Back to Journals » Clinical and Experimental Gastroenterology » Volume 19
Irritable Bowel Syndrome Prevalence in Patients with Inflammatory Bowel Disease in Remission: Single-Center Experience
Authors Golubovic O ![]() , Knezevic Ivanovski T, Kralj D
, Knezevic Ivanovski T, Kralj D ![]() , Mitrovic M, Milić A, Svorcan P
, Mitrovic M, Milić A, Svorcan P ![]() , Markovic S
, Markovic S
Received 18 February 2026
Accepted for publication 26 April 2026
Published 3 June 2026 Volume 2026:19 582517
DOI https://doi.org/10.2147/CEG.S582517
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Santosh Shenoy
Olga Golubovic,1 Tamara Knezevic Ivanovski,1 Djordje Kralj,1 Milos Mitrovic,1 Aleksandar Milić,1 Petar Svorcan,1,2 Srdjan Markovic1,2
1Department of Gastroenterology and Hepatology, University Hospital Medical Center Zvezdara, Belgrade, Serbia; 2Faculty of Medicine, University of Belgrade, Belgrade, Serbia
Correspondence: Olga Golubovic, Department of Gastroenterology and Hepatology, University Hospital Medical Center Zvezdara, Dimitrija Tucovica 161, Zvezdara, Belgrade, 11000, Serbia, Tel +381637612413, Fax +381113809650, Email [email protected]
Background: Irritable bowel syndrome (IBS) and inflammatory bowel diseases (IBD) are characterized by features of abdominal pain and changes in bowel habits, making it hard to differentiate between the two. Early studies that estimated prevalence of IBS in IBD patients defined remission based only on clinical scores, potentially overestimating IBS symptoms and underestimating subclinical inflammation. The aim of this study was to determine prevalence of IBS in IBD patients who are treated with biologics and have reached clinical, biologic and endoscopic remission, thereby applying a more stringent definition of remission.
Methods: This single-center cross-sectional study included 136 patients (68 patients with Crohn’s disease and 68 with ulcerative colitis) who are treated with biologics from December 2022 to June 2023 and have reached clinical, biologic and endoscopic remission. Clinical remission was defined as Crohn’s disease activity index (CDAI) ≤ 150 for patients with Crohn’s disease (CD), and Mayo partial score ≤ 1 for patients with ulcerative colitis (UC). Biologic remission was defined as faecal calprotectin (FCP) ≤ 250 ug/g, and endoscopic remission was defined as the absence of ulcerations for CD and Mayo subscore ≤ 1 for UC patients. The presence of IBS was defined by Rome IV criteria.
Results: A total of 28 (20.6%) patients in complete remission reported symptoms consistent with IBS, based on Rome IV criteria. The prevalence of IBS was higher in patients with Crohn’s disease than in those with ulcerative colitis (CD 27.9% (19/68) vs UC 13.2% (9/68), p = 0.034). Females and smokers with Crohn’s disease are more likely to report IBS symptoms.
Conclusion: Prevalence of IBS symptoms in IBD patients varies according to how remission is defined. When using stringent clinical, biological and endoscopic remission criteria, 20% of patients present with IBS symptoms, more commonly in those with CD.
Keywords: IBS, IBD, prevalence
Introduction
Irritable bowel syndrome (IBS), with a prevalence of approximately 11% in the general population, is one of the most common functional bowel disorders seen in clinical practice, and it is often a reason to seek a gastroenterology consultation.1,2 According to Rome IV criteria, IBS is defined as “recurrent abdominal pain, at least once a week, in the last 3 months, associated with two or more of the following – relation to defecation, change in stool frequency and/or change in appearance of the stool”, in the absence of abnormal findings on routine clinical tests that could explain the symptoms.3–5 Several organic gastrointestinal disorders can present in the same way as IBS, including, inflammatory bowel diseases (IBD).
IBD is a continuum of diseases that is comprised of Crohn’s disease (CD), ulcerative colitis (UC), and in a small percentage, indeterminate colitis.6 They are characterized by a wide spectrum of clinical symptoms, predominantly abdominal pain, diarrhea (watery or bloody in CD and UC respectively) and other alarm symptoms, like weight loss and fever.3 Unlike in IBS, laboratory findings of IBD patients can show anemia, leukocytosis, thrombocytosis, elevated CRP levels and elevated fecal calprotectin (FCP) levels.7 The course of inflammatory bowel disease is defined by periods of remission and relapses. In recent years, the prevalence of IBD has increased significantly, especially in high-income countries.8
Symptoms consistent with irritable bowel syndrome are often reported among patients with inflammatory bowel diseases that are considered to be in remission.9 However, since both entities are characterized by features of abdominal pain and changes in bowel habits, it is hard to differentiate between irritable bowel syndrome and relapse of inflammatory bowel disease.10 This can sometimes lead to unnecessary drug treatment escalation, whereas overlooking an IBD flare can have serious consequences for the patient.11,12 Early studies that estimated prevalence of IBS in IBD patients defined remission based only on clinical scores,13 not biologic and endoscopic markers of remission. This led to the conclusion that the prevalence of IBS in IBD patients is more than 40%, which is significantly higher than in the general population.2
Therefore, the aim of this study was to determine the prevalence of IBS in IBD patients, using more stringent criteria of remission, including clinical, laboratory and endoscopic parameters, in order to avoid overestimation of IBS and underestimation of subclinical inflammation, thus preventing inadequate treatment decisions.
Materials and Methods
Participants
This single-center cross-sectional study included all 136 patients (68 patients with Crohn’s disease and 68 with ulcerative colitis) that have reached clinical, biologic and endoscopic remission, out of 473 patients who were treated with biologics in our medical center, from December 2022 to June 2023. This study focused on patients treated with biologic therapy, as their standardized and regular monitoring, including fecal calprotectin levels and endoscopy, enables reliable assessment of clinical, biologic and endoscopic remission. Clinical remission was defined as Crohn’s disease activity index (CDAI) ≤ 150 for patients with Crohn’s disease, and Mayo partial score ≤ 1 for patients with ulcerative colitis. Biologic remission was defined as fecal calprotectin (FCP) ≤ 250 ug/g to ensure the comparability with prior studies, while endoscopic remission was defined as absence of ulcerations for CD and Mayo subscore ≤ 1 for UC patients. The presence of IBS was assessed by using validated diagnostic Rome IV criteria. All data were collected from medical records.
Data Analysis
For our analyses, we used the SPSS20 statistical package program. Numerical variables were described using mean and standard deviation or median and interquartile ranges, while categorical variables were described using frequency and percentage values. For correlation between the categorical variables, we used X2 test and Fisher’s test. For continuous variables, when the distribution was normal, we used two sample T-test, and non-parametric test (Mann Whitney U), when it was not. Statistical significance was defined as a value of p <0.05.
Results
Out of 473 IBD patients receiving biologic therapy from December 2022 to June 2023 in the University Hospital Medical Center “Zvezdara” at the time of our cross-sectional study, we have selected all 136 patients that have reached clinical, laboratory and endoscopic remission, based on previously defined criteria. The characteristics of our study population, divided into two groups (patients with Crohn’s disease and patients with ulcerative colitis) are shown in Tables 1 and 2, respectively. Among 136 patients in complete remission, a total of 28 (20.6%) patients reported symptoms consistent with irritable bowel syndrome, based on Rome IV criteria. The prevalence of IBS was higher in patients with Crohn’s disease than in those with ulcerative colitis (CD 27.9% (19/68) vs UC 13.2% (9/68), p = 0.03), and in the subgroup of patients with Crohn’s disease, it was more common in women (p = 0.01).
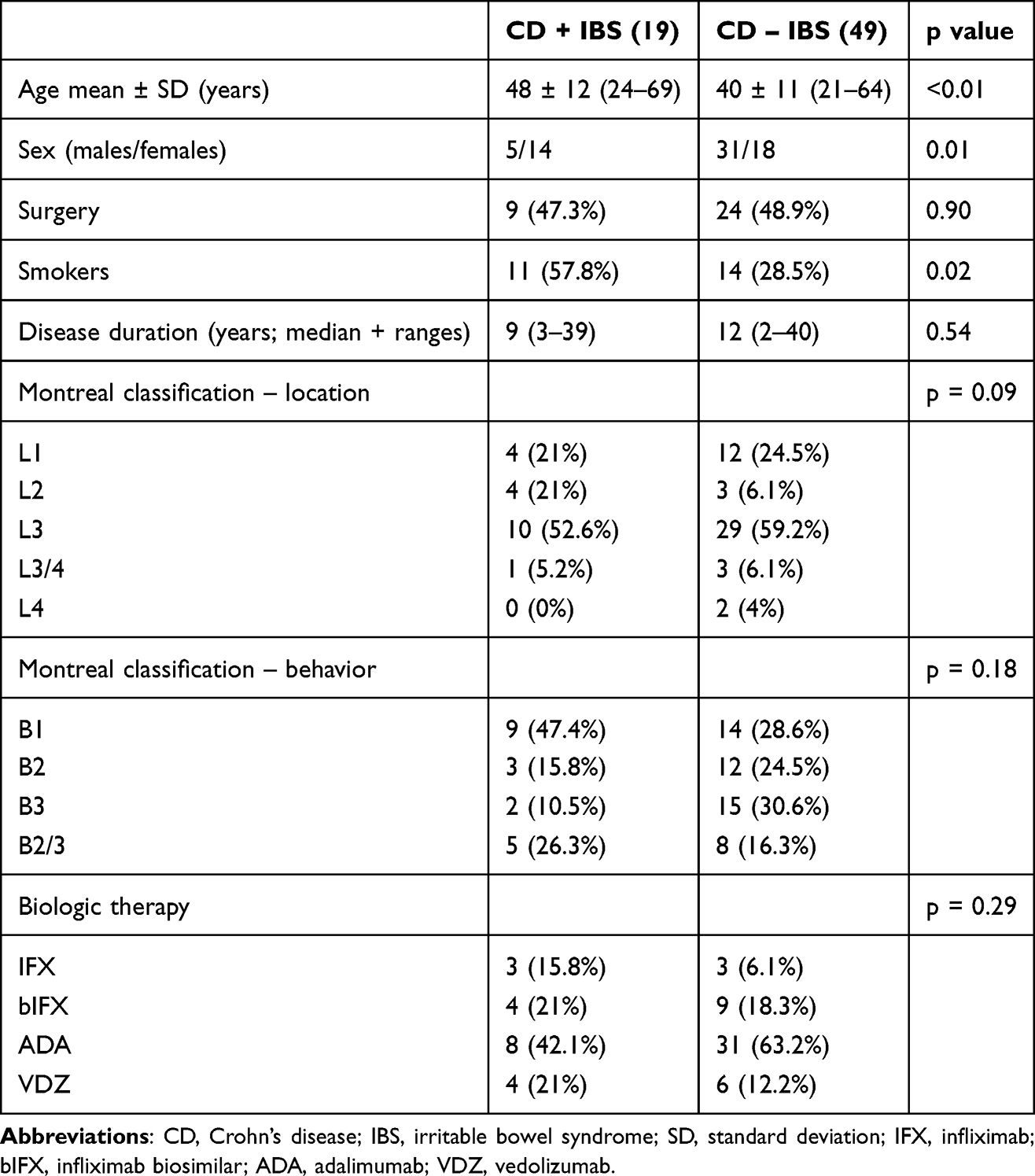 |
Table 1 Summary of CD Patients’ Characteristics |
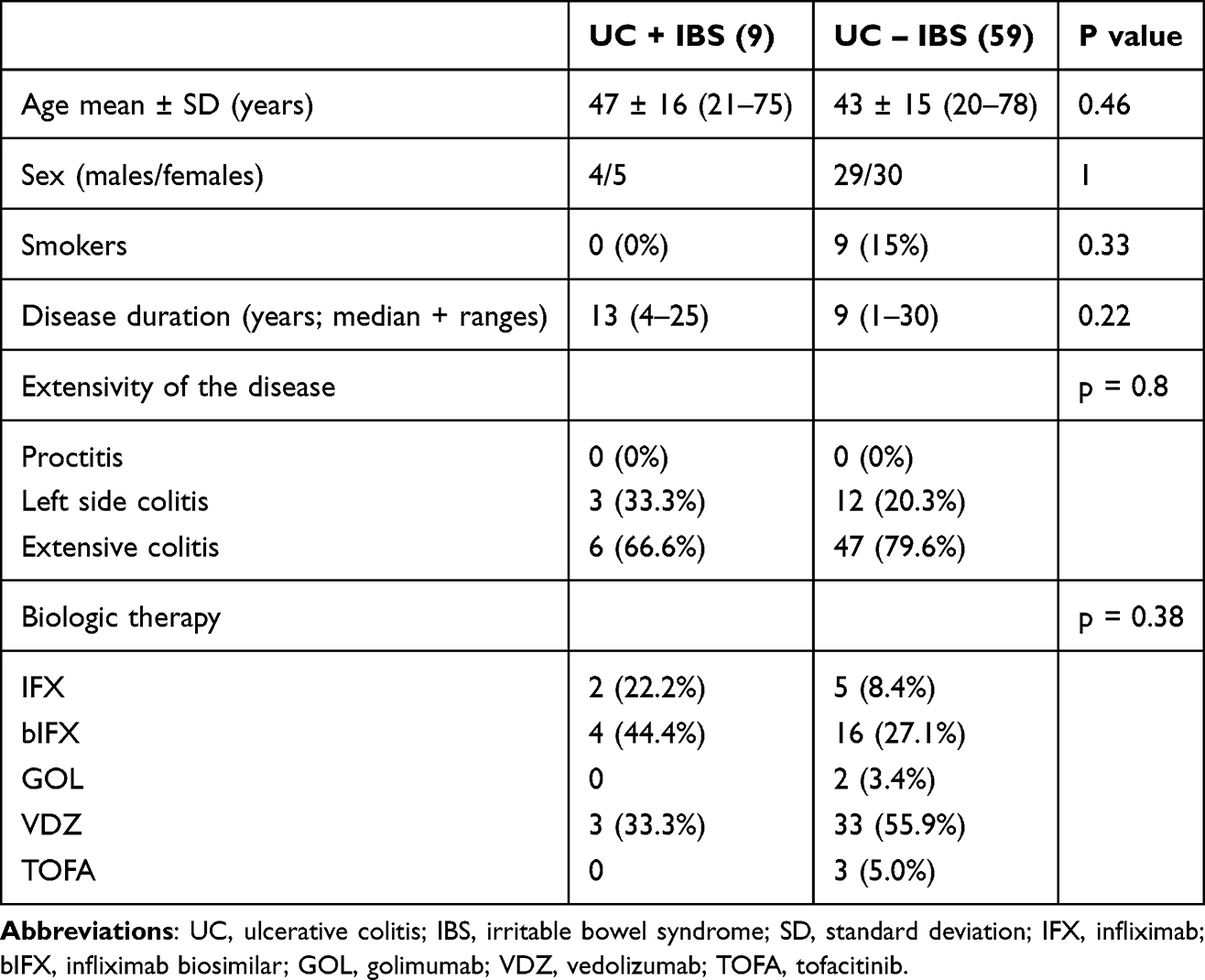 |
Table 2 Summary of UC Patients’ Characteristics |
In the group of patients with Crohn’s disease, there was no association between disease location or disease behavior based on Montreal classification and presence of IBS symptoms (p = 0.09 and p = 0.18 respectively).
Similarly, in patients with UC the extent of disease at diagnosis did not influence the occurrence of IBS symptoms (p = 0.08).
Previous surgery was not a significant risk factor for IBS (p = 0.27), nor was smoking (p = 0.08). However, when we compared smoking in subgroups of CD and UC patients individually, our data showed that patients with Crohn’s disease that smoke, are more likely to have IBS symptoms (p = 0.02), whereas no statistical significance was found in the subgroup of UC patients (p = 0.33).
Discussion
In clinical practice, remission of inflammatory bowel disease does not necessarily mean the absence of symptoms. IBD patients can still report symptoms that are of insufficient severity to be regarded as an IBD flare, but are consistent with irritable bowel syndrome. The primary question is whether IBD patients truly have coexisting IBS or if underlying inflammation is being overlooked.14 Many studies estimated the prevalence of IBS in IBD; however, initial studies used only clinical scores or FCP levels to define IBD remission.13 This led to the conclusion that IBS is more common in IBD patients than in general population. However, labeling our patient’s symptoms as IBS can postpone the decision to change treatment, which can later lead to poor outcome.15 Therefore, using stringent clinical, biological and endoscopic criteria for remission of IBD can help us avoid overestimation of IBS and underestimation of subclinical inflammation.
Firstly, our study showed that the prevalence of IBS-type symptoms in IBD patients is approximately 20%, when remission is defined based on clinical, laboratory and endoscopy criteria, which is significantly lower than in previous studies, when the only criteria for remission were clinical scores or levels of FCP.1–3,8,9 Our data concur with a systemic review and meta-analysis, done by Fairbrass et al, which showed that the pooled prevalence of IBS in IBD was around 23% when endoscopic assessment was used to define remission8 This raises the question: can implement more strict criteria, such as achieving pathohistological and radiological remission, further reduce the observed prevalence of IBS in patients with IBD?
Secondly, our study confirmed that symptoms consistent with IBS are more commonly seen in patients with Crohn’s disease than in those with ulcerative colitis.8,16 However, it is more difficult to exclude low-grade inflammation in patients with CD, since Crohn’s disease can affect all layers of the intestine wall, as well as all segments of the GI tract, including small bowel, which for the most part is not accessible to endoscopy.14
There was no difference in demographic characteristics of IBD patients with and without IBS overall. However, when we compared demographic characteristics in subgroups of patients with Crohn’s disease and patients with ulcerative colitis, we found that patients with Crohn’s disease that report IBS symptoms are more likely to be female (77.7% (14/18) vs 16.1% (5/31), p = 0.01), and they also tend to be older (48.05 vs 39.83 p < 0.01). This can be explained by the fact that women are more likely to experience IBS in general.17–19 Although the prevalence of IBS in general population decreases after the age of 50,20 our observation can be contributed to the longer duration of the inflammatory bowel disease in older patients.3
Hoekman et al have shown that Crohn’s disease patients with IBS are more likely to have ileal form of the disease, compared with CD patients without IBS1 This was not demonstrated in our study likely due to small sample size. Moreover, our data showed no difference in disease behaviour between Crohn’s disease patients with and without IBS symptoms, which is in line with previous studies.1,14
In our study, data showed no correlation between disease extensivity in patients with ulcerative colitis and presence of IBS symptoms, which is in concordance with previous studies.3,14,21
When it comes to smoking, overall comparison showed no statistical significance, but when we compared subgroups of patients with CD and UC separately, it showed that patients with Crohn’s disease that report IBS symptoms are more likely to smoke (p = 0.02). This data concurs with previous studies,14 and can be explained by negative effects of smoking on Crohn’s disease.22
Lastly, in our study IBS-type symptoms were not reported more frequently in the group of patients with previous surgery, which correlates with findings of Hoekman et al and Farrokhyar et al.1,9
There are, of course, limitations to this study. Our study was limited due to small sample size and likely presence of selection bias as we only included patients on biologic therapy, who are by definition patients with more severe and complicated disease. Our selection was due to the fact that these patients have tight control with regular visits, frequently done FCP levels and endoscopy, which allowed us to select patients in remission based on all these criteria. A formal power calculation was not performed, and given the relatively small sample size and low number of patients in certain subgroups, some analysis may have been underpowered to detect statistically significant differences. The absence of multivariate analysis also represents a limitation, as it precludes adjustment for potential cofounding factors. These limitations may be addressed by future multicentric studies and real-world data, which would provide larger and more diverse patient population, as well as the possibility for evaluating independent predictors of IBS symptoms in patients with IBD. FCP cut off value of 250 ug/g was used to ensure comparability with previous studies, since a threshold of > 250 ug/g has been commonly applied in the literature for active disease.23,24 However, novel studies show that FCP levels have higher accuracy at predicting remission at lower thresholds,25 which could in future studies further reduce the population of patients considered to be in remission. Even though we applied strict criteria to define remission, there is still a possibility that microscopic inflammation or small bowel inflammation was missed in patients with UC and Crohn’s disease respectively. Further studies that would include pathohistological and radiological criteria as well, are warranted.
Conclusion
Prevalence of IBS symptoms in IBD patients varies according to how remission is defined. When using stringent clinical, biologic and endoscopic criteria for definition of IBD remission, the prevalence of IBS symptoms is 20%. The symptoms are more common in patients with Crohn’s disease than in patients with ulcerative colitis, especially in women. Also, Crohn’s disease patients that smoke, are more likely to have IBS symptoms. These results should be interpreted in light of the study limitations, including cross-sectional design and small sample size.
Abbreviations
ADA, Adalimumab;bIFX, Infliximab biosimilar; CD, Crohn’s disease; CDAI, Crohn’s disease activity index; CRP, C reactive protein; FCP, fecal calprotectin; GOL, Golimumab; IBD, inflammatory bowel disease; IBS, irritable bowel syndrome; IFX, Infliximab; SD, standard deviation; SPSS, statistical package for the social sciences; TOFA, Tofacitinib; UC, ulcerative colitis; VDZ, Vedolizumab.
Data Sharing Statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained prior to its initiation from the Institutional Ethics Committee of the University Medical Centre “Zvezdara”, Belgrade, Serbia (No. IRB00009457). The study was conducted in accordance with national regulations and international guidelines for research involving human participants. The study included adult patients (≥18 years) diagnosed with Crohn’s disease or ulcerative colitis who were treated with biologic therapy at the University Medical Centre “Zvezdara” at the time of the cross-sectional study. Written informed consent was obtained from all participants prior to study commencement, permitting the use of their medical record data for research purposes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There has been no significant financial support for this work that could have influenced outcome.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Hoekman DR, Zeevenhooven J, D’Haens GR, Benninga MA. The prevalence of irritable bowel syndrome-type symptoms in inflammatory bowel disease patients in remission. Eur J Gastroenterol Hepatol. 2017;29(9):1086–7. PubMed PMID: 28639969. doi:10.1097/MEG.0000000000000921
2. Halpin SJ, Ford AC. Prevalence of symptoms meeting criteria for irritable bowel syndrome in inflammatory bowel disease: systematic review and meta-analysis. Off J Am Coll Gastroenterol ACG. 2012;107(10):1474. doi:10.1038/ajg.2012.260
3. Ozer M, Bengi G, Colak R, Cengiz O, Akpinar H. Prevalence of irritable bowel syndrome-like symptoms using Rome IV criteria in patients with inactive inflammatory bowel disease and relation with quality of life. Medicine. 2020;99(19):e20067. PubMed PMID: 32384473; PubMed Central PMCID: PMC7220554. doi:10.1097/MD.0000000000020067
4. Perera LP, Radigan M, Guilday C, et al. Presence of irritable bowel syndrome symptoms in quiescent inflammatory bowel disease is associated with high rate of anxiety and depression. Dig Dis Sci. 2019;64(7):1923–1928. PubMed PMID: 30725303. doi:10.1007/s10620-019-05488-8
5. Lacy BE, Mearin F, Chang L, et al. Bowel disorders. Gastroenterology. 2016;150(6):1393–1407.e5. doi:10.1053/j.gastro.2016.02.031
6. Yu YR, Rodriguez JR. Clinical presentation of Crohn’s, ulcerative colitis, and indeterminate colitis: symptoms, extraintestinal manifestations, and disease phenotypes. Semin Pediatr Surg. 2017;26(6):349–355. doi:10.1053/j.sempedsurg.2017.10.003
7. Vermeire S, Van Assche G, Rutgeerts P. Laboratory markers in IBD: useful, magic, or unnecessary toys? Gut. 2006;55(3):426–431. PubMed PMID: 16474109; PubMed Central PMCID: PMC1856093. doi:10.1136/gut.2005.069476
8. Fairbrass KM, Costantino SJ, Gracie DJ, Ford AC. Prevalence of irritable bowel syndrome-type symptoms in patients with inflammatory bowel disease in remission: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2020;5(12):1053–1062. PubMed PMID: 33010814. doi:10.1016/S2468-1253(20)30300-9
9. Farrokhyar F, Marshall JK, Easterbrook B, Irvine EJ. Functional gastrointestinal disorders and mood disorders in patients with inactive inflammatory bowel disease: prevalence and impact on health. Inflamm Bowel Dis. 2006;12(1):38–46. PubMed PMID: 16374257. doi:10.1097/01.mib.0000195391.49762.89
10. Teruel C, Garrido E, Mesonero F. Diagnosis and management of functional symptoms in inflammatory bowel disease in remission. World J Gastrointest Pharmacol Ther. 2016;7(1):78–90. PubMed PMID: 26855814; PubMed Central PMCID: PMC4734957. doi:10.4292/wjgpt.v7.i1.78
11. Jelsness-Jørgensen LP, Bernklev T, Moum B. Fatigue and disease-related worries among inflammatory bowel disease patients in remission; is it a reflection of coexisting IBS-like symptoms? A short report. J Psychosom Res. 2012;73(6):469–472. PubMed PMID: 23148817. doi:10.1016/j.jpsychores.2012.08.009
12. Barratt HS, Kalantzis C, Polymeros D, Forbes A. Functional symptoms in inflammatory bowel disease and their potential influence in misclassification of clinical status. Aliment Pharmacol Ther. 2005;21(2):141–147. doi:10.1111/j.1365-2036.2005.02314.x
13. Minderhoud IM, Oldenburg B, Wismeijer JA, van Berge Henegouwen GP, Smout AJPM. IBS-like symptoms in patients with inflammatory bowel disease in remission; relationships with quality of life and coping behavior. Dig Dis Sci. 2004;49(3):469–474. PubMed PMID: 15139501. doi:10.1023/b:ddas.0000020506.84248.f9
14. Keohane J, O’Mahony C, O’Mahony L, O’Mahony S, Quigley EM, Shanahan F. Irritable bowel syndrome-type symptoms in patients with inflammatory bowel disease: a real association or reflection of occult inflammation? Am J Gastroenterol. 2010. 105(8):1788,1789–94. quiz 1795. PubMed PMID: 20389294. doi:10.1038/ajg.2010.156
15. Jayasooriya N, Baillie S, Blackwell J, et al. Systematic review with meta-analysis: time to diagnosis and the impact of delayed diagnosis on clinical outcomes in inflammatory bowel disease. Aliment Pharmacol Ther. 2023;57(6):635–652. PubMed PMID: 36627691. doi:10.1111/apt.17370
16. Gracie DJ, Williams CJM, Sood R, et al. Negative effects on psychological health and quality of life of genuine irritable bowel syndrome–type symptoms in patients with inflammatory bowel disease. Clin Gastroenterol Hepatol. 2017;15(3):376–384.e5. PubMed PMID: 27189912. doi:10.1016/j.cgh.2016.05.012
17. Oka P, Parr H, Barberio B, Black CJ, Savarino EV, Ford AC. Global prevalence of irritable bowel syndrome according to Rome III or IV criteria: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2020;5(10):908–917. PubMed PMID: 32702295. doi:10.1016/S2468-1253(20)30217-X
18. Bryant RV, van Langenberg DR, Holtmann GJ, Andrews JM. Functional gastrointestinal disorders in inflammatory bowel disease: impact on quality of life and psychological status. J Gastroenterol Hepatol. 2011;26(5):916–923. PubMed PMID: 21214889. doi:10.1111/j.1440-1746.2011.06624.x
19. Berrill JW, Green JT, Hood K, Campbell AK. Symptoms of irritable bowel syndrome in patients with inflammatory bowel disease: examining the role of sub-clinical inflammation and the impact on clinical assessment of disease activity. Aliment Pharmacol Ther. 2013;38(1):44–51. PubMed PMID: 23668698. doi:10.1111/apt.12335
20. Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: a meta-analysis. Clin Gastroenterol Hepatol. 2012;10(7):712–721.e4. doi:10.1016/j.cgh.2012.02.029
21. Simrén M, Axelsson J, Gillberg R, Abrahamsson H, Svedlund J, Björnsson ES. Quality of life in inflammatory bowel disease in remission: the impact of IBS-like symptoms and associated psychological factors. Am J Gastroenterol. 2002;97(2):389–396. PubMed PMID: 11866278. doi:10.1111/j.1572-0241.2002.05475.x
22. Rozich JJ, Holmer A, Singh S. Effect of lifestyle factors on outcomes in patients with inflammatory bowel diseases. Am J Gastroenterol. 2020;115(6):832–840. PubMed PMID: 32224703; PubMed Central PMCID: PMC7274876. doi:10.14309/ajg.0000000000000608
23. Colombel JF, Panaccione R, Bossuyt P, et al. Effect of tight control management on Crohn’s disease (CALM): a multicentre, randomised, controlled Phase 3 trial. Lancet. 2017;390(10114):2779–2789. PubMed PMID: 29096949. doi:10.1016/S0140-6736(17)32641-7
24. Lasson A, Öhman L, Stotzer PO, et al. Pharmacological intervention based on fecal calprotectin levels in patients with ulcerative colitis at high risk of a relapse: a prospective, randomized, controlled study. United Eur Gastroenterol J. 2015;3(1):72–79. PubMed PMID: 25653861; PubMed Central PMCID: PMC4315686. doi:10.1177/2050640614560785
25. Singh A, Bhardwaj A, Sharma R, et al. Predictive accuracy of fecal calprotectin for histologic remission in ulcerative colitis. Intest Res. 2025;23(2):144–156. doi:10.5217/ir.2024.00068
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.