Back to Journals » Journal of Healthcare Leadership » Volume 18
Investigating the Impact of Professional Certification on Leadership Practices and Effectiveness in Health Administration in Saudi Arabia: A Cross-Sectional Mixed-Methods Study
Authors Alyaemni AA ![]() , Alomran SA
, Alomran SA
Received 26 March 2026
Accepted for publication 27 June 2026
Published 14 July 2026 Volume 2026:18 607265
DOI https://doi.org/10.2147/JHL.S607265
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Zhanming Liang
Asmaa Abdullah Alyaemni,1 Sumaih Abdullah Alomran2
1Health Administration Department, College of Business Administration, King Saud University, Riyadh, Saudi Arabia; 2Respiratory Medicine Division, Prince Sultan Military Medical City, Riyadh, Saudi Arabia
Correspondence: Asmaa Abdullah Alyaemni, Health Administration Department, College of Business Administration, King Saud University, Riyadh, Saudi Arabia, Email [email protected]
Background: Professional certification is increasingly promoted as a strategy for enhancing leadership competencies among healthcare administrators. However, evidence on its influence on leadership practices and effectiveness remains limited.
Objective: To examine the relationship between professional certification, leadership practices, and leadership effectiveness among healthcare administrators.
Methods: A cross-sectional mixed-methods study was conducted among healthcare administrators working in diverse healthcare settings. Using purposive sampling, 200 administrators were invited through email, institutional networks, and professional forums; 163 completed the survey. Leadership practices were assessed using a six-item Leadership Practices Scale, and leadership effectiveness was measured using a two-item Leadership Effectiveness Score. We evaluated Reliability and validity using Cronbach’s alpha and exploratory factor analysis. We examined associations between certification status and leadership outcomes through Independent-samples t-tests, multiple linear regression, and logistic regression. We use thematic content analysis method for qualitative responses.
Results: Participants reported high levels of leadership practices (M = 4.48, SD = 0.44) and leadership effectiveness (M = 4.12, SD = 0.69). The Leadership Practices Scale showed acceptable reliability (Cronbach’s α = 0.772) and a unidimensional structure. Although certified respondents reported slightly higher leadership practices and leadership effectiveness scores than non-certified respondents, these differences were not statistically significant in either bivariate or multivariate analyses. Certification was not an independent predictor of leadership practices or leadership effectiveness after controlling for education level and years of experience. Nevertheless, respondents perceived certification as beneficial to leadership development. Frequently reported areas of improvement included decision-making (71.7%), strategic thinking (68.6%), communication (67.9%), and organisational planning (63.5%). Additionally, 89.0% of respondents reported that certification increased or significantly increased their confidence as leaders. Qualitative findings highlighted enhanced leadership competencies, increased professional credibility, positive organisational outcomes, barriers to certification, and recommendations to expand certification opportunities.
Conclusion: Professional certification was not significantly associated with leadership practices or leadership effectiveness. In contrast, participants reported improvements in leadership competencies following certification and viewed it as contributing to teamwork, decision-making, and organisational effectiveness. These findings suggest that expanding access to certification programs may support leadership development in healthcare organizations.
Keywords: professional certification, healthcare administration, leadership development, leadership practices, leadership effectiveness, healthcare leadership
Introduction
Health administrators are essential to the delivery of efficient, high-quality healthcare services. They coordinate clinical operations, manage teams, ensure regulatory compliance, and support strategic decision-making. This wide scope of responsibility demands leadership approaches that promote adaptability, collaboration, and innovation.
Transformational leadership competencies, which emphasize vision, motivation, intellectual stimulation, and individualized consideration, have been associated with improved staff satisfaction, innovation, and organisational outcomes in healthcare settings. It supports the development of strong interpersonal relationships and eases change management, both of which are critical in healthcare environments.1–3
Professional certification is increasingly recognized as a means of validating leadership competencies in healthcare administration.4,5 Examples of widely recognized credentials include the Fellow of the American College of Healthcare Executives (FACHE) and the Certified Professional in Healthcare Quality (CPHQ). In Saudi Arabia, healthcare administrators may also pursue professional credentialing and continuing professional development opportunities through the Saudi Commission for Health Specialties (SCFHS). In addition, Master of Health Administration (MHA) programs offered by universities provide advanced training in healthcare leadership, strategic management, health policy, and organizational performance.6–8 It promotes structured learning and enhances key traits such as strategic thinking, emotional intelligence, and communication.9 Continuing professional development (CPD), often achieved through certification, aligns with broader goals in healthcare systems to improve service quality and reduce risks.10,11
In Saudi Arabia, the Vision 2030 reform agenda emphasize leadership development and workforce transformation. As the healthcare system modernizes, there is a growing demand for certified professionals capable of navigating complex organizational needs. However, despite national efforts, significant barriers are still. Financial costs, time limitations, and lack of institutional support continue to restrict access to certification programs.12,13
Although studies have linked certification to improved healthcare outcomes and employee retention, its direct impact on leadership behavior has not been well documented.4,6 In particular, the relationship between certification and leadership approaches—such as transformational, transactional, and servant leadership—is still under-explored in the context of healthcare system reform.
This study is guided by Bass’s Full Range Leadership Theory (FRLT), which serves as the overarching conceptual framework. The theory proposes that leadership exists along a continuum encompassing transformational, transactional, and laissez-faire approaches and has been widely applied in healthcare leadership research.12,14 Transformational leadership focuses on inspiring and motivating followers through a shared vision, intellectual stimulation, individualized consideration, and idealized influence. Leaders adopting this style encourage innovation, collaboration, and professional growth.1,3,14,15 Transactional leadership is based on exchanges between leaders and followers, emphasizing performance expectations, monitoring, and rewards or corrective actions to achieve organizational goals.2 Servant leadership, although not originally included in the FRLT model, complements contemporary healthcare leadership perspectives by prioritizing service to others, empowering team members, promoting ethical behavior, and fostering supportive workplace relationships.12
Professional certification may contribute to leadership development by enhancing competencies related to strategic thinking, evidence-based decision-making, communication, performance management, and professional confidence. These competencies are conceptually aligned with behaviors associated with transformational and transactional leadership approaches and may influence how healthcare administrators enact leadership practices in organisational settings. Accordingly, this study examines whether certification is associated with self-reported leadership practices and perceived leadership effectiveness among healthcare administrators. It compares certified and non-certified administrators in Saudi Arabia, about leadership behavior, competency development, and perceived impact on organizational performance.
Materials and Methods
Study Design
A cross-sectional mixed-methods design was employed to examine the association between professional certification and leadership styles among healthcare administrators. The study combined quantitative survey data, qualitative responses, and a literature review. This approach was to enable both statistical comparisons and the exploration of contextual insights.
Setting and Participants
We conducted this study in public and private healthcare facilities across multiple regions in Saudi Arabia. Participants included healthcare administrators at various levels of leadership, including department heads, supervisors, and executive-level managers. Inclusion criteria were: (a) holding a leadership or administrative role in a healthcare setting, and (b) having at least one year of managerial experience. We included Certified and non-certified individuals to allow comparative analysis.
Sampling and Data Collection
A non-probability purposive sampling approach was used to recruit eligible healthcare administrators who met the study inclusion criteria. Participants had to be currently employed in a healthcare administrative or managerial position and to provide voluntary consent. We collected the study data between 3 February 2025 and 20 April 2025 using a structured online questionnaire distributed via email, institutional networks, and professional forums. Before administration, the questionnaire underwent expert review and pilot testing to assess clarity, relevance, and content validity. A total of 200 eligible participants were invited, of whom 163 completed the questionnaire, yielding a response rate of 77.0%.
Variables and Measures
The questionnaire consisted of five sections. The first section collected demographic and professional characteristics, including age, gender, educational level, years of healthcare experience, healthcare setting, and professional certification status.
Leadership practices were assessed using six items adapted from the healthcare leadership literature. The items measured key leadership behaviours, including adaptability, collaboration, goal setting, performance feedback, strategic vision, and evidence-based decision-making. Responses were rated on a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Because factor analysis supported a single underlying construct, the six items were combined into a composite Leadership Practices Score, with higher scores indicating stronger self-reported leadership practices.
Leadership effectiveness was measured using two self-reported items assessing overall leadership performance and the frequency of positive stakeholder feedback. Responses were recorded on a five-point Likert scale, with higher scores reflecting greater perceived leadership effectiveness.
Professional certification status was assessed as a dichotomous variable (certified vs non-certified). Additional questions examined participants’ perceptions of the impact of certification on leadership competencies, professional confidence, and organizational outcomes.
The final section included five open-ended questions that explored participants’ experiences with professional certification, perceived benefits and challenges, and recommendations for leadership development and certification programs.
Questionnaire items were adapted from previously published studies in healthcare leadership and management and were reviewed by experts in health administration to establish content validity before data collection.
Validity and Reliability Assessment
Construct validity was assessed using Exploratory Factor Analysis (EFA) on the six leadership practice items. The Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy was 0.825, and Bartlett’s Test of Sphericity was significant (p <0.001), indicating suitability for factor analysis. EFA yielded a single-factor solution supporting the unidimensionality of the Leadership Practices Scale. Reliability was evaluated with Cronbach’s alpha (α = 0.772), indicating acceptable internal consistency.
Leadership effectiveness was assessed using two self-reported indicators: an overall leadership effectiveness rating and the frequency of positive stakeholder feedback. The items showed moderate positive correlation (r = 0.462, p <0.001) and were combined into a composite Leadership Effectiveness Score.
Data Analysis
Quantitative data were analyzed using SPSS version 25. Descriptive statistics summarized participant characteristics and study variables. Independent t-tests compared leadership outcomes between certified and non-certified groups, excluding those currently pursuing certifications. Multiple linear regression examined associations between certification and leadership practices/effectiveness, controlling for education and experience. Logistic regression tested associations with high leadership effectiveness categories. Statistical significance was set at p < 0.05.
Qualitative open-ended responses were analyzed using thematic content analysis, coded inductively, and grouped into themes on leadership development, certification impact, organizational outcomes, barriers, and recommendations.
Ethical Considerations
Ethical approval was granted by King Saud University Institutional Review Board (Ref. KSU-HE-25-180). Riyadh, Saudi Arabia. Participation was voluntary with informed consent. Data were anonymized.Participants could withdraw at any point without any consequences.
Results
Participant Characteristics
In total, 163 healthcare administrators participated. Most (48.5%) were aged 31–40 years, followed by 41–50 years (29.4%). The majority were male (71.2%)—education levels: 56.4% master’s degree, 27.0% bachelor’s, 14.7% doctorate. Almost half (48.5%) had over 11 years of administrative experience. Certification status: 54.0% certified, 39.9% not certified, 6.1% currently pursuing. Most worked in hospitals (81.0%) (Table 1).
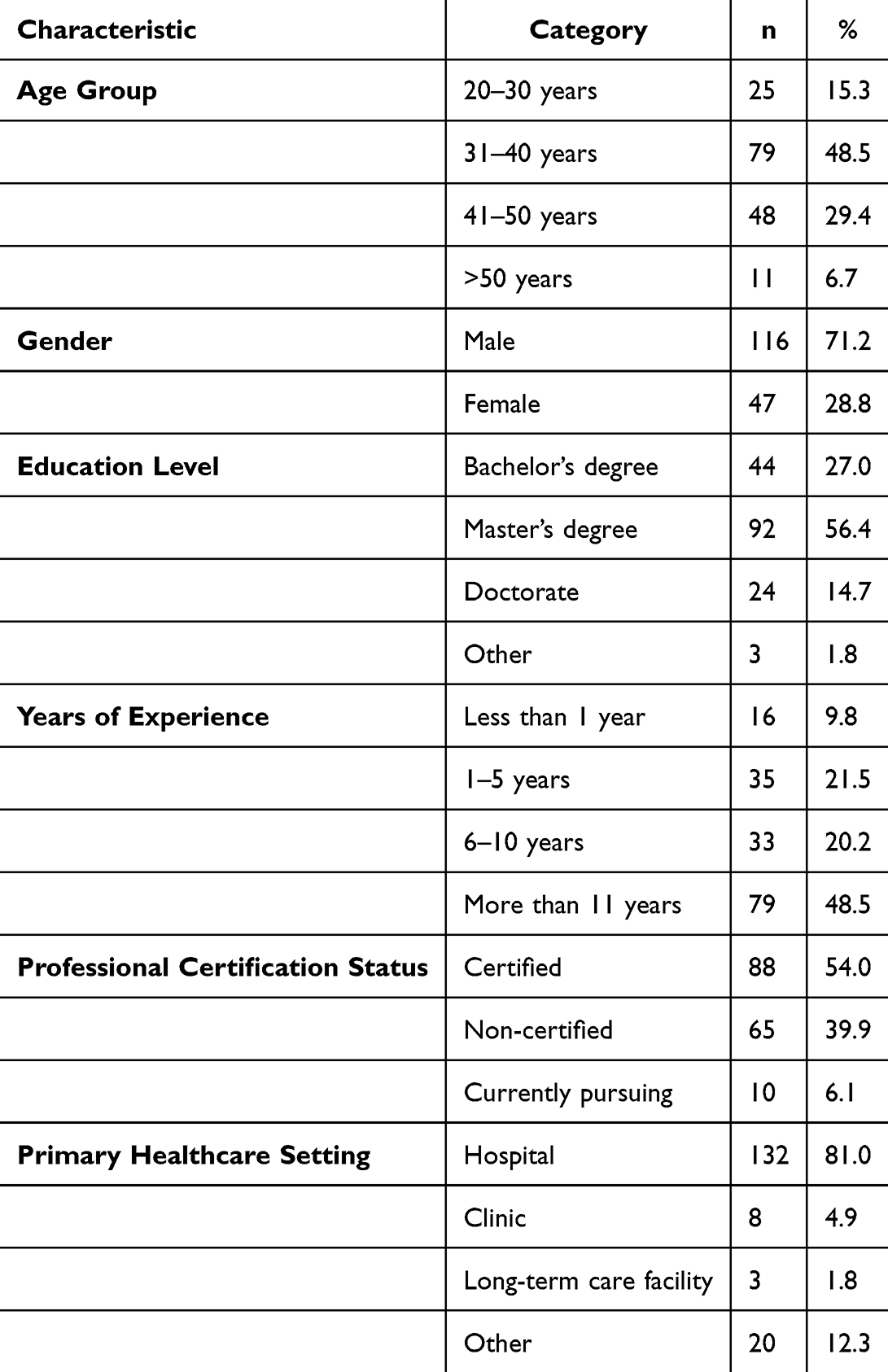 |
Table 1 Demographic Characteristics of Participants (N = 163) |
Reliability and Validity of Leadership Measures
EFA supported a unidimensional structure for leadership practice items. Internal consistency was good (α = 0.772). Leadership effectiveness items correlated moderately (r = 0.462, p<0.001), supporting aggregation (Table 2).
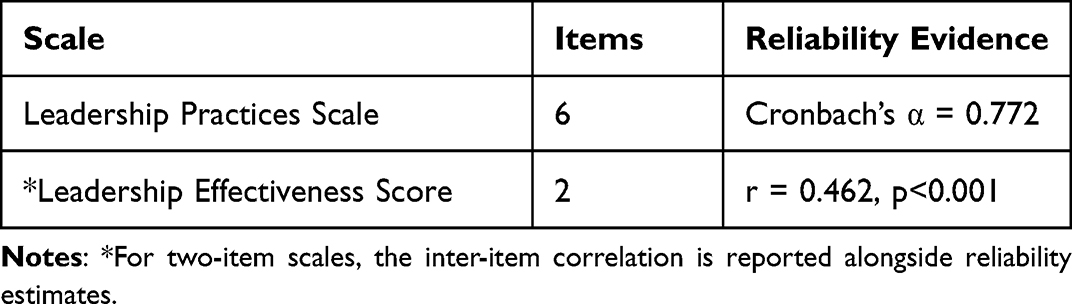 |
Table 2 Reliability and Validity Assessment of Study Scales (n = 163) |
Descriptive Statistics
Participants reported high leadership practices (M = 4.48, SD = 0.44) and leadership effectiveness (M = 4.12, SD = 0.69) (Table 3).
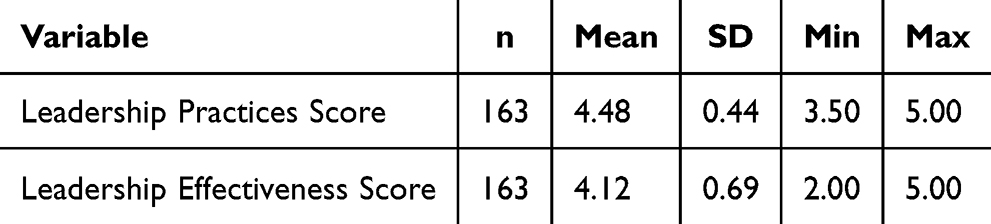 |
Table 3 Descriptive Statistics of Study Variables (n = 163) |
Comparison by Certification
Independent t-tests showed that certified administrators scored higher on leadership practices (M = 4.54) than non-certified administrators (M = 4.43), but the difference was not statistically significant (p =0.131). For leadership effectiveness, certified scored 4.22 versus 4.00 for non-certified (p = 0.055) (Table 4).
 |
Table 4 Comparison of Leadership Outcomes by Certification Status (n=153) |
Regression Analyses
Multiple linear regression showed that certification was not a significant predictor of leadership practices (B = 0.100, p = 0.175) or leadership effectiveness (B = 0.122, p = 0.314) after controlling for education and experience. Years of experience had a marginal positive association with leadership practices (p = 0.065). Models explained limited variance (Tables 5 and 6).
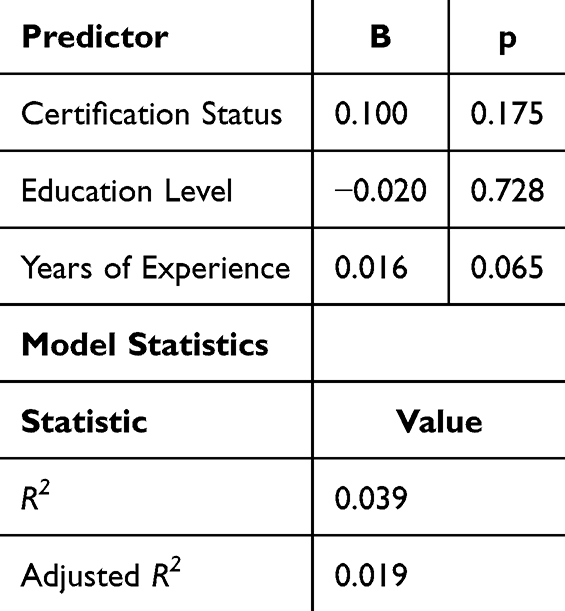 |
Table 5 Multiple Linear Regression Predicting Leadership Practices (n=153) |
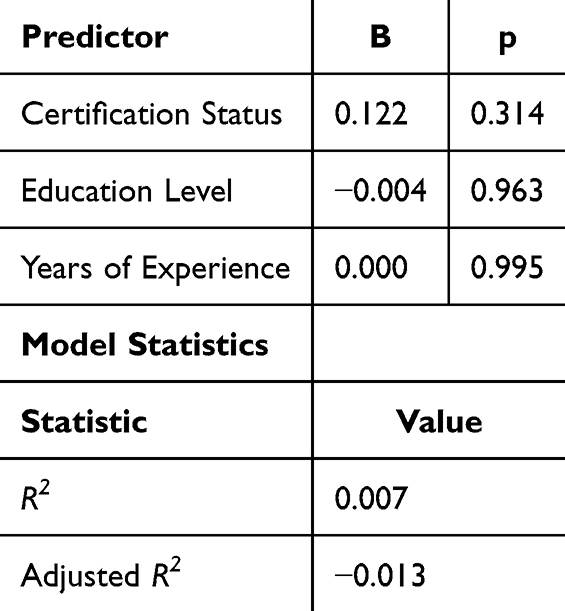 |
Table 6 Multiple Linear Regression Predicting Leadership Effectiveness (n=153) |
Logistic Regression
Professional certification was not associated with high leadership effectiveness after adjustment (OR = 1.10; 95% CI: 0.54–2.27; p = 0.786) (Table 7).
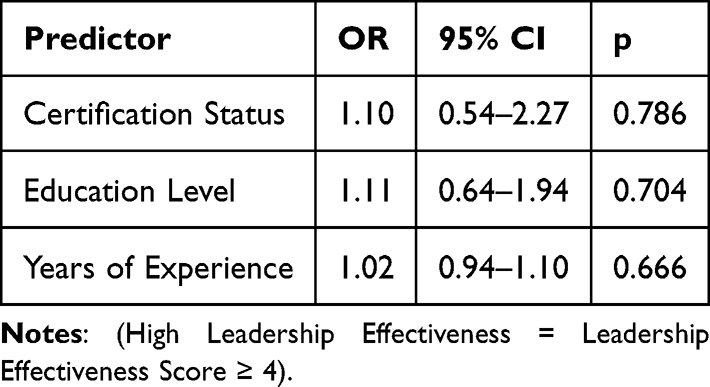 |
Table 7 Logistic Regression Predicting High Leadership Effectiveness (n=153) |
Competency Improvements
Respondents reported the greatest competency improvements with certification in decision-making (71.7%), strategic thinking (68.6%), communication (67.9%), organizational planning (63.5%), emotional intelligence (56.0%), and conflict resolution (50.9%) (Table 8).
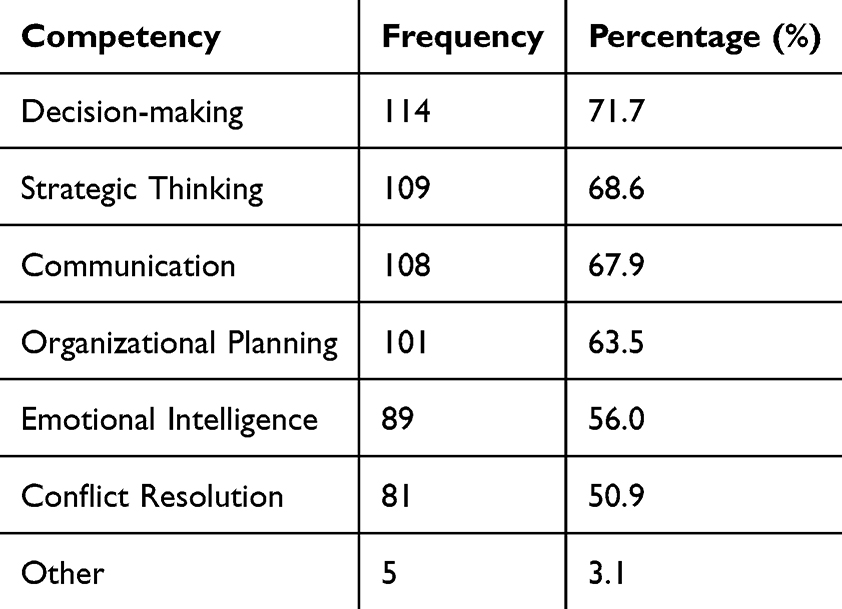 |
Table 8 Perceived Competencies Improved Through Professional Certification (n = 163) |
Leadership Confidence
Most respondents (89%) showed certification increased or significantly increased their leadership confidence (Table 9).
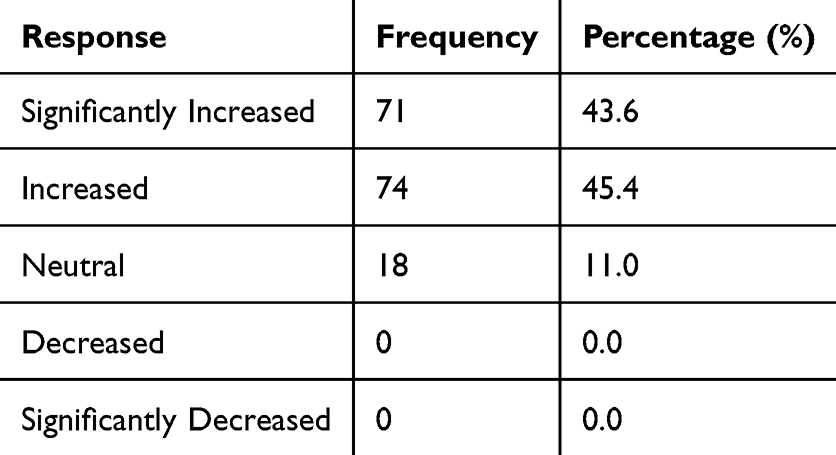 |
Table 9 Impact of Professional Certification on Leadership Confidence (n = 163) |
Qualitative Findings
Enhanced Leadership Competencies
Participants often reported that professional certification contributed to the development of key leadership competencies, including leadership skills, decision-making abilities, communication, and strategic thinking. Many respondents perceived certification as providing practical knowledge and frameworks that improved their effectiveness in leadership roles and strengthened their ability to address workplace challenges. One participant noted that certification “enhances leadership skills and improves leadership practices.” Another stated that it “gives different ways of making decisions and looking at things from different angles.” Participants also highlighted the role of certification in strengthening professional communication and applying best practices, with one respondent explaining that certification “shows you the guidelines and enhances your skills, as well as strengthens and develops communication.” Collectively, these findings suggest that certification may support leadership development by broadening managerial perspectives, improving decision-making capabilities, and enhancing communication skills necessary for effective healthcare administration.
Increased Professional Credibility
Participants reported that professional certification enhanced their professional credibility, confidence, and reputation within their organizations. Many respondents perceived certification as a means of gaining greater trust, authority, and respect from colleagues and team members. Certification was also viewed as providing validation of professional knowledge and competence, reinforcing confidence in leadership and decision-making roles. One participant said that certification is “an improvement tool and it’s helping to be a leader with confidence.” Another noted that “the certificates [are] important to define things and let you know if you are on the right track.” These findings suggest that certification may strengthen professional identity and increase perceived credibility, thereby supporting leadership development and effectiveness in healthcare administration.
Positive Organizational Outcomes
Participants often perceived professional certification as contributing to positive organizational outcomes, including improved patient care quality, stronger employee engagement, enhanced teamwork, and greater organizational effectiveness. Respondents emphasized that certification strengthened communication, collaboration, and leadership capabilities, thereby facilitating more effective teamwork and workplace relationships. One participant noted that certification “helps with teamwork, as well as understanding the work itself through explanation and asking questions.” Others highlighted the influence of leadership on team performance and patient care, saying that “leadership has a great impact on the team by inspiring and motivating them to serve patients and recognize work that is well done.” Participants also suggested that certification improved their ability to respond to diverse patient needs, with one respondent explaining that “it affects how we deal with different patients, as they all have different experiences.” Collectively, these findings suggest that certification may support organizational performance by enhancing leadership competencies, teamwork, staff engagement, and patient-centered care.
Barriers to Certification
Participants identified several barriers to obtaining professional certification, primarily related to time constraints, financial costs, and limited organizational support. Many respondents reported difficulty balancing work responsibilities with the time required for study and professional development, noting that “Managing work responsibilities leaves limited time for personal development.” Others highlighted the inflated costs associated with certification programs and examination fees as significant obstacles, explaining that “The fees and time required for study are major barriers, as certification costs are often high.”
Greater Certification Uptake
Participants suggested several strategies to improve access to professional certification, including providing dedicated study leave and expanding educational support. One participant recommended “dedicated days off for studying or participating in online training,” while another advocated for “one centralized platform with regular programs, discounted fees, qualified trainers, and a well-prepared curriculum.” These recommendations highlight the importance of organizational and institutional support in facilitating certification attainment.
Overall, the qualitative findings suggest that professional certification may support leadership development and positively influence organizational culture, teamwork, professional credibility, and perceived organizational effectiveness beyond individual skill enhancement.
Discussion
This study examined the association between professional certification and leadership practices and effectiveness among healthcare administrators in Saudi Arabia. Although certified respondents reported marginally higher leadership practices and effectiveness scores than non-certified respondents, these differences were not statistically significant in either bivariate or multivariate analyses. This lack of significant association contrasts with some prior research that has reported positive correlations between certification and improved leadership performance and organizational outcomes.3,4,6 One explanation for the null findings is the uniformly high self-reported leadership scores across participants regardless of certification status, which may have led to a ceiling effect, restricting variability and reducing the statistical power to detect differences. Additionally, the sample size and cross-sectional design might have limited the ability to capture subtle or long-term effects of certification on leadership behavior.
Although the quantitative analyses did not prove statistically significant differences in leadership practices or effectiveness between certified and non-certified healthcare administrators, the qualitative findings suggest that professional certification may contribute to organizational outcomes through several indirect pathways. The respondents identified specific competencies—decision-making, strategic thinking, communication, organizational planning, emotional intelligence, and conflict resolution—that were strengthened through certification. These competencies are essential for effective healthcare leadership, especially in complex and rapidly changing healthcare environments,9,10 which is known to influence leadership effectiveness positively.7,14 Thematic analysis further elucidated how certification contributes to leadership growth, increasing professional credibility among peers and fostering enhanced organizational outcomes such as improved patient care quality, stronger employee engagement, and teamwork. These findings support prior studies suggesting that certification bolsters leadership identity and professional recognition, which can translate to improved organizational culture and performance.4,11,14
However, respondents also highlighted persistent barriers to certification, including financial costs, time constraints due to workloads, and limited institutional support. These challenges are consistent with previous research indicating that organizational and policy-level interventions are necessary to facilitate broader access to certification programs.11,14 Strategies such as employer sponsorship, flexible timing, online certification courses, and financial aid may alleviate these barriers and encourage more administrators to pursue certification.
The results suggest that while professional certification may not yield immediately measurable improvements in overall leadership practices or effectiveness as captured by survey scales, it influences important leadership competencies and fosters confidence, which are likely to contribute to long-term leadership development and organizational success. Given the critical role of leadership in healthcare transformation initiatives such as Saudi Arabia’s Vision 2030, supporting certification as part of a comprehensive leadership development strategy appears beneficial.12,14
Future research should use larger, longitudinal study designs incorporating validated and nuanced leadership assessment tools to better capture the dynamic impacts of professional certification over time. Additionally, exploring objective organizational performance metrics alongside leadership assessments would strengthen understanding of the practical value of certification in healthcare administration.
Limitations of the Study
This study has several limitations that should be considered when interpreting the findings. First, the cross-sectional design captures participants’ perceptions at a single point in time and therefore does not permit conclusions regarding causal relationships between certification status and leadership outcomes. Second, leadership behaviors were assessed using self-reported measures, which may be subject to social desirability and response biases. Third, the use of purposive sampling may limit the generalizability of the findings to other healthcare settings or professional groups. Finally, the relatively high leadership scores reported across participants may have reduced score variability, potentially limiting the ability to detect subtle differences between certified and non-certified individuals. Future longitudinal studies with larger and more diverse samples are recommended to further examine the long-term impact of professional certification on leadership development.
Conclusion
Professional certification was not significantly associated with leadership practices or leadership effectiveness based on quantitative measures. However, certification was associated with perceived improvements in leadership-related competencies and was widely viewed by participants as enhancing confidence, professional development, and professional credibility. Qualitative findings further suggested that certification may contribute to positive organizational outcomes through stronger teamwork, improved communication, enhanced decision-making, greater employee engagement, and more patient-centered care.
Although these findings should be interpreted cautiously given the cross-sectional design and reliance on self-reported measures, they indicate that professional certification may provide value beyond measurable differences in leadership practices and effectiveness. For healthcare organizations, certification may serve as a practical part of leadership development initiatives by strengthening competencies that support effective management and organizational performance. Expanding access to certification opportunities and integrating certification into leadership development pathways may help build workforce capacity, strengthen leadership pipelines, and support organizational effectiveness. Future research using longitudinal designs and objective organizational performance indicators is needed to further evaluate the long-term impact of professional certification on leadership and healthcare organizational outcomes.
Acknowledgments
Supported by Ongoing Research Funding program (ORF-2026-870), King Saud University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bass BM, Avolio BJ. Improving Organizational Effectiveness Through Transformational Leadership. Thousand Oaks, CA: Sage Publications; 1994.
2. Specchia ML, Cozzolino MR, Carini E, et al. Leadership styles and nurses’ job satisfaction: results of a systematic review. Int J Environ Res Public Health. 2021;18(4):1552. doi:10.3390/ijerph18041552
3. Jacobsen CB, Andersen LB, Bøllingtoft A, Eriksen TLM. Can leadership training improve organizational effectiveness? Evidence from a randomized field experiment on transformational and transactional leadership. Public Adm Rev. 2021;82(1):117–11. doi:10.1111/puar.13356
4. Hejazi MM, Al-Rubaki SS, Bawajeeh OM, et al. Attitudes and perceptions of health leaders for the quality enhancement of workforce in Saudi Arabia. Healthcare. 2022;10(5):891.
5. Rahman R. The privatization of health care system in Saudi Arabia. Health Serv Insights. 2020;13:1178632920934497. doi:10.1177/1178632920934497
6. Giovanelli L, Rotondo F, Fadda N. Management training programs in healthcare: effectiveness factors, challenges, and outcomes. BMC Health Serv Res. 2024;24(1).
7. Mlambo M, Silén C, McGrath C. Lifelong learning and Nurses’ continuing professional development, a metasynthesis of the literature. BMC Nurs. 2021;20:62.
8. Hassan Z. Employee retention through effective human resource management practices in maldives: mediation effects of compensation and rewards system. Questa Soft. 2022.
9. Odeh RBM, Obeidat BY, Jaradat MO, Masa’deh R, Alshurideh MT. The transformational leadership role in achieving organizational resilience through adaptive cultures: the case of Dubai Service Sector. Int J Prod Perform Manag. 2021;72(2):440–468. doi:10.1108/IJPPM-02-2021-0093
10. Young M, Smith MA. Standards and Evaluation of Healthcare Quality, Safety, and Person-Centered Care. PubMed; StatPearls Publishing; 2022.
11. Alilyyani B, Kerr MS, Wong C, Wazqar DY. An integrative review of nursing leadership in Saudi Arabia. Nursing Open. 2021;9(1):140–155. doi:10.1002/nop2.1117
12. Canavesi A, Minelli E. Servant leadership: a systematic literature review and network analysis. Employee Respons Rights J. 2022;34(3):267–289. doi:10.1007/s10672-021-09381-3
13. Bass BM, Riggio RE. Transformational Leadership.
14. Rahman R, Qattan A. Vision 2030, and sustainable development: state capacity to revitalize the healthcare system in Saudi Arabia. Inquiry. 2021;58.
15. Alotaibi SY. Accreditation of Primary Health Care Centers in the KSA: lessons from developed and developing countries. J Taibah Univ Med Sci. 2023;18(4):711–725. doi:10.1016/j.jtumed.2022.12.012
16. Hussain MK, Khayat RAM. The impact of transformational leadership on job satisfaction and organisational commitment among hospital staff: a Systematic review. J Health Manag. 2021;23(4):614–630. doi:10.1177/09720634211050463
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Bridging the Leadership Gap: Developing a Culturally Adapted Leadership Program for Healthcare Professionals in Oman
Al Sawafi A, Al Yahyaei A, Al Azri NH, Al Sabei SD, Al Maamari AM, Al Battashi H, Al Ismaili SR, Al Maskari JK
Journal of Healthcare Leadership 2025, 17:365-381
Published Date: 12 August 2025