Back to Journals » Patient Preference and Adherence » Volume 20
Intraoperative Inner Experiences of Patients Undergoing Percutaneous Lung Tumor Radiofrequency Ablation Guided by CT in a Chinese Tertiary Hospital: A Qualitative Study
Authors Lu X, Deng H, Wang H, Yu M
Received 26 March 2026
Accepted for publication 7 July 2026
Published 15 July 2026 Volume 2026:20 608120
DOI https://doi.org/10.2147/PPA.S608120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Xuan Lu,1,* Hui Deng,1,* Heping Wang,1 Min Yu2
1Department of Geriatrics, Nanjing Drum Tower Hospital, Affiliated Nanjing University Medical School, Nanjing, Jiangsu, 210008, People’s Republic of China; 2Department of Respiratory and Critical Care, Nanjing Drum Tower Hospital, Affiliated Nanjing University Medical school, Nanjing, Jiangsu, 210008, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Heping Wang, Department of Geriatrics, Nanjing Drum Tower Hospital, The Affiliated Nanjing University Medical School, Nanjing, Jiangsu, People’s Republic of China, Email [email protected] Min Yu, Department of Respiratory and Critical Care, Nanjing Drum Tower Hospital, The Affiliated Nanjing University Medical school, Nanjing, Jiangsu, People’s Republic of China, Email [email protected]
Background: Pulmonary tumors rank among the most common thoracic diseases. Optimized therapies are critical to improve patient prognosis and quality of life. Radical surgery is risky and unsuitable for elderly frail patients or those with poor cardiopulmonary function and distant metastasis. CT-guided percutaneous lung radiofrequency ablation is a validated minimally invasive therapy with minor trauma, few complications, and rapid recovery. Existing quantitative studies mainly evaluate its therapeutic efficacy, whereas few investigate patients’ distinctive psychological experiences during ablation. Sustained immobilization and treatment concerns trigger anxiety that undermines procedural cooperation and recovery. This qualitative study explores patients’ perioperative feelings to provide evidence for individualized psychological interventions.
Objective: To explore the authentic perioperative physical and psychological experiences of patients with lung tumors receiving CT-guided percutaneous radiofrequency ablation, so as to provide evidence for developing targeted perioperative nursing interventions.
Methods: A qualitative descriptive design was adopted. Purposive sampling was used to recruit 14 patients hospitalized at a tertiary hospital in Nanjing from September to November 2025 who were scheduled for CT-guided percutaneous radiofrequency ablation. Semi-structured one-on-one interviews were conducted to collect patients’ first-hand perioperative narratives. Data were analyzed via Colaizzi’s seven-step qualitative analysis procedure, with the Health Belief Model applied as the theoretical framework to categorize and interpret extracted themes.
Results: With the Health Belief Model (HBM) adopted as the analytical framework, this study extracted the authentic perioperative experiences of patients receiving CT-guided percutaneous radiofrequency ablation for lung tumors from psychological, physical, and cognitive dimensions. Three core themes including 14 subthemes were summarized: (1) Complex ambivalent emotions, (2) Coexisting multiple physical discomforts, (3) Disease cognition and care needs.
Conclusion: Clinical staff should fully recognize the diversified physical and psychological distress experienced by ablation patients. Standardized preoperative health education covering procedural knowledge and cooperation tips, together with stage-specific supportive care strategies, are recommended to relieve patient suffering. Given the single-center exploratory nature of this study, the findings cannot be widely generalized, and further multi-center verification is required.
Keywords: lung tumor, lung puncture, radiofrequency ablation, experience, qualitative study
Introduction
Lung tumors, malignant disorders with persistently high global incidence and mortality, render the optimization of their therapeutic regimens a core priority in clinical research.1 Traditional surgical resection was once the preferred treatment for early-stage lung tumor patients. However, surgical resection is a double-edged sword for elderly, frail patients, individuals with limited cardiopulmonary reserve, distant metastases, or lesions inaccessible to open thoracotomy. Severe surgical trauma may not only precipitate major complications but also accelerate physical decline.2 Against this backdrop, the emergence of minimally invasive techniques has pioneered new pathways in lung tumor treatment.2 Among various minimally invasive modalities, CT-guided percutaneous radiofrequency ablation (RFA) has evolved into an irreplaceable clinical technique owing to its strengths in precise positioning and focal tumor ablation. Under CT guidance, radiofrequency electrodes are percutaneously deployed into target lesions. High-frequency alternating current generates localized thermal energy that triggers coagulative necrosis of neoplastic cells, yielding effective tumor volume reduction while optimally preserving the functional parenchyma of normal lung tissue.3,4 This therapeutic modality brings promising prospects for prolonging overall survival and enhancing health-related quality of life among patients with advanced lung malignancy or those ineligible for surgical resection.5
Accumulated clinical evidence supports the safety and wide applicability of CT-guided radiofrequency ablation, which has been included in authoritative international guidelines as part of multidisciplinary lung tumor therapy.5,6 It yields comparable long-term survival for small early-stage lesions versus surgery, accompanied by fewer mild, easily managed complications such as minor pneumothorax and hemoptysis, and also enables palliative relief for multiple pulmonary metastases.7,8 Advances in imaging and AI positioning further shorten operation time and lower patients’ radiation load.
Despite abundant evidence confirming the technical and oncological advantages of CT-guided percutaneous radiofrequency ablation, most existing research centers on objective clinical endpoints and tumor control, with insufficient attention paid to patients’ subjective perioperative physical and psychological experiences.4,7 Available qualitative studies rarely systematically analyze patients’ ambivalent emotions, physical discomfort, radiation-related worries and financial stress during puncture and ablation.9
Clinically, practitioners tend to prioritize tumor curative effects yet overlook the full spectrum of patients’ treatment-related burdens.10 Patients face multiple stressors across the whole care pathway: preoperatively, repeated examinations such as enhanced CT raise anxiety over contrast allergies; intraoperatively, prolonged forced immobilization under CT scanning brings severe physical suffering, especially for elderly, weak patients and those with musculoskeletal disorders. Meanwhile, persistent fears about puncture pain, hemorrhage, tumor recurrence and uncertain prognosis pervade the procedure.4,9 Such negative feelings reduce intraoperative cooperation and may disrupt neuroendocrine and immune functions, impairing treatment response and postoperative rehabilitation. Relevant evidence further demonstrates that patients with intense pretreatment anxiety suffer a 2.5-fold higher complication risk and longer recovery periods than emotionally stable counterparts.11
The Health Belief Model (HBM) is a classical theoretical framework of social psychology to explain health behaviors.12 It evaluates individuals from three aspects of physiology, psychology, and cognition, with the core dimensions of perceived susceptibility and severity of disease threat, perceived benefits of health-promoting behaviors, perceived behavioral barriers and self-efficacy.12,13 Literature on CT-guided percutaneous lung tumor ablation, perioperative symptom management, patients’ psychological distress, qualitative interview methods, medical cost burden, and targeted nursing interventions has confirmed that patients’ complex perioperative feelings during ablation accurately reflect the interaction between the dimensions of HBM.14,15 These studies provided a solid methodological foundation for the use of semi-structured qualitative interviews and the Colaizzi’s seven-step analysis guided by the HBM,16 while clarifying the significance of exploring the real experience of patients in clinical care.
In view of the lack of a systematic description of the physical and mental burden of patients with CT-guided puncture ablation in the current qualitative research, this study captured the real physical discomfort, ambivalence, radiation concerns and economic pressure of patients through in-depth semi-structured interviews from the perspective of the HBM theory. The results of this study can provide clinical staff with targeted insight into the unmet needs of patients, provide support for the development of individualized perioperative supportive interventions, reduce the pain of patients and promote rehabilitation, improve the overall intraoperative treatment experience of patients, and promote the implementation of patient-centered quality care concept in patients with lung tumor in respiratory department.
Methods
Design
A descriptive phenomenological approach was used to delve deeply into the in-situ real-life experiences of lung tumor patients undergoing CT-guided lung puncture and radiofrequency ablation surgery. Face-to-face, semi-structured interviews were conducted with patients to gather information on intraoperative authenticity experiences and feelings.
Participants and Setting
A qualitative descriptive design was adopted. Purposive sampling was used to recruit 14 patients hospitalized at a tertiary hospital in Nanjing from September to November 2025 who were scheduled for CT-guided percutaneous radiofrequency ablation. Inclusion criteria: (1) Age ≥18 years; diagnosed by a physician at the level of deputy chief physician or above as meeting the indications for percutaneous radiofrequency ablation of lung tumors, with planned or completed surgery; (2) Clear consciousness and adequate verbal communication ability; (3) Voluntary signing of informed consent and willingness to participate in the study. Exclusion criteria: (1) Patients with severe mental illness or hearing impairment preventing interview cooperation; (2) Patients who abandoned treatment during surgery or could not continue cooperating with the procedure. During semi-structured interviews, continuous comparative analysis was conducted concurrently with data collection. Data saturation was deemed achieved when no new categories, concepts, or unique viewpoints emerged from consecutive interview transcripts, and the extracted themes were sufficiently repeated and mutually verified across participants.16 Subsequent recruitment of additional participants was not pursued. Ultimately, interviewing 14 lung tumor patients. See Table 1.
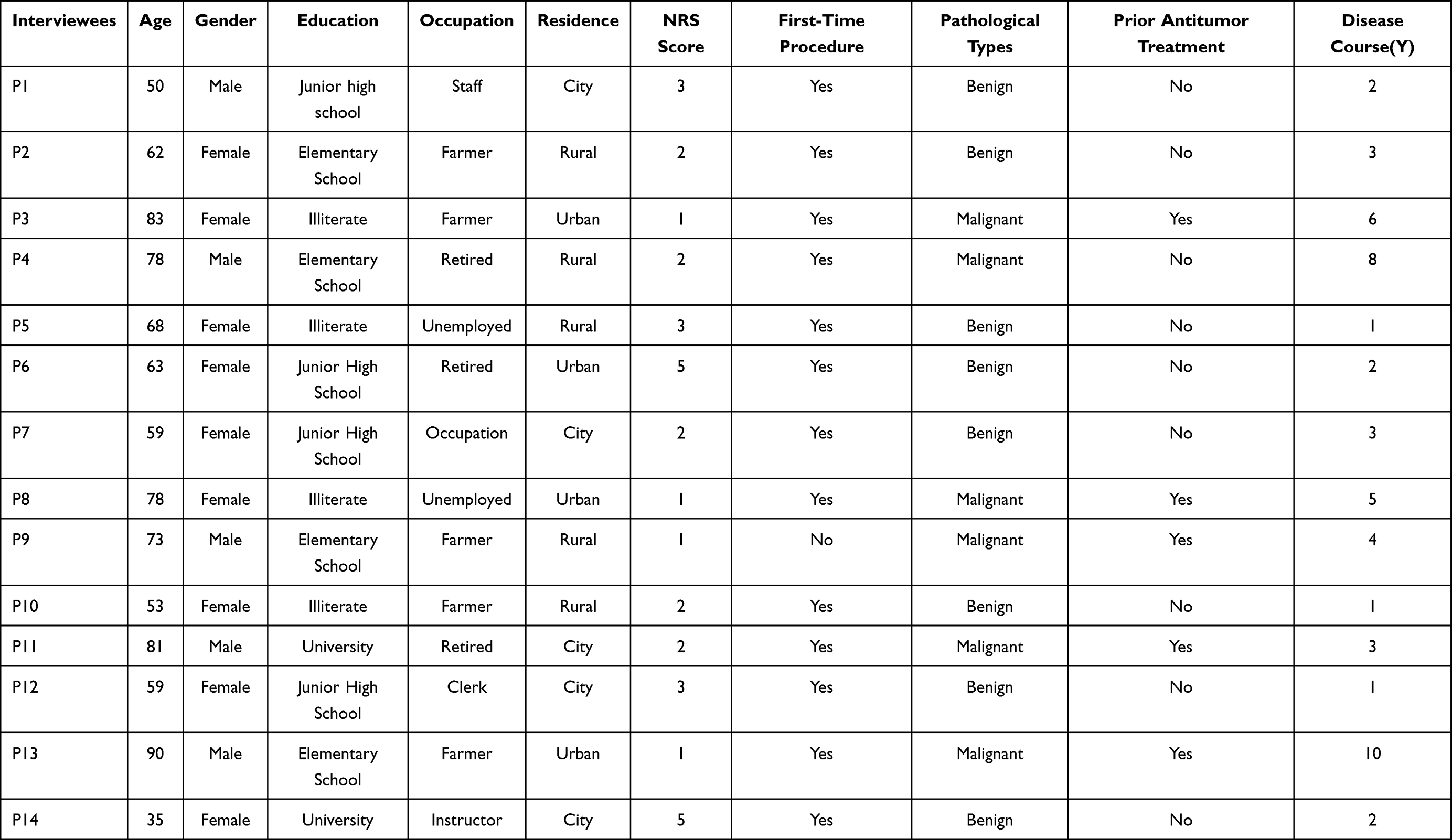 |
Table 1 Characteristics of Interviewees (n=14) |
Interview Topic Guide
Based on the research objectives and HBM, a preliminary interview outline was developed after reviewing relevant domestic and international literature, consulting experts, and conducting team discussions. A pre-interview was conducted with three patients who had undergone CT-guided percutaneous radiofrequency ablation for lung tumors. The interview outline was further polished and finalized. The HBM based interview questions are detailed in Figure 1.
 |
Figure 1 HBM based interview questions. |
Data Collection
A phenomenological approach was adopted, with semi-structured one-on-one face-to-face interviews for data collection. All interviews took place 6–24 hours after CT-guided radiofrequency ablation. Researchers prearranged the interview time and venue with each participant. Prior to each session, patients were fully briefed on the study purpose, interview process and confidentiality rules, and all provided signed written informed consent that was securely archived.
A standardized interview outline was prepared in advance to define core themes and workflow. Each interview followed three phases: ice-breaking introduction, in-depth thematic discussion, and concluding feedback. The ward department arranged a quiet interview space and placed a “Do not disturb” sign to reduce external disruptions. The interviewers were ward nurses who were not in charge of the daily care of the enrolled participants, which helped reduce response bias caused by doctor-patient dependency. Researchers used plain, easy-to-understand questions and encouraged participants to elaborate their true feelings to advance dialogue, while documenting all nonverbal cues in real time. The formal interview segment lasted 20–40 minutes per participant.
Each team member has a wealth of nursing education, clinical management, and research expertise that supports accurate identification of the real life experiences of patients. The educational background of the main team members included 2 doctoral degrees, 1 master’s degree and 1 bachelor’s degree, all of whom had completed the professional training of qualitative research. A strict bias control strategy was used during the analysis. Coding and theme extraction were performed independently by two researchers. Disagreements on norms were resolved through panel and expert consensus to ensure credible and objective results. Continuous researcher reflexivity is practiced to limit individual subjectivity and faithfully reflect the true views of respondents.
Data Analysis
Data collection and data analysis proceeded concurrently. Within 48 hours of each interview, researcher triangulation was implemented. Two researchers independently imported audio recordings and verbatim transcripts into NVivo 11 for sorting and coding, after which their analytical results were cross-compared. When coding discrepancies emerged, a third senior qualitative expert specializing in nursing research joined group discussions to reconcile differences until a unified consensus was reached.
Colaizzi’s seven-step phenomenological analysis method guided all data processing.13 This dedicated phenomenological analytical framework consists of seven standardized procedures: (1) repeatedly reading all transcripts to fully immerse in participants’lived experiences; (2) extracting all significant original statements related to intraoperative experience of CT-guided pulmonary neoplasm radiofrequency ablation; (3) constructing formulated meanings from these significant statements; (4) grouping formulated meanings into preliminary subthemes through open coding; (5) integrating subthemes to form an exhaustive descriptive account of the research phenomenon; (6) distilling the exhaustive description into the essential structural framework of patients’ authentic feelings; (7) validating preliminary analytical outcomes via member checking.
To guarantee the trustworthiness and authenticity of findings, comprehensive member checking was conducted within 48 hours after finishing all analytical drafts. Nine participants were invited to review the preliminary thematic results, confirm whether the summarized descriptions matched their real experiences, and supplement any overlooked key viewpoints. Minor textual adjustments were made according to participants’ feedback, while no core themes were modified or deleted, which strongly supported the credibility of our analysis.
Ethical Considerations
This study was approved by the Ethics Committee of Nanjing Drum Tower Hospital, Affiliated Hospital of Nanjing University Medical School (Approval No. 2025–0137-02). This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. All procedures in this study were strictly performed in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) to ensure standardized and transparent research reporting. Prior to the interview, all participants were provided with comprehensive study information, including confidentiality details. Participants were fully informed of their right to withdraw from the study at any time during the interview without any penalty. They were also asked for their agreement to have the entire interview recorded. If participants declined recording, the interview was promptly switched to manual documentation. Importantly, the written informed consent obtained from all participants explicitly permitted the publication of their anonymized response data and de-identified direct interview quotes for academic research purposes. All participants provided signed written informed consent and participated voluntarily in this study.
Results
Using HBM as the theme analysis framework, this study refined the inner authentic experience of lung tumor patients during CT-guided percutaneous radiofrequency ablation from three aspects: psychological, physiological and cognitive aspects, including three themes: superposition of complex ambivalence, coexistence of a variety of physical discomfort, and disease cognition and needs, a total of 14 sub-themes. See Table 2.
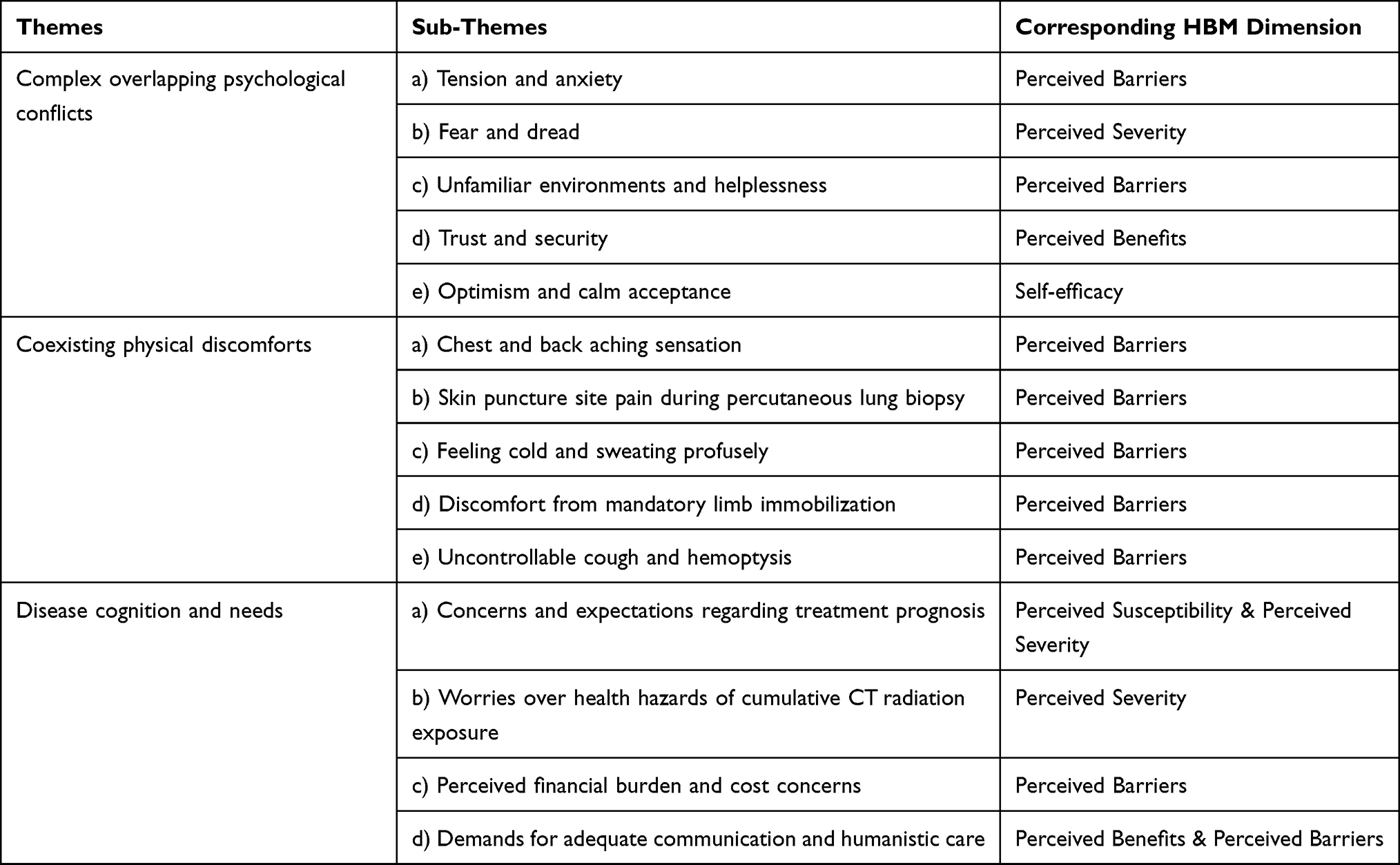 |
Table 2 Themes and Sub-Themes |
Theme 1: Complex Contradictions Psychological Overlapping
Subtheme One: Anxiety and Tension
Most participants reported persistent nervousness throughout the perioperative period. Tension is a natural psychological response to perceived threats; mild nervousness serves as a self-protective mechanism, yet severe, sustained anxiety impairs intraoperative cooperation and physical tolerance to procedural stimulation.
P2, preoperative expectations and intraoperative experiences:“I started feeling anxious before surgery. I even cried this morning. I couldn’t move at all during the entire procedure—I was extremely nervous. The doctors and nurses reassured me not to be afraid, but it didn’t help”.
P6, preoperative expectations and intraoperative experiences:“I was anxious before surgery and kept feeling nauseous. I remained tense during the procedure, but managed to relax a bit after trying to self-regulate”.
Subtheme Two: Fear and Dread
Fear stems from uncertainty about the unknown operation, potential procedural complications and unexpected intraoperative symptoms, creating severe psychological distress among participants.
P3, preoperative expectations and intraoperative experiences:“I’ve never had any surgery before. Honestly, I barely slept last night (the night before surgery). I was terrified of the procedure and trembled the entire time—I was extremely scared”.
P5, intraoperative experiences:“I felt calm at first, but I suddenly had violent coughing with hemoptysis. I was seized by terrible fear, worrying that the operation had failed or that a serious accident had happened”
Subtheme Three: Unfamiliar Environments and Helplessness
Patients often feel unfamiliar and helpless in the unfamiliar environment and presence of surgical instruments and equipment during surgery.
P1, intraoperative experiences:“During this surgery, I was conscious the whole time. Lying on the CT room bed, moving back and forth on it, I didn’t know what was happening. It felt incredibly agonizing. At one point, they (the medical staff) all left, and I was alone”.
P7, intraoperative experiences:“As soon as I entered the room and lay down, my eyes were covered with gauze. I couldn’t see anything; everything was pitch black. I felt utterly helpless and didn’t dare make a sound, afraid it might disturb the doctors performing the surgery”.
Subtheme Four: Sense of Trust and Psychological Security
Trust in medical staff serves as a core protective psychological factor that facilitates smooth implementation of CT-guided radiofrequency ablation. Patients build a sense of safety through adequate preoperative communication, recognition of clinicians’ professional proficiency, and real-time intraoperative comfort.
P9, preoperative expectation:“The doctors and nurses communicated with me thoroughly before the operation. They explained the purpose of the surgery and relevant precautions in detail. I fully trust them and feel very safe. And, this is my second time having this surgery. Last time, it was this doctor who performed it, and this time it’s him again. I trust his skills (thumbs up)”.
P13, intraoperative experiences and postoperative reflections:“I’m 90 years old. Hospitals back home wouldn’t dare operate on me. I came here after extensive inquiries. Nanjing’s major hospitals are different—they were willing to perform the procedure, calling it minimally invasive. I remained conscious throughout and experienced minimal discomfort. I’m deeply grateful to the surgeon”.
P7, preoperative expectations and intraoperative experiences:“I was extremely tense at the beginning and dared not move or breathe smoothly. The doctor kept comforting me and telling me to breathe normally, and I slowly calmed down with a strong sense of safety (smiles)”.
Subtheme Five: Optimism and Calm Acceptance
A positive, composed attitude helps stabilize neuroendocrine and immune function, which can improve physical tolerance to intraoperative stimuli and support favorable treatment recovery. Such positive cognition originates from personal life experience and positive reference cases of similar diseases.
P4, preoperative expectations and postoperative reflections:“I even fought in wars when I was young. Now I’ve lived well over 70 years—I’ve lived a full life. I feel my life has been worthwhile. I’ve experienced everything I needed to, so there’s nothing to worry about (proud)”.
P11, preoperative expectations:“This illness is not a big deal. A friend of mine had lung tumor a few years ago and is still alive today. We are not even sure if mine is malignant yet”.
Theme 2: Multiple Physical Discomfort Coexisting
Subtheme One: Chest and Back Aching Sensation
The lung tissue has relatively sparse nerve distribution, and most patients receive local anesthesia before lung biopsy. Therefore, the needle entering the lung tissue typically causes no pain. However, it may stimulate nerve endings in the lung tissue, leading to a mild sensation of soreness or pressure in the chest and back.
P6, intraoperative experiences:“As the needle gradually entered my skin and then deeper into my lung, I felt a sour, swollen ache in my back that was very uncomfortable I could not help but let out a soft groan”.
P14, intraoperative experiences:“Throughout the procedure, I felt a swollen sensation in my chest and back—not the usual kind of pain. Especially when the doctor told me it was almost finished and they were ablating the diseased lung tissue, the swelling and pain intensified, and I also felt a slight burning sensation”.
Subtheme Two: Skin Puncture Site Pain During Percutaneous Lung Biopsy
During percutaneous lung biopsy, as the needle traverses the chest wall, brief stinging may occur when it passes through intercostal nerves. This primarily involves chest wall discomfort rather than direct lung tissue pain, but it can still cause patient distress during the procedure.
P1, intraoperative experiences:“That needle (the syringe with lidocaine) really hurt a bit when it first went in. After a few minutes, maybe because of the anesthetic, it did not hurt much anymore. I could basically tolerate that pain”.
P12, intraoperative experiences:“It hurt more when they gave the anesthetic. Later, when the needle went in, there was also a slight pain in the chest wall skin. It was an indescribable discomfort”.
Subtheme Three: Feeling Cold and Sweating Profusely
During lung puncture, some patients experience chills and cold sweats due to environmental and psychological factors, influenced by multiple variables.
P14, intraoperative experiences:“Throughout the procedure, I felt extremely cold, likely because my upper body was exposed. Strangely, I also sweated profusely—my clothes became soaked”.
P12, intraoperative experiences:“The CT room was really cold, especially in winter with no heating. I was covered in a blanket but kept sweating profusely and shivering. I dared not make a sound”.
Subtheme Four: Physical Discomfort from Mandatory Immobilization
Complete limb and body immobilization is mandatory throughout CT-guided radiofrequency ablation to guarantee puncture precision. Any unintended body movement may shift the needle away from target lesions, raising operational risks and compromising therapeutic effects. Long-term fixed postures inevitably bring severe physical fatigue and soreness to patients.
P1, intraoperative experiences:“The CT examination table was extremely narrow. Monitors for blood pressure and oxygen saturation were attached to my body, and I was required to keep both arms raised overhead without any movement for roughly 30 minutes after puncture. My arms ached unbearably, and the waiting time felt endless, leaving me physically and mentally drained”.
P10, intraoperative experiences:“I never imagined this minimally invasive surgery would be so difficult. Lying face-down with my arms stretched forward was exhausting. I dared not move at all. Later, a doctor supported my arms briefly, which helped somewhat, but I remained exhausted. I literally counted every second, desperate for it to end”.
Subtheme Five: Uncontrollable Coughing and Hemoptysis
Due to patient factors and surgical techniques, damage to the airway mucosa, pulmonary tissue vessels, and alveolar rupture may occur, leading to hemoptysis. Stimulation of the lungs can also trigger coughing.
P12, intraoperative experiences:“I felt the doctor puncturing my body back and forth countless times. At first, I did not feel much, but after about 20 minutes, I started wanting to cough. I held it in, but eventually could not anymore and coughed continuously. There was phlegm, and then I coughed up blood. I saw several large mouthfuls of blood “.
P8, intraoperative experiences and postoperative reflections:“The doctor informed me preoperatively that abundant blood vessels surround my lesion with a potential bleeding risk, but I did not expect severe hemoptysis intraoperatively. I suffered persistent coughing with recurrent blood expectoration for nearly 10 minutes after puncture”.
Theme 3: Disease Awareness and Needs
Subtheme One: Concerns About Treatment Outcomes and Expectations
Patients’ conflicting feelings about the efficacy of “minimally invasive but not curative” treatments affect treatment adherence. Additionally, patients harbor various concerns and expectations regarding surgery.
P14, postoperative reflections:“I am actually quite worried about whether the condition will recur or worsen after this surgery. I hope it can be cured in one go so I will not suffer anymore”.
P9, preoperative expectations:“I am getting older. Our county hospital recommended traditional Chinese medicine treatment, but I declined. Later, a friend introduced me to this minimally invasive surgery, so I came to the hospital for the procedure. I am unsure if it can cure me completely in one go”.
Subtheme Two: Worries Over Health Hazards of Cumulative CT Radiation Exposure
Repeated CT positioning scans are required for precise puncture, triggering patients’ independent cognitive concerns regarding cumulative radiation and its potential long-term damage to physical health. This rational risk perception acts as a major inducement of anxiety rather than emotional tension itself.
P6, intraoperative experiences and postoperative reflections:“During my procedure, I went in and out of the CT scanner five or six times. I know the general recommendation is one CT scan per year, but this surgery required so many scans. I am quite concerned about the cumulative radiation exposure and its potential harm to my body”.
P7, preoperative expectations, intraoperative experiences, and postoperative reflections:“I know CT radiation can increase cancer risk, so I am usually careful. But I never expected this procedure would require so many scans. I feel like I have never had this many CT scans in my entire life. Both my family and I have concerns about this”.
Subtheme Three: Concerns About Treatment Costs and Financial Burden for the Operation
The cost of percutaneous radiofrequency ablation surgery generally ranges from 2876.00 USD $ to 14,380 USD $. Specific expenses depend on multiple factors, including the type of disease being treated, medical equipment used, hospital location and grade, and the patient’s individual circumstances. For many patients, these high medical costs can impose significant financial burdens and psychological stress.
P2, preoperative expectations and postoperative reflections:“This procedure costs over 20,000 RMB, and I heard it’s not covered by medical insurance. Ugh, it’s adding to the family’s burden (frowns)”.
P10, postoperative reflections:“Actually, my family did not explain the details when I had this surgery. Just now I heard they said the 15,000 RMB deposit is already used up and there’s an outstanding balance. How can such a minor procedure be so expensive? (confused)”.
Subtheme Four: Information Communication and Care Needs
Patients undergoing lung biopsy face disease uncertainty and surgical risks, often experiencing anxiety, fear, and other negative emotions. The presence and care of family and friends are crucial for alleviating psychological stress.
P8, preoperative expectations and intraoperative experiences:“I was fully conscious throughout the procedure and terrified. No one explained the surgery beforehand, and during the operation, no one updated me on its progress. Though the medical staff tried to reassure me, I remained anxious. Having family by my side would have been so much better”.
P2, intraoperative experiences:“My eyes were covered during the procedure, and I could not see anything. I was extremely nervous. The doctor periodically updated me on the progress as they worked step by step. The doctor and nurses left me alone several times. How I wished someone could have stayed with me the whole time!”
Discussion
Cultivate Objective Illness Cognition and Attach Importance to Patients’ Perioperative Psychological Experiences
Guiding patients to form a scientific understanding of their own diseases, and focusing on their psychological feelings before and after the surgery, are the core nursing priorities directly extracted from the theme of practical life experience in this study. Consistent with the core constructs of the HBM, the results of our qualitative research indicate that patients exhibit complex and contradictory psychological states during CT-guided lung puncture and ablation treatment, which can be divided into two dimensions: positive and negative.
The positive experiences derived from the patients’ accounts include a sense of security, trust in medical staff, optimism, and a calm state of mind. These positive psychological states are mainly attributed to an individual’s psychological resilience, recognition of the doctor’s professional competence, and the continuous emotional support provided by nurses during the treatment process. From the perspective of the HBM research, these factors can reduce the patients’ perceived treatment obstacles and become effective motivating factors for their active participation in the treatment.14 On the contrary, tension, anxiety, fear of the treatment process, discomfort with the unfamiliar medical environment, and helplessness, etc, are all clearly recorded in the original interview data. The fundamental cause of these negative emotions lies in the patients’ incomplete or inaccurate understanding of their own condition and the ablation procedure, resulting in insufficient psychological preparation before the intervention.14 This conclusion is consistent with the research results of Cao et al.17
According to the interpretation of the HBM theory, excessive reinforcement of the disease susceptibility perception and severity perception can significantly reduce the intraoperative cooperation degree, hinder the postoperative recovery process, and may increase the risk of poor ablation efficacy and poor long-term prognosis.18 Based on the cognitive biases identified in the subjects, it is recommended to take targeted nursing intervention measures to improve this situation. Nurses should conduct repeated and detailed preoperative health education for patients and their families, fully explaining the purpose of the surgery, the ablation operation process, and the required fixation postural requirements during CT scans, in order to correct cognitive misunderstandings and alleviate negative emotions.19 In combination with the feedback from patients about their fear of unfamiliar equipment, we suggest formulating an intraoperative psychological optimization plan based on qualitative evidence support, such as, nurses should accompany patients to the CT room 5–10 minutes in advance to help them familiarize with the environment and equipment, thereby alleviating the fear and unease caused by the environment.17 In conclusion, all of the above targeted nursing measures can, under the guidance of the HBM, reduce patients’ psychological barriers, improve treatment compliance, and ultimately optimize treatment outcomes.
Strengthen Humanistic Care and Identify Patients’ Intraoperative Physical Stress Responses
Physical discomfort during the operation was identified as the main treatment obstacle factor in the qualitative data of this study, which is consistent with the obstacle dimensions in the HBM scale. All the subjects remained fully conscious during the lung puncture and ablation procedures. The original interview records confirmed that they not only endured great psychological pressure but also experienced various physical discomfort symptoms, such as chest and back pain during the puncture and ablation process, limb pain and stiffness caused by long-term immobilization, uncontrollable coughing, and occasional hemoptysis. This physical discomfort characteristic is consistent with the conclusions of existing clinical studies.9
Given that the patient has multiple different physical stress responses, nurses need to implement humanized and personalized care as targeted intervention measures to alleviate the physical impairments we identified in our study. Medical staff should enhance their empathy-based care skills, keenly detect changes in the patient’s physical and mental state, and provide individualized care support that matches their actual level of discomfort. Existing research shows that using simple gesture signals (such as raising the thumb) for narrative communication helps patients express their physical discomfort promptly, enabling nurses to quickly implement symptom treatment and provide humane comfort care.20 Moreover, scheduling CT examinations reasonably can alleviate the waiting fatigue of patients; fully covering the skin during the scan can avoid unnecessary skin exposure and cold discomfort. Guiding patients to practice progressive muscle relaxation and synchronize with the rhythm of deep breathing (inhale for 4 seconds, hold for 2 seconds, exhale for 6 seconds) can effectively relieve physical tension and ensure the smooth operation.21
Provide Multi-Channel Professional Information Support to Promote Patients’ Autonomous Decision-Making
The lack of professional disease knowledge is a significant factor contributing to patients’ perception of treatment uncertainty based on the Health Belief Model (HBM). This was clearly demonstrated in our qualitative interview data. Most patients have widespread concerns about CT-guided radiofrequency ablation for pulmonary nodules, including doubts about the efficacy, anxiety about the CT radiation risk, and concerns about the economic burden. Patients mainly obtain scattered disease knowledge through online media or non-professional advice provided by friends and relatives, lacking standardized and authoritative information channels. At the same time, patients’ autonomous treatment decisions are significantly influenced by systematic professional guidance from clinical medical staff.
Based on the information acquisition barriers identified in this study, we proposed a multi-channel standardized information supply strategy to enhance patients’ disease awareness and decision-making ability. Existing research has shown that providing professional and integrated information services through hospital WeChat official accounts, printed guidance manuals, and online consultation platforms can help patients obtain accurate knowledge about ablation treatment, enhance their psychological adaptability and treatment compliance to the intervention, and improve long-term prognosis.22 Establishing postoperative patient peer support groups is also an effective information intervention measure. Within one to three months after the ablation surgery, patients can share their real rehabilitation experiences, thereby eliminating common misunderstandings derived from interview records, such as equating radiofrequency ablation with complete surgical removal.23 Additionally, research has shown that implementing an intervention program including aerobic exercise (such as brisk walking), resistance training, and eight-step Tai Chi practice within 12 weeks after treatment can improve the feasibility and safety of this therapy.14 With the development of smart hospitals, we also suggest that based on the HBM-action framework support, patients can obtain multi-channel professional information through the “Internet+” platform, which can help correct patients’ biased cognition of the disease, reduce their perception of treatment obstacles, and promote patients’ transition from passive acceptance to active and autonomous medical decision-making.24
Limitations
This single-center qualitative study employed purposive sampling and recruited participants exclusively from a tertiary hospital in Nanjing. This approach may introduce potential selection bias and significantly limit the transferability and generalizability of the research results. All participants shared similar cultural backgrounds. Cultural perceptions of pain, disease risks, and medical costs shaped patients’ emotional expressions and nursing needs. Therefore, the research results cannot be directly applied to populations with different cultures or geographical backgrounds. Moreover, the existing data only provided an exploratory description of patients’ inner experiences during the perioperative period and lacked quantitative validation of the effectiveness of targeted supportive intervention measures. Future studies need to conduct multi-center qualitative research, develop scales, and conduct large-sample mixed-method studies covering different regions, age groups, and disease stages to verify and expand the current conclusions.
Conclusions
Based on the HBM, this qualitative study explored the real experiences of patients undergoing CT-guided percutaneous radiofrequency ablation for lung tumors during the perioperative period, and identified three core experience dimensions: complex psychological conflicts, multiple physical discomforts, disease-related cognition, and nursing needs. The results of this study provide a theoretical and practical foundation for designing individualized perioperative nursing intervention measures to alleviate patients’ pain and optimize their treatment experience.
Given the limitations of single-center recruitment and the limited sample size, conclusions cannot be generalized to all medical Settings or patient populations. The related clinical application strategies are only tentative directions and need to be further verified. In the future, multi-center, multi-region, multi-age and multi-disease severity studies are needed to enrich the relevant evidence. In addition, the results of this study provide clear clues for the development of targeted interventions, and follow-up studies can integrate digital tools such as virtual reality and telemedicine to provide convenient and efficient psychological intervention and preoperative health education services.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author[Heping Wang or Min Yu]. Data are not made public due to privacy and ethical restrictions.
Acknowledgments
We sincerely express our gratitude to the patients with lung tumors who participated in this study and generously shared their experiences and thoughts with us. We also extend our appreciation to Respiratory and Critical Care Medicine Department workers who provided us with invaluable assistance and guidance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Xuan Lu and Hui Deng are co-first authors for this work. The authors declare no conflicts of interest in this work.
References
1. Yang G, Zhang X, Zhang H, et al. Expert consensus on integrated traditional and western medicine management of pulmonary nodules. Chin J Exp Tradit Med Formulae. 2024;30(01):149–14. doi:10.13422/j.cnki.syfjx.20240492
2. Zhou D, Yao T, Huang X, et al. Real-world comprehensive diagnosis and “Surgery + X” treatment strategy of early-stage synchronous multiple primary lung cancer. Cancer Med. 2023;12(12):12996–13006. doi:10.1002/cam4.5972
3. Shen X, Shen C, Xiao CJ, et al. Progress in ablation therapy of pulmonary nodules. Chin J Clin Thorac Cardiovasc Surg. 2025;32(3):401–405. doi:10.7507/1007-4848.202306025
4. Venturini M, Cariati M, Marra P, et al. CIRSE standards of practice on thermal ablation of primary and secondary lung tumours. Cardiovasc Intervent Radiol. 2020;43(5):667–683. doi:10.1007/s00270-020-02432-6
5. Zheng X, Shao J, Zhou L, et al. A comprehensive nomogram combining CT imaging with clinical features for prediction of lymph node metastasis in Stage I-IIIB non-small cell lung cancer. Ther Innov Regul Sci. 2022;56(1):155–167. doi:10.1007/s43441-021-00345-1
6. Sang J, Ye X. Potential biomarkers for predicting immune response and outcomes in lung cancer patients undergoing thermal ablation. Front Immunol. 2023;14:1268331. doi:10.3389/fimmu.2023.1268331
7. Ambrogi MC, Fanucchi O, Dini P, et al. Wedge resection and radiofrequency ablation for stage I nonsmall cell lung cancer. Eur Respir J. 2015;45(4):1089–1097. doi:10.1183/09031936.00188014
8. Schneider T, Reuss D, Warth A, et al. The efficacy of bipolar and multipolar radiofrequency ablation of lung neoplasms-results of an ablate and resect study. Eur J Cardiothorac Surg. 2011;39(6):968–973. doi:10.1016/j.ejcts.2010.08.055
9. Zhu Y, Cao J, Dai Q, et al. A qualitative study of symptom experience in elderly patients with lung cancer after microwave ablation. Geriatr Health Care. 2025;31(1):69–73. doi:10.3969/j.issn.1008-8296.2025.01.015
10. Tan N, Kuang ZS. Effects of preoperative anxiety on early postoperative rehabilitation in patients with lung cancer surgery. Chin J Health Psychol. 2022;30(6):830–834. doi:10.13342/j.cnki.cjhp.2022.06.007
11. Spicer JD, Cascone T, Wynes MW, et al. Neoadjuvant and adjuvant treatments for early stage resectable NSCLC: consensus recommendations from the international association for the study of lung cancer. J Thorac Oncol. 2024;19(10):1373–1414. doi:10.1016/j.jtho.2024.06.010
12. De Leon AN, Peterson R, Dvorak RD, et al. The health belief model in the context of alcohol protective behavioral strategies. Psychiatry. 2023;86(1):1–16. doi:10.1080/00332747.2022.2114270
13. Ban HJ, Kim HS. Applying the modified health belief model (HBM) to Korean medical tourism. Int J Environ Res Public Health. 2020;17(10):3646. doi:10.3390/ijerph17103646
14. Yang Z, Zhu Y, Xiang G, et al. First-line atezolizumab plus chemotherapy in advanced non-squamous non-small cell lung cancer: a cost-effectiveness analysis from China. Expert Rev Pharmacoecon Outcomes Res. 2021;21(5):1061–1067. doi:10.1080/14737167.2021.1899813
15. Liu C, Cheng J, He C, et al. Preoperative health belief model-based nursing intervention on anxiety and pain-related stress in lung cancer patients. J Vis Exp. 2026;14(230). doi:10.3791/69760
16. O’Brien BC, Harris IB, Beckman TJ, et al. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388
17. Cao JW, Wu Y, Zhao WJ, et al. The establishment and nursing safety management of daytime operation mode for percutaneous lungbiopsy in outpatient clinic. J Intervent Radio. 2020;29(08):838–841. doi:10.3969/j.issn.1008-794X.2020.08.022
18. Yang J, Yin Y, Yu G, et al. Facilitators and barriers to help-seeking behavior for symptoms in patients with lung cancer in China-a qualitative study. Front Psychol. 2026;16:1718034. doi:10.3389/fpsyg.2025.1718034
19. Huang CM, Zhou YZ, Xu J, et al. Exploration and challenge of whole course follow-up management model for small cell lung cancer. Chin J Lung Cancer. 2025;28(01):47–54. doi:10.3779/j.issn.1009-3419.2025.106.01
20. Sun XX, Wang YL, Lv W, et al. Application research of narrative care to the management of symptom clusters and post-traumatic growth in patients undergoing lung cancer surgery. Chin J Lung Cancer. 2025;28(1):40–46. doi:10.3779/j.issn.1009-3419.2024.102.44
21. Mei SL, Wu XY, Yang J, et al. Application of precise nursing strategy based on multidisciplinary collaboration in elderly patients undergoing thoracoscopic lung cancer surgery. J Sichuan Univ. 2023;54(5):1052–1057. doi:10.12182/20230960508
22. Cao CC, Wang YM, Lu MH, et al. Experience and demand of virtual reality analgesia for patients after resection for lung cancer: a qualitative research. Tianjin J Nurs. 2025;33(01):1–5. doi:10.3969/j.issn.1006-9143.2025.01.001
23. Zhang Z, Mao YJ. Effect of multidisciplinary team nursing model in patients with lung cancer undergoing CT guided radiofrequency ablation during perioperative period. Nurs J Chin PLA. 2022;39(02):80–83. doi:10.3969/j.issn.1008-9993.2022.02.020
24. Song Y, LMi C, Liu J, et al. Application effect of internet + continuity nursing in 3D small pulmonary nodules biopsy guided by coplanar template. Chin J Med Herald. 2021;18(19):181–184. doi:10.20047/j.issn1673-7210.2021.19.043
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.