Back to Journals » Clinical Ophthalmology » Volume 20
IOL Calculators Variability in Toric Lens Planning: A Retrospective Paired Comparison of the Planning Discrepancies Between the Johnson & Johnson Toric Calculator and ESCRS-Hosted Engines
Authors Klimek M, Tamberger M ![]() , Schauer S, Botic D
, Schauer S, Botic D ![]() , Mihaltz K, Vécsei-Marlovits PV
, Mihaltz K, Vécsei-Marlovits PV
Received 16 April 2026
Accepted for publication 27 May 2026
Published 3 June 2026 Volume 2026:20 615859
DOI https://doi.org/10.2147/OPTH.S615859
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Michal Klimek,1,2 Maximilian Tamberger,1,2 Stephanie Schauer,1,2 Dejan Botic,1,2 Kata Mihaltz,1,2 Pia Veronika Vécsei-Marlovits1,2
1Department of Ophthalmology, Klinik Hietzing, Wiener Gesundheitsverbund, Vienna, Austria; 2Karl Landsteiner Institut für Prozessoptimierung und Qualitätsmanagement in der Katarakt-Chirurgie, Vienna, Austria
Correspondence: Michal Klimek, Department of Ophthalmology, Klinik Hietzing, Wiener Gesundheitsverbund, Wolkersbergenstraße 1, Vienna, 1130, Austria, Tel +43 664 8132466, Fax +43 1 801 10 2266, Email [email protected]
Purpose: To determine the frequency, magnitude, and direction of toric intraocular lens (IOL) planning discrepancies between the Johnson & Johnson (J&J) official calculator and European Society of Cataract and Refractive Surgeons (ESCRS)-hosted toric engines, and to identify preoperative predictors of clinically relevant disagreements.
Methods: This retrospective, single-center study included 182 eyes of 127 patients undergoing toric IOL implantation (TECNIS). For each eye, planning results were generated using identical biometric data (IOLMaster 700, CASIA2 keratometry) across all calculators. The primary comparison was J&J with posterior corneal astigmatism correction enabled (PCA-ON) versus ESCRS-Barrett – secondary comparisons included Kane, EVO 2.0, and Hoffer QST. Clinically relevant discrepancy (ClinRel) was defined as a toric cylinder step difference ≥ 1 and/or axis difference ≥ 10°. Logistic regression, including Firth-penalized estimation, identified predictors of ClinRel. The primary analysis set comprised one eye per patient (n=127).
Results: ClinRel between J&J PCA-ON and Barrett occurred in 59.8% of eyes (76/127; 95% CI: 51.1– 68.0%), driven almost only by step differences. J&J PCA-ON recommended a higher step in 56.7% of eyes, with only 2.4% showing the opposite. Discrepancies were concentrated in with-the-rule eyes (72.3%) and nearly absent in against-the-rule eyes (5.6%). Rates were higher for secondary engines (Kane 83.8%, EVO 74.4%, Hoffer QST 76.7%). An Alpins-style paired-planning analysis yielded a Correction Index of 1.20, with the Difference Vector concentrated at the vertical meridian (84°). Posterior corneal astigmatism grade was the strongest independent predictor (Firth-adjusted OR = 203.5; p=0.014). An empirical PCA threshold of 0.36 D (Youden index; sensitivity 91.6%, specificity 56.0%) identified eyes at elevated risk of calculator disagreement.
Conclusion: Calculators’ variability in toric IOL planning is substantial (~60% of eyes) and concentrated in with-the-rule eyes with elevated posterior corneal astigmatism. In this subgroup, consulting multiple calculators is recommended; in against-the-rule eyes, calculator choice rarely alters the recommendation.
Keywords: toric IOL, calculator comparison, posterior corneal astigmatism, toric planning variability, ESCRS toric calculator, Johnson & Johnson toric calculator
Introduction
Modern phacoemulsification cataract surgery has progressed into a refractive procedure in which the predictability of postoperative refraction is a major factor of patient satisfaction and clinical success.1 Recent series indicate that only approximately 73% of eyes achieve a postoperative prediction error within ±0.50 D, with inaccuracies in axial length, keratometry, and anterior chamber depth measurements accounting for approximately 36%, 22%, and 42% of total IOL power-calculation errors, respectively.2,3 In eyes with regular corneal astigmatism, toric intraocular lens (IOL) implantation is an established strategy to reduce postoperative refractive cylinder and reduce spectacle dependence for distance vision.4
The effectiveness of toric correction depends on reliable preoperative biometry, correct modeling of corneal optics – including the contribution of the posterior corneal curvature – accurate selection of the toric cylinder and implantation axis, and precise intraoperative alignment.5 Koch et al demonstrated that posterior corneal astigmatism (PCA) is steep vertically in more than 85% of eyes, creating against-the-rule refractive astigmatism, and that ignoring this contribution leads to systematic overcorrection in with-the-rule (WTR) and undercorrection in against-the-rule (ATR) eyes6,7 These observations automatically triggered the development of modern toric calculators that incorporate PCA, either through internal algorithmic estimation or by accepting clinically measured posterior corneal data.8,9
Several toric calculators are now available, including the Barrett toric calculator, the Kane toric formula, the Emmetropia Verifying Optical (EVO) 2.0 formula, and the Hoffer QST formula, all accessible through, for example, the European Society of Cataract and Refractive Surgeons (ESCRS) online toric platform. In parallel, the Johnson & Johnson (J&J) toric calculator provides a dedicated platform for the TECNIS toric IOL family, incorporating an optional posterior cornea adjustment.10,11 Published comparative studies have primarily focused on the refractive accuracy of these calculators, reporting mean absolute prediction errors of approximately 0.5 to 0.6 diopters across modern formulae, with generally comparable performance between Barrett, Kane, and EVO approaches.12–15
However, from the perspective of a high-volume public cataract clinic, a complementary question is pragmatically important: how often and by how much do toric planning recommendations differ between calculators when identical biometric data is being used? Toric IOL planning outputs are not direct measurement parameters – they are the result of calculator-specific modeling choices that may differ in approach to the handling of posterior corneal astigmatism, the conversion between corneal and IOL planes, the treatment of surgically induced astigmatism, and rounding rules related to discrete toric steps within a given IOL platform.8,9,11 Calculator-dependent variability in these modeling pathways may introduce planning discrepancies that affect clinical decision making and workflow standardization, even if without differences in postoperative refractive accuracy.
To our knowledge, no study has systematically quantified the frequency and magnitude of toric planning discrepancies between the J&J toric calculator and ESCRS-hosted engines using a paired within-eye design with standardized inputs. The purpose of this retrospective study was therefore to determine how frequently toric IOL planning recommendations differ between these calculators, to characterize the direction and magnitude of these discrepancies, and to identify the preoperative factors – in particular posterior corneal astigmatism – that could predict clinically relevant planning disagreements.
Methods
The study adhered to the general ethical standards of the Declaration of Helsinki and Good Clinical Practice guidelines. It was approved by the Ethics Committee of the City of Vienna (Ethikkommission der Stadt Wien; MA15-EK 26–035-VK). The requirement for individual informed consent was waived by the Ethics Committee of the City of Vienna owing to the retrospective, observational design of the study and the use of fully anonymized routine clinical data.
This single-center, retrospective, paired planning study was conducted at the Department of Ophthalmology, Klinik Hietzing (Wiener Gesundheitsverbund), Vienna, Austria. The analysis included data of all consecutive eyes receiving toric IOL implantation (TECNIS DIU platform) between January 2023 and March 2026 for which the routine preoperative measurements required to run the toric planning calculators were still available.
The inclusion criteria were: (1) cataract surgery with implantation of a toric IOL (DIU platform) during the study period, (2) availability of complete preoperative IOLMaster 700 biometry (axial length, anterior chamber depth, lens thickness) and CASIA2 keratometry within 90 days before surgery, (3) regular corneal astigmatism suitable for toric correction, (4) sufficient data to reconstruct paired calculator outputs under standardized modeling assumptions, and (5) availability of a preoperative CASIA2 report, as anterior keratometric inputs were standardized from CASIA2 under a protocol-defined analyzed-zone rule (central 3.0 mm). Eyes were excluded if they had prior corneal or intraocular surgery (except uncomplicated intravitreal injections), corneal pathology (eg. ectasia, significant scarring), incomplete or poor-quality measurements, documented irregular astigmatism, major intraoperative complications or non-standard modeling assumptions that could not be harmonized across calculator runs.
Data extraction and management were performed by a single investigator (M.K.) using a structured electronic case-report form with pre-defined fields for every biometric, keratometric, and calculator-output variable. Source documents (CASIA2 reports, IOLMaster 700 printouts, and the original calculator outputs archived at the time of preoperative planning) were re-checked against the database after data entry. To reduce the risk of bias, all calculator pathways were run under fully standardized inputs (identical IOLMaster 700 biometry, identical CASIA2 anterior keratometry, fixed target refraction, incision meridian, and SIA for every eye), so that the only element varying between paired runs was the calculator itself. Eyes were processed consecutively in chronological order of surgery, without selection of calculator outputs after the fact. The principal investigator (P.V.V.-M.) reviewed a random 10% sample of completed case-report entries against the original source documents; no systematic discrepancies were identified.
For each eligible eye, toric planning outputs were generated (or retrospectively taken from archived documents) using a standardized input framework in which all calculator runs received identical biometric inputs (IOLMaster 700), identical anterior keratometry values (CASIA2), and identical modeling assumptions (target refraction, incision meridian, and surgically induced astigmatism). The only element that differed between paired runs was the calculator. Pathway A used the Johnson & Johnson toric calculator with posterior corneal astigmatism correction enabled (PCA-ON). Pathway B used the ESCRS toric platform with the Barrett engine (PCA predicted) as primary comparator; the Kane, EVO 2.0, and Hoffer QST engines were evaluated as secondary comparators.
Toric cylinder recommendations were organized by the DIU step scale using a nearest-step mapping rule. The primary endpoint was the proportion of eyes with a clinically relevant planning discrepancy between J&J PCA-ON and ESCRS-Barrett, defined a priori as a toric cylinder step change ≥ 1 step and/or an absolute implantation axis difference ≥ 10°. Secondary endpoints included discrepancy metrics for additional ESCRS engines, within-eye variability across ESCRS engines, predicted residual astigmatism differences analyzed both as Thibos power-vector components (J0/J45 decomposition) and as an Alpins-style paired analysis of the planning outputs (Difference Vector, Magnitude of Error, Correction Index, and Angle of Error between J&J PCA-ON and ESCRS-Barrett), and predictors of clinically relevant discrepancies. A pre-specified sensitivity analysis repeated the primary comparison with J&J PCA set to OFF to quantify the contribution of posterior cornea handling within the J&J pathway.
Statistical Analysis
Sample size considerations – with an expected primary endpoint proportion (ClinRel) of approximately 0.55–0.65 and a target confidence-interval half-width of ±8 percentage points (95% CI), the minimum required sample for a one-proportion estimate was approximately 144 eyes. The available cohort (N=182 all-eyes; N=127 primary set) therefore exceeded this requirement and provided a 95% CI half-width of approximately ±8.4 percentage points at the observed proportion. The primary analysis set included one eye per patient to avoid within-patient correlation – if both eyes were eligible, the first operated eye was selected. Proportions were reported with Wilson 95% confidence intervals. Univariate and multivariable logistic regression models were used to identify predictors of clinically relevant discrepancies (ClinRel). Potential predictors included magnitude of keratometric astigmatism, anterior astigmatism class (WTR/ATR/oblique), posterior corneal astigmatism magnitude and vector components (J0/J45), axial length, anterior chamber depth, lens thickness, and white-to-white distance. Because standard maximum-likelihood logistic regression showed evidence of quasi-complete separation for the posterior corneal astigmatism predictor, Firth-penalized logistic regression was performed as a pre-specified sensitivity analysis.16 To characterize the relationship between posterior corneal astigmatism magnitude and clinically relevant discrepancies, ClinRel rates were computed across predefined posterior CYL bins. An empirical threshold was identified using Youden index analysis, maximizing the sum of sensitivity and specificity for the prediction of ClinRel. To complement the Thibos power-vector analysis and to provide Alpins-compatible reporting of astigmatism vector differences, the paired planning outputs of J&J PCA-ON and ESCRS-Barrett were additionally summarized using Alpins-style metrics applied at the planning level: the Difference Vector (DV) between predicted residual astigmatism vectors (magnitude and meridian), the signed Magnitude of Error (ME) defined as the IOL-plane toric cylinder of J&J PCA-ON minus that of ESCRS-Barrett, the Correction Index (CI) defined as the ratio of the J&J PCA-ON to the ESCRS-Barrett IOL-plane toric cylinder, and the Angle of Error (AE) between the two recommended axes. The Index of Success (IOS) requires postoperative refraction and is therefore not applicable to this planning-level comparison. Continuous predictors were checked for non-linearity. All tests were two-sided with α=0.05. Analyses were performed using R version 4.5.3 (R Foundation for Statistical Computing, Vienna, Austria).17
Results
A total of 182 eyes from 127 patients were included in the analysis (all-eyes set with 88 OD, 94 OS). The primary analysis set (one eye per patient) included 127 eyes. Modeling assumptions were fully standardized across all calculator runs: target refraction −0.30 D, incision meridian 135°, and SIA 0.40 D for all eyes.
Baseline biometric and corneal characteristics are shown in Table 1. Mean axial length was 24.09 ± 1.41 mm, mean anterior chamber depth 3.19 ± 0.35 mm, and mean anterior corneal astigmatism (CASIA2) 2.45 ± 0.80 D. Posterior corneal astigmatism had a mean magnitude of 0.47 ± 0.22 D. The majority of eyes showed with-the-rule (WTR) anterior astigmatism (137 eyes, 75.3%), followed by against-the-rule (ATR; 36 eyes, 19.8%) and oblique (9 eyes, 4.9%). The distribution of J&J PCA-ON recommended DIU steps was: DIU150 (9 eyes), DIU225 (50), DIU300 (58), DIU375 (30), DIU450 (14), DIU525 (20), and DIU600 (1).
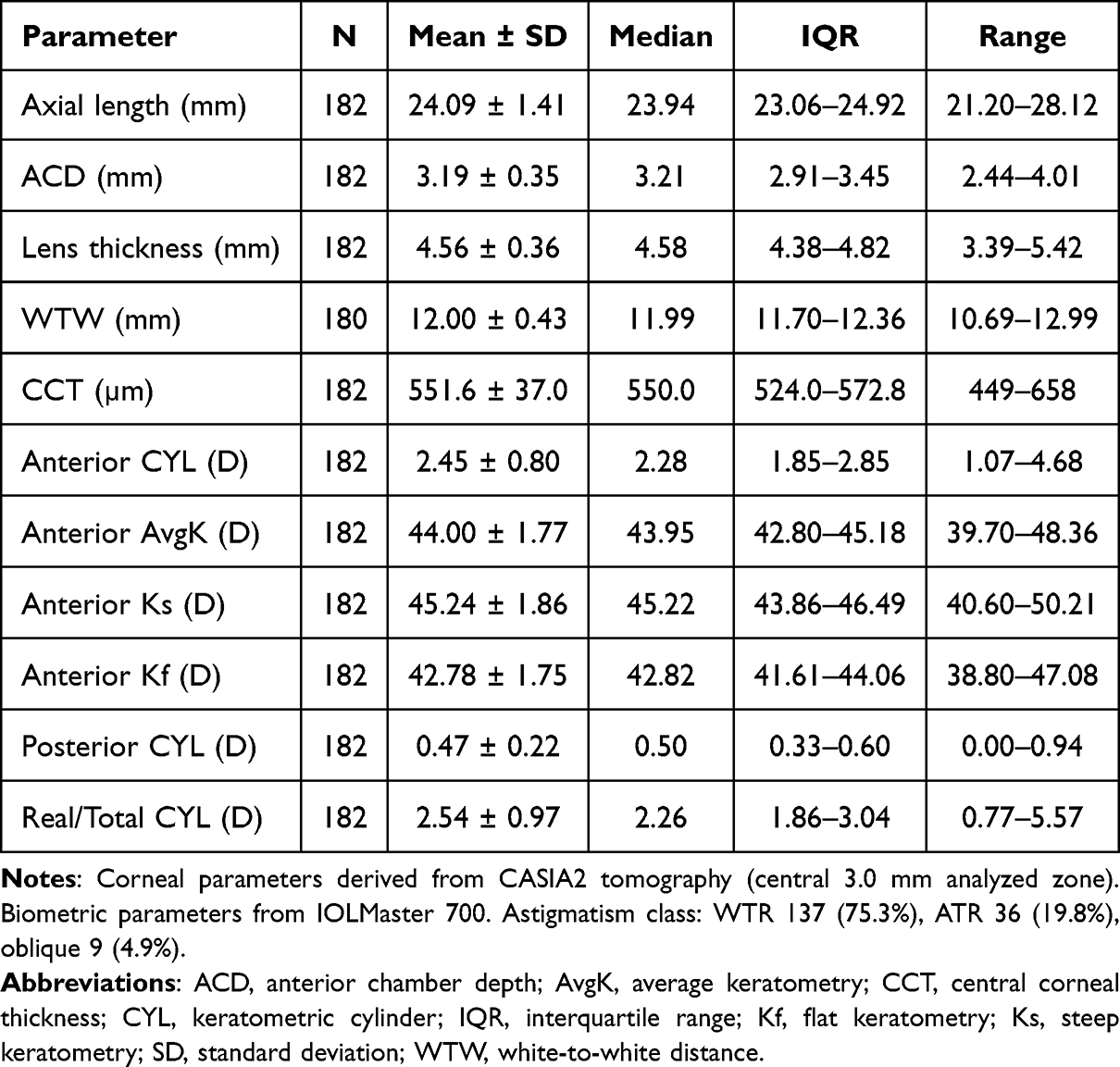 |
Table 1 Baseline Biometric and Corneal Characteristics (All Eyes, N = 182) |
Primary Outcome: Clinically Relevant Planning Discrepancy (J&J PCA-ON vs. ESCRS-Barrett)
In the primary analysis set (n=127), ClinRel between the J&J calculator with PCA-ON and the ESCRS-Barrett engine occurred in 76 of 127 eyes (59.8%; 95% CI: 51.1–68.0%; Table 2, Panel A). The discrepancy was almost entirely driven by toric cylinder step differences: 75 of 127 eyes (59.1%; 95% CI: 50.4–67.2%) showed a step difference ≥ 1 on the DIU scale, and only 3 eyes (2.4%; 95% CI: 0.8–6.7%) showed an axis difference ≥ 10°. The all-eyes sensitivity set (n=182) resulted in a consistent ClinRel rate of 58.8% (95% CI: 51.5–65.7%).
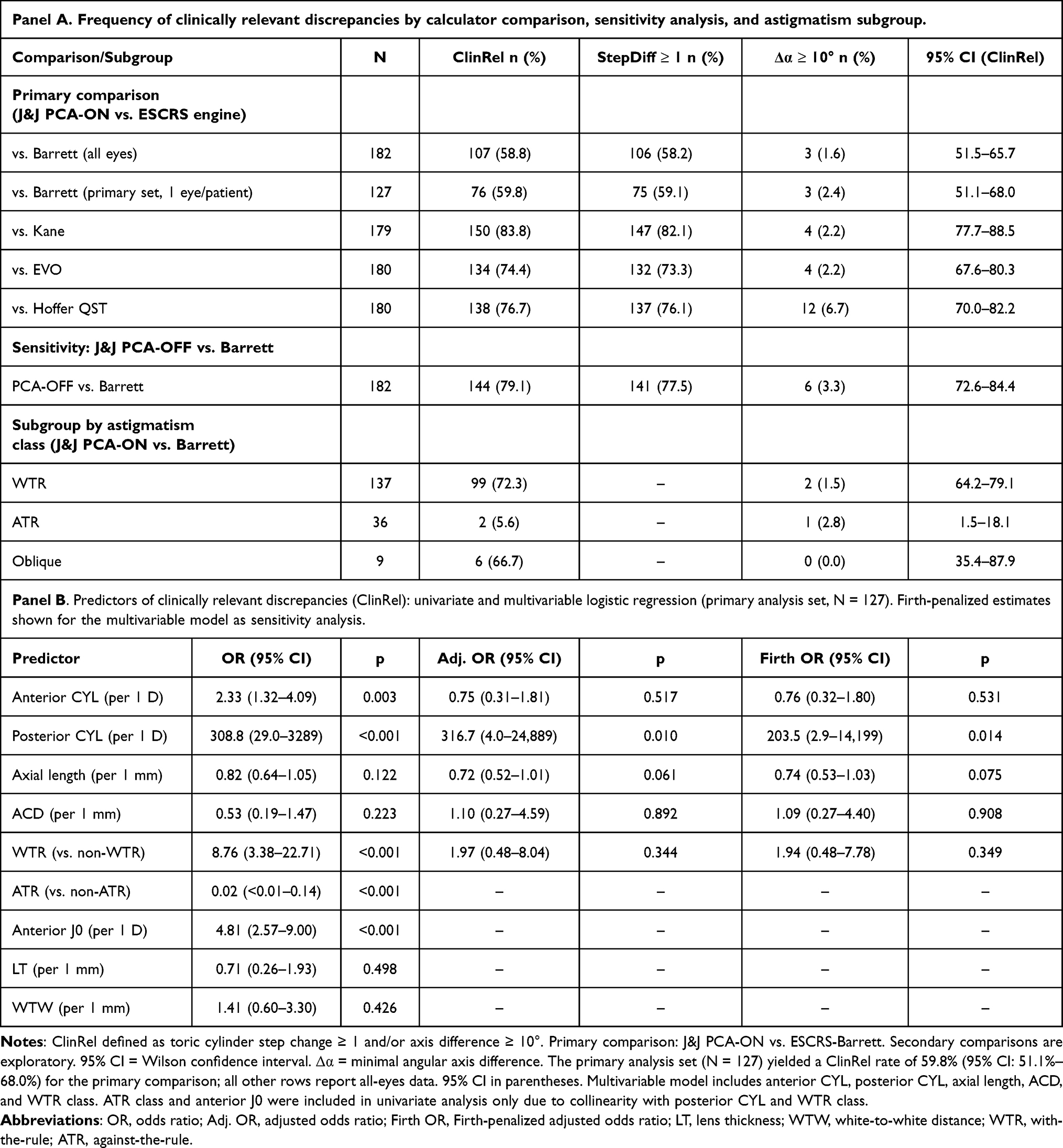 |
Table 2 Calculator Discrepancy Outcomes and Predictors of Clinically Relevant Planning Discrepancies |
The majority of inconsistent eyes differed by one DIU step (58.3% in the primary set), with only one eye (0.8%) differing by two steps. The direction of disagreement was strongly unidirectional (Figure 1B): in the primary set, J&J PCA-ON recommended a higher DIU step than Barrett in 72 eyes, whereas Barrett recommended the higher step in only 3 eyes (mean signed step difference: +0.55 ± 0.56; median: 1). Axis discrepancies were small overall (mean Δα: 2.1° ± 7.3°; median: 1°; IQR: 0°–2°).
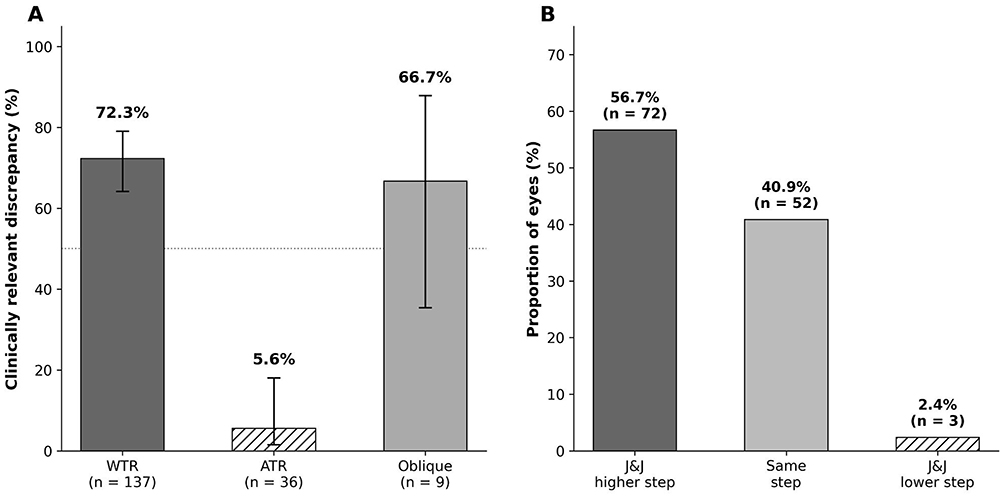 |
Figure 1 Subgroup analysis and directionality of toric planning discrepancies (J&J PCA-ON versus ESCRS-Barrett). (A) Proportion of eyes with clinically relevant discrepancies (ClinRel) stratified by anterior astigmatism phenotype (all eyes, n=182). Error bars represent Wilson 95% confidence intervals. The dotted horizontal line indicates 50%. (B) Directionality of toric step disagreement (primary analysis set, one eye per patient, n=127). Bars show the proportion of eyes in which J&J PCA-ON recommended a higher DIU step than Barrett (black), the same step (gray), or a lower step (hatched). Absolute eye counts are shown above each bar. Abbreviations: WTR, with-the-rule; ATR, against-the-rule. |
Secondary Outcomes
Calculator Discrepancies with Additional ESCRS Engines
Discrepancy rates between J&J PCA-ON and the secondary ESCRS engines were consistently higher than for the primary Barrett comparison (Table 2, Panel A and Figure 2). ClinRel rates were 83.8% for Kane (n=179), 74.4% for EVO (n=180), and 76.7% for Hoffer QST (n=180). Step differences ≥ 1 represented the majority of these discrepancies in all comparisons (Figure 2).
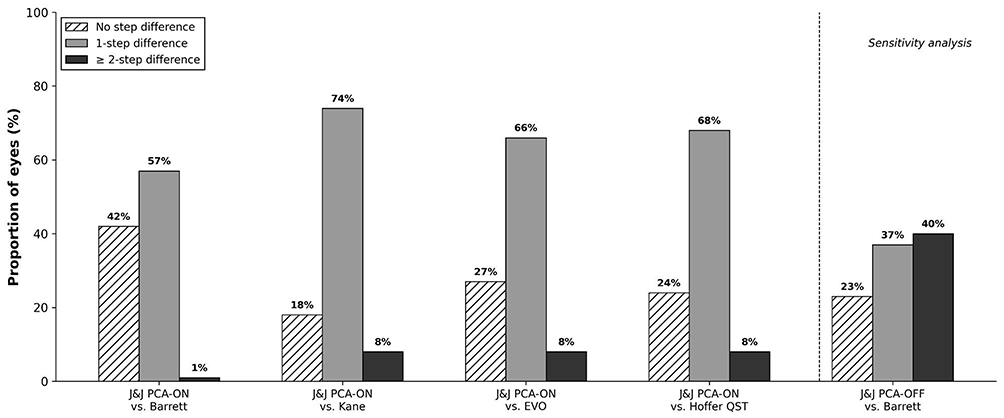 |
Figure 2 Distribution of toric cylinder step differences between the Johnson & Johnson (J&J) toric calculator and ESCRS-hosted engines (n=179-182). For each pairwise comparison, bars represent the proportion of eyes with no step difference (hatched), a 1-step difference (gray), or a ≥ 2-step difference (black) on the DIU scale. The four left-hand comparisons show J&J with posterior corneal astigmatism correction enabled (PCA-ON) versus ESCRS-Barrett (primary comparison), Kane, EVO 2.0, and Hoffer QST. The right-hand comparison, separated by a dashed line, shows the pre-specified sensitivity analysis with J&J PCA set to OFF versus Barrett. Percentages are rounded to the nearest integer. |
Within-Eye Variability Across ESCRS Engines
Among ESCRS engines, 86 of 181 eyes (47.5%; 95% CI: 40.4–54.8%) showed a range of ≥ 1 DIU step across the four engines for the same eye. Axis disagreement ≥ 10° between at least two ESCRS engines occurred in 29 of 181 eyes (16.0%).
Predicted Residual Astigmatism Discrepancy (Thibos and Alpins Frameworks)
In the Thibos power-vector decomposition, the mean difference in predicted residual astigmatism between J&J PCA-ON and Barrett was −0.018 ± 0.094 D for J0 and 0.005 ± 0.064 D for J45, indicating a small systematic offset in the horizontal/vertical component. Re-expressed as an Alpins-style Difference Vector (DV) between the two calculators’ predicted residual astigmatism vectors, the per-eye DV magnitude was 0.208 ± 0.100 D (median 0.200 D; IQR 0.14–0.27 D) in the primary set, with the per-eye DV meridian clustering around the vertical (mean 84°, median 84°), (Figure 3A) – anatomically consistent with the meridian at which posterior corneal astigmatism predominantly acts in with-the-rule eyes. The Alpins-style paired-planning summary of the IOL-plane toric cylinder revealed a signed Magnitude of Error (J&J PCA-ON minus Barrett) of +0.43 ± 0.40 D and a Correction Index (J&J PCA-ON / Barrett) of 1.20 (IQR 1.00–1.33; CI > 1 in 60.6% and CI < 1 in only 2.4% of eyes), indicating that J&J PCA-ON systematically prescribed approximately 20% more toric cylinder than Barrett (Figure 3B). The Angle of Error between the two recommended axes was negligible (mean 1.8° ± 7.4°; median 1°), confirming that calculator disagreement is almost entirely a magnitude phenomenon rather than an axis-orientation phenomenon.
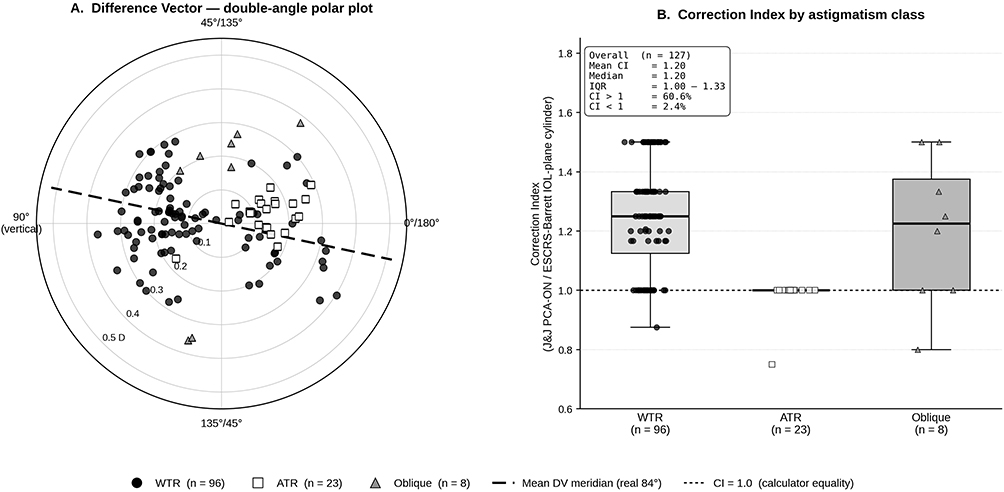 |
Figure 3 Alpins-style paired-planning vector analysis (J&J PCA-ON vs ESCRS-Barrett). (A) Double-angle polar plot of the per-eye Difference Vector (DV) between the predicted residual astigmatism vectors of J&J PCA-ON and ESCRS-Barrett, stratified by anterior astigmatism class (with-the-rule, against-the-rule, oblique). Angular labels around the rim denote the real astigmatism Meridian (single-angle); the double-angle convention places vectors at real meridian θ on the polar plot at 2θ. Radial distance represents the DV magnitude in diopters at the corneal plane. The black dashed line indicates the mean DV meridian (real 84°), computed as the magnitude-weighted circular mean of the per-eye DVs and anatomically consistent with the meridian at which posterior corneal astigmatism predominantly acts in with-the-rule eyes. (B) Distribution of the Correction Index (J&J PCA-ON/ESCRS-Barrett IOL-plane toric cylinder) by anterior astigmatism class. Boxes show the interquartile range and median; whiskers extend to the most extreme non-outlier values; individual eye-level points are overlaid. The black dotted line marks the line of calculator equality (CI = 1.0). In with-the-rule eyes the Correction Index is systematically above unity (median 1.25), indicating an approximately 20–25% over-prescription of toric cylinder by the J&J pathway relative to ESCRS-Barrett. In against-the-rule eyes the two calculators are in near-complete agreement (CI = 1.00 in nearly all eyes). Inset summary statistics refer to the full cohort. Abbreviations: WTR, with-the-rule; ATR, against-the-rule; CI, Correction Index; DV, Difference Vector. |
Sensitivity Analysis: J&J PCA-OFF vs. Barrett
With J&J posterior corneal astigmatism handling set to OFF, the ClinRel rate increased to 144 of 182 eyes (79.1%; 95% CI: 72.6–84.4%), compared with 58.8% with PCA-ON (Table 2, Panel A). The proportion of eyes with a step difference ≥ 1 increased to 77.5%. Notably, the proportion of eyes with a step difference ≥ 2 increased from 1.1% with PCA-ON to 40.1% with PCA-OFF, indicating the expected logical conclusion, that disabling posterior cornea correction not only increased the frequency of discrepancies but also substantially increased their magnitude.
Planning Robustness: Decision Margin (J&J PCA-ON)
The J&J decision margin – defined as the difference in predicted residual astigmatism between the recommended and the best alternative DIU step – had a mean of 0.220 ± 0.175 D (median: 0.225 D; IQR: 0.09–0.35 D). 41 eyes (22.5%) had a small decision margin (<0.10 D). Notably, 7 eyes (3.8%) showed negative decision margins, indicating that the recommended DIU step had a higher predicted residual astigmatism than the nearest alternative step – in these eyes, the alternative step typically produced a lower residual magnitude but with an axis flip, so that the algorithm favored preserving the original axis orientation over pure residual minimization.
Subgroup Analysis by Astigmatism Class
The ClinRel rate differed markedly by anterior astigmatism phenotype (Table 2, Panel A and Figure 1A). In WTR eyes, 99 of 137 (72.3%; 95% CI: 64.2–79.1%) showed a clinically relevant discrepancy, compared with only 2 of 36 ATR eyes (5.6%; 95% CI: 1.5–18.1%) and 6 of 9 oblique eyes (66.7%; 95% CI: 35.4–87.9%). In WTR eyes, J&J PCA-ON almost systematically recommended one DIU step higher than Barrett (mean signed step difference: +0.72). In ATR eyes, agreement between calculators was nearly complete.
Predictors of Clinically Relevant Discrepancies
Univariate logistic regression in the primary analysis set (n=127) identified posterior corneal astigmatism magnitude (OR = 308.8; 95% CI: 29.0–3288.8; p<0.0001), WTR class (OR = 8.76; 95% CI: 3.38–22.71; p<0.0001), anterior J0 component (OR = 4.81; 95% CI: 2.57–9.00; p<0.0001), and anterior corneal astigmatism magnitude (OR = 2.33; 95% CI: 1.32–4.09; p=0.003) as significant predictors of ClinRel (Table 2, Panel B). ATR class was strongly protective (OR = 0.02; 95% CI: 0.00–0.14; p<0.001). Biometric parameters (axial length, anterior chamber depth, lens thickness, white-to-white distance) and the J45 components were not significant.
In the multivariable model (Table 2, Panel B), posterior corneal astigmatism magnitude was the strongest independent predictor of clinically relevant discrepancies (adjusted OR = 316.7; 95% CI: 4.03–24,889.1; p=0.010). This extreme OR reflects nearly complete separation – almost all eyes with higher posterior CYL and WTR orientation showed calculator disagreement. Axial length showed a trend toward significance (adjusted OR = 0.72; 95% CI: 0.52–1.01; p = 0.061), suggesting that longer eyes may have marginally lower discrepancy rates. Anterior corneal astigmatism magnitude and WTR class did not hold significance after adjustment for posterior CYL.
Because the standard maximum-likelihood model showed evidence of quasi complete separation for the posterior CYL predictor, Firth-penalized logistic regression was performed as a pre-specified sensitivity analysis (Table 2, Panel B). Firth penalization reduced the multivariable adjusted OR for posterior CYL from 316.7 to 203.5 (95% CI: 2.92–14,199.3; p=0.014), representing an approximately 36% reduction, while preserving statistical significance. For all other predictors, differences between standard and Firth estimates were negligible, confirming that separation was confined to the posterior CYL variable. The Firth analysis confirmed that posterior corneal astigmatism magnitude is a robust independent predictor of clinically relevant calculator discrepancies, irrespective of the estimation method.
The relationship between posterior corneal astigmatism magnitude and ClinRel followed a sigmoid pattern (Figure 4A). In eyes with posterior CYL <0.15 D, the ClinRel rate was 8.7% (2/23). Between 0.15 and 0.30 D, the rate increased to 15.8% (3/19). A steep transition occurred between 0.30 and 0.45 D, where the ClinRel rate reached 67.6% (23/34). Above 0.45 D, ClinRel rates remained consistently high: 66.7% (0.45–0.60 D; 42/63), 84.0% (0.60–0.75 D; 21/25), and 88.9% (≥ 0.75 D; 16/18). Youden index analysis identified a posterior CYL of 0.36 D as the optimal empirical threshold (sensitivity 91.6%, specificity 56.0%). Mean posterior corneal astigmatism differed markedly between astigmatism classes (Figure 4B): WTR eyes had a mean posterior CYL of 0.56 ± 0.16 D, compared with 0.14 ± 0.10 D in ATR eyes and 0.33 ± 0.13 D in oblique eyes (Table 1). This anatomical difference explains why WTR class lost significance after adjustment for posterior CYL in the multivariable model: WTR functions as a surrogate marker for higher posterior corneal astigmatism.
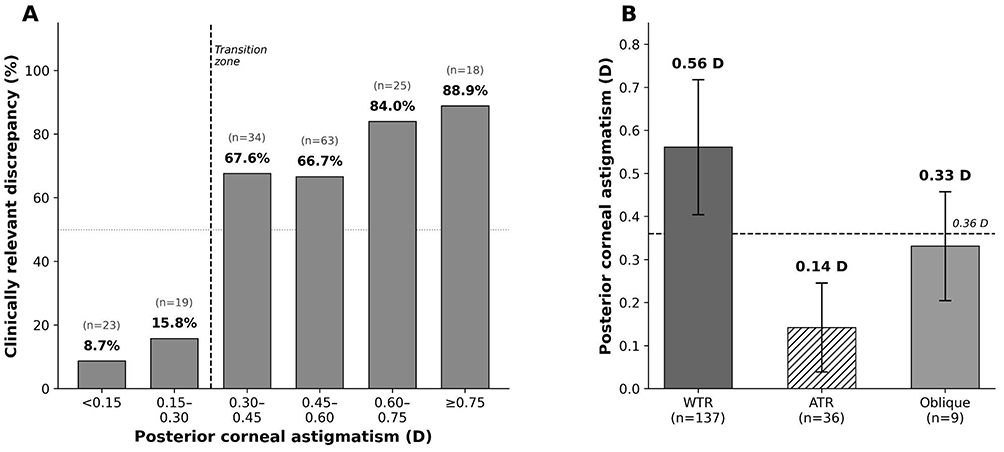 |
Figure 4 Relationship between posterior corneal astigmatism magnitude and calculator discrepancies (J&J PCA-ON versus ESCRS-Barrett, all eyes, n=182). (A) Proportion of eyes with clinically relevant discrepancies (ClinRel) stratified by posterior corneal astigmatism bins. Percentages and eye counts are shown above each bar. The dashed vertical line indicates the transition zone at approximately 0.30 D, where the ClinRel rate increases from below 20% to above 60%. The dotted horizontal line indicates 50%. (B) Mean posterior corneal astigmatism magnitude (± SD) by anterior astigmatism class. The dashed horizontal line indicates the empirical threshold of 0.36 D identified by Youden index analysis. Abbreviations: WTR, with-the-rule; ATR, against-the-rule. |
Discussion
In this study, we systematically quantified calculators variability in toric IOL planning by comparing the J&J toric calculator with four ESCRS-hosted engines under a standardized, paired within-eye design and we managed to identify three principal findings: first, clinically relevant planning discrepancies between J&J PCA-ON and ESCRS-Barrett occurred in approximately 60% of eyes, driven almost exclusively by toric cylinder step differences rather than axis disagreement; second, these discrepancies were strongly concentrated in WTR eyes and almost absent in ATR eyes; and third, posterior corneal astigmatism magnitude was the strongest independent predictor of calculator disagreement.
An important methodological consideration concerns the choice of the ClinRel threshold. Because the DIU step scale is discrete, a step difference of 1 represents the minimum possible “nonzero” discrepancy, and our primary endpoint therefore captures any planning disagreement. We considered this threshold appropriate because each step difference directly determines which physical IOL is ordered for surgery, and even a 1-step difference corresponds to approximately 0.75 D of toric cylinder at the IOL plane – a magnitude that exceeds the commonly cited 0.50 D threshold for functionally relevant residual astigmatism.
Unlike published toric calculator comparisons, which have focused predominantly on postoperative refractive accuracy,12–15 our study humbly addresses a different and complementary question: the frequency and magnitude of planning disagreements between calculators. This is clinically relevant because in routine practice, the choice of calculator can directly determine which toric step is ordered and implanted. By using a paired within-eye approach with fully standardized inputs – identical biometry, keratometry, target refraction, incision meridian, and SIA for every calculator run – logically, we isolated the effect of the calculator itself, removing measurement related confounding that limits the interpretability of many device-comparison studies.
Published comparisons of modern toric formulae have generally reported comparable postoperative accuracy. Kane and Connell compared six toric formulae in 823 eyes and found that the Kane formula showed a significantly lower prediction error than all other formulas (p<0.001), while no significant differences existed among the Barrett and EVO 2.0 formulas.12 Pantanelli et al confirmed similar accuracy between the Barrett and EVO calculators in a multicenter trial of 109 eyes13 More recently, Xian et al evaluated six calculators in 53 eyes and reported mean absolute prediction errors ranging from 056 D (Barrett TK) to 0.63 D (Barrett predicted PCA), again without significant overall differences.14 Liu et al compared five ESCRS toric formulae in 85 eyes and found that EVO, Barrett, and Hoffer QST achieved comparable accuracy within 050 D in approximately 59–62% of eyes, whereas the Kane formula showed slightly lower performance in their cohort.15 Although these studies establish that modern calculators achieve broadly similar refractive outcomes, they do not address the question of how frequently the calculators actually disagree on the preoperative planning recommendation – a question that is directly relevant to workflow standardization in high-volume settings.
Our finding that J&J PCA-ON recommended a higher DIU step than Barrett in 72 of 127 eyes (56.7%), with only 3 eyes showing the reverse pattern, reveals a strongly unidirectional systematic pattern. This is consistent with the known differences in posterior corneal astigmatism handling between these platforms. The Barrett toric calculator uses an internal algorithmic estimation of posterior corneal contribution that has been shown to perform well in population-level validation studies.9,12 The J&J calculator with PCA-ON incorporates a dedicated posterior cornea adjustment that, in our data, systematically resulted in a higher toric cylinder recommendation in WTR eyes. This pattern is biologically plausible: in WTR eyes, the posterior cornea is typically steep vertically, creating ATR astigmatism that partially compensates anterior WTR astigmatism.6,7 Different algorithmic approaches to modeling this compensation – internal prediction versus regression-based adjustment – can produce meaningfully different net corneal astigmatism estimates and, consequently, different toric step recommendations.
The near-complete absence of discrepancies in ATR eyes (ClinRel 5.6%) further supports this interpretation. In ATR eyes, posterior corneal astigmatism adds to rather than compensates the anterior component, and the algorithmic differences between calculators become less consequential.6,7 The sensitivity analysis confirmed this mechanism: switching J&J PCA handling to OFF increased the ClinRel rate from 58.8% to 79.1%, demonstrating that the J&J posterior cornea correction reduces the disagreement with Barrett by approximately 20 percentage points but does not eliminate it. Moreover, the shift was not limited to the frequency of disagreement: the proportion of ≥ 2-step discrepancies did rise from approximately 1% to 40%, indicating that without posterior cornea correction, the J&J pathway diverges from Barrett not only more often but by substantially larger magnitudes. This underscores the clinical importance of activating posterior cornea handling when using the J&J calculator. The residual discrepancy likely reflects additional modeling differences, including corneal-to-IOL plane conversion, SIA treatment, and rounding rules for discrete toric steps.8,11
Notably, discrepancy rates were even higher for the secondary ESCRS engines (Kane 83.8%, EVO 74.4%, Hoffer QST 76.7%) compared with Barrett (58.8%). This indicates that the level of inter-calculator agreement depends strongly on which engines are compared and that Barrett showed the closest alignment with the J&J pathway among the tested ESCRS engines.
The predictor analysis identified posterior corneal astigmatism magnitude as the dominant independent predictor of clinically relevant discrepancies, with extreme OR that were confirmed by Firth-penalized regression to address such quasi complete separation.16 This finding has a direct clinical implication: in eyes with higher posterior corneal astigmatism – particularly those with WTR orientation – clinicians should be aware that the choice of calculator is most likely to produce divergent recommendations. In these eyes, consulting multiple calculators and explicitly evaluating the posterior corneal phenotype may be especially warranted.
The threshold analysis further refines this finding: the relationship between posterior corneal astigmatism and calculator disagreement is not linear but sigmoid, with a steep transition between approximately 0.30 and 0.45 D and a plateau above 0.50 D. Below 0.30 D, calculators agreed in approximately 85% of eyes. This non-linear pattern explains the quasi-complete separation observed in the logistic models and suggests that a pragmatic posterior CYL threshold of approximately 0.36 D could identify eyes at elevated risk of calculator disagreement. This anatomical pattern also clarifies why anterior astigmatism class lost significance in the multivariable model: WTR eyes had a four-fold higher mean posterior corneal astigmatism than ATR eyes (0.56 vs. 0.14 D), consistent with the known concordance between anterior and posterior corneal steepening in WTR anatomy. The posterior corneal astigmatism magnitude – not the anterior classification per se – is the mechanistic driver of inter-calculator variability.
The finding that 7 eyes (3.8%) showed negative decision margins in the J&J output – where the recommended step had a higher predicted residual astigmatism than the nearest alternative – is noteworthy. It suggests that the J&J algorithm may incorporate axis-optimization criteria that prioritize alignment over pure residual magnitude minimization.
The deliberate restriction of this study to the planning level warrants further consideration. Prior calculator-comparison work in toric IOL surgery has overwhelmingly focused on postoperative refractive accuracy, and modern engines now achieve broadly similar mean absolute prediction errors of approximately 0.5 D. From that perspective alone, calculators appear interchangeable. However, in routine clinical workflow the calculator output is not an abstract refractive prediction – it directly determines which physical toric IOL is ordered from the manufacturer, which step is loaded onto the instrument table, and which axis is marked on the eye. A one-step disagreement in 60% of cases is therefore not a purely academic finding, but a logistically and clinically substantive observation that has not, to our knowledge, been systematically quantified before. By holding biometry, keratometry, target refraction, incision meridian, and SIA constant across paired calculator runs, this design isolates the calculator-specific modeling contribution from measurement noise and surgical variability that would dominate any outcome-only study with comparable sample size. The complementary prospective outcome cohort, currently in preparation, will address which planning pathway produces the most accurate postoperative refraction in eyes with discrepant recommendations.
The classical Alpins framework – Target Induced Astigmatism, Surgically Induced Astigmatism, Magnitude of Error, Angle of Error, Correction Index, Difference Vector, and Index of Success – is constructed to compare an intended surgical correction with the achieved postoperative refractive change, and is therefore the gold-standard reporting framework for surgical outcome studies. The present study, however, compares two preoperative planning outputs generated from identical biometric inputs, without postoperative refraction; concepts such as Index of Success, which require a measured postoperative vector, cannot be defined in this setting. The Thibos J0/J45 power-vector decomposition is mathematically equivalent to the Alpins meridional resolution18 and is widely accepted for the description of paired astigmatism vectors. We additionally re-expressed the paired planning outputs in Alpins terminology: the Difference Vector between J&J PCA-ON and ESCRS-Barrett predicted residual astigmatism vectors had a mean magnitude of 0.21 D and a mean meridian of approximately 84°, anatomically consistent with the meridian at which posterior corneal astigmatism predominantly acts in with-the-rule eyes; the Correction Index (J&J PCA-ON / ESCRS-Barrett IOL-plane cylinder) was 1.20, indicating a systematic ~20% over-prescription by the J&J pathway relative to Barrett; the Angle of Error was negligible (mean 1.8°). These observations are illustrated in Figure 3. The convergence of the two frameworks on the same interpretation – that calculator disagreement is a meridional, magnitude-dominated, posterior-cornea-driven phenomenon – reinforces rather than weakens the conclusion.
Several limitations should be considered. First, this study was designed as a planning-level comparison without postoperative outcome validation. A prospective outcome study is in preparation to address this limitation. Second, the study was conducted at a single center using a single toric IOL platform (DIU) with standardized modeling assumptions (fixed target refraction, incision meridian, SIA), which enhances internal validity but may limit generalizability to centers using different platforms, incision strategies, or SIA values. Third, the sample size – although adequate for the primary descriptive endpoint – produced wide confidence intervals for the predictor analysis due to near-complete separation in the posterior CYL variable. Larger multicenter cohorts would be needed to estimate the precise magnitude of this effect. Fourth, calculator algorithms may be updated over time; the results reflect the calculator versions accessed during the study period and may not apply to future updates. Fifth, CASIA2 anterior keratometry was used as the standardized input across all calculators; centers using IOLMaster keratometry or other devices as their primary input source may observe different discrepancy patterns.
In conclusion, calculator-dependent planning variability in toric IOL surgery is substantial and clinically relevant, affecting approximately 60% of eyes in the primary comparison and up to 84% with certain engine combinations. Discrepancies are concentrated in eyes with WTR astigmatism and are driven by differences in posterior corneal astigmatism modeling. These findings have direct clinical value: in eyes with with-the-rule astigmatism and a posterior corneal astigmatism above approximately 0.36 D, the choice of calculator is most likely to alter the toric step that is ordered and implanted. We therefore recommend that, in this anatomically definable subgroup, surgeons consult at least two independent toric calculators and explicitly review the posterior corneal phenotype before finalizing the toric step; in eyes with against-the-rule astigmatism, the choice of calculator is unlikely to influence the recommendation. When calculators disagree, clinicians should consider the patient’s posterior corneal astigmatism phenotype and be aware that the J&J pathway with PCA-ON systematically favors a higher toric step in WTR eyes compared with Barrett. A prospective follow-up study is in preparation to determine which calculator pathway produces superior refractive outcomes in eyes with discrepant planning recommendations.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
Not applicable (no identifiable patient data or images).
Informed Consent
The requirement for informed consent was waived by the Ethics Committee of the City of Vienna (Ethikkommission der Stadt Wien) owing to the retrospective, observational design and the exclusive use of anonymized routine clinical data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article, gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work. Specifically: MK conceived and designed the study, collected and managed the data, performed the statistical analysis, and drafted the manuscript. MT and SS contributed to data collection and critical revision. DB contributed to data acquisition and data management. KM contributed to study design and critical revision. PVV-M supervised the study, provided clinical oversight, and critically revised the manuscript.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests in this work.
References
1. Lundström M, Dickman M, Henry Y, et al. Risk factors for refractive error after cataract surgery: analysis of 282 811 cataract extractions reported to the European registry of quality outcomes for cataract and refractive surgery. J Cataract Refract Surg. 2018;44(4):447–13. doi:10.1016/j.jcrs.2018.01.031
2. Stopyra W, Voytsekhivskyy O, Grzybowski A. Accuracy of 7 artificial intelligence-based intraocular lens power calculation formulas in medium-long eyes: 2-center study. Can J Ophthalmol. 2025;60(4):200–207. doi:10.1016/j.jcjo.2025.01.020
3. Stopyra W, Voytsekhivskyy O, Grzybowski A. Comparison of the accuracy of twenty intraocular lens power calculation formulas in long eyes. Asia Pac J Ophthalmol. 2025;14(3):100198. doi:10.1016/j.apjo.2025.100198
4. Kessel L, Andresen J, Tendal B, Erngaard D, Flesner P, Hjortdal J. Toric intraocular lenses in the correction of astigmatism during cataract surgery: a systematic review and meta-analysis. Ophthalmology. 2016;123(2):275–286. doi:10.1016/j.ophtha.2015.10.002
5. Visser N, Bauer NJC, Nuijts RMMA. Toric intraocular lenses: historical overview, patient selection, IOL calculation, surgical techniques, clinical outcomes, and complications. J Cataract Refract Surg. 2013;39(4):624–637. doi:10.1016/j.jcrs.2013.02.020
6. Koch DD, Ali SF, Weikert MP, Shirayama M, Jenkins R, Wang L. Contribution of posterior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg. 2012;38(12):2080–2087. doi:10.1016/j.jcrs.2012.08.036
7. Koch DD, Jenkins RB, Weikert MP, Yeu E, Wang L. Correcting astigmatism with toric intraocular lenses: effect of posterior corneal astigmatism. J Cataract Refract Surg. 2013;39(12):1803–1809. doi:10.1016/j.jcrs.2013.06.027
8. Savini G, Abulafia A. Toric calculations. In: Aramberri J, Hoffer KJ, Olsen T, Savini G, Shammas HJ, editors. Intraocular Lens Calculations. Essentials in Ophthalmology. Cham: Springer; 2024:871–876. doi:10.1007/978-3-031-50666-6_62
9. Abulafia A, Hill WE, Franchina M, Barrett GD. Comparison of methods to predict residual astigmatism after intraocular lens implantation. J Refract Surg. 2015;31(10):699–707. doi:10.3928/1081597X-20150928-03
10. Reitblat O, Levy A, Kleinmann G, Abulafia A, Assia EI. Effect of posterior corneal astigmatism on power calculation and alignment of toric intraocular lenses: comparison of methodologies. J Cataract Refract Surg. 2016;42(2):217–225. doi:10.1016/j.jcrs.2015.11.036
11. Canovas C, Alarcon A, Rosén R, et al. New algorithm for toric intraocular lens power calculation considering the posterior corneal astigmatism. J Cataract Refract Surg. 2018;44(2):168–174. doi:10.1016/j.jcrs.2017.11.008
12. Kane JX, Connell B. A comparison of the accuracy of 6 modern toric intraocular lens formulas. Ophthalmology. 2020;127(11):1472–1486. doi:10.1016/j.ophtha.2020.04.039
13. Pantanelli SM, Sun A, Kansara N, Smits G. Comparison of Barrett and Emmetropia verifying optical toric calculators. Clin Ophthalmol. 2022;16:177–182. doi:10.2147/OPTH.S346925
14. Xian H, Li B, Xia Z, et al. Comparative evaluation of several toric intraocular lens calculators for predicting postoperative refractive astigmatism in cataract surgery: a real-world study. BMC Ophthalmol. 2025;25:35. doi:10.1186/s12886-025-03856-9
15. Liu C, Wang M, Long D, Zhang Y, Chen Y, Wu Q. Comparison of the accuracy of toric intraocular lens formulas used by the online calculator of the European Society of Cataract and Refractive Surgeons. J Refract Surg. 2025;41(2):e120–e130. doi:10.3928/1081597X-20241219-01
16. Heinze G, Schemper M. A solution to the problem of separation in logistic regression. Stat Med. 2002;21(16):2409–2419. doi:10.1002/sim.1047
17. R Core Team. R: a Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria; 2026. Available from: https://www.R-project.org/.
18. Freitas GO, Ambrósio Júnior R, Alves MR. Vector analysis of astigmatism according to the methods of Alpins and Thibos: a systematic review. eOftalmo. 2016;2(3):1–6. doi:10.17545/e-oftalmo.cbo/2016.58
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.