Back to Journals » Clinical Ophthalmology » Volume 13
Intrastromal Corneal Ring Segments Implantation And Corneal Cross-Linking For Keratoconus In Children With Vernal Keratoconjunctivitis – Three-Year Results
Authors Abozaid MA ![]() , Hassan AAA, Abdalla A
, Hassan AAA, Abdalla A
Received 17 June 2019
Accepted for publication 27 September 2019
Published 5 November 2019 Volume 2019:13 Pages 2151—2157
DOI https://doi.org/10.2147/OPTH.S219688
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Mortada Ahmed Abozaid.
Views: 885
Mortada Ahmed Abozaid,1 Amin Abo-Ali Hassan,1 Abdelsalam Abdalla2
1Department of Ophthalmology, Faculty of Medicine, Sohag University, Sohag, Egypt; 2Department of Ophthalmology, Faculty of Medicine, Assiut University, Assiut, Egypt
Correspondence: Mortada Ahmed Abozaid
Ophthalmology Department, Faculty of Medicine, Sohag University, Sohag, Egypt
Tel +20932309244
Fax +20932325531
Email [email protected]
Purpose: To assess the 3-year safety and efficacy of femtosecond laser-assisted intrastromal corneal ring segments’ (ICRS) implantation followed or accompanied by transepithelial accelerated corneal collagen cross-linking (TE-ACXL) as a treatment of keratoconus in children with vernal keratoconjunctivitis (VKC).
Patients and methods: Fifty two eyes of 28 children with keratoconus and vernal VKC were included in this study. Cases were divided into 2 groups; the first group had been treated with femtosecond laser-assisted ICRS (Keraring) implantation accompanied or followed by TE-ACXL, while the second group had been treated by TE-ACXL only and all cases completed a follow-up period of 3 years.
Results: In group 1: the mean uncorrected (UCVA) and best-corrected (BCVA) visual acuity, spherical equivalent, K-max and Q-value improved markedly from 0.97 ± 0.19, 0.67 ± 0.18, −8.75 ± 4.55, 60.41 ± 4.98, and −1.18 ± 0.54 preoperatively to 0.61 ± 0.27, 0.39±0.21, −3.25 ± 3.56, 55.22 ± 5.72, and −0.44 ± 0.68 postoperatively respectively. While in group 2: the preoperative mean UCVA, BCVA, spherical equivalent, K-max and Q-values were 0.68 ± 0.28, 0.38 ± 0.24, −2.84 ± 2.59, 50.29 ± 4.04, and-0.58 ± 0.23 respectively while their corresponding postoperative values were 0.58 ± 0.34, 0.19 ± 0.17, −2.35 ± 2.07, 49.58 ± 3.26, and −0.57 ± 0.25. Only one case in group 1 required repeat cross-linking.
Conclusion: Although the long-term safety and efficacy of femtosecond laser-assisted ICRS implantation accompanied or followed by TE-ACXL in children with keratoconus and VKC is high, some cases still may need repeat cross-linking.
Keywords: accelerated transepithelial cross-linking, Keraring, pediatric keratoconus, spring catarrh
Introduction
Keratoconus is a bilateral non-inflammatory corneal disorder characterized by progressive thinning of the stroma leading to a conical-shaped cornea. It has an estimated annual incidence of two in 100,000 and a prevalence of 54.5 in 100,000. The induced myopia and irregular astigmatism lead to a variable degree of vision impairment.1–3
The onset of keratoconus is usually around puberty but may develop earlier, especially in conditions associated with chronic eye rubbing like vernal keratoconjunctivitis (spring catarrh).2
Vernal keratoconjunctivitis (VKC) is a severe form of allergic keratoconjunctivitis that appears in children and adolescents with seasonal recurrence. It is more common in boys than girls and tends to resolve at puberty. It is relatively common in regions with warm dry climates including upper Egypt4 where this study was performed.
Pediatric keratoconus is rapidly progressive and its diagnosis is usually delayed.5
Corneal collagen cross-linking (CXL) has become the standard treatment of non-advanced keratoconus. It strengthens the cornea and prevents progression of the disease and thereby delays or avoids the need for keratoplasty.6,7 The transepithelial (epithelium-on) method of CXL is preferred by some surgeons in children over the epithelium-off method because it is as effective but less painful, and less complicated.8
Implantation of intrastromal corneal ring segments (ICRS) into a circular corneal tunnel reduces the central corneal steepening and improves visual acuity in ectatic corneas with high accuracy when assisted by femtosecond laser.9,10 Keraring is a type of ICRS made of polymethylmethacrylate. It is triangular in cross section with a 600-µm base and is available in different arc lengths (90–210 degrees) and variable thicknesses (0.15–0.35 mm).11
The purpose of this study was to evaluate the 3-year safety and efficacy of femtosecond laser-assisted keraring implantation accompanied or followed by transepithelial accelerated corneal cross linking (TE-ACXL) compared to (TE-ACXL) alone in children with keratoconus and VKC.
Materials And Methods
Patient charts of 28 children with keratoconus and VKC were included in this retrospective comparative study in the period between January 2015 to October 2018 at the ophthalmology department of Sohag university hospital in association with Sohag Future Femtolasik center in Egypt. The study followed the declaration of Helsinki and approval was obtained from the ethics committee of Sohag faculty of medicine (reference number 882/2018). Written consent was obtained from the parents to review the medical records of their children.
The inclusion criteria at the time of surgery were patients less than 18 years old with progressive keratoconus (progression is defined as 1 D increase in steepest keratometric reading over a 6-month period), clear central cornea and mild to moderate VKC. After surgery, all patients completed a follow-up period of at least 3 years.
The exclusion criteria at the time of surgery included patients with severe form of VKC or advanced keratoconus and eyes with corneal opacity, active ocular infection or inflammation or previous surgery.
Preoperative and postoperative assessment of the patients included uncorrected (UCVA) and best-corrected (BCVA) visual acuity, manifest and cycloplegic refraction, slit lamp and fundus examination in addition to measurement of intraocular pressure. Diagnosis, staging, and follow-up of keratoconus were done using a Sirius Scheimflug imaging camera (CSO, Italy). Staging of keratoconus was based on the Amsler-Krumeich classification. Vector analysis of the manifest cylinder was done using the following equations:


where J0 represents cylinder power set at 90° and 180° meridians with positive values indicating “with-the rule” astigmatism, and negative values indicating “against the rule” astigmatism while J45 refers to cylinder power set at 45° and 135° meridians, representing oblique astigmatism and  is the axis of the cylinder.
is the axis of the cylinder.
The cases (operated on by 3 surgeons) were divided into 2 groups:
Group 1 (Keraring Implantation + CXL)
Included, at the time of surgery, children with stage 2 or 3 keratoconus and poor BCVA (less than 6/18) and with corneal thickness of at least 450 µm at the planned site of Keraring implantation. The choice of suitable segments was based on the Keraring nomogram provided by the manufacturer, Mediphacos. The keraring implantation was done under general anesthesia in uncooperative children (17 children) followed after 2–4 weeks by transepithelial cross-linking under topical anesthesia in order to ensure good fixation during cross-linking. While in older cooperative children, the keraring implantation and transepithelial cross-linking were done simultaneously under topical anesthesia. In patients with active VKC, the surgery was delayed until complete subsidence of the episode occurs by medical treatment including topical steroids and topical mast cell stabilizers ± oral antihistamines.
Surgical Procedure
- Femtosecond laser-assisted Keraring implantation: in children requiring general anesthesia, marking the center of the cornea by asking the patient to look at the flashing light of the microscope should be done before induction of anesthesia. The suction ring is applied and the corneal tunnel is created with femtosecond laser (iFS Advanced femtosecond laser, Abbott, Chicago, Illinois, USA). After confirming the patency of the tunnel with a spatula, the Keraring segments are inserted. A contact lens is applied and left for 7 days.
- Transepithelial accelerated corneal cross-linking: was done for all cases under topical anesthesia as follows:
dextran-free hypo-osmolar riboflavin drops containing benzalkonium chloride to enhance epithelium permeability (ParaCel, Avedro, Waltham, Massachusetts, USA) were dripped onto the cornea every 1.5 min for 4.5 mins and then benzalkonium chloride-free riboflavin drops (VibexXtra, Avedro, Waltham, Massachusetts, USA) were dripped every 1.5 min for 6 mins. This was followed by 2 mins and 40 seconds of accelerated CXL (The KXL accelerated CXL System, Avedro, Waltham, Massachusetts, USA) using the pulsed mode (2 seconds on/1 second off) with a power of 45 mW/cm2 and a total energy radiated of 7.2 J/cm2. A contact lens was then applied and left for one week and eye drops (artificial tears, steroids and antibiotics) were prescribed for 4 weeks.
Group2: (CXL Only)
Included, at the time of surgery, children with stage 1 keratoconus and those with stage 2 or 3 but with BCVA of more than 6/18 or those who refused ICRS implantation or could not afford it. All cases had minimal corneal thickness of 400 µm. These eyes were subjected to transepithelial collagen cross linking only as mentioned in group 1 and were followed for at least 3 years.
Postoperative Treatment
The topical treatment included the antibiotic moxifloxacin, the steroid prednisolone, and artificial tears. The artificial tears were used every hour during the first day, and five times daily for 1 month. The antibiotic was used every hour for the first day, and then decreased to five times daily for 10 days. The steroid was used every hour for the first day, then decreased to five times daily for 1 week, and then decreased gradually over 4 weeks. A systemic analgesic was prescribed to manage pain due to CXL.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics for Windows version 20.0. (SPSS Inc, Chicago, Illinois, USA) Quantitative data were expressed as means ± standard deviation. Qualitative data were expressed as number and percentage. The data were tested for normality using Shapiro-Wilk test. The Independent Samples T test, and Paired Samples T test were used for normally distributed data. The nonparametric Mann–Whitney test, and Wilcoxon Signed Ranks test were used for data which were not normally distributed. Chi-Square test was used for comparison between qualitative variables. A 5% level was chosen as a level of significance in all statistical tests used in the study.
Results
This retrospective study included 28 children with keratoconus and VKC: twenty patients (32 eyes) in group 1 and 14 patients (20 eyes) in group 2 with 6 patients included in both groups (one eye received Keraring+CXL and the other eye received CXL only). The mean age of group 1 was 14.1 ± 2.4 years (range 10–17 years) while that of group 2 was 14.64 ± 2.34 years (range 9–17 years). Group 1 included 12 boys and 8 girls while group 2 included 7 boys and 7 girls.
The preoperative values of both groups are shown in Table 1. All parameters showed statistical difference between the 2 groups except for J45, thinnest location and corneal volume. This can be explained by difference in stage of keratoconus between the 2 groups.
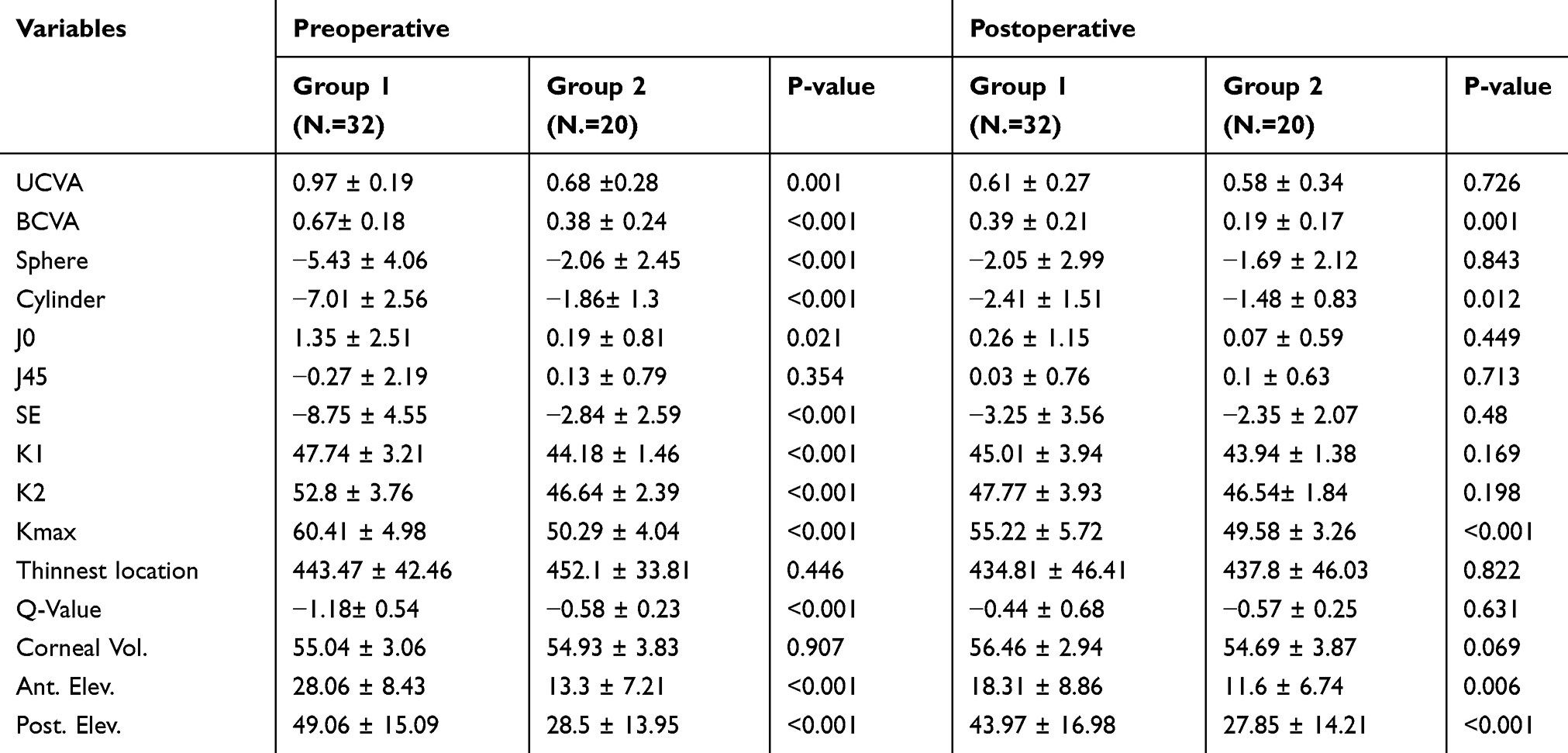 |
Table 1 Comparison Between The 2 Groups Regarding Preoperative And Postoperative Measures |
Comparing the preoperative and postoperative values in group 1 showed significant change in all parameters except J45, as shown in Table 2 and Figures 1–3. There was significant decrease in UCVA and BCVA (log MAR), significant decrease in sphere, cylinder, SE and J0. The reduction in J0 denotes improvement in “with the rule” astigmatism. All the tomographic parameters were reduced significantly including K1, K2, K-max, Q-value at 8 mm, anterior elevation, and posterior elevation. Also, the thinnest location decreased significantly, probably from increased compactness of the cornea due to CXL rather than progression of the disease. The 10-mm corneal volume increased significantly, probably from the tissue expanding effect of the ICRS. Only the J45 value did not show significant change which can be attributed to limited effect of ICRS on oblique astigmatism.
 |
Table 2 Comparison Between Preoperative And Postoperative Measures In The 2 Groups |
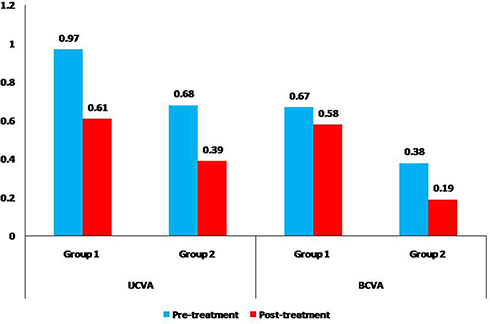 |
Figure 1 Chart showing a comparison between the study groups regarding the mean preoperative and postoperative uncorrected (UCVA) and best-corrected (BCVA) visual acuity. |
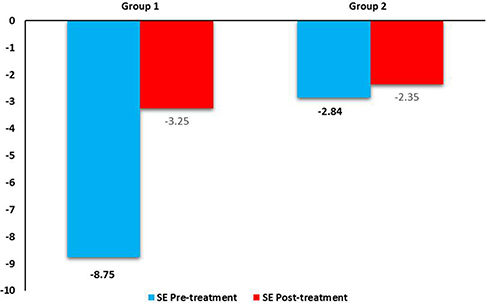 |
Figure 2 Chart showing a comparison between the study groups regarding the mean preoperative and postoperative spherical equivalent (SE). |
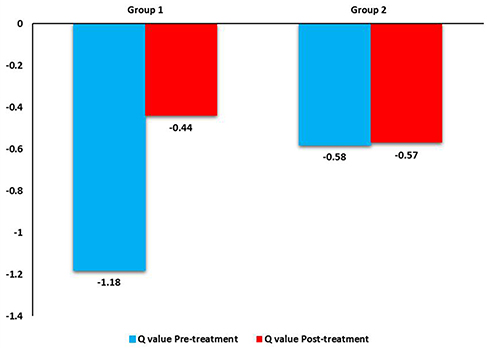 |
Figure 3 Chart showing a comparison between the study groups regarding the mean preoperative and postoperative 8mm Q-value. |
When comparing the preoperative and postoperative values in group 2, there was significant improvement in the visual parameters only (Figure 1). There were reductions in refractive and tomographic parameters but they did not reach the statistical significance level of 5% as seen in Table 2 and Figures 2–4.
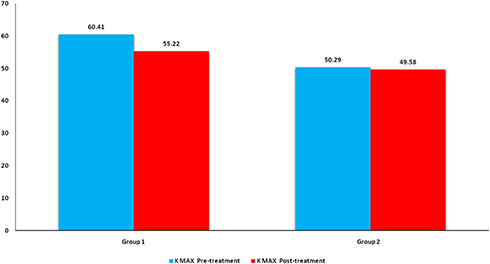 |
Figure 4 Chart showing a comparison between the study groups regarding the mean preoperative and postoperative Kmax. |
When comparing the postoperative values of the 2 groups (Table 1), significant differences in the BCVA, cylindrical error, K-max, anterior elevation, and posterior elevation are revealed. This may highlight the efficacy of ICRS in improving UCVA, spherical error, K1, K2 and 8 mm Q value to levels approximating those of group 2 patients.
During 3 years of follow-up, one patient in group 1 showed progression of her keratoconus after one year of combined Keraring implantation and CXL as detected by progressive increase in her K readings (K2 increased from 47.88 to 49.29 D), myopia (from −4.00 to −6.00 D) and astigmatism (from 2.00 to 3.00D) as shown in Figure 5. This case received repeat transepithelial accelerated CXL and showed stability uptill now.
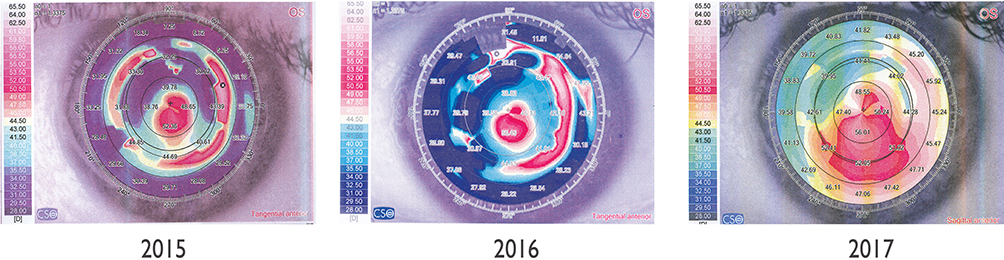 |
Figure 5 Consecutive Scheimflug images of the case that required repeat cross-linking. |
Discussion
The association between keratoconus and vernal keratoconjunctivitis is relatively common in upper Egypt where the climate is hot and dry. Children with both keratoconus and VKC are difficult to manage because of delayed diagnosis, rapid progression of their ectasia, persistent eye rubbing, and poor compliance. At the same time, poor access to donor eye-banks in addition to difficulties and high cost necessitate more efforts to avoid or delay the need for keratoplasty in these children.
In this study, the safety and efficacy of femtosecond laser-assisted keraring implantation accompanied or followed by transepithelial accelerated CXL in children with keratoconus and VKC, were retrospectively evaluated and compared to transepithelial accelerated CXL alone. After 3 years of observation, both techniques can be considered effective in stabilizing the ectatic condition, although the combined ICRS and CXL can, in addition, improve the visual, refractive, and tomographic parameters. Also, both techniques can be considered safe as no major complication such as ring segment extrusion, corneal vascularization or opacification was recorded in all cases. However, one case in group 1 showed progression of ectasia and required repeat cross-linking.
In 2011, Khan and Muhtaseb reported the first case of ICRS implantation in an 11 year old boy with keratoconus and VKC. They did bilateral simultaneous implantation of one 0.40 Intacs segment in each eye using the manual technique to create the tunnels.12 The ICRS implantation was not accompanied or followed by CXL and the child did well during a 12-month follow-up.
In his prospective pilot study on children with keratoconus and VKC,13 Abozaid proved the safety and efficacy after one year of femtosecond laser-assisted keraring implantation followed by transepithelial cross linking. Unlike his study, this study was retrospective, had longer follow-up duration, had larger sample size, had a control group with CXL alone, and studied more parameters such as the corneal volume, Q value, and vector analysis of the astigmatism.
Abdelmassih et al14 retrospectively evaluated ICRS (Intacs and Kerarings) followed after one month by standard epithelium-off CXL in 12 children (17 eyes) with keratoconus (mean age 12.3 years) and found marked improvement in UDVA and CDVA with reduction in keratometry and spherical equivalent which were stable through relatively long duration of 4 years. The only complication reported in this study was removal of one ring segment after two years due to vascularization and corneal thinning.
In their retrospective case series, Olivo-Payne et al15 showed tomographic and refractive stability in more than 91% of eyes with pediatric progressive keratoconus who underwent transepithelial accelerated CXL. Fourteen children (23 eyes) were included in their study, of them, 14 eyes of 8 patients had associated atopy. A clear and continuous demarcation line was detected in 19 eyes (82.6%) with average central depth of 210.63±27.50 μm.
Tian et al16 retrospectively evaluated transepithelial accelerated CXL in 18 eyes of 17 children with keratoconus (mean age 14.44 ± 1.98 years). After 12 months, they noted improvement in the BCVA in 7 (38.89%) eyes, stabilization in 8 (44.44%) eyes, and worsening in 3 (16.67%) eyes and concluded that accelerated transepithelial CXL is a safe and effective treatment in children with progressive keratoconus.
Sarac et al17 compared the 2-year results of accelerated and standard cross-linking in children with keratoconus and concluded that the 2 procedures have similar efficacy and safety and recommended the accelerated technique, being rapid, for this group of patients.
Conclusion
The results of this study should encourage ophthalmologists to adopt the use of ICRS and CXL when indicated in children with keratoconus and VKC to avoid or delay the need for keratoplasty. The complications that may arise from persistent eye rubbing such as infection, extrusion or vascularization can be avoided by proper selection of cases and prompt treatment of new episodes of allergy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Krachmer JH, Feder RS, Belin MW. Keratoconus and related noninflammatory corneal thinning disorders. Surv Ophthalmol. 1984;28:293–322. doi:10.1016/0039-6257(84)90094-8
2. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42:297–319. doi:10.1016/s0039-6257(97)00119-7
3. Kennedy RH, Bourne WM, Dyer JA. A 48-year clinical and epidemiologic study of keratoconus. Am J Ophthalmol. 1986;101:267–273. doi:10.1016/0002-9394(86)90817-2
4. Saro AS, Radwan GA, Mohammed UA, Abozaid MA. Screening for keratoconus in a refractive surgery population of upper Egypt. Delta J Ophthalmol. 2018;19:19–23. doi:10.4103/DJO.DJO_39_17
5. El-Khoury S, Abdelmassih Y, Hamade A, et al. Pediatric keratoconus in a tertiary referral center: incidence, presentation, risk factors, and treatment. J Refract Surg. 2016;32(8):534–541. doi:10.3928/1081597X-20160513-01
6. Wollensak G, Spoerl E, Seiler T. Stress–strain measurements of human and porcine corneas after riboflavin-ultraviolet-A-induced cross-linking. J Cataract Refract Surg. 2003;29:1780–1785. doi:10.1016/s0886-3350(03)00407-3
7. Goldich Y, Marcovich AL, Barkana Y, Avni I, Zadok D. Safety of corneal collagen cross-linking with UV-A and riboflavin in progressive keratoconus. Cornea. 2010;29:409–411. doi:10.1097/ICO.0b013e3181bd9f8c
8. Magli A, Forte R, Tortori A, Capasso L, Marsico G, Piozzi E. Epithelium-off corneal collagen cross-linking versus transepithelial cross-linking for pediatric keratoconus. Cornea. 2012;1–5.
9. Colin J, Cochener B, Savary G, Malet F. Correcting keratoconus with intracorneal rings. J Cataract Refract Surg. 2000;26(8):1117–1122. doi:10.1016/s0886-3350(00)00451-x
10. Chan CC, Sharma M, Wachler BS. Effect of inferior-segment Intacs with and without C3-R on keratoconus. J Cataract Refract Surg. 2007;33(1):75–80. doi:10.1016/j.jcrs.2006.09.012
11. El-Raggal TM. Sequential versus concurrent KERARINGS insertion and corneal collagen cross-linking for keratoconus. Br J Ophthalmol. 2011;95(1):37–41. doi:10.1136/bjo.2010.179580
12. Khan MI, Muhtaseb M. Intrastromal corneal ring segments for bilateral keratoconus in an 11-year-old boy. J Cataract Refract Surg. 2011;37(1):201–205. doi:10.1016/j.jcrs.2010.10.023
13. Abozaid MA. Sequential Keraring implantation and corneal cross-linking for the treatment of keratoconus in children with vernal keratoconjunctivitis. Clin Ophthalmol. 2017;24(11):1891–1895. doi:10.2147/OPTH.S150022
14. Abdelmassih Y, El-Khoury S, Dirani A, et al. Safety and efficacy of sequential intracorneal ring segment implantation and cross-linking in pediatric keratoconus. Am J Ophthalmol. 2017;178:51–57. doi:10.1016/j.ajo.2017.03.016
15. Olivo-Payne A, Serna-Ojeda JC, Hernandez-Bogantes E, et al. Trans-epithelial accelerated corneal cross-linking for keratoconus in children. Int J Ophthalmol. 2017;10(12):1919–1921. doi:10.18240/ijo.2017.12.20
16. Tian M, Jian W, Sun L, Shen Y, Zhang X, Zhou X. One-year follow-up of accelerated transepithelial corneal collagen cross-linking for progressive pediatric keratoconus. BMC Ophthalmol. 2018;18(1):75. doi:10.1186/s12886-018-0739-9
17. Sarac O, Caglayan M, Uysal BS, Uzel AGT, Tanriverdi B, Cagil N. Accelerated versus standard corneal collagen cross-linking in pediatric keratoconus patients: 24 months follow-up results. Cont Lens Anterior Eye. 2018;41(5):442–447. doi:10.1016/j.clae.2018.06.001
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.