Back to Journals » Clinical Ophthalmology » Volume 11
Irrigation dynamic pressure-assisted hydrodissection during cataract surgery
Authors Masuda Y, Iwaki H, Kato N, Takahashi G, Oki K, Tsuneoka H
Received 12 October 2016
Accepted for publication 28 December 2016
Published 14 February 2017 Volume 2017:11 Pages 323—328
DOI https://doi.org/10.2147/OPTH.S124528
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Supplementary video of iH during phacoemulsification cataract surgery.
Views: 361575
Yoichiro Masuda,1 Hisaharu Iwaki,2 Noriko Kato,1 Genichiro Takahashi,1 Kotaro Oki,3 Hiroshi Tsuneoka4
1Department of Ophthalmology, The Jikei University, Katsushika Medical Center, 2Iwaki Eye Clinic, 3Oki Eye Surgery Center, 4Department of Ophthalmology, The Jikei University, School of Medicine, Tokyo, Japan
Abstract: The irrigation dynamic pressure-assisted hydrodissection technique (irrigation-hydro [iH]) does not require performing manual hydrodissection using a syringe and cannula to achieve cortical-capsular cleavage during cataract surgery. Since the iH technique uses the phaco tip to intentionally vacuum the intraocular fluid in order to induce the irrigation dynamic pressure for cortical-capsular cleavage, there is a reduction in the intraocular pressure (IOP) from the bottle-height-dependent hydrostatic pressure. Thus, since the peak irrigation pressure derived from the phaco tip sleeve will be limited by the height of the irrigation fluid bottle, this is advantageous in helping to avoid excessively high IOP during cortical-capsular hydrodissection. Using this technique, we were able to effectively perform phacoemulsification without complications in 607 of 609 cataract eyes. Our findings show that utilization of the iH technique would be of benefit to patients, as it prevents high-pressure hydrodissection-related complications, such as capsular block syndrome and tears in the anterior hyaloid membrane during cataract surgery.
Keywords: cataract surgery, hydrodissection, irrigation pressure, hydrodissection-related complication, capsular block syndrome, anterior hyaloid membrane tear, FLACS
Introduction
Modern phacoemulsification cataract surgery commonly uses manual cortical cleaving hydrodissection, which is performed via a syringe and cannula (manual-hydro). This technique requires the presence of an adequate injected fluid pressure in order to achieve the cortical-capsular cleavage.1–3 Intraocular pressure (IOP) during this procedure depends on several factors, including the volume of the injected fluid, the volume and type of the injected ophthalmic viscosurgical device (OVD), the incision size, and the surgeon’s technique. Due to these factors, an excessively high pressure can occur within the endocapsular space, the capsule-zonule complex, and the posterior chamber–anterior hyaloid membrane barrier area, which can potentially induce severe complications.4–6 Complications associated with the high-pressure hydrodissection include capsular block syndrome, posterior capsular rupture, anterior capsule tear extension through the posterior capsule, tears in the anterior hyaloid membrane, and acute aqueous misdirection syndrome.5–14 Although there is a low rate of incidence, an occurrence can lead to more severe complications, such as endophthalmitis, retinal break, and retinal detachment. Therefore, surgeons need to carefully ensure that these complications do not occur.
The peak irrigation pressure derived from the phacoemulsification tip (phaco tip) sleeve is limited by the height of the irrigation fluid bottle (ie, hydrostatic pressure). Therefore, it is important to not exceed this hydrostatic pressure during the phacoemulsification cataract surgery. The bottle-height-dependent hydrostatic pressure can change in accordance with the 1) pressure loss in the irrigation line; 2) static pressure in the eye (IOP); and 3) dynamic pressure from the phaco tip sleeve during irrigation flows. Since the irrigation dynamic pressure is equal to the irrigation kinetic energy, this can potentially be used for cortical-capsular cleavage. Based on these known findings, we propose that the irrigation dynamic pressure could be utilized for cortical-capsular cleavage, thereby reducing the intraocular stress that is normally induced by high pressure. Thus, in this study, we describe a new technique for irrigation dynamic pressure-assisted hydrodissection during cataract surgery, which we refer to as irrigation-hydro (iH).
Patients and methods
This study retrospectively reviewed the medical records of 609 consecutive eyes that underwent iH during phacoemulsification cataract surgery. The surgeries were performed by three different surgeons. The data recorded included age, gender, preexisting ocular pathology, ocular axial length, nuclear hardness, preoperative and postoperative best corrected visual acuities (BCVAs), intraocular lens (IOL) material and position, and information on any complications that occurred. The study was performed in accordance with the Declaration of Helsinki ethical principles for medical research involving human subjects. The study protocol was approved by the ethics committee of Jikei University School of Medicine. The patient’s consent to review their medical records was not deemed necessary by the Institutional Review Board of Jikei University School of Medicine due to the retrospective nature of the study.
Surgical techniques
iH technique
The peak irrigation pressure derived from the phaco tip sleeve is limited by the irrigation fluid bottle height. Therefore, we hypothesized that the irrigation dynamic pressure from the tip of the sleeve could be used to cleave the cortical-capsular layer without causing an IOP that was excessively higher than the bottle-height-dependent hydrostatic pressure. In a preliminary study, we confirmed that the irrigation dynamic pressure derived from the phaco tip sleeve could cleave the porcine lens cortical-capsular layer when using the open-sky method with a 50 cm bottle height, which is commonly utilized in phacoemulsification cataract surgery (Video S1). We created the iH technique as a way of replacing the manual-hydro technique. When using this technique during phacoemulsification cataract surgery, one or two stages are performed during the procedure (Figures 1 and 2).
Phacoemulsification instrument parameters used for iH mode
To ensure that the irrigation dynamic pressure is sufficient for achieving an effective cortical-capsular cleavage, the phaco instrument settings for iH are very important. The two different phaco machines used in this study were: 1) the Constellation Vision System (Alcon Laboratories, Inc., Fort Worth, TX, USA), which contains a 0.9 mm diameter phaco tip with a micro-sleeve and 2) the Centurion Vision System (Alcon Laboratories, Inc.), which contains a 0.9 mm diameter phaco tip with an ultra-sleeve. The phacoemulsification parameters used by the Constellation Vision System included the following: vacuum system, Venturi pump; vacuum pressure, 200 mmHg; irrigation pressure, 60 cm H2O; and ultrasound power, 0. The phacoemulsification parameters used by the Centurion Vision System included the following: vacuum system, peristaltic pump; vacuum pressure, 350 mmHg; irrigation pressure, 36 mmHg; aspiration flow rate, 45 cc/min, and ultrasound power, 0.
Posterior iH technique
After the phaco tip is passed under the anterior capsule within the possible range, the phaco tip is then used to sculpt a vertical groove (Figure 1A). Once the sculpturing of the vertical groove is completed, centrifugal force is exerted by the phacoemulsification tip on the base of the left-hand wall of the trench and by the hook on the base of the right-hand wall of the trench (referred to as cross action), with vacuuming of the intraocular fluid by the phaco tip. In addition, there is induction of the irrigation flow from the phaco tip sleeve into the posterior cortical-capsular layers (Figure 1B). As a result of the vertical groove sculpture, the two hemispheres are cracked into two and the irrigation dynamic pressure from the tip sleeve causes cleavage of the posterior cortical-capsular layer. Through repetition of this method at several different points along the vertical groove sculpture, along with further repetitions after inverting the tip and hook position (referred to as non-cross action), these actions make it possible to achieve complete posterior iH. In soft cataract surgery cases, however, this stage is not required.
 | Figure 1 Posterior iH technique. |
Anterior iH technique
Following placement of the phaco tip under the capsulorhexis edge, the intraocular fluid is vacuumed, which induces the irrigation flow into the anterior cortical-capsular layer. The induced irrigation dynamic pressure from the phaco tip sleeve then cleaves the anterior, equatorial cortical-capsular layers (Figure 2A and B). One of the beneficial options of this technique is that the irrigation flow from the tip sleeve can be induced by depressing the side-port by a hook, with the irrigation flow able to compensate for the loss of intraocular fluid.
 | Figure 2 Anterior iH technique. |
Cortical cleavage can be effectively performed using this one- or two-stage iH technique. The following section describes the actual surgical procedure.
iH during phacoemulsification cataract surgery
Posterior iH following vertical groove sculpture
After completion of the initial steps of the cataract surgery (incision, OVD injection, and continuous curvilinear capsulorhexis [CCC]), the phaco tip is inserted into the anterior chamber without performing the manual-hydro procedure. After the phaco tip is passed under the anterior capsule and the anterior capsular-connection is separated within the possible range (Figure 3A), a conventional vertical groove is sculpted in accordance with the divide and conquer method (Figure 3B). Subsequently, posterior iH is performed sequentially at both ends and at the center of the vertical groove sculpture (Figure 3C). When performing the posterior iH, we found that the bottom of the vertical groove sculpture was the best place to use when completing the procedure. The vertical groove sculpture is cracked into two hemispheres, and the irrigation dynamic pressure from the tip sleeve is used to cleave the posterior cortical-capsular layer (Figure 3C). For effective posterior iH, the side hole of the sleeve is directed forward onto the posterior capsule, thereby making it possible for the irrigation flow to effectively cleave the posterior capsular connection. As a result, the posterior cortical-capsular connection can then be separated. If the anterior cortical-capsular connection is also separated using just this procedure, the anterior iH can be skipped, with the lens then freed from the cortical-capsular connection and rotated circumferentially by the phaco tip and a hook for removal. Videos S2 and S3 present this technique in detail.
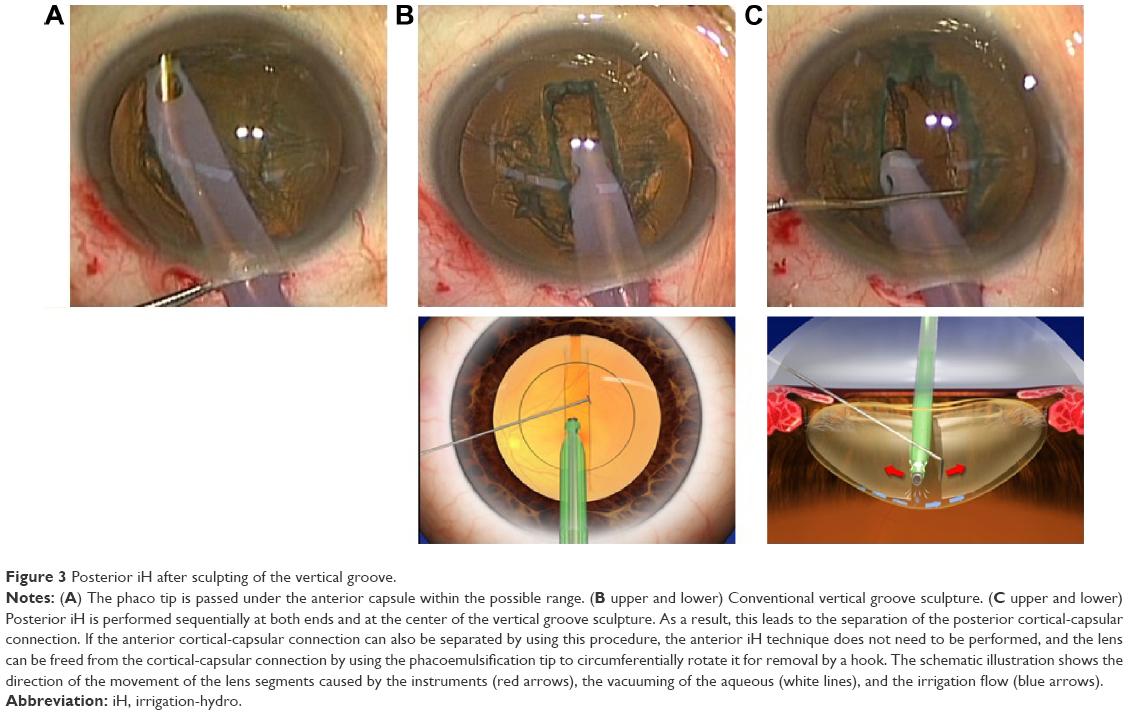 | Figure 3 Posterior iH after sculpting of the vertical groove. |
Anterior iH following posterior iH (if needed)
Anterior iH is performed after the posterior iH, if needed (Figure 4). After placing the phaco tip under the left capsulorhexis edge, the anterior cortical-capsular iH is performed on the left hemi-nucleus (Figure 4A) to free it from the cortical-capsular connection. Subsequently, anterior cortical-capsular iH is performed on the right hemi-nucleus (Figure 4B), which is then also freed. Cortical-capsular separation is now complete and the lens can be rotated circumferentially (Figure 4C). Videos S2 and S3 present the technique in detail.
 | Figure 4 Anterior iH after posterior cleavage, if needed. |
The remainder of the procedure, including the cataract removal and IOL implantation, is then performed in a normal manner.
Results
The patients included 352 females and 257 males, with an average age of 72.9 years old (range 32–93 years). Anterior ocular segment conditions present at surgery included pseudoexfoliation syndrome in 17 eyes, phacodonesis in 15 eyes, inadequate mydriasis in 45 eyes (moderate: 39 eyes, poor: 6 eyes), shallow anterior chamber in 13 eyes, corneal opacity in 3 eyes, previous traumatic eye in 1 eye, anterior capsule calcification in 4 eyes, posterior polar cataract in 9 eyes, post-laser iridotomy in 6 eyes, and intraoperative floppy iris syndrome in 1 eye. Posterior ocular segment conditions present at surgery included diabetic retinopathy in 10 eyes, age-related macular degeneration (AMD) in 11 eyes, glaucoma in 20 eyes, epiretinal membrane in 10 eyes, chorioretinal atrophy in 1 eye, and a previously vitrectomized eye in 2 eyes. The ocular axial length was <21.5 mm in 10 eyes, 21.5–26 mm in 556 eyes, 26–30 mm in 42 eyes, and >30 mm in 1 eye. The nucleus hardness was grade 1 or softer in 22 eyes, grade 2 in 285 eyes, grade 3 in 274 eyes, and grade 4 or harder in 28 eyes.
A polyacrylic IOL was implanted in 609 eyes, including 606 IOLs implanted in the bag and 3 IOLs implanted out of the bag. In 6 eyes with poor mydriasis, the pupil was dilated using a Malyugin pupil expansion device or sphincterotomy.
Posterior capsule rupture occurred in 2 eyes (0.3%). In both cases, the IOL was implanted out of the bag and the final BCVA was better than the preoperative BCVA. Although a CCC tear occurred in 4 eyes, iH and phacoemulsification were successfully performed in all of the eyes without expansion of the tear to the posterior capsule.
Preoperative BCVA was better than 20/40 in 377 eyes (61.9%), 20/40–20/80 in 157 eyes (25.8%), and worse than 20/100 in 75 eyes (12.3%). Postoperative BCVA was better than 20/40 in 590 eyes (96.7%), 20/40–20/80 in 12 eyes (2.0%), and worse than 20/100 in 7 eyes (1.1%). The low visual acuities found in the 7 patients were related to AMD, diabetic retinopathy, epiretinal membrane, glaucoma, retinal vein occlusion, optic neuropathy, and amblyopia.
Discussion
The iH technique presented here is used for cortical-capsular cleavage during phacoemulsification cataract surgery. The mechanism underlying this technique involves the use of the irrigation dynamic pressure derived from the phaco tip sleeve to cleave the cortical-capsular connection. Therefore, the key element in this technique is the intentional induction of the irrigation flow from the tip sleeve within the endocapsular space; that is, elimination of the intraocular fluid from the endocapsular space. As a result, this induces an irrigation flow that compensates for the volume of the intraocular fluid that is lost during the procedure. Therefore, we intentionally removed the intraocular fluid via the phaco tip and then used it to induce the irrigation flow from the sleeve. The net result of this action is that there is a reduction in the IOP during the iH procedure. Furthermore, as the IOP does not increase above the irrigation bottle-height-dependent hydrostatic pressure, it is then possible to perform cortical-capsular hydrodissection by using the irrigation flow within the range of the expected peak IOP. In addition, we can perform the iH without any absorption and/or rupture of the capsule, as the nucleus stretches the capsule centrifugally and the ultrasound power is zero.
The utility of the iH technique was shown in 607 of 609 consecutive cases, with the procedure performed without complications in cases with pseudoexfoliation syndrome, phacodonesis, brunescent/white cataract, small pupil, shallow anterior chamber, and long or short ocular axial length, all of which are considered to be high risks in cataract surgery.15,16
Complications associated with the manual-hydro procedure are caused by stress due to high pressure within the endocapsular space, capsule–zonule complex, and posterior chamber–anterior hyaloid membrane barrier area.4–14 The iH technique may be able to solve these problems, as the intraocular peak pressure depends on the bottle-height hydrostatic pressure, which does not lead to the development of additional excessive pressure during the phacoemulsification surgery. Capsular block syndrome induced by the manual-hydro procedure during femtosecond laser-assisted cataract surgery (FLACS) has also recently been reported to occur because of the expansion of the endocapsular volume by the laser-induced intracapsular gas and cortical changes.9 In cases with FLACS, it is important to reduce the intracapsular gas before the hydrodissection procedure in order to avoid high-pressure complications. Thus, the vertical groove sculpture procedure that is performed in iH might reduce the intracapsular gas and be safer for FLACS as compared to the manual-hydro procedure. Since phacoemulsification techniques now tend to use smaller incisions,17 high-pressure hydrodissection-related complications may occur more frequently due to this decreased incision size. Furthermore, in order to reduce these high-pressure complications, several different methods are now being used instead of the manual-hydro procedure.18,19 In addition, when using the iH technique, cataract surgery can be performed without encountering the potential high pressures that occur during the manual-hydro procedure.
Conclusion
In conclusion, the iH technique was developed for the purpose of separating the cortical-capsular connection in order to permit the removal of the lens. This technique uses a bottle-height-dependent limited peak pressure, which may contribute to avoidance of high-pressure complications. This technique also utilizes common phacoemulsification instruments, which should permit the straightforward adoption of the iH technique by experienced cataract surgeons.
Acknowledgments
We thank Toshinori Okamoto, Kunihiro Asakawa, and Akiko Kiriyama for their helpful suggestions regarding this technique.
Disclosure
The authors report no conflicts of interest in this work.
References
Faust KJ. Hydrodissection of soft nuclei. Am Intra-Ocular Implant Soc J. 1984;10(1):75–77. | ||
Fine IH. Cortical cleaving hydrodissection. J Cataract Refract Surg. 1992;18(5):508–512. | ||
Varsavada AR, Singh R, Apple DJ, Trivedi RH, Pandey SK, Werner L. Effect of hydrodissection on intraoperative performance: randomized study. J Cataract Refract Surg. 2002;28(9):1623–1628. | ||
Khng C, Packer M, Fine IH, Hoffman RS, Moreira FB. Intraocular pressure during phacoemulsification. J Cataract Refract Surg. 2006;32(2):301–308. | ||
Kawasaki S, Suzuki T, Yamaguchi M, et al. Disruption of the posterior chamber-anterior hyaloid membrane barrier during phacoemulsification and aspiration as revealed by contrast-enhanced magnetic resonance imaging. Arch Ophthalmol. 2009;127(4):465–470. | ||
Kawasaki S, Tasaka Y, Suzuki T, et al. Influence of elevated intraocular pressure on the posterior chamber-anterior hyaloid membrane barrier during cataract operations. Arch Ophthalmol. 2011;129(6):751–757. | ||
Ota I, Miyake S, Miyake K. Dislocation of the lens nucleus into the vitreous cavity after standard hydrodissection. Am J Ophthalmol. 1996;121(6):706–708. | ||
Miyake K, Ota I, Ichihashi S, Miyake S, Tanaka Y, Terasaki H. New classification of the capsular block syndrome. J Cataract Refract Surg. 1998;24(9):1230–1234. | ||
Roberts TV, Sutton G, Lawless MA, Jindal-Bali S, Hodge C. Capsular block syndrome associated with femtosecond laser-assisted cataract surgery. J Cataract Refract Surg. 2011;37(11):2068–2070. | ||
Hurvitz LM. Posterior capsular rupture at hydrodissection (letter). J Cataract Refract Surg. 1991;17(6):866. | ||
Osher RH, Yu BC, Koch DD. Posterior polar cataracts: a predisposition to intraoperative posterior capsular rupture. J Cataract Refract Surg. 1990;16(2):157–162. | ||
Marques FF, Marques DMV, Osher RH, Osher JM. Fate of anterior capsule tears during cataract surgery. J Cataract Refract Surg. 2006;32(10):1638–1642. | ||
Mackool RJ, Sirota M. Infusion misdirection syndrome. J Cataract Refract Surg. 1993;19(6):819. | ||
Gryzmowski A, Prasad S. Acute aqueous misdirection syndrome: pathophysiology and management. J Cataract Refract Surg. 2014;40(12):2167. | ||
Gupta A, Singh J, Dhillon B. Cataract classification system for risk stratification in surgery. J Cataract Refract Surg. 2011;37(7):1363–1364. | ||
Butler TK. Risk stratification and assessment in cataract surgery. J Cataract Refract Surg. 2012;38(1):184. | ||
Tsuneoka H, Shiba T, Takahashi Y. Ultrasonic phacoemulsification using a 1.4 mm incision: clinical results. J Cataract Refract Surg. 2002;28(1):81–86. | ||
Masuda Y, Tsuneoka H. Hydrodissection-free phacoemulsification surgery: mechanical cortical cleaving dissection. J Cataract Refract Surg. 2014;40(8):1327–1331. | ||
Soda M, Yaguchi S. Phacoemulsification without hydrodissection: semi-crater and split technique. J Cataract Refract Surg. 2015;41(6):1132–1136. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.