Back to Journals » Patient Preference and Adherence » Volume 15
Investigating the Influence of the Shared Decision-Making Perception on the Patient Adherence of the Home- and Exercise-Based Cardiac Rehabilitation After Percutaneous Coronary Intervention
Authors Cao Q, Xu L, Wen S, Li F ![]()
Received 14 November 2020
Accepted for publication 30 December 2020
Published 22 February 2021 Volume 2021:15 Pages 411—422
DOI https://doi.org/10.2147/PPA.S292178
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Qinqin Cao,1,2,* Linqi Xu,1,* Shujuan Wen,2 Feng Li1
1School of Nursing, Jilin University, Changchun, Jilin Province, People’s Republic of China; 2Affiliated Hospital of Jining Medical University, Jining, Shandong Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Feng Li
School of Nursing, Jilin University, No. 965, Xin Jiang Avenue, Changchun, Jilin Province, 130000, People’s Republic of China
Email [email protected]
Background: In 2016, the Global Burden of Disease study pointed out that cardiovascular disease (CVDs) were the most common causes of death and accounted for the largest disease burden worldwide. Percutaneous coronary intervention (PCI) is one of the main treatments for coronary artery disease (CAD). Moreover, home- and exercise-based cardiac rehabilitation (CR) is of great importance for improving the prognosis of patients undergoing PCI. However, poor adherence to CR remains a challenging problem in these patients.
Aim: This study aimed to investigate the current status of adherence to home- and exercise-based CR in patients undergoing PCI and to explore the factors affecting patient adherence to home- and exercise-based CR.
Methods: This study was a prospective longitudinal survey that included 300 patients who met the established criteria. The selected patients completed a pre-hospital discharge questionnaire, which targeted factors that may affect patient adherence to home- and exercise-based CR. All patients were followed up 1 month after the discharge from hospitals.
Results: This study analyzed 283 questionnaires and found that only 64.66% of patients had good adherence to home- and exercise-based CR. Eight independent variables, namely, shared decision-making (SDM), age, dimension of risk factors, predisposing factors, treatment methods, secondary prevention in the Perceived Knowledge Scale for CAD, and dimension of life and emotional management in the Scale of Self-Management with Coronary Artery Disease, were identified as the main factors affecting patient adherence to home- and exercise-based CR, which explains 88.9% variation (Nagel kerke R2 = 0.889).
Conclusion: Patients who underwent PCI had poor adherence to home- and exercise-based CR. Age, SDM, knowledge about CAD, and self-management behavior were identified as independent factors affecting patient adherence to CR after PCI.
Keywords: shared decision-making, percutaneous coronary intervention, cardiac rehabilitation
Introduction
Cardiovascular disease (CVD) is the most common cause of death globally.1,2 In China, 7.7 million people died from CVDs in 2015; of these deaths, 7.4 million deaths were attributed to coronary artery disease (CAD).3,4 Percutaneous coronary intervention (PCI) has the benefits of less trauma and rapid recovery and has been widely used in clinical practice as the main treatment for CAD.5,6 However, PCI could only temporarily solve mechanical stenosis of the coronary arteries and is unable to prevent disease progression. In the presence of risk factors for the disease, patients are prone to adverse cardiac events such as stent stenosis and angina pectoris.7
As an effective intervention, cardiac rehabilitation (CR) has been shown to significantly reduce the incidence of adverse cardiac events in patients after undergoing PCI, which is important for improving patient prognosis after PCI.8,9 However, in most European countries, less than half of eligible patients participate in center-based CR.10 Compared with center-based CR, home-based CR can promote patient participation and has the same benefits as center-based CR in improving patients’ functional capacity and quality of life and reducing the risk of death.11 However, poor adherence to home-based CR remains problematic, which may be because patients’ preferences are not included in the home-based CR program during the long-term and self-helping process.
A new type of decision-making model12—shared decision-making (SDM)—requires information sharing between the doctor and the patient and incorporates patient’s preferences into the decision-making process. Therefore, the present study incorporated SDM into the survey. Meanwhile, patients’ expectation from decision-making was also included. As exercise is a basic part of the CR,13 this study only investigated patient adherence to home- and exercise-based CR for accuracy. Studies have found that patients’ knowledge about CAD and self-management behavior are independent factors affecting the adherence of patients with CAD.14,15 In order to eliminate the influence of covariates and explore the influence of SDM on adherence to home- and exercise-based CR, patients’ knowledge about CAD and their self-management behavior were included in the study.
The purpose of this study was to explore the current status of adherence to home- and exercise-based CR in patients undergoing PCI. Moreover, in order to provide theoretical basis and data support for future studies on this topic, we aimed to analyze the current status of SDM, type of expectation from decision-making, knowledge of CAD, and self-management behavior and their impact on adherence to home- and exercise-based CR.
Methods
Design and Sample
This study is a prospective longitudinal survey. Patients who met the established criteria were recruited from a cardiology unit at a tertiary medical center in China between October 2017 and April 2018, and they were followed up 1 month after hospital discharge. The sample size was calculated based on 52 entries in the Perceived Knowledge Scale for CAD (PKS-CAD), which comprised the most items in these questionnaires,16 and the sample loss of 10%-20%17 was considered. Moreover, in order to ensure sufficient sample size, a total of 300 questionnaires were distributed. Therefore, 300 patients with CAD who underwent PCI were recruited to participate using convenience sampling. Patients were included if they (1) were aged ≥18 years; (2) had a history of CAD ≥ 3 months; (3) accomplished Phase I of CR after PCI and was allowed to enter the early stage of Phase II in home- and exercise-based CR by a CR specialist; and (4) had no language communication barriers and were willing to participate in this study. Patients were excluded if they (1) had complications (severe aortic stenosis, severe pulmonary hypertension, valvular heart disease, and hypertrophic obstructive cardiomyopathy) or other diseases that impede exercise or (2) were suffering from disturbance of consciousness or mental illness.
Instruments and Measurements
The 9-Item Shared Decision-Making Questionnaire (SDM-Q-9)
The SDM-Q-9 was compiled by the German scholar Kriston et al,18 and its Chinese version was used to measure patients’ perception of SDM in the home- and exercise-based CR program.19 The questionnaire consists of 9 items, ranging from “completely disagree” (0) to “completely agree” (5). The original score ranges from 0 to 45. The higher the score, the better the SDM level.
Control Preference Scale (CPS)
The CPS was developed by Degner et al,20 and the Chinese version was used to measure the type of expectation from decision-making,21 which is evaluated using 5 questions. The obtained results can be divided into active, passive, and cooperative.
Perceived Knowledge Scale for CAD (PKS-CAD)
The PKS-CAD was designed by Chinese scholars, which was used to measure patients’ knowledge about CAD.16 The questionnaire has a total of 52 items, with 8 dimensions. The higher the score, the higher the patients’ knowledge of CHD.
Self-Management Scale (SSMC)
The Scale of Self-Management with Coronary Artery Disease (SSMC) was developed by Chinese scholars to measure the self-management of patients with CAD.22 The questionnaire has 27 entries, with 7 dimensions. Moreover, it is based on the 5-point Likert scale, ranging from 1 to 5. The higher the score, the better the patients’ self-management behavior.
Questionnaire to Assess Adherence to Home- and Exercise-Based CR
The researchers designed a telephone follow-up questionnaire to investigate patient adherence to home- and exercise-based CR based on previous studies, patients’ home- and exercise-based CR prescription, Chinese expert consensus on exercise-based CR for patients after PCI,23,24 and study on patient adherence to home- and exercise-based rehabilitation by scholars from Peking Union Medical College.25 The questionnaire contains 6 items and is scored using the 4-point Likert scale, ranging from 1 to 4. The higher the cumulative score, the better the adherence.
Procedure
The CR can be divided into three phases: phase I is the in-hospital CR period, phase II is the early out-of-hospital CR period, and Phase III is the long-term out-of-hospital CR period.23,24 Among the phases, phase II is the early outpatient CR period and is divided into the early stage, which occurs 1 month after discharge, the middle stage, which occurs 3 months after discharge, and the later stage, which occurs 6 months after discharge.
In the hospital: After the patients completed phase I CR in the hospital, data were collected via the survey after obtaining written informed consent from all patients. The questionnaire topics in this phase included patient demographics, type of expectation from decision-making, SDM, patient’s knowledge of CAD, and self-management behavior.
After discharge: Considering the time effect of SDM, it was decided that data regarding patient adherence to home- and exercise-based CR after PCI would be obtained via telephone follow-up at the early stage of Phase II.
Ethical Considerations
The study was approved by the medical ethics committee of the School of Nursing, Jilin University, and this study was conducted in accordance with the Declaration of Helsinki.
Data Analysis
Data were analyzed using the Statistical Package for the Social Sciences software (SPSS), version 23.0 (IBM SPSS Statistics). Descriptive statistics for variables included frequencies, percentages, means, and standard deviations (SDs). The impact of patient demographics on patient adherence to home- and exercise-based CR was analyzed using χ2 test. The impact of SDM perception, knowledge of CAD, and self-management behavior on patient adherence was analyzed using logistic regression analysis. Furthermore, multifactor unconditional logistic regression analysis was conducted to analyze the major factors influencing patient adherence to home- and exercise-based CR. A p-value of <0.05 was considered to indicate statistical significance.
Technical Route
Figure 1 shows the technical roadmap for this study.
 |
Figure 1 The technical roadmap of this study. Abbreviations: PCI, percutaneous coronary intervention; CHD, coronary heart disease; PKS-CHD, Perceived Knowledge Scale for Coronary Heart Disease; SDM-Q-9, The 9-item Shared Decision Making Questionnaire; SSMC, The Scale of Self-Management with Coronary Artery Disease; CR, cardiac rehabilitation. |
Results
Patient Demographics
In this study, 300 questionnaires were distributed, out of which 5 were removed because of obvious contradictions in contents and 17 were removed because of missing responses. Finally, 283 questionnaires were selected and administered to the patients. The effective response rate was 94.3%. The age range of patients was 23–84 years, with an average age of 60 ± 11.844. Most patients were men (164, 58%), were married (270, 95.4%), had primary school education or below (101, 35.7%), and were living in cities (129 people, 45.6%). Among the participants, 49.5% had hypertension, 25.8% had diabetes, and 30.4% had hyperlipidemia. Moreover, the type of expectation from participation in the decision-making was mainly cooperative (157 patients, 55.5%). Furthermore, as for the number of stent grafts, 60.4% patients implanted one stent, 25.1% implanted two stents, 14.5% implanted more than three stents. Table 1 presents a detailed information on the study participants.
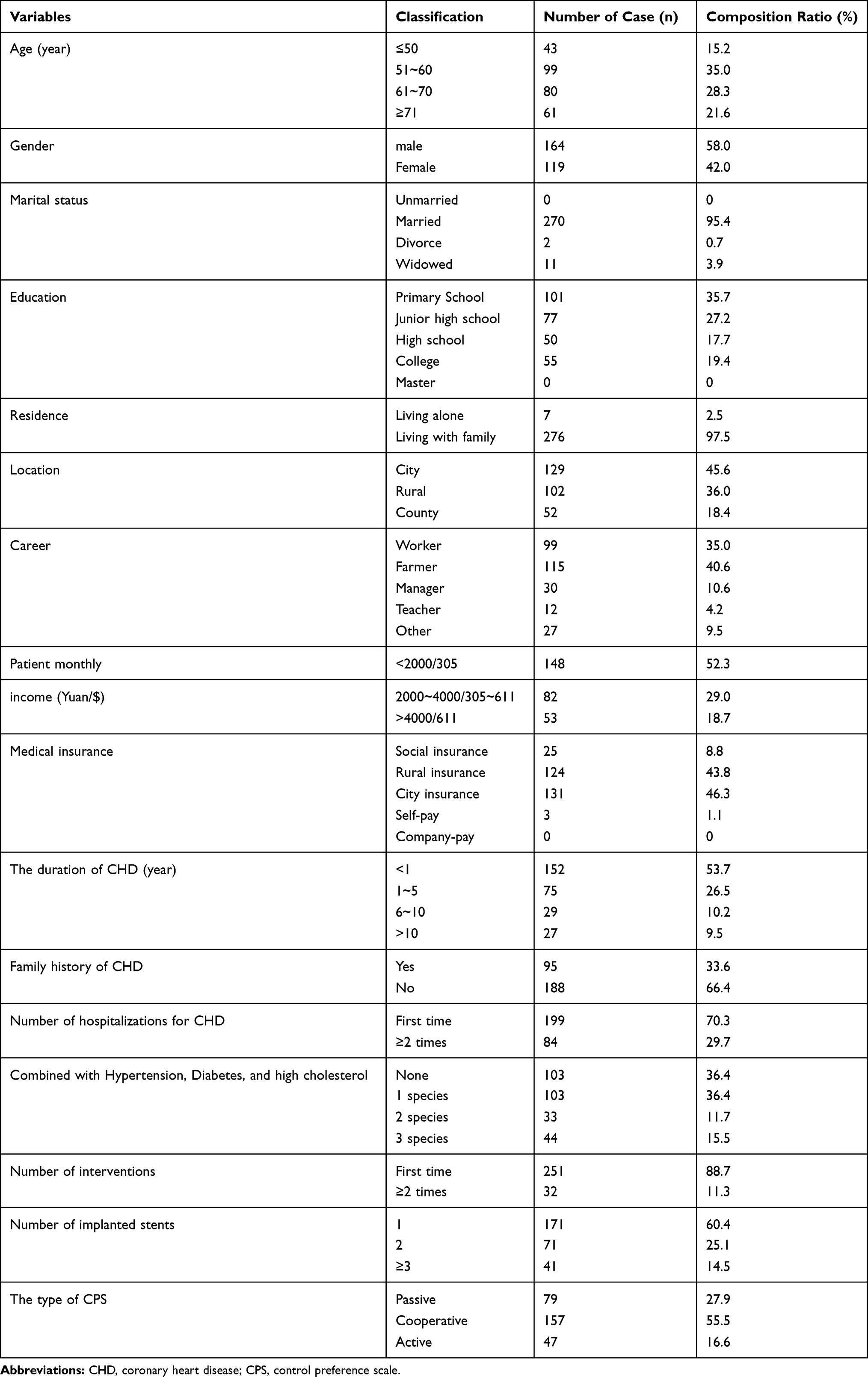 |
Table 1 Sample Characteristics (n = 283) |
Status of Adherence to Home- and Exercise-Based CR
The questionnaire score ranged from 6 to 24 points, with an average score of 18.54 ± 4.96 and an average score of each item of 3.09 ± 0.83. Among the questionnaire items, the item “remember the precautions for rehabilitation, stop or seek medical treatment in the case of discomfort?” had the highest score among the participants, whereas the item “actively evaluates and achieves the intensity of rehabilitation for example slight sweating and monitoring the pulse rate” had the lowest score. In order to objectively reflect patient adherence to home- and exercise-based CR, this study converted the adherence score into the adherence rate, based on which, adherence was divided into high (≥75%) and low (<75%) levels.26 It was found that 64.66% of patients (n = 183) had a high adherence level (Table S1).
Status of SDM Perception to Home- and Exercise-Based CR
The obtained score for SDM perception ranged from 12 to 45, with an average score of the questionnaire of 28.87 ± 7.77 and an average score of each item of 3.21 ± 0.86. The item “The doctor clearly informed the patient that the decision must be made” scored the highest, with an average score of 4.58 ± 1.05, whereas the item “Doctor asked the patient how they want to participate in the decision” scored the lowest, with an average score of 2.25 ± 1.84 (Table S2).
Status of Knowledge About CAD
The questionnaire scores on knowledge of CAD ranged from 20 to 52, with an average score of the questionnaire of 38.19 ± 6.57 and an average score of each item of 0.73 ± 0.13. Among the items, the dimension “coronary heart disease concept” scored the highest, with an average score of 0.94 ± 0.18, and the dimension “drug knowledge” scored the lowest, with an average score of 0.46 ± 0.29 points (Table S3).
Status of Self-Management Behavior
The questionnaire scores on self-management behavior ranged from 42 to 122, with an average score of the questionnaire of 80.51 ± 12.90 and an average score of each item of 2.98 ± 0.48. Among the items, the dimension “life management” scored the highest, with an average score of 3.41 ± 0.65, and the dimension “medical management” scored the lowest, with an average score of 2.47 ± 0.59 (Table S4).
Univariate Analysis of Adherence to Home- and Exercise-Based CR
Influence of Demographic Data on Adherence to Home- and Exercise-Based CR
Age, number of coronary interventions, and number of stent grafts were found to significantly affect patient adherence to home- and exercise-based CR (P < 0.05; Table 2).
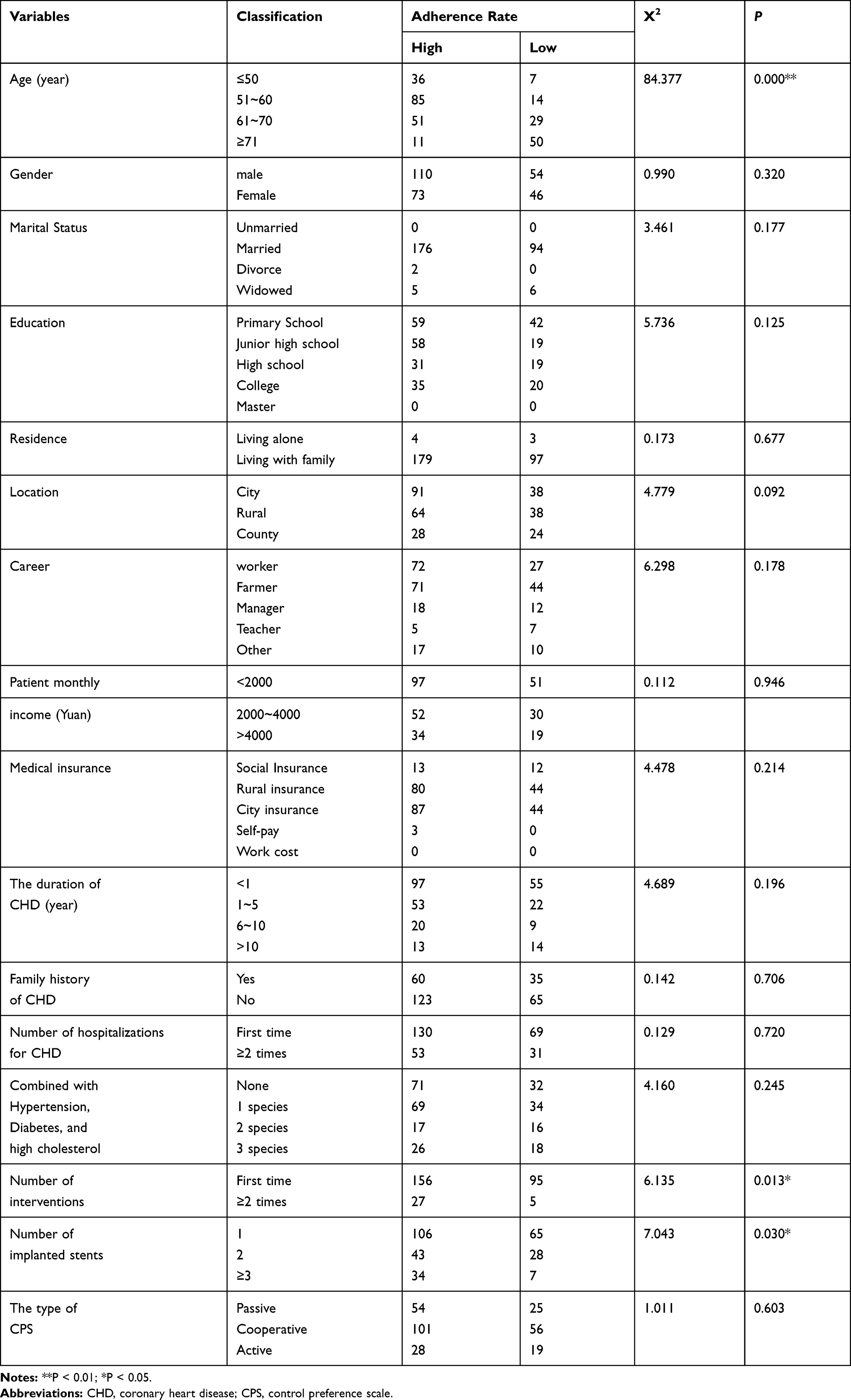 |
Table 2 The Influence of Demographic Data on the Adherence of Home- and Exercise-Based Cardiac Rehabilitation (n = 283) |
Influence of SDM on Adherence to Home- and Exercise-Based CR
SDM was found to be a factor influencing adherence to home- and exercise-based CR (P < 0.01; Table 3).
 |
Table 3 The Influence of the Perception of Shared Decision-Making on the Adherence of Home- and Exercise-Based Cardiac Rehabilitation (n = 283) |
Influence of Knowledge About CAD on Adherence to Home- and Exercise-Based CR
In addition to the dimension of “clinical examination,” the remaining dimensions also had an influence on patient adherence to home- and exercise-based CR (Table 4).
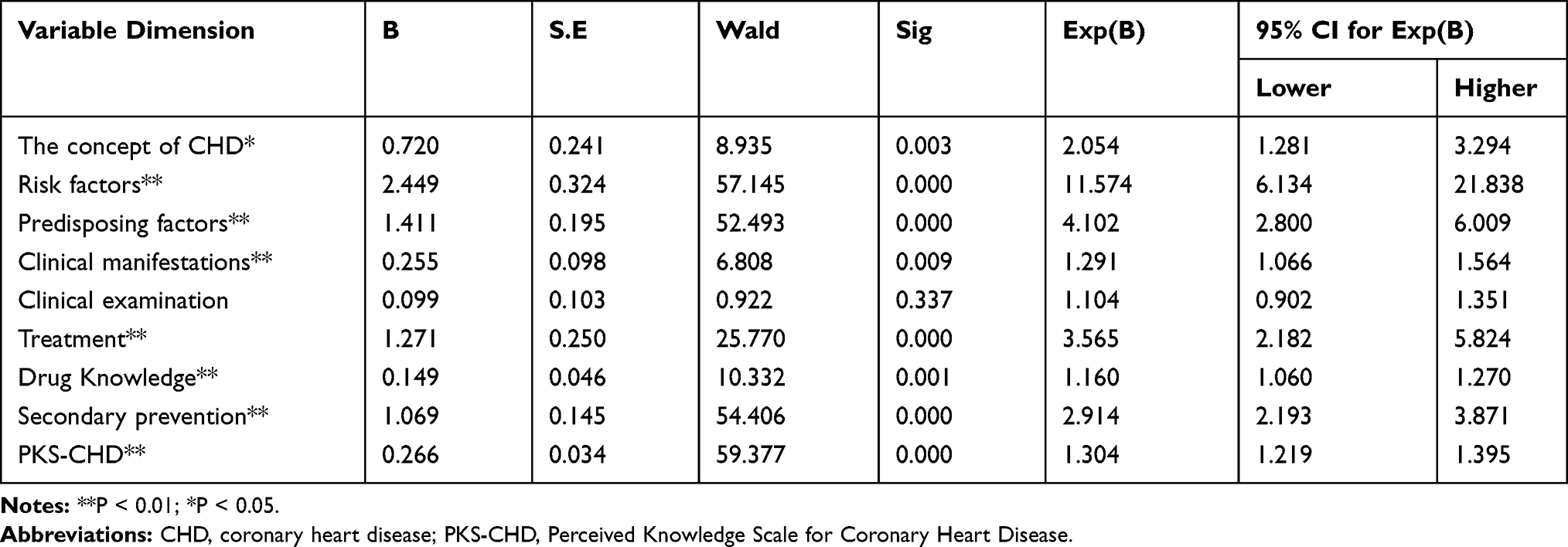 |
Table 4 The Influence of Knowledge of CHD on the Adherence of Home- and Exercise-Based Cardiac Rehabilitation (n = 283) |
Influence of Self-Management Behavior on Adherence to Home- and Exercise-Based CR
Self-management behavior was found to be a factor influencing adherence to home- and exercise-based CR (P < 0.01; Table 5).
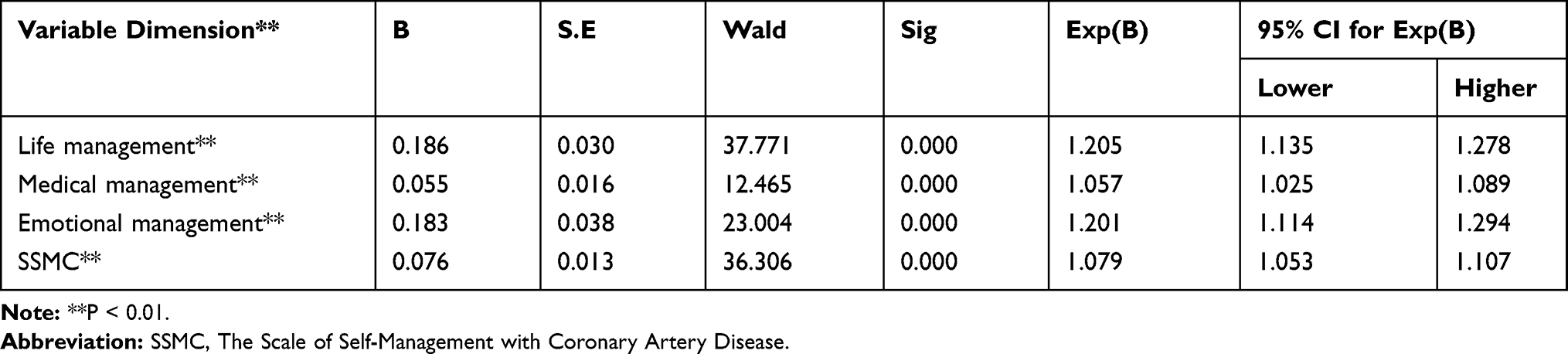 |
Table 5 The Influence of Self-Management Behavior with CHD on the Adherence of Home- and Exercise-Based Cardiac Rehabilitation (n = 283) |
Multivariate Analysis of Adherence to Home- and Exercise-Based CR
The results showed that eight independent variables, namely, SDM, age, dimension of risk factors, predisposing factors, treatment methods, secondary prevention in the PKS-CAD, and dimension of life and emotional management in the scale of SSMC, were the main factors affecting adherence to home- and exercise-based CR in patients after PCI, which explains 88.9% variation (Nagel kerkeR2= 0.889). Table 6 shows the calculated results.
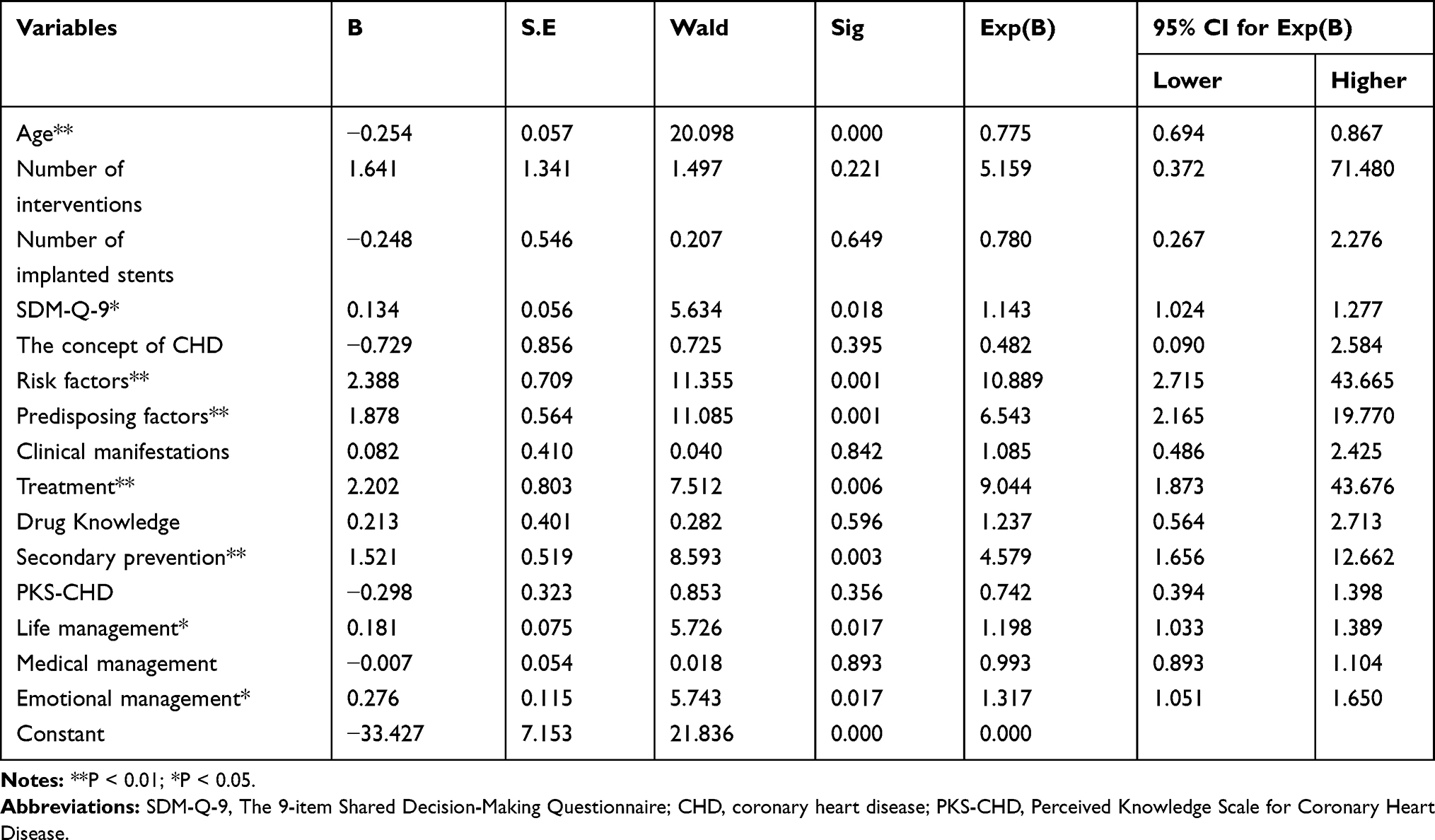 |
Table 6 Multivariate Analysis of Adherence with Home- and Exercise-Based Cardiac Rehabilitation (n = 283) |
Discussion
In the times of COVID-19, it is difficult to deliver group-based, center-based traditional CR. An alternative strategy for increasing the availability and accessibility of CR services is to implement home-based CR, which has been proven to be safe, feasible, and effective as center-based programs.27 Adherence to home- and exercise-based CR directly affects the efficacy of CR programs. However, patients often have poor adherence during home-based CR. The present study explored the current status of adherence to home- and exercise-based CR and its influencing factors. Our study may provide reference for improving the adherence level of home- and exercise-based CR to overcome the challenges of COVID-19.
Adherence to Home- and Exercise-Based CR in Participants
In the present study, 64.66% of patients showed good adherence to home- and exercise-based CR, which was slightly lower than obtained in previous studies (73%-95%).28,29 This difference may be due to the late development of CR in China, and thereby slower understanding of the concept of CR in Chinese residents. The main forms of exercise included hiking, combination of fast walking and jogging on the treadmill, tai chi, table tennis, and bicycle riding. Among these exercises, hiking was found to be the most common form, consistent with the findings of another study.30 The participation rate of home- and exercise-based CR was 97.9% in this study, consistent with the findings of previous studies (94%-100%).31,32 Further analysis of the adherence to home- and exercise-based CR and scores of the entries revealed that the item “Remember the precautions for rehabilitation, stop or seek medical treatment in case of discomfort?” had the highest score. Moreover, 71% of patients said that they could fully comply to the CR, and as an important safety precaution, this item is related to the patient’s own safety and is more likely to attract the attention of these patients. The results are in excellent agreement with those obtained in a previous study.33 It was found that patients do not pay enough attention to the intensity of home- and exercise-based CR. Insufficient exercise intensity was found to be a common problem regarding home- and exercise-based CR in the participants; the results were in good consistency with those obtained in another study.34
Perception of SDM in Participants
The average score of SDM in this study was 28.87 ± 7.77. In order to compare with the previous studies, the score of the questionnaire was changed to a percentage system, and the average score was found to be 64.15 ± 17.27. Woltz et al35 used this questionnaire to measure the SDM perception of patients involved in the surgical plan and found that the average score of SDM was 74.00 ± 23.00. Tinsel et al36 used this questionnaire to measure the perception of SDM in patients with hypertension, according to whether the clinician participated in the relevant training of SDM. Furthermore, the researchers divided the subjects into experimental and control group and found that the experimental group’s score was 73.00 ± 17.66, whereas the control group’s score was 70.67 ± 20.24. These findings indicate that the perception of SDM with home- and exercise-based CR in patients undergoing PCI was lower in this study than in previous studies, which may be because the implementation of SDM requires the support of decision aids, while the development of decision aids is still in its infancy in China. Moreover, training of the medical staff has a positive effect on the implementation of SDM. However, to date, no training regarding SDM has been undertaken for the medical staff in China.
PKS-CAD and SSMC in Participants
The average score of PKS-CAD in this study was 38.19 ± 6.57. The longitudinal study design was superior to the cross-sectional study, and it is similar to the intervention study.37 This may be because the patients in this study received phase I CR before the questionnaire survey was started. In order to enable patients to better complete the home- and exercise-based CR, the specialists of CR conducted a health-themed lecture in phase I CR. Therefore, patients have a higher level of knowledge about CAD.
The average score of SSMC was 80.51 ± 12.90 and the total score rate was 59.6%, suggesting that patients’ self-management behavior was poor. The obtained results are similar to those of other study.38 Further analysis found that this may be related to the lower level of patient’s education and the lack of attention to the CR.
Multivariate Analysis of the Adherence to Home- and Exercise-Based CR
Among the demographic data of patients, only age was found to be an independent factor affecting the adherence to home- and exercise-based CR (P < 0.01) in the Multivariate Analysis. The obtained results were consistent with those of Krishnamurthi’s study39 in which he pointed out that age and coronary artery bypass grafting (CABG) were independent factors influencing the participation rate and adherence to home- and exercise-based CR. However, this result is different from those of another study.34 Tang indicated that the adherence to home- and exercise-based CR was significantly positively correlated with the cognition of CR and exercise habits (P < 0.05) but was not significantly correlated with patients’ age, sex, and education level.33 Analysis of the reasons for this discrepancy between findings revealed that it may be related to the study population, in that the present study and Krishnamurthi’s study included patients aged ≥18 years, whereas Tang’s study included middle and elderly-aged patients, which eliminated the influence of age.
To the best of our knowledge, this study is the first one to explore the impact of SDM on patient adherence to home- and exercise-based CR, which thereby can be considered as the novelty of this study. Lofland et al40 investigated the correlation between drug adherence and SDM in patients with autoimmune diseases and observed that SDM affected patients’ drug adherence. Moreover, they concluded that a higher degree of SDM results in better patient adherence, which is in reasonable consistency with the findings of the present study. Involving patients in the decision-making process and incorporating patients’ preferences into the process both improve patient’s performance of the decisions that are made, thereby improving patient adherence.
The present study shows that based on the questionnaire administered, dimensions of knowledge about CAD and self-management behavior were the main influencing factors affecting the adherence to home- and exercise-based CR. The obtained results are consistent with the findings of a previous study.41 Knowledge about CAD and self-management behavior, which are key factors in the self-care of patients with CAD, should be paid attention to by the medical staff and health-care providers in order to improve patient adherence.
Implications for Practice
The role of physical and rehabilitation medicine (PRM) specialists is different in home- and exercise-based CR compared with center-based CR42. In home-based CR, PRM specialists should not only pay attention to patient safety during the CR program but also keep an account of patient adherence to the program. This requires them to determine the clinical and psychological status of each patient, such as SDM, knowledge of CAD, and self-management behavior, and undertake some interventions to improve the compliance among patients with low adherence.
Limitations
The present study has several limitations. First, our study did not examine the status of adherence to home- and exercise-based CR after 12 months, and the long-term effects of the influencing factors on adherence were not explored. Cohort studies should be conducted in the future to examine real-world patient experiences over the long term regarding home-based CR. Second, we applied convenience sampling, which may result in selection bias. Third, our study did not examine the impact of family support on patient adherence to CR, which has been stressed out in previous studies. We plan to include this influencing factor in our future study.
Conclusion
The present study found that patients who underwent PCI had poor adherence to home- and exercise-based CR, SDM perception in the CR program was low, knowledge of CAD was better, and self-management behavior was poor.
It should be indicated that SDM is an independent influencing factor affecting the adherence to home- and exercise-based CR in patients after PCI. Furthermore, the age of patients, dimension of risk factors, predisposing factors, treatment methods, secondary prevention in PKS-CAD, and dimension of life and emotional management in the SSMC were also independent influencing factors affecting the adherence of adherence to CR in patients after PCI.
Acknowledgment
Qinqin Cao and Linqi Xu are co-first authors for this study.
Funding
This study was supported by a Norman Bethune Plan Research Program Grant from Jilin University (Study code: 2018A04) awarded to Dr. Feng Li.
Disclosure
All authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Naghavi M, Abajobir AA, Abbafati C, et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet. 2017;390(10100):1151–1210.
2. Miller T. 4. Global, Regional, and National incidence and prevalence, and years lived with disability for 328 diseases and injuries in 195 countries, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2010;390:1211–1259.
3. World Health Organization. Cardiovascular diseases (CVDs): fact Sheet. Available from: www.who.int/mediacentre/factsheets/fs317/en/.
4. Hu S, Gao R, Liu L, et al. Summary of “Chinese Cardiovascular Disease Report 2018”. Chin J Circ. 2019;34(03):209–220.
5. Yeh RW, Mauri L, Wolf RE, et al. Population trends in rates of coronary revascularization. JAMA Intern Med. 2015;175(3):454–456.
6. Chinese Cardiovascular Health Alliance. CCIF 2018|2017 Chinese Mainland coronary heart disease interventional therapy data release! [EB/OL]. Available from: https://baijiahao.baidu.com/s?id=1598328473875482034&wfr=spider&for=pc.
7. Yang N, Li N. Risk factors and preventive nursing of patients with acute myocardial infarction undergoing percutaneous coronary intervention. J Clin Med Pract. 2018;22(22):117–120.
8. Zheng Z, Shan Y, Qiang W. Exercise rehabilitation after coronary heart disease intervention. Cardiovasc Prog. 2018;39(04):602–605.
9. Yang G, Li S. Current status and progress of exercise rehabilitation after PCI in patients with myocardial infarction. J Clin Cardiol. 2018;34(07):640–642.
10. Bjarnason-Wehrens B, McGee H, Zwisler AD, et al. Cardiac rehabilitation in Europe: results from the European cardiac rehabilitation inventory survey. Eur J Cardiovasc Prev Rehabil. 2010;17(4):410–418.
11. Buckingham SA, Taylor RS, Jolly K, et al. Home-based versus centre-based cardiac rehabilitation: abridged Cochrane systematic review and meta-analysis. Open Heart. 2016;3(2):e000463.
12. Ferguson C, Hendriks J Partnering with patients in shared decision-making for stroke prevention in atrial fibrillation, 2017.
13. Anderson L, Oldridge N, Thompson DR, et al. Exercise-based cardiac rehabilitation for coronary heart disease: cochrane systematic review and meta-analysis. J Am Coll Cardiol. 2016;67(1):1–12.
14. Zhao Y, Chen Y, Zou J, et al. Study on medication adherence and its influencing factors in patients with coronary heart disease. Chin Pract Med. 2018;13(23):190–191.
15. Ma W, Yang F, Lu X, et al. Analysis of the status quo and influencing factors of self-management behavior in patients undergoing percutaneous coronary intervention. J Nurs. 2018;25(20):1–4.
16. Xiao M. Evaluation of Individualized Health Education in Hospitalized Patients with Coronary Heart Disease [D]. Central South University; 2007.
17. Kendall M. Multivariate Analysis[M]. London: Charles Griffin; 1975.
18. Kriston L, Scholl I, Hölzel L, et al. The 9-item Shared Decision Making Questionnaire (SDM-Q-9). Development and psychometric properties in a primary care sample. Patient Educ Couns. 2010;80(1):94–99.
19. Global Alliance Network. Shared Decision Making Questionnaire (Patient Edition) [EB/OL]. Available from: https://www.alliancehealthplan.org/providers/shared-decision-making-tools/. Accessed January 28, 2021
20. Degner LF, Sloan JA, Venkatesh P. The control preferences scale. Can J Nurs Res Arch. 1997;(3):29.
21. Xiaolin X. Compilation of Patient Satisfaction Scores for Medical Decision-Making Participation and Evaluation of Reliability and Validity [D]. Central South University; 2010.
22. Hongyan R. Development of Self-Management Scale for Coronary Heart Disease and Health Education Research [D]. Chongqing Medical University; 2009.
23. Yiqi M. Chinese expert consensus on sports therapy for patients with coronary heart disease. Interpretation. 2015;30(s2):71–74.
24. Hu S, Wang L, Guo L. Interpretation of the consensus of sports rehabilitation after percutaneous coronary intervention. J Shanghai Univ. 2018;24(1):9–15.
25. Cao Q. Study on the Effect of Intervention Based on WeChat to Improve the Adherence of Home Function in Patients Undergoing Total Knee Arthroplasty [D]. Peking Union Medical College; 2017.
26. Brieger D, Chow C, Gullick J, et al. Improving patient adherence to secondary prevention medications 6 months after an acute coronary syndrome: observational cohort study. Intern Med J. 2018;48(5):541–549.
27. Ribeiro F, Santos M. Rehabilitación cardiaca basada en el ejercicio en tiempos de COVID-19: un pequeño paso para los sistemas de salud, un gran salto para los pacientes [Exercise-based cardiac rehabilitation in COVID-19 times: one small step for health care systems, one giant leap for patients]. Rev Esp Cardiol. 2020;73(11):969–970.
28. Dalal HM, Evans PH, Campbell JL, et al. Home-based versus hospital-based rehabilitation after myocardial infarction: a randomized trial with preference arms—Cornwall Heart Attack Rehabilitation Management Study (CHARMS). Int J Cardiol. 2007;119(2):202–211.
29. Jolly K, G Y H L, R S T, et al. The Birmingham Rehabilitation Uptake Maximisation study (BRUM): a randomised controlled trial comparing home-based with centre-based cardiac rehabilitation. Heart. 2009;95(1):36–42.
30. Yichao Y. Investigation on the Status of Exercise Rehabilitation in Patients with Coronary heart Disease After Discharge from Hospital [D]. Hebei University; 2017.
31. Varnfield M, Karunanithi M, Lee CK, et al. Smartphone-based home care model improved use of cardiac rehabilitation in postmyocardial infarction patients: results from a randomised controlled trial. Heart. 2014;
32. Piotrowicz E, Baranowski R, Bilinska M, et al. A new model of home‐based telemonitored cardiac rehabilitation in patients with heart failure: effectiveness, quality of life, and adherence. Eur J Heart Fail. 2010;12(2):164–171.
33. Rongjing D, Limin G, Liang Y, et al. Effectiveness and safety of community-based self-help cardiac rehabilitation model under the guidance of tertiary hospitals. Chin J Cardiovasc Dis. 2017;45(3):209–216.
34. Lian T, Liu C, Li W, et al. Investigation of cardiac rehabilitation awareness and exercise adherence after coronary intervention in elderly patients with coronary heart disease. Chin J Multiple Organ Dis. 2018;17(1):66–69.
35. Woltz S, Krijnen P, Meylaerts SAG, et al. Shared decision making in the management of midshaft clavicular fractures: nonoperative treatment or plate fixation. Injury. 2017;48(4):920–924.
36. Tinsel I, Buchholz A, Vach W, et al. Shared decision-making in antihypertensive therapy: a cluster randomised controlled trial. BMC Fam Pract. 2013;14(1):135.
37. Peng Y. Analysis of the effect of cognitive behavioral intervention on self-efficacy of patients after coronary intervention. J Armed Police Logistics Univ. 2015;24(10):795–799.
38. Ji X. Related Factors of Self-Management Behavior in Patients with Coronary Heart Disease Undergoing Percutaneous Coronary Intervention[D]. Tianjin Medical University; 2016.
39. Krishnamurthi N, Schopfer DW, Ahi T, et al. Predictors of patient participation and completion of home-based cardiac rehabilitation in the veterans health administration for patients with coronary heart disease. Am J Cardiol. 2019;123(1):19–24.
40. Lofland JH, Johnson PT, Ingham MP, et al. Shared decision-making for biologic treatment of autoimmune disease: influence on adherence, persistence, satisfaction, and health care costs. Patient Prefer Adherence. 2017;11:947.
41. Hwang R, Bruning J, Morris NR, et al. Home-based telerehabilitation is not inferior to a centre-based program in patients with chronic heart failure: a randomised trial. J Physiother. 2017;63(2):101–107.
42. Papathanasiou J, Troev T, Ferreira AS, et al. Advanced role and field of competence of the physical and rehabilitation medicine specialist in contemporary cardiac rehabilitation. Hellenic J Cardiol. 2016;57(1):16–22. doi:10.1016/s1109-9666(16)30013-6.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.