among the important aspects of acculturation. Individuals are less acculturated if they show more knowledge of their heritage cultures than they do of the new contact cultures, and if the persons possess more knowledge of the host cultures they are seen as being more acculturated. According to this model, the steepest decline in cultural knowledge occurs between the first and second generation. Hence, study participants who were born in Norway are the second generation of the Somali community in Norway. They are more comfortable in speaking Norwegian than Somali, and probably have a limited understanding of Somali culture and traditions, including the practice of FC. However, despite being born in Norway, it is vital to educate young boys and girls of Somali descent about the adverse effect of this practice. With limited knowledge about the adverse consequences of the practice, they can easily be misinformed in favor of the practice.
The rationale behind FC in Somalia is that young girls may not be eligible for marriage if left uncircumcised, as FC is considered important for the virginity and thus marriageability of girls.36 This study shows that young girls in Norway have either no idea about the connection between their marriage and FC, or they think it will not have any negative consequence on their marriage, while boys do not consider FC as important to marriageability. This finding is supported by a recent study (soon to be published), showing that two-thirds of women who sought clinical help for FC in Norway demanded to be de-infibulated, an indication that virginity created by FC is no longer relevant among women from FC-practicing countries living in Norway. It is generally known that culture is a dynamic process that changes with the circumstances that surround it. Nevertheless, although the number of immigrant traditions may easily dissolve with migration, the tradition of FC may differ from other traditions. It is a social norm in which a decision made by one family is dependent on the decision made by other families in the intermarrying community. Before families decide not to cut their daughter, they must have an assurance that their daughter will have a secure marriage without FC. This assurance may be obtained when families realize and accept that other families within the intermarrying group have abandoned the practice. At that stage, families may accept that FC has no incentive to anyone in their community, so the demand for circumcised girls in the marriage market may be replaced by a demand for uncircumcised girls. Most of the Somali participants in an earlier study mentioned that Somalis in Norway have abandoned the practice,3 which indicates that families accepted that others with similar mind-sets have abandoned the practice.
Young participants who have lived in Norway for less than a year believed that FC should continue. This is in line with previous findings from Oslo which showed that the majority of newly arrived immigrants have positive attitudes toward FC.3 This immigrant group came from an environment where being uncircumcised is unknown, and the circumcision of girls is a social norm that every family is expected to conform to.36 Subsequently, when they migrate to another country, they carry a positive attitude toward the practice of FC. Nonetheless, a prior study from Oslo showed an association between the duration of residence in Norway and negative attitudes toward FC.3 As young participants who come with positive attitudes toward FC continue being in Norway, where FC is not associated with any status, they will gradually meet other Muslims who do not circumcise their girls, fellow countrymen who abandoned the practice, and they will learn more about the position of Islam in regards to FC, as well as its negative health and social consequences. This increased exposure and knowledge about FC may motivate people to question the importance of the practice, and they are more likely to eventually abandon the practice.
While the findings from this study are in agreement with other findings that FC may be in the process of dissolution in Norway, it is worth mentioning that migration from FC-practicing countries to Norway is an ongoing process, and therefore the newly arrived immigrants carry positive attitudes toward the practice. This highlights the fact that the abandonment of FC among Norwegian immigrants is largely dependent on a global abandonment of FC. For this reason, the continuance of FC abandonment efforts in Norway is of paramount importance, and may be more efficient if immigrants are targeted early in their arrival. For example, knowledge of FC can be integrated into introduction program classes that immigrants attend shortly after their residence permit is accepted. Additionally, more of a focus should be given to the provision of quality care to women who have already experienced the practice. Our earlier study found that most participants were not aware of the health care available for women regarding FC, even when they needed de-infibulation. Subsequently, it seems important to conduct information campaigns to increase women’s awareness that health care is available for women who have experienced FC and where that care can be accessed.
This study has limitations. The results of the study reflect the perceptions of a limited number of young people who participated in the study, and not necessarily those of the entire Somali immigrant population in Oslo. Most of the views and opinions were, however, repeatedly expressed among different individuals in personal interviews, thereby increasing our confidence in the validity of the findings.
Disclosure
The authors declare that they have no competing interests in this work.
References
UNICEF. Female Genital Mutilation/Cutting: A statistical overview and exploration of the dynamics of change. UNICEF; 2013. Available from: http://www.unicef.org/media/files/UNICEF_FGM_report_July_2013_Hi_res.pdf. Accessed October 19, 2015. | ||
Gele AA, Johansen EB, Sundby J. When female circumcision comes to the West: Attitudes toward the practice among Somali Immigrants in Oslo. BMC Public Health. 2012;12:697. | ||
Gele AA, Kumar B, Hjelde KH, Sundby J. Attitudes towards female circumcision among Somali immigrants in Oslo: a qualitative study. Int J Womens Health. 2012;4:7–17. | ||
Beret B, Olav E. Forskningsbasert politikk? En gjennomgang av forskningen på tvangsekteskap, kjønnslemlestelse og alvorlige begrensninger av unges frihet, og av de politiske tiltakene på feltet. [Research based policy? An overview of research and the policy decisions and measures on Forced Marriages, Female genital mutilation and the restrictions and limitations to young people’s freedom] 2014. | ||
World Health Organization [homepage on the Internet]. Classification of female genital mutilation. Geneva: World Health Organization; 2008. Available from: http://www.who.int/reproductivehealth/topics/fgm/overview/en/. Accessed October 19, 2015. | ||
WHO study group on female genital mutilation and obstetric outcome, Banks E, Meirik O, et al. Female genital mutilation and obstetric outcome: WHO collaborative prospective study in six African countries. Lancet. 2006;367(9525):1835–1841. | ||
World Health Organization [homepage on the Internet]. Health complications of female genital mutilation. Geneva: World Health Organization; 2013 [updated 2013]. Available from: http://www.who.int/reproductivehealth/topics/fgm/health_consequences_fgm/en/. Accessed October 19, 2015. | ||
Vangen S, Stoltenberg C, Johansen RE, Sundby J, Stray-Pedersen B. Perinatal complications among ethnic Somalis in Norway. Acta Obstet Gynecol Scand. 2002;81(4):317–322. | ||
Lax RF. Socially Sanctioned Violence against Women: Female Genital Mutilation is its Most Brutal Form. Clinical Social Work Journal. 2000;28(4):403–412. | ||
UNICEF. Female genital mutilation/cutting: A statistical exploration. UNICEF; 2005. Available from: http://www.unicef.org/publications/files/FGM-C_final_10_October.pdf. Accessed October 19, 2015. | ||
Yoder PS, Noureddine A, Zhuzhuni A. Female Genital Cutting in the Demographic and Health Surveys: A Critical and Comparative Analysis. DHS Comparative Reports No 7. ORC Macro; 2004. Available from: http://dhsprogram.com/pubs/pdf/cr7/cr7.pdf. Accessed October 19, 2015. | ||
Bellmaker RH. Successful cultural change: the example of female circumcision among Israeli Bedouins and Israeli Jews from Ethiopia. Isr J Psychiatry Relat Sci. 2012;49(3):178–183. | ||
Mackie G. Ending footbinding and infibulation: A convention account. American Sociological Review. 1996;61(6):999–1017. | ||
Population Reference Bureau. Female genital mutilation/cutting: Data and Trends. Population Reference Bureau; 2010. Available from: http://www.prb.org/pdf10/fgm-wallchart2010.pdf. Accessed October 19, 2015. | ||
UNICEF. Women and Children in Somalia: A situation Analysis. UNICEF;1987. | ||
World Bank and the United Nations Population Fund. Female genital mutilation/cutting in Somalia. World Bank and the United Nations Population Fund; 2004. Available from: http://siteresources.worldbank.org/INTSOMALIA/Data%20and%20Reference/20316684/FGM_Final_Report.pdf. Accessed October 19, 2015. | ||
Dirie MA, Lindmark G. The risk of medical complications after female circumcision. East Afr Med J. 1992;69(9):479–482. | ||
Jaldesa GW, Askew I, Njue C, Wanjiru M. Female Genital Cutting among the Somali of Kenya and Management of its Complications. Population Council’s FRONTIERS Program report; 2005. Available from: http://www.popcouncil.org/uploads/pdfs/frontiers/FR_FinalReports/Kenya_Somali.pdf. Accessed October 19, 2015. | ||
Gele AA, Mbalilaki AJ. Overweight and obesity among African immigrants in Oslo. BMC Res Notes. 2013;6:119. | ||
Norwegian Ministries. Action Plan for Combating Female Genital Mutilation: Action Plan 2008–2011. Norwegian Ministries; 2008. Available from: https://www.politi.no/vedlegg/skjema/Vedlegg_668.pdf. Accessed October 19, 2015. | ||
Lien I. Tiltak mot kjønnslemlestelse: evaluering av OK-prosjektet – det nasjonale prosjektet for iverksetting av tiltak i handlingsplanen mot kjønnslemlestelse. NIBR-rapport 2005:8 [Measures to combat female genital mutilation: evaluation of the OK project: the national project for implementation of measures in the action plan to combat female genital mutilation. NIBR report 2005:8.] Oslo: Norwegian Institute for Urban and Regional Research. | ||
Liden H, Benzen T. Female Genital Mutilation in Norway. Institute of Social Research. 2008. Available from: http://www.google.no/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0CBwQFjAAahUKEwjWv9etyvHIAhWi83IKHTYiDag&url=http%3A%2F%2Fwww.samfunnsforskning.no%2Fcontent%2Fdownload%2F13981%2F397997%2Ffile%2FTfs_2_2008_web%5B1%5D.pdf&usg=AFQjCNHEXhfGZ8p1ECTZxq4WldO7JuzTHg&bvm=bv.106379543,d.bGQ. | ||
Johansen B. Experience and perceptions of pain, sexuality and childbirth: A study of female genital cutting among Somalis in Norwegian exile, and their health care providers [PhD thesis]. Oslo University; 2006. | ||
Talle A. Kalturens makt [The power of culture]. Kristiansand: Norwegian Academic Press; 2010. Norwegian. | ||
Tonje B. How big is the scope of female circumcision in Norway? In: Nina F, editor. Circumcision: Stop. Oslo: Cappelen Damm AS; 2010:77–93. | ||
Johnsdotter S. Somali women in western exile: Reassessing female circumcision in the light of Islamic teaching. Journal of Muslim Minority Affairs. 2010;23(2):361–373. | ||
Grassivaro Gallo P, Abdisamed M. Female circumcision in Somalia: anthropological traits. Anthropol Anz. 1985;43(4):311–326. | ||
Halila S, Belmaker RH, Abu RY, Froimovici M, Applebaum J. Disappearance of female genital mutilation from the Bedouin population of Southern Israel. J Sex Med. 2009;6(1):70–73. | ||
Makie G, John L. Social dynamics of abandonment of harmful practices: A new look at the theory. UNICEF Innocenti Research Centre; 2009. Available from: http://www.unicef-irc.org/publications/558. Accessed October 19, 2015. | ||
UNICEF. Coordinated strategy to abandon female genital mutilation/cutting in one generation. UNICEF; 2007. Available from: http://www.childinfo.org/files/fgmc_Coordinated_Strategy_to_Abandon_FGMC__in_One_Generation_eng.pdf. Accessed October 19, 2015. | ||
Padilla AM. The role of cultural awareness and ethnic loyalty in acculturation. In: Padilla AM, editor. Acculturation, theory, models, and some new findings. Boulder CO: Westview Pr; 1980:47–84. | ||
Shell-Duncan B, Herniund Y. Are there “stages of change” in the practice of female genital cutting? Qualitative research findings from Senegal and The Gambia. Afr J Reprod Health. 2006;10(2):57–71. | ||
Leininger M. Ethnography and ethnonursing: models and modes of qualitative data analysis. In: Leininger M, editor. Qualitative Research Methods in Nursing. New York, NY: Grune and Stratton; 1985:33. | ||
Taylor S, Bogdan R. Introduction to Qualitative Research Methods: The Search for Meanings. New York, NY: Wiley and Sons; 1984. | ||
Crocker J, Voekl K, Testa M, Major B. Social stigma: The affective consequences of attributional ambiguity. J Pers Soc Psychol. 1991;60:218–228. | ||
Gele AA, Bo BP, Sundby J. Have we made progress in Somalia after 30 years of interventions? Attitudes toward female circumcision among people in the Hargeisa district. BMC Res Notes. 2013;6:122. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.