Back to Journals » Drug Design, Development and Therapy » Volume 18
Intraoperative Use of Sodium Bicarbonate Ringer’s Solution Instead of Sodium Lactate Ringer’s Solution to Reduce Endothelial Glycocalyx Degradation and Improve Postoperative Recovery During Cardiopulmonary Bypass Cardiac Surgery: A Single-Center Prospective Cohort Study
Authors Shi Y, Shi Y, Tao Y, Xu B ![]() , Wang X, Xie Y, Zhang M
, Wang X, Xie Y, Zhang M
Received 19 October 2024
Accepted for publication 3 December 2024
Published 10 December 2024 Volume 2024:18 Pages 5881—5893
DOI https://doi.org/10.2147/DDDT.S501657
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Yujie Shi,1,* Yuan Shi,2,* Yujia Tao,1 Bingyan Xu,1 Xiaoming Wang,1 Yanhu Xie,1 Min Zhang1
1Department of Anesthesiology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230001, People’s Republic of China; 2Department of Anesthesiology, Wannan Medical College, Wuhu, Anhui, 241000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Min Zhang, Department of Anesthesiology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230001, People’s Republic of China, Tel +86 13866716646, Email [email protected]
Objective: To investigate the effect of sodium bicarbonate Ringer’s solution (BRS) on the degradation of endothelial glycocalyx components in patients undergoing cardiopulmonary bypass (CPB) during cardiac surgery, and to evaluate its impact on endothelial glycocalyx preservation and postoperative recovery.
Patients and Methods: A total of eight patients scheduled for elective CPB heart surgery were included and randomly divided into two groups: the sodium lactate Ringer’s solution (LRS) group and the BRS group. ELISA was used to measure plasma concentrations of syndecan-1, matrix metalloproteinase-9 (MMP-9), matrix metalloproteinase-3 (MMP-3), IL-6, IL-8, TNF-α, and TGF-β at predefined time points: T0 (before induction of anesthesia), T3 (immediately after weaning from CPB), T5 and T6 (24 and 72 hours postoperatively). Serum creatinine concentrations were measured within 48 hours postoperatively. The incidence of postoperative delirium (POD) was assessed three days after surgery. Postoperative mechanical ventilation time, duration of stay in the intensive care unit and hospital stay were also documented.
Results: The BRS group had significantly lower plasma concentrations of syndecan-1 at T3 (7.98 [7.43, 8.92] ng/mL vs 9.54 [8.4, 10.73] ng/mL, P < 0.001) and T5 (4.20 [3.31, 4.96] ng/mL vs 5.40 [3.95, 6.55] ng/mL, P = 0.001) in comparison with the LRS group (P< 0.01). Syndecan-1 levels in both groups were similar at T6 (3.18 [2.88, 3.5]ng/mL vs 3.12 [2.77, 3.45] ng/mL, P > 0.05). Additionally, MMP-9, MMP-3, IL-6 and IL-8 were significantly lower at T3 and T5 in the BRS group (P< 0.05 and P< 0.01, respectively). However, no significant differences were observed between the two groups in the incidence of acute kidney injury (AKI) or POD (P > 0.05).
Conclusion: BRS has the potential to reduce glycocalyx degradation in patients undergoing heart valve surgery with CPB. However, both groups demonstrated similar post-postoperative clinical outcomes, including the rates of AKI and POD.
Keywords: sodium bicarbonate Ringer’s solution, endothelial glycocalyx, cardiopulmonary bypass, postoperative recovery
Introduction
Cardiopulmonary bypass (CPB) cardiac surgery represents a cornerstone intervention in management of complex congenital and acquired cardiovascular disease. Advancements in CPB technology have significantly improved the feasibility of surgical interventions for these complex conditions. Despite the crucial role that CPB plays in cardiac surgery, its associated physiological impacts cannot be overlooked.1 These responses may amplify systemic inflammation and contribute to tissue damage, ultimately resulting in widespread endothelial injury and dysfunction.2,3 Cardiac surgical patients present unique challenges, particularly due to their reduced tolerance for intravascular volume changes and heightened susceptibility to hemodynamic fluctuations, necessitating a more rigorous approach to fluid management.4 Currently, crystalloids are extensively used during CPB in heart operation to maintain hemodynamic stability through fluid replacement. Various formulations, including balanced salt solutions and lactated Ringer’s solution, are employed to regulate acid-base status and electrolyte balance.5,6 The appropriate selection of crystalloid solutions can attenuate perioperative inflammatory responses, potentially improving patient outcomes.7 Nevertheless, the optimal choice and strategy for crystalloid administration remain subjects of ongoing clinical investigation to enhance therapeutic efficacy. Recently, sodium bicarbonate Ringer’s solution (BRS) has emerged as a promising alternative in cardiac surgery, owing to its potential benefits in mitigating acidosis, reducing inflammation, and minimizing oxidative stress.8
During cardiopulmonary bypass, mechanical damage, stress responses, and hemodynamic alterations can lead to various complications, including postoperative delirium (POD), systemic inflammatory response syndrome (SIRS), and acute kidney injury (AKI). Such complications not only impede recovery but may also exert a detrimental influence on long-term patient outcomes.9–11 Research indicates that the release of inflammatory mediators and endothelial cell injury during surgery can exert far-reaching effects, extending beyond the local site to impact cerebral endothelial cells via the bloodstream. This systemic involvement may contribute to neurofunctional disturbances, making it a key factor in the development of POD.12 The kidneys, as vital organs of blood filtration, experience endothelial damage due to postoperative systemic inflammation and hemodynamic changes. This damage leads to vasoconstriction and hypoxia, accelerating the progression of acute kidney injury (AKI).13 Endothelial cells regulate vascular tone, blood flow, and inflammation through the secretion of bioactive substances. Dysfunction of these cells is a key contributor to the development of these complications.14 The endothelial glycocalyx (EG) is a glycoprotein and proteoglycan complex that covers the surface of endothelial cells. It plays a crucial role in maintaining vascular permeability, protecting endothelial cells from mechanical injury, and regulating hemorheology.15 Composed of various glycosaminoglycans and membrane-bound proteoglycans, the glycocalyx includes syndecan-1 as a key component and a marker of glycocalyx degradation.16 During extracorporeal circulation, the glycocalyx is particularly vulnerable to damage. The degradation products released into the circulation can amplify inflammatory responses and contribute to further endothelial injury,17,18 which is closely linked to postoperative complications, negatively affecting recovery and long-term prognosis.
Thus, reducing EG degradation and minimizing postoperative complications remain critical clinical challenges in CPB heart surgery. Recent studies suggest that BRS not only assists in acid-base balance but may also provide endothelial protection by alleviating oxidative stress and inflammatory responses.19 This finding opens a new avenue for research into the use of BRS in cardiac surgery. However, clinical evidence regarding its protective effect on the EG remains limited, particularly concerning its specific impact on glycocalyx degradation products during cardiopulmonary bypass. Consequently, the aim of this study was to evaluate the effects of BRS on the EG integrity and its impact on postoperative recovery by comparing outcomes in patients receiving BRS with those receiving sodium lactate Ringer’s solution (LRS).
Materials and Methods
Study Groups
This prospective, randomized, double-blind, single-center clinical trial was approved by the Medical Ethics Committee of the First Affiliated Hospital of the University of Science and Technology of China (2022KY-312) and registered at ClinicalTrials.gov (ChiCTR2300067798). Written informed consent was obtained from all participants prior to enrollment. A total of 80 adult patients scheduled for elective cardiac valve operation with CPB between December 2023 and June 2024 were included. IBM SPSS Statistics 25 (IBM SPSS Inc., Chicago, USA) was used to generate a computer-based randomization sequence, through which participants were randomly allocated to one of two groups-BRS or LRS, with 40 patients in each group.
Inclusion criteria for the study were: age between 18 and 65 years, American Society of Anesthesiologists (ASA) physical status II–IV, and elective heart valve surgery with CPB under general anesthesia. Exclusion criteria included: patients requiring reoperation, those with pre-existing hepatic or renal dysfunction, patients undergoing deep hypothermic circulatory arrest, and individuals with a history of cognitive or psychiatric disorder. Prior to the induction of anesthesia, an individual not involved in the research prepared and provided the study infusion solutions to both the anesthetist and perfusionist.
Perioperative Management
Upon admission to the operating room, patients were monitored for oxygen saturation, electrocardiogram (ECG), invasive arterial pressure, central venous pressure, body temperature, and bispectral index (BIS, Covidien ltd, America). Anesthesia was induced with a single injection of sufentanil citrate 0.5 to 1 μg kg−1, and etomidate 0.3 mg kg−1 companied with rocuronium 0.6 mg kg−1. General anesthesia was maintained with a combination of intravenous and inhalational agents. During the procedure, propofol (4–6 mg·kg⁻¹·h⁻¹) and sufentanil (0.5–0.8 μg·kg⁻¹·h⁻¹) were administered continuously infused, while sevoflurane was administered at 0.8–1.0 minimum alveolar concentration (MAC). The BIS value was maintained between 40 to 60 throughout the procedure.
The extracorporeal circulation system consisted of a centrifugal pump, temperature and humidity controller, and oxygenator (CAPIOX® FX, Terumo, Tokyo, Japan), supplemented by a disposable blood microparticle filter (MicroPort, Guangdong, China). Anticoagulation was achieved with heparin at a dose of 300 IU/kg, and extracorporeal circulation was initiated once the activated clotting time (ACT) exceeded 480 seconds, with additional doses of heparin administered as needed. During the procedure, intermittent infusion of high-potassium cold cardioplegia (Bretschneider HTK) were administered via the aortic root. After weaning from CPB, protamine was given at a 1:1 ratio to neutralize the anticoagulant effects of heparin. Residual fluid from both the intrathoracic and extracorporeal circuits was collected, washed, and reinfused into the patient using C.A.T.S autologous blood recovery machine (Fresenius Kabi AG, Bad Homburg, Germany). Postoperatively, patients remained intubated and were transferred to the intensive care unit (ICU).
Fluid Management
Following the induction of anesthesia, patients were administered an intravenous infusion of either BRS (H20190021, Hengrui Pharmaceuticals Co. Ltd. Jiangsu, China) or LRS (H20057107, Cisen Pharmaceutical Ltd. Shandong, China) crystalloids. The use of colloids was left to the discretion of the attending anesthetist. After the priming and pressure measurement of the CPB, a portion of crystalloid solutions was filtered through a microsphere filter, with additional crystalloids administered as deemed necessary. Both groups were preloaded with 1000 mL of succinylated gelatin (H20113119, B.Braun, Sunzhou, China), followed by a preload of 500–1000 mL of crystalloid solution. During CPB, the perfusionist adjusted the rate of crystalloid infusion as clinically indicated. A non-pulsatile pump flow was maintained between 2.2 L min−1 m−2 and 2.6 L min−1 m−2, with temperature regulated between 34°C and 36°C. Norepinephrine was administered to maintain mean arterial pressure (MAP) within the target range of 60–75 mmHg, and any acid-base imbalances were corrected based on arterial blood gas analysis. Following the termination of extracorporeal circulation, intravenous infusions of crystalloids or colloids were resumed to ensure the maintenance of a mean arterial pressure (MAP) of at least 60 mmHg, a central venous pressure (CVP) of 5–12 cmH2O, and a hemoglobin concentration above 8 g/dL.
ELISA Sample Collection
Blood samples were collected from the central venous catheter at four predefined time points: T0 (before induction of anesthesia), T3 (immediately following weaning from CPB), T5 (24 hours postoperatively) and T6 (72 hours postoperatively). Samples were collected into 5 mL tubes containing EDTA for anticoagulation. After collection, the samples were centrifuged at 1000g for 10 minutes at 4°C. The plasma supernatants were aliquoted into Eppendorf tubes and stored at −80°C. Enzyme-linked immunosorbent assay (ELISA) was used to measure the plasma concentrations of syndecan-1 (Cat. No. MM-12530H1, MEIMIAN Group, Jiangsu, China), matrix metalloproteinase-9 (MMP-9, Cat. No. MM-0149H1, MEIMIAN Group, Jiangsu, China), matrix metalloproteinase-3 (MMP-3, Cat. No. MM-0108H1, MEIMIAN Group, Jiangsu, China), as well as the inflammatory biomarkers interleukin- 6 (IL-6, Cat. No. MM-0049H1, MEIMIAN Group, Jiangsu, China), IL-8 (Cat. No. MM-1558H1, MEIMIAN Group, Jiangsu, China), tumor necrosis factor-α (TNF-α, Cat. No. KE00367, ProteinTech Group, Wuhan, China) and transforming growth factor-β (TGF-β, Cat. No. MM-63141H1, MEIMIAN Group, Jiangsu, China). All assays were performed according to the manufacturers’ protocols. Standards and samples were loaded onto 96-well plates pre-coated with capture antibodies and incubated at room temperature. Absorbance was recorded at 450 nm using a Varioskan ALF Multimode Microplate Reader (Thermo Fisher Scientific, Waltham, USA) and sample concentrations were calculated using a standard curve. All measurements were conducted in duplicate.
Blood Gas Analyzer
Arterial blood samples were collected at seven specified time points for blood gas analysis: T0, T1 (immediately at the initiation of CPB), T2 (60 minutes after CPB initiation or just before weaning), T3, T4 (6 hours postoperatively), T5, and T6. Blood gas analysis was conducted using the ABL90 FLEX analyzer (Radiometer Medical ApS, Brøndby, Denmark), which processes each sample within 35 seconds to ensure rapid and reliable results. The same instrument was consistently used for the blood gas analysis of all patients to ensure uniformity and comparability across measurements. At each time point, the parameters were measured included pH, bicarbonate (HCO3⁻), base excess (BE), lactate, and electrolytes such as potassium, calcium, sodium, and chloride. These measurements provided a comprehensive assessment of acid-base status and electrolyte balance. The volume of solution was recorded which included pre-CPB, priming volume and post-CPB administration.
Postoperative Observation Metrics
Acute kidney injury (AKI) was defined based on the 2012 KDIGO criteria as an increase in serum creatinine (Cr) of ≥ 26.5 μmol/L within 48 hours postoperatively.20 Then, serum creatinine concentrations were measured preoperatively and reassessed in the first 48 hours following surgery. Delirium incidence was assessed using the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) and the CAM-Mixed Scale during postoperative days 1, 2, and 3. Additionally, the duration of mechanical ventilation, length of day in the intensive care unit (ICU) and hospital were documented.
Sample Size
In this research, Syndecan-1, a metabolite of the EG, was utilized as the primary indicator. Previous research has demonstrated that its concentration approximately doubles before and after cardiopulmonary bypass. A comparison between two independent groups was planned with an overall α level of 0.05 and a statistical power of 80%. The sample size was calculated using the formula: n = (1.6449+1.2816)2·22/12≈34.3. Considering a dropout rate of 10%, a sample size of 40 participants per group was selected.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics 25. Continuous variables with a normal distribution were presented as mean and standard deviation, while non-normally distributed data were presented as median and interquartile range. Categorical data were expressed as counts (percentages). The comparisons of numerical data between groups were conducted using either Student’s t-test or Mann–Whitney U-test, at stake. For categorical variables, chi-square tests or Fisher’s exact tests were used. Time-dependent changes between groups were analyzed using repeated measures analysis of variance. Spearman’s test was performed to analyze the correlation between syndecan-1 and enzymes and inflammatory biomarkers. P less than 0.05 was considered statistically significant.
Results
A total of 80 patients scheduled for elective CPB without pre-existing mental disorders were enrolled and randomly assigned to two groups. In the LRS group, one patient required reoperation on the day of the surgery, and another patient was withdrawn from the study due to a major aortic root hemorrhage during surgery. Consequently, the final analysis included 78 patients (Figure 1). No statistically significant differences were observed between the two groups in terms of age, BMI, ASA classification, preoperative comorbidities, or type of surgery (P > 0.05, Table 1).
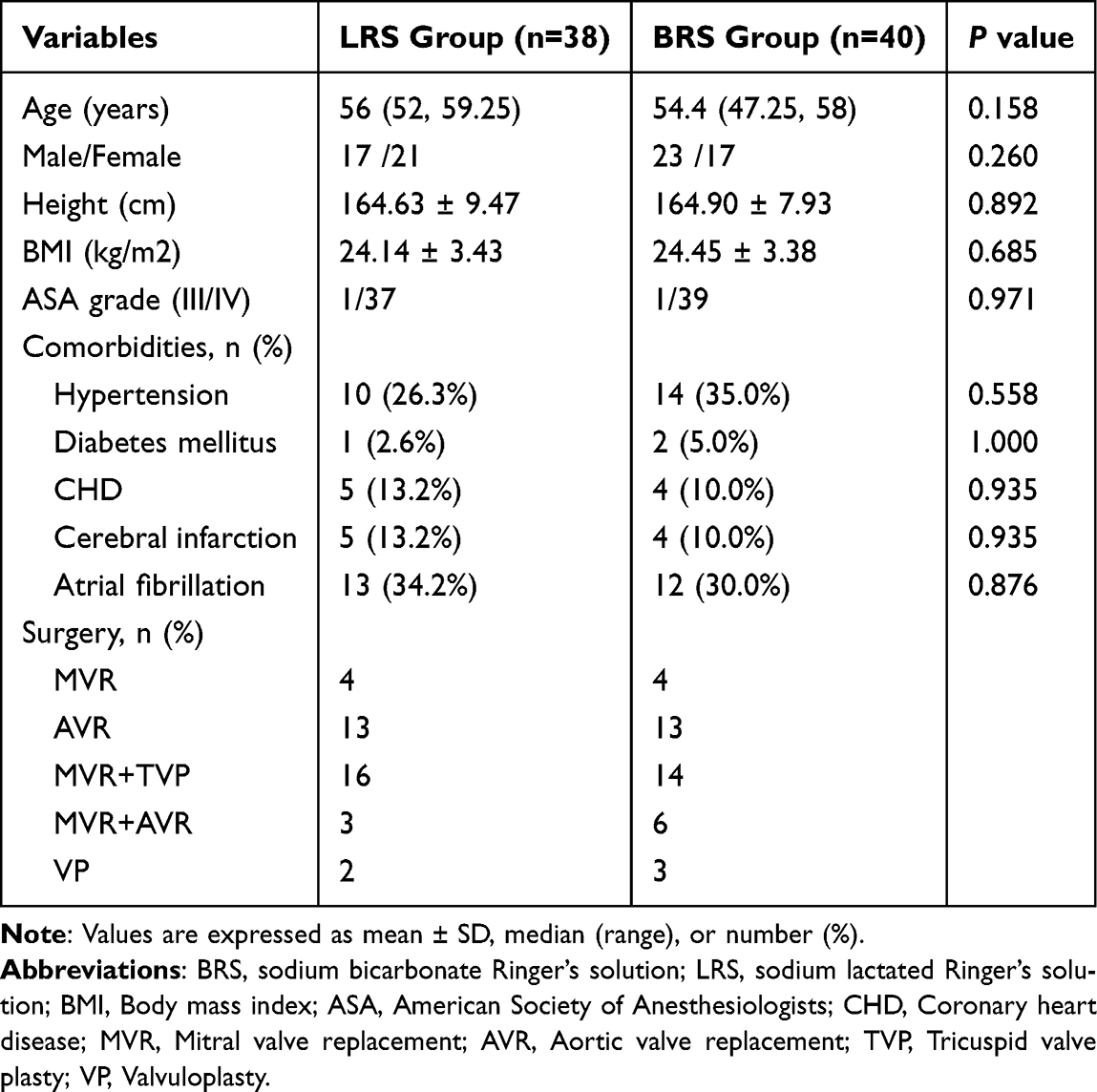 |
Table 1 Patients Baseline Characteristics |
 |
Figure 1 Participants flow diagram. Abbreviations: BRS, sodium bicarbonate Ringer’s solution; LRS, sodium lactated Ringer’s solution. |
The duration of CPB was comparable between the two groups (121.33 ± 43.32 min vs 126.95 ± 38.05 min, P > 0.05), as was the duration of anesthesia (338.88 ± 63.47 min vs 338.26 ± 70.05 min, P > 0.05). No significant differences were observed in the use of vasopressors to maintain hemodynamic stability and support left ventricular function post-CPB between the two groups (P > 0.05). To manage acid-base balance, 5% sodium bicarbonate injection was administered intraoperatively. The volume of 5% sodium bicarbonate injection used was significantly lower in the BRS group compared to the LRS group (100 [50, 123.75] mL vs 150 [100, 200] mL, P < 0.001). However, no significant differences were observed between the two groups in the volume of crystalloids, colloids, red blood cells, fresh frozen plasma, or autologous blood administered during the procedure (P > 0.05, Table 2).
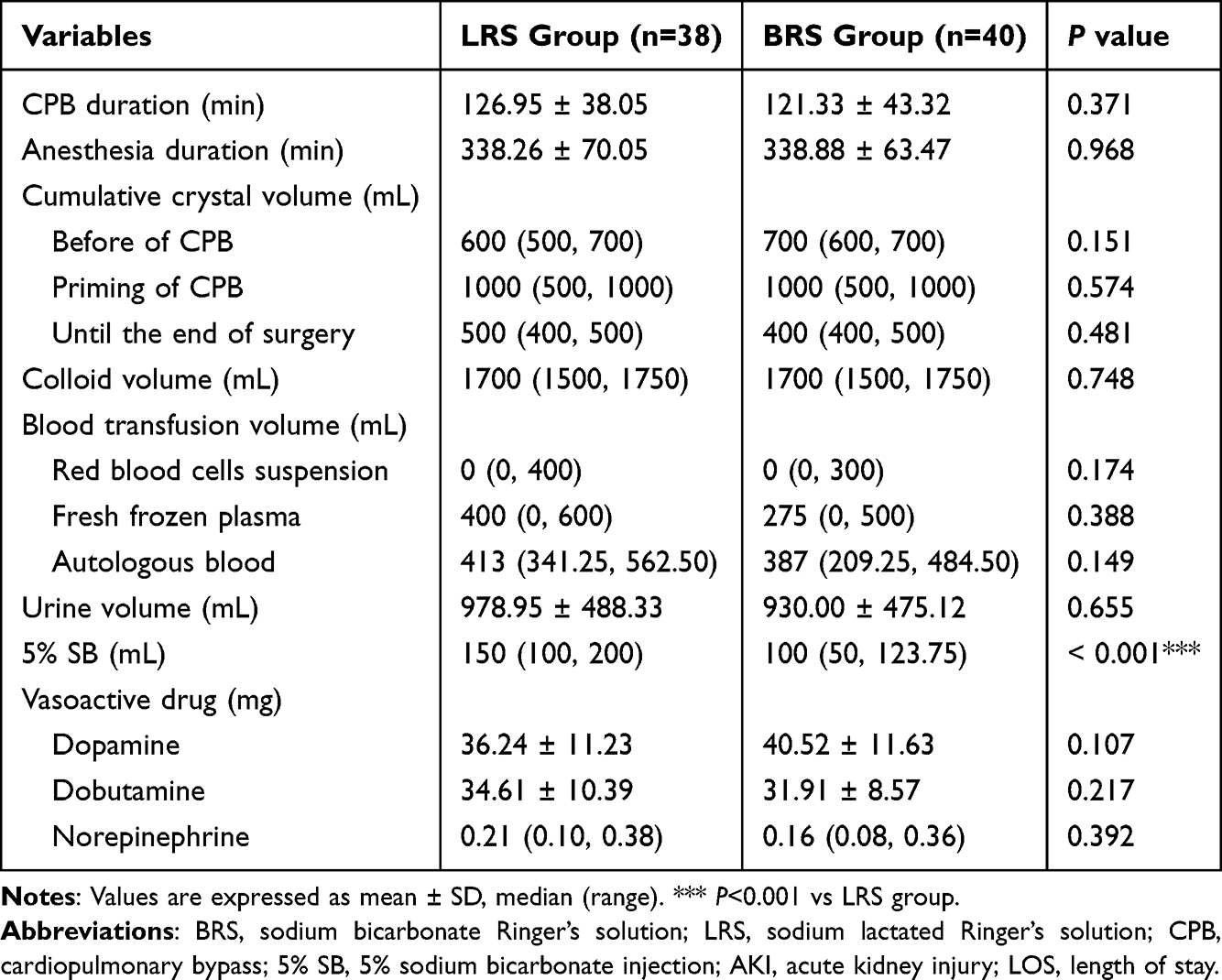 |
Table 2 Perioperative Profiles of the Patients |
Plasma Endothelial Glycocalyx and Other Indicators
At baseline (T0), no statistically significant differences were found in plasma concentrations of syndecan-1, matrix metalloproteinase-9 (MMP-9), or matrix metalloproteinase-3 (MMP-3) between the two groups (P > 0.05). Over time, both groups exhibited similar trends in these markers. At T3, plasma syndecan-1 levels markedly increased in both groups. However, the BRS group demonstrated lower levels compared with the LRS group (7.98 [7.43, 8.92] ng/mL vs 9.54 [8.4, 10.73] ng/mL, P < 0.001). At T5, syndecan-1 concentrations in both groups had decreased relative to T3, but the BRS group continued to exhibit lower levels compared to the LRS group (4.20 [3.31,4.96] ng/mL vs 5.40 [3.95, 6.55] ng/mL, P = 0.001; Figure 2A). Plasma MMP-9 levels in both groups notably increased at T3, with the BRS group exhibiting lower levels than the LRS group (2164.24 [2032.03, 2293.48] μg/L vs 2575.66 [2357.56, 2858.05] μg/L, P < 0.001). At T5, MMP-9 levels in the BRS group remained lower than in the LRS group (1345.03 [1068.16, 1533.81] μg/L vs 1527.08 [1240.69, 2117.14] μg/L, P = 0.005; Figure 2B). Similarly, MMP-3 concentration showed significant increases at both T3 and T5 in both groups; however, the BRS group exhibited lower levels in relation to the LRS group (166.57 [158.73, 175.68] μg/L vs 173.31 [166.70, 189.27] μg/L, P= 0.006; 121.53 [112.18, 128.39] μg/L vs 127.29 [117.05, 137.74] μg/L, P = 0.013; Figure 2C).
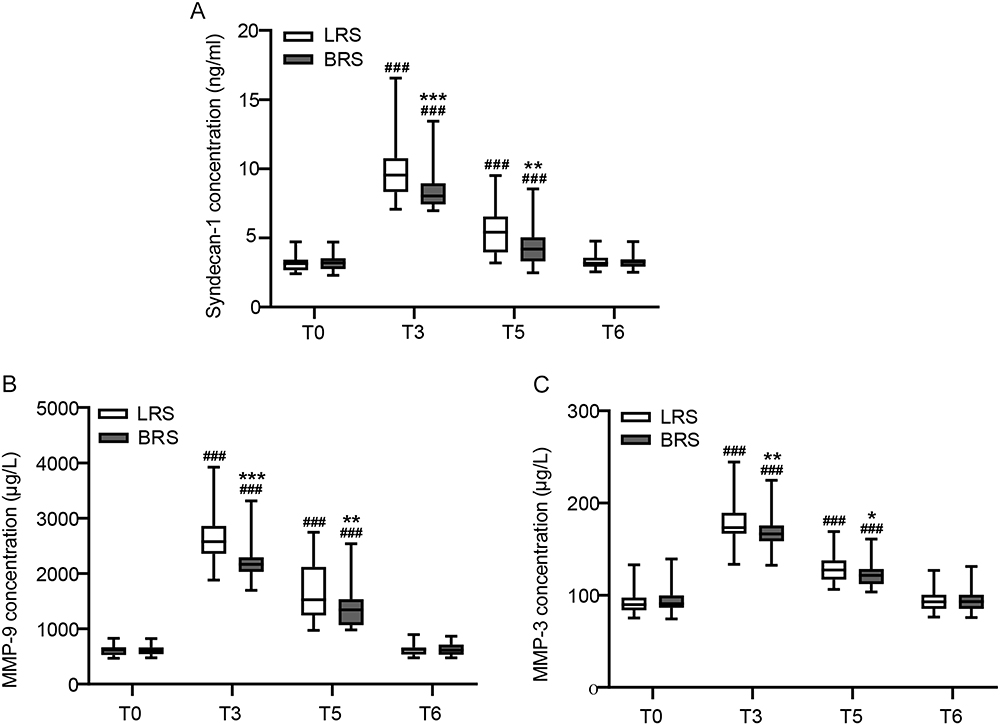 |
Figure 2 Plasma concentration of syndecan-1, MMP-9 and MMP-3 in the BRS and LRS groups. Abbreviations: MMP-9, matrix metalloproteinase-9; MMP-3, matrix metalloproteinase-3; BRS, sodium bicarbonate Ringer’s solution; LRS, sodium lactated Ringer’s solution; T0, before anesthetic induction; T3, immediately after weaning from CPB; T5, 24h postoperatively; T6, 72h postoperatively. Note: (A) Syndecan-1 concentration in both groups; (B) MMP-9 concentration in both groups; (C) MMP-3 concentration in both groups. The other groups vs T0 group (###P<0.001); at the same time point, BRS group vs LRS group (*P<0.05, **P<0.01, ***P<0.001). |
Inflammatory Markers
Baseline levels and perioperative changes in inflammatory markers were illustrated in Figure 2. At T3, the pro-inflammatory cytokines IL-6 and IL-8 reached their peak concentrations in both groups (P < 0.01). The increases in IL-6 and IL-8 were less pronounced in the BRS group compared to the LRS group (IL-6: 40.31 [37.41, 47.68] pg/mL vs 49.98 [43.21, 54.61] pg/mL, P = 0.002; IL-8: 497.24 [433.89, 541.32] pg/mL vs 544.98 [494.86, 576.32] pg/mL, P = 0.005). At T5, inflammatory markers followed a similar pattern in both groups (IL-6: 29.15 [25.56, 33.11] pg/mL vs 35.40 [27.02, 40.81] pg/mL, P = 0.009; IL-8: 393.94 [342.88, 416.10] pg/mL vs 423.05 [375.36, 467.07] pg/mL, P = 0.011; Figure 3A and B). At T3 and T5, TNF-α levels were significantly elevated in both groups compared to preoperative levels; however, no statistically significant differences were detected between the groups (P > 0.05, Figure 3C). Similarly, TGF-β levels were significantly reduced at T3 and T5 relative to T0 in both groups, with no significant intergroup differences observed (P > 0.05, Figure 3D). Changes in plasma SDC-1 concentrations were positively correlated with the levels of matrix metalloproteinases MMP-9 and MMP-3, as well as the inflammatory markers IL-6 and IL-8, while exhibiting a negative correlation with TGF-β levels (Figure 4).
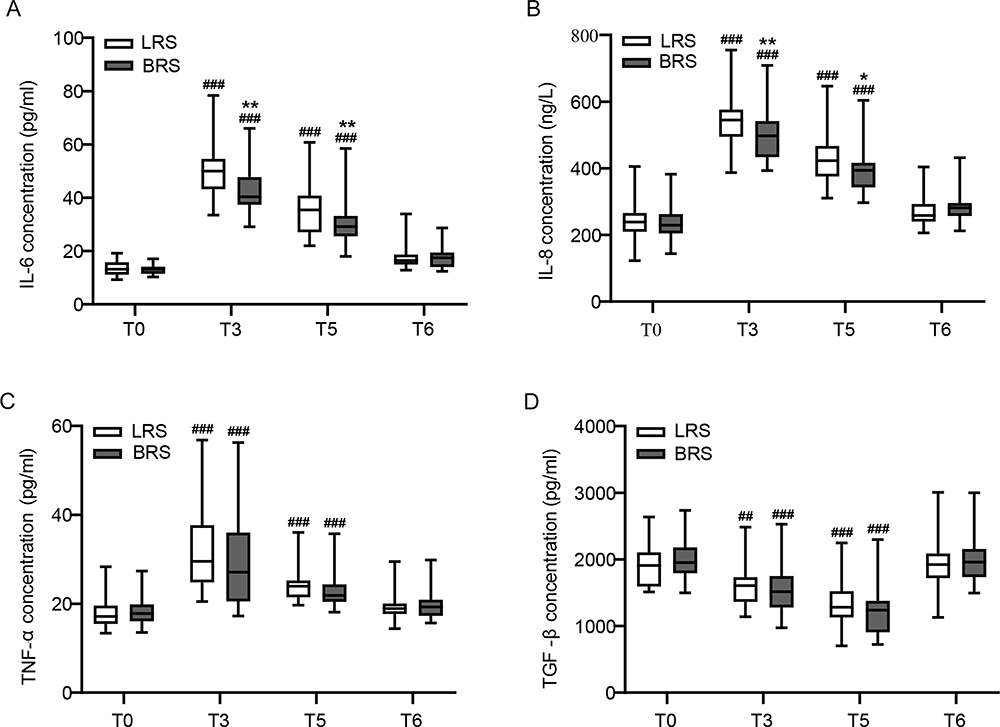 |
Figure 3 Perioperative levels of inflammatory markers in the BRS and LRS groups. Abbreviations: IL-6, interleukin-6; IL-8, interleukin-8; TNF-α, tumor necrosis factor-α; TGF-β, transforming growth factor-β; BRS, sodium bicarbonate Ringer’s solution; LRS, sodium lactated Ringer’s solution; T0, before anesthetic induction; T3, immediately after weaning from CPB; T5, 24h postoperatively; T6, 72h postoperatively. Note: (A) IL-6 concentration in both group; (B) IL-8 concentration in both group; (C) TNF-α concentration in both group; (D) TGF-β concentration in both group; The other groups vs T0 group (##P<0.01, ###P<0.001); at the same time point, BRS group vs LRS group (*P<0.05, **P<0.01). |
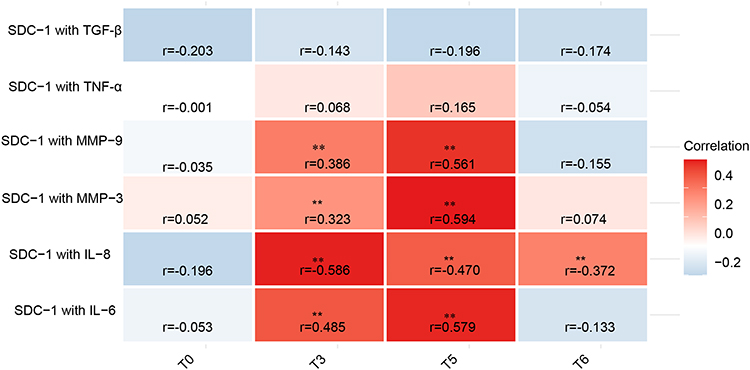 |
Figure 4 A series of correlation analyses of glycocalyx marker associated with matrix metalloproteinases or inflammatory factors. *P<0.05, **P<0.01. Abbreviations: SDC-1, syndecan-1; MMP-9, matrix metalloproteinase-9; MMP-3, matrix metalloproteinase-3; IL-6, interleukin-6; IL-8, interleukin-8; TNF-α, tumor necrosis factor-α; TGF-β, transforming growth factor-β; T0, before anesthetic induction; T3, immediately after weaning from CPB; T5, 24h postoperatively; T6, 72h postoperatively. |
Blood Gas Analysis
At the preoperative baseline (T0), blood gas parameters, including pH, base excess (BE), bicarbonate (HCO3⁻), potassium (K+), calcium (Ca2+), and lactate levels, were comparable between the two groups. During the progression of surgery, no significant differences were observed between the groups in pH, potassium, or calcium concentrations (P > 0.05). However, changes in BE and HCO3⁻ levels were noted, with fluctuations in the BRS group being significantly less pronounced than in the LRS group during the initiation of CPB. Lactate levels began to rise at T2 and peaked at T4 (P < 0.01), with the increase in lactate concentration being lower in the BRS group than in the LRS group (P < 0.05) (Table 3).
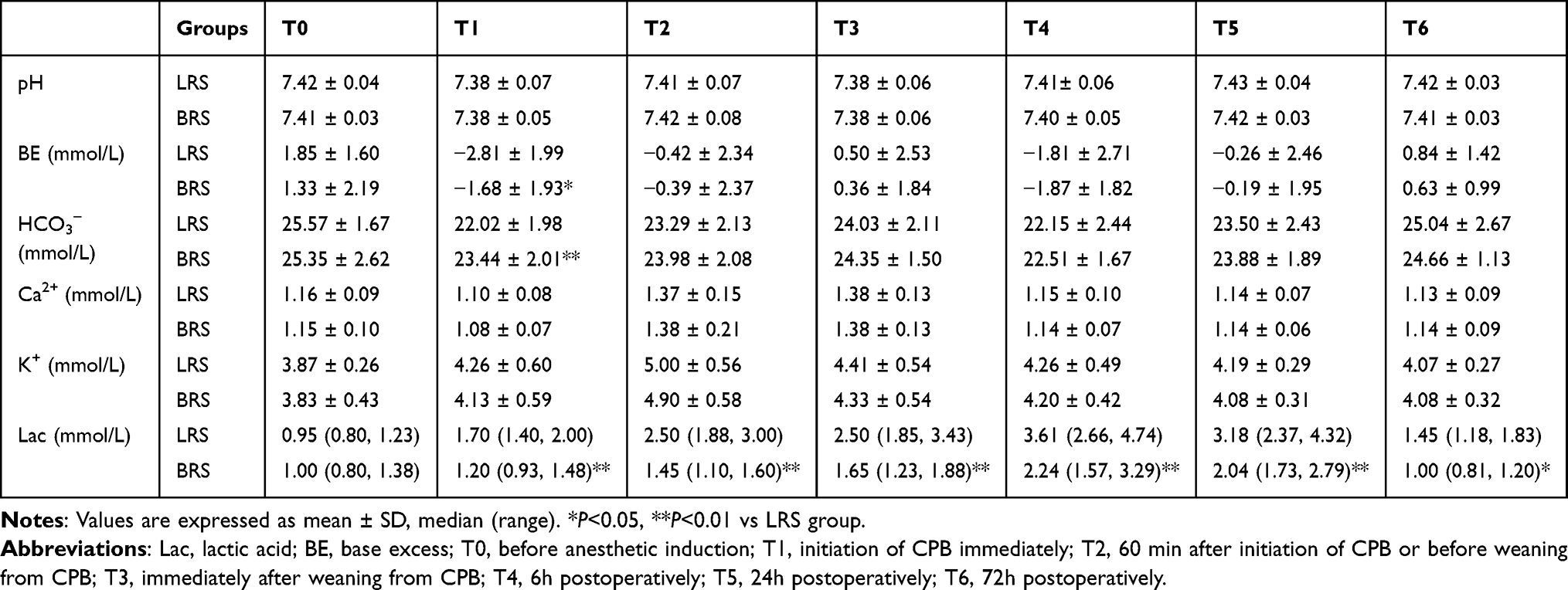 |
Table 3 Perioperative Arterial Blood Gas Analysis |
Postoperative Observation Indicators
The incidence of acute kidney injury (AKI) was monitored in both groups. The results demonstrated that the incidence of AKI was lower in the BRS group relative to the LRS group, but the difference did not reach statistical significance (7 [17.5%] vs 14 [36.8%], P = 0.095). Although the BRS group had a lower incidence of postoperative delirium (POD) during the first three postoperative days compared to the LRS group, this difference was not statistically significant (P > 0.05). Additionally, there were no significant differences between the two groups regarding the duration of mechanical ventilation, length of ICU or hospital (P > 0.05, Table 4).
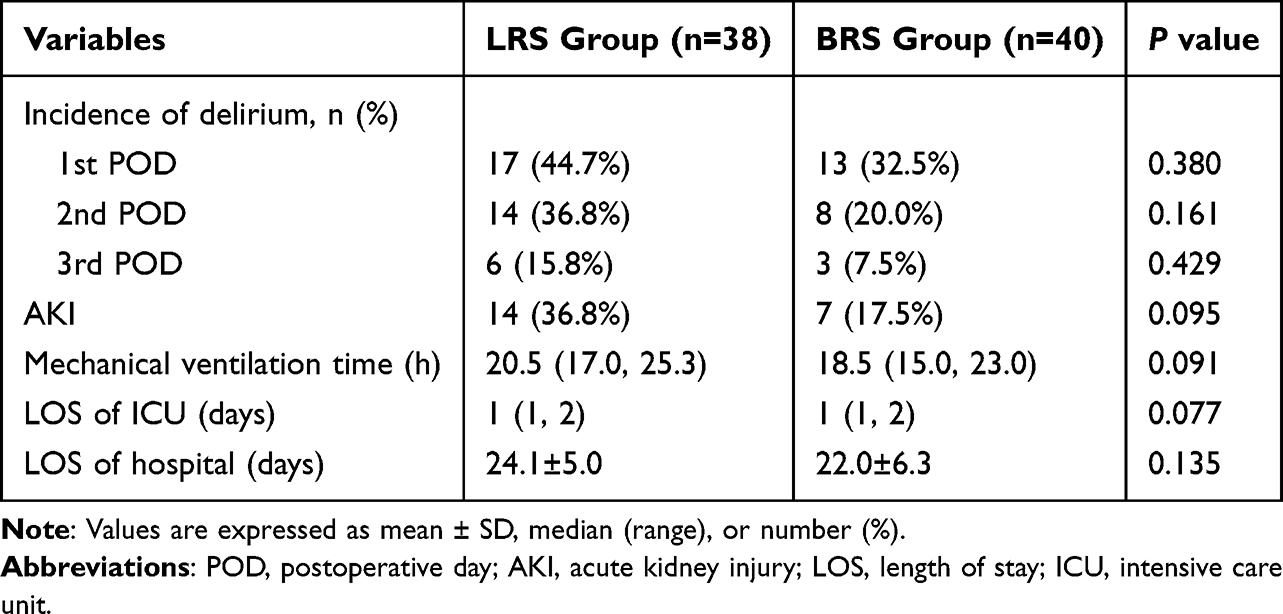 |
Table 4 Postoperative Parameters |
Discussion
This study aimed to investigate the impact of BRS on EG degradation products, postoperative inflammatory markers, and clinical outcomes in patients undergoing cardiac surgery. We analyzed the changes in the levels of syndecan-1, matrix metalloproteinases MMP-9 and MMP-3, along with inflammatory cytokines including cytokines IL-6, IL-8, TNF-α, and TGF-β. Additionally, arterial blood gas and key postoperative outcomes parameters were recorded recovery. The primary finding of the study was a significant reduction in plasma syndecan-1 levels in the BRS group. However, both groups demonstrated comparable postoperative recovery metrics, including the incidence of AKI and POD.
The endothelial glycocalyx, a crucial protective barrier of endothelial cells, plays an essential role in maintaining vascular function and stability.21 Evidence suggests that CPB induces an inflammatory response, oxidative stress, and ischemia-reperfusion injury, all of which contribute to the degradation of the glycocalyx. Syndecan-1, a principal protein component of the glycocalyx, is used as a biomarker indicative of the extent of glycocalyx damage.22 Glycocalyx degradation has been documented in patients with sepsis and critical illness, with elevated levels of glycocalyx biomarkers in the blood correlating with adverse clinical outcomes.23,24 Previous studies have demonstrated that plasma syndecan-1 concentrations exhibit a highly dynamic temporal pattern, with a notable increase during CPB cardiac surgery.25 Our investigation revealed a significant rise in plasma syndecan-1 levels after weaning from of CPB. Notably, patients administered BRS exhibited lower plasma syndecan-1 levels than those receiving LRS, with this difference persisted through the first postoperative day. The solution’s ability to reduce glycocalyx damage may be attributed to its role in neutralizing acidosis, particularly in cases of traumatic shock, where it has been shown to be more effective than LRS.26 Sheng et al demonstrated that treatment with BRS better preserved glycocalyx integrity and induced a less pronounced inflammatory response compared to lactated Ringer’s solution.27 Wu et al confirmed that in liver transplantation, the use of sodium bicarbonate Ringer’s solution reduced microcirculatory kidney injury and lowered the risk of increased vascular permeability.28 Our findings aligned with these studies, supporting the hypothesis that BRS may protected endothelial cells by mitigating acidosis and reducing inflammatory responses.
Matrix metalloproteinases (MMPs) such as MMP-9 and MMP-3 are pivotal in the degradation of the EG by cleaving its protein components, which accelerates its destruction.29,30 Furthermore, endotoxin-induced acute respiratory distress syndrome (ARDS) has been associated with elevated MMP-9 levels, accelerating glycocalyx degradation.31–33 Our study found that patients administered BRS group exhibited significantly lower concentrations of MMP-9 and MMP-3. This observation further supported the potential protective effect of BRS in reducing glycocalyx damage. Inflammatory cytokines are crucial in the systemic inflammatory response triggered by CPB.34 Previous studies have demonstrated that plasma levels of IL-6 and IL-8 can be used to evaluate the severity of systemic inflammatory response syndrome (SIRS) following coronary artery bypass grafting (CABG) and serve as prognostic indicators.35 Within this research, the concentrations of IL-6 and IL-8 were significantly lower in the BRS group than the LRS group, suggesting that BRS may effectively suppress the inflammatory response by reducing the release of these key cytokines. Conversely, no significant differences were observed in the levels of the anti-inflammatory factor TGF-β between the two groups. Pesonen et al previously reported a correlation between perioperative changes in syndecan-1 levels and the expression of pro-inflammatory cytokines in patients undergoing CPB heart surgery.36 In this research, we observed that syndecan-1 concentrations at T3 and T5 were positively correlated with levels of MMP-9, MMP-3, and the inflammatory cytokines IL-6 and IL-8. These findings indicated that BRS may influence the inflammatory response and tissue remodeling processes by modulating syndecan-1 levels. This modulation could impact the underlying pathophysiological mechanisms associated with glycocalyx degradation and inflammation.
Elevated lactate levels after cardiac surgery indicate poor tissue perfusion and multi-organ dysfunction, particularly in the myocardium and kidneys.37,38 BRS group patients showed smaller fluctuations and lower levels than LRS group. Following cardiac surgery, acute kidney injury (AKI) is associated with electrolyte imbalances and an increased risk of postoperative infections.39,40 Previous research has indicated that BRS can reduce the incidence of kidney injury in critically ill patients.41 In this study, although the incidence of AKI was lower in the BRS group than in the LRS group, the difference did not achieve statistical significance, likely due to the limited sample size. POD is a well-recognized complication of cardiopulmonary bypass (CPB) surgery.42 Vascular injury, a key risk factor for POD, highlights the critical role of vascular and endothelial integrity in its development.43 In this study, no significant differences were observed between the two groups in terms of POD incidence, mechanical ventilation duration, or length of ICU and hospital stays.
Limitations
This study had several limitations. First, endothelial glycocalyx (EG) degradation was assessed solely through the measurement of plasma syndecan-1, a component shed from the EG However, syndecan-1 is not specific to endothelial cells, and its plasma concentration does not provide a direct measure of the structural or functional integrity of the EG Furthermore, direct visualization techniques, such as intravital microscopy, are not practical in a clinical setting. Nonetheless, syndecan-1 has been shown to correlate well with EG thickness in experimental models.44 Second, the sample size was calculated based on syndecan-1 concentrations. However, the sample size may have been insufficient to adequately assess prognostic outcomes.
Conclusion
This study suggests that BRS may mitigate endothelial glycocalyx degradation and suppress pro-inflammatory cytokines release during CPB in cardiac surgery. However, the two groups exhibited comparable postoperative recovery outcomes, including the incidence of AKI and POD.
Data Sharing Statement
The novel contributions of this study are thoroughly elaborated within the article. For further information or specific inquiries, please direct your correspondence to the corresponding author.
Ethical Statements
Our study was approved by the Medical Ethics Committee of the First Affiliated Hospital of the University of Science and Technology of China (2022KY-312). This study was conducted in accordance with the “Ethical Principles for Medical Research Involving Human Subjects” outlined in the Declaration of Helsinki by the World Medical Association.
Funding
This project is supported by the clinical special funding project of the China Primary Health Care Foundation (No: YLGX-MZ-2022005).
Disclosure
Yujie Shi and Yuan Shi are co-first authors. The authors state that there are no conflicts of interest associated with this work.
References
1. Bartoszko J, Karkouti K. Managing the coagulopathy associated with cardiopulmonary bypass. J Thromb Haemost. 2021;19(3):617–632. doi:10.1111/jth.15195
2. Do-Nguyen CC, Sturmer DL, Yang G, et al. Oxygen delivery thresholds during cardiopulmonary bypass and risk for acute kidney injury. Ann Thorac Surg. 2023;116(3):607–613. doi:10.1016/j.athoracsur.2023.04.049
3. Bangalore H, Carter MJ, Parmar K, et al. Degradation of the endothelial glycocalyx contributes to metabolic acidosis in children following cardiopulmonary bypass surgery. Pediatr Crit Care Med. 2021;22(11):e571–e581. doi:10.1097/PCC.0000000000002746
4. Xian-Yu CY, Xu JB, Ma YT, et al. Management of priming fluids in cardiopulmonary bypass for adult cardiac surgery: network meta-analysis. Ann Med. 2023;55(2):2246996. doi:10.1080/07853890.2023.2246996
5. Nam JS, Kim WJ, Seo WW, et al. Effects of balanced versus saline-based solutions on acute kidney injury in off-pump coronary artery bypass surgery: a randomized controlled trial. J Cardiothorac Vasc Anesth. 2024;38(9):1923–1931. doi:10.1053/j.jvca.2024.06.001
6. Vlasov H, Wilkman E, Petäjä L, et al. Comparison of 4% albumin and Ringer’s acetate on hemodynamics in on-pump cardiac surgery: an exploratory analysis of a randomized clinical trial. J Cardiothorac Vasc Anesth. 2024. doi:10.1053/j.jvca.2024.07.025
7. Collins MG, Fahim MA, Pascoe EM, et al. Balanced crystalloid solution versus saline in deceased donor kidney transplantation (BEST-Fluids): a pragmatic, double-blind, randomised, controlled trial. Lancet. 2023;402(10396):105–117. doi:10.1016/S0140-6736(23)00642-6
8. Shafique MA, Shaikh NA, Haseeb A, et al. Sodium bicarbonate Ringer’s solution for hemorrhagic shock: a meta-analysis comparing crystalloid solutions. Am J Emerg Med. 2024;76:41–47. doi:10.1016/j.ajem.2023.11.003
9. Cai S, Li J, Gao J, et al. Prediction models for postoperative delirium after cardiac surgery: systematic review and critical appraisal. Int J Nurs Stud. 2022;136:104340. doi:10.1016/j.ijnurstu.2022.104340
10. Milam AJ, Liang C, Mi J, et al. Derivation and validation of clinical phenotypes of the cardiopulmonary bypass-induced inflammatory response. Anesth Analg. 2023;136(3):507–517. doi:10.1213/ANE.0000000000006247
11. Menzenbach J, Frede S, Petras J, et al. Perioperative vascular biomarker profiling in elective surgery patients developing postoperative delirium: a prospective cohort study. Biomedicines. 2021;9(5):553. doi:10.3390/biomedicines9050553
12. Thudium M, Ellerkmann RK, Heinze I, et al. Relative cerebral hyperperfusion during cardiopulmonary bypass is associated with risk for postoperative delirium: a cross-sectional cohort study. BMC Anesthesiol. 2019;19(1):35. doi:10.1186/s12871-019-0705-y
13. Turgut F, Awad AS, Abdel-Rahman EM. Acute kidney injury: medical causes and pathogenesis. J Clin Med. 2023;12(1):375. doi:10.3390/jcm12010375
14. Foote CA, Soares RN, Ramirez-Perez FI, et al. Endothelial glycocalyx. Compr Physiol. 2022;12(4):3781–3811. doi:10.1002/cphy.c210029
15. Piotti A, Novelli D, Meessen J, et al. Endothelial damage in septic shock patients as evidenced by circulating syndecan-1, sphingosine-1-phosphate and soluble VE-cadherin: a substudy of ALBIOS. Crit Care. 2021;25(1):113. doi:10.1186/s13054-021-03545-1
16. Kusuzawa K, Suzuki K, Okada H, et al. Measuring the concentration of serum syndecan-1 to assess vascular endothelial glycocalyx injury during hemodialysis. Front Med. 2021;8:791309. doi:10.3389/fmed.2021.791309
17. Jufar AH, Lankadeva YR, May CN, et al. Renal and cerebral hypoxia and inflammation during cardiopulmonary bypass. Compr Physiol. 2021;12(1):2799–2834. doi:10.1002/cphy.c210019
18. Huang X, Hu H, Sun T, et al. Plasma endothelial glycocalyx components as a potential biomarker for predicting the development of disseminated intravascular coagulation in patients with sepsis. J Intensive Care Med. 2021;36(11):1286–1295. doi:10.1177/0885066620949131
19. Zhang J, Han D, Zhang K, et al. Observation on the effectiveness and safety of sodium bicarbonate Ringer’s solution in the early resuscitation of traumatic hemorrhagic shock: a clinical single-center prospective randomized controlled trial. Trials. 2022;23(1):825. doi:10.1186/s13063-022-06752-5
20. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4):c179–c184. doi:10.1159/000339789
21. Hamrangsekachaee M, Wen K, Yazdani N, et al. Endothelial glycocalyx sensitivity to chemical and mechanical sub-endothelial substrate properties. Front Bioeng Biotechnol. 2023;11:1250348. doi:10.3389/fbioe.2023.1250348
22. Fei Y, Huang X, Ning F, et al. NETs induce ferroptosis of endothelial cells in LPS-ALI through SDC-1/HS and downstream pathways. Biomed Pharmacother. 2024;175:116621. doi:10.1016/j.biopha.2024.116621
23. Qiao X, Kashiouris MG, L’Heureux M, et al. Biological effects of intravenous vitamin C on neutrophil extracellular traps and the endothelial glycocalyx in patients with sepsis-induced ARDS. Nutrients. 2022;14(20):4415. doi:10.3390/nu14204415
24. Kim HB, Soh S, Kwak YL, et al. High preoperative serum syndecan-1, a marker of endothelial glycocalyx degradation, and severe acute kidney injury after valvular heart surgery. J Clin Med. 2020;9(6). doi:10.3390/jcm9061803
25. Passov A, Schramko A, Salminen US, et al. Endothelial glycocalyx during early reperfusion in patients undergoing cardiac surgery. PLoS One. 2021;16(5):0251747. doi:10.1371/journal.pone.0251747
26. Han SJ, Zhou ZW, Yang C, et al. Hemorrhagic, hypovolemic shock resuscitated with Ringer’s solution using bicarbonate versus lactate: a CONSORT-randomized controlled study comparing patient outcomes and blood inflammatory factors. Medicine. 2022;101(46):e31671. doi:10.1097/MD.0000000000031671
27. Xu S, Qiu Z, Zheng C, et al. Effect of miR-21-3p on lung injury in rats with traumatic hemorrhagic shock resuscitated with sodium bicarbonate Ringer’s solution. Ann Transl Med. 2022;10(24):1331. doi:10.21037/atm-22-5148
28. Wu H, Meng G, Zuo C, et al. The effects of sodium bicarbonate Ringer’s solution on acute kidney injury and the clinical outcomes after liver transplantation: a randomized controlled trial. Front Pharmacol. 2022;13:982472. doi:10.3389/fphar.2022.982472
29. Xue Y, Liu W, Su L, et al. Quantitative electroencephalography predicts postoperative delirium in cardiac surgical patients after cardiopulmonary bypass: a prospective observational study. Front Med. 2023;10:1163247. doi:10.3389/fmed.2023.1163247
30. Lin L, Qiu D, Yang F, et al. Hydrogen-rich saline upregulates the Sirt1/NF-κB signaling pathway and reduces vascular endothelial glycocalyx shedding in sepsis-induced acute kidney injury. Shock. 2024;62:416–425. doi:10.1097/SHK.0000000000002404
31. Kong G, Li D, Liu X, et al. PLD2 deficiency alleviates endothelial glycocalyx degradation in LPS-induced ARDS/ALI. Biochem Biophys Res Commun. 2024;716:150019. doi:10.1016/j.bbrc.2024.150019
32. Zhou P, Song NC, Zheng ZK, et al. MMP2 and MMP9 contribute to lung ischemia-reperfusion injury via promoting pyroptosis in mice. BMC Pulm Med. 2022;22(1):230. doi:10.1186/s12890-022-02018-7
33. Fernández-Sarmiento J, Molina CF, Salazar-Pelaez LM, et al. Biomarkers of glycocalyx injury and endothelial activation are associated with clinical outcomes in patients with sepsis: a systematic review and meta-analysis. J Intensive Care Med. 2023;38(1):95–105. doi:10.1177/08850666221109186
34. Toner AJ, Corcoran TB, Vlaskovsky PS, et al. Inflammation risk before cardiac surgery and the treatment effect of intraoperative dexamethasone. Anaesth Intensive Care. 2024;52(1):28–36. doi:10.1177/0310057X231195098
35. Hudetz JA, Gandhi SD, Iqbal Z, et al. Elevated postoperative inflammatory biomarkers are associated with short- and medium-term cognitive dysfunction after coronary artery surgery. J Anesth. 2011;25(1):1–9. doi:10.1007/s00540-010-1042-y
36. Pesonen E, Passov A, Andersson S, et al. Glycocalyx degradation and inflammation in cardiac surgery. J Cardiothorac Vasc Anesth. 2019;33(2):341–345. doi:10.1053/j.jvca.2018.04.007
37. Huang X, Lu F, Tian H, et al. Association between plasma glycocalyx component levels and poor prognosis in severe influenza type a (H1N1). Sci Rep. 2022;12(1):163. doi:10.1038/s41598-021-04146-2
38. Ray CC, Pollack MM, Gai J, et al. The association of the lactate-albumin ratio with mortality and multiple organ dysfunction in PICU patients. Pediatr Crit Care Med. 2023;24(9):760–766. doi:10.1097/PCC.0000000000003272
39. Xiong C, Jia Y, Wu X, et al. Early postoperative acetaminophen administration and severe acute kidney injury after cardiac surgery. Am J Kidney Dis. 2023;81(6):675–683. doi:10.1053/j.ajkd.2022.11.009
40. Lobasso M, Schneider J, Sanchez-Pinto LN, et al. Acute kidney injury and kidney recovery after cardiopulmonary bypass in children. Pediatr Nephrol. 2022;37(3):659–665. doi:10.1007/s00467-021-05179-5
41. Bian Y, Xu T, Le Y, et al. The efficacy and safety of sodium bicarbonate Ringer’s solution in critically ill patients: a retrospective cohort study. Front Pharmacol. 2022;13:829394. doi:10.3389/fphar.2022.829394
42. Ordóñez-Velasco LM, Hernández-Leiva E. Factors associated with delirium after cardiac surgery: a prospective cohort study. Ann Card Anaesth. 2021;24(2):183–189. doi:10.4103/aca.ACA_43_20
43. Brown CH, Kim AS, Yanek L, et al. Association of perioperative plasma concentration of neurofilament light with delirium after cardiac surgery: a nested observational study. Br J Anaesth. 2024;132(2):312–319. doi:10.1016/j.bja.2023.10.043
44. Iwata H, Katoh T, Truong SK, et al. Hydrogen attenuates endothelial glycocalyx damage associated with partial cardiopulmonary bypass in rats. PLoS One. 2023;18(12):e0295862. doi:10.1371/journal.pone.0295862
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.