Back to Journals » Clinical Ophthalmology » Volume 20
Intraoperative Degree Misalignment in Toric Intraocular Lens Implantation When Using Conventional Compared to Digital Marking
Authors Kandavel R ![]() , Dredge J, Jackson H, Landingin J, Henderson SK, Alam T, Hall B
, Dredge J, Jackson H, Landingin J, Henderson SK, Alam T, Hall B ![]()
Received 8 October 2025
Accepted for publication 3 March 2026
Published 16 March 2026 Volume 2026:20 572712
DOI https://doi.org/10.2147/OPTH.S572712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Rom Kandavel,1 Justin Dredge,1 Hayden Jackson,1 Jaymil Landingin,1 Shani K Henderson,1 Tamanna Alam,1 Brad Hall2
1Colvard-Kandavel Eye Center, Encino, CA, USA; 2Sengi, Penniac, NB, Canada
Correspondence: Rom Kandavel, Colvard-Kandavel Eye Center, Encino, CA, USA, Tel +1 818 906 2929, Email [email protected]
Purpose: To evaluate the difference in degrees between a digital marker and a manual marker as measured intraoperatively.
Methods: This was a prospective, single-site, comparative, observational study. Preoperative biometry and planning was assessed with the Argos SS-OCT biometer. All subjects received both digital and conventional marking. The ToriCAM application was used to mark the patient manually at the bedside. A Mendez marker was used to mark the final axis of the IOL, as calculated by Argos. Digital marking was performed using the VERION image guided system. The primary outcome measure was the difference in degrees between the digital marker and the manual marker as measured intraoperatively. Other outcome measures included IOL rotation, residual astigmatism, absolute prediction error (APE), and monocular visual acuity at 2 months postoperatively.
Results: A total of 41 eyes of 41 subjects completed the study. At 2 months postoperatively, the absolute difference in degrees between intraoperative digital and manual marking was 6.6 ± 5.2 (range 0.0 to 22.5). Mean absolute IOL rotation in degrees was 3.5 ± 2.9 (range 0.3 to 14.8) at 2 months. Mean postoperative residual astigmatism was 0.24 ± 0.24 D, and mean APE (spherical equivalent) was 0.39 ± 0.27 D. Mean monocular corrected distance visual acuity was 0.02 ± 0.05 logMAR.
Conclusion: Results suggest good postoperative refractive accuracy was achieved using Argos combined with a digital marker microscope. The manual marking was significantly misaligned when compared to the intended digital marking axis, which may cause significant postoperative residual astigmatism.
Keywords: digital marking, toric IOL, Argos, Clareon
Introduction
Postoperative residual astigmatism can severely impact patient outcomes and satisfaction following cataract surgery and intraocular lens (IOL) implantation. A large retrospective study reported that even small amounts (0.25 to 0.5 D) of residual astigmatism can affect visual acuity and satisfaction.1 Surgeons have a variety of tools to choose from to correct astigmatism, including toric IOLs, corneal incisions, or corneal refractive procedures.2–4
When implanting toric IOLs, it is important to have the axis of the lens placed exactly as intended, as each 1 degree misalignment can leave ~3% of the astigmatism uncorrected by scalar comparison of astigmatism magnitudes.5 Manual marking is a common approach to align the axis of the toric IOL. This is typically done preoperatively at the slit lamp, with the patient in a sitting position. While manual marking is regarded as the gold standard, it is prone to human error. In addition, cyclotorsion can cause patient eyes to rotate by up to 12 degrees when supine (compared to a seated position).6 New technologies have now enabled toric alignment to be done using digital image guidance, which may reduce human error and correct for cyclotorsion. Commercially available devices include the Callisto Eye with Z-Align (Carl Zeiss Meditec AG), SensoMotoric Instruments (SMI), and VERION Digital Marker (Alcon Vision, LLC).
The VERION Digital Marker (Alcon Vision, LLC) utilizes a pre-recorded registration image that captures key features of the eye, such as limbus and iris structures and conjunctival vasculature, to help align the toric IOL intraoperatively during surgery. It can also account for any posture-induced cyclotorsion and may reduce human error compared to manual marking. It is integrated in the Argos biometer (Movu, aSantec company), allowing measurements to be automatically incorporated into the surgical plan. Previous studies of the VERION Digital Marker have reported good outcomes following toric IOL implantation.7–9 However, to date there are minimal data on toric alignment and refractive accuracy using the Argos biometer and a digital marker microscope compared to manual marking.
The purpose of this study was to evaluate intraoperative degree alignment of the common toric manual marking method when compared to Argos combined with a digital marker microscope.
Methods
This was a prospective, comparative, observational study of intraoperative degree alignment of digital marking compared to manual marking. The study was reviewed and approved by an independent institutional review board (Salus IRB, approval # 24349). An independent IRB was used as the study was conducted in private practice. All subjects gave written informed consent. Good clinical practice, the tenets of the Declaration of Helsinki, and International Harmonization (ICH) guidelines were followed. The study was registered on clinicaltrials.gov (NCT07176897).
Inclusion criteria were adults (50–90 years of age) that were candidates for uncomplicated cataract surgery and planned to be implanted with toric IOLs (CCWOTx, Alcon Vision, LLC). Exclusion criteria were history of amblyopia, macular disease, glaucoma, corneal disease, prior corneal surgery, or diabetes, ocular comorbidity that might hamper post operative visual acuity, previous ocular or refractive surgery, expected post-op VA worse than 0.10 logMAR, irregular corneal astigmatism and keratoconus, or severe/uncontrolled ocular surface disease or dry eye disease.
Preoperative biometry was performed using the Argos, and the integrated Barrett Toric calculator was used for preoperative planning. The reference image for digital marking was also obtained during preoperative biometry acquisition. Each patient’s eye received both digital and manual marking. Preoperatively, patients were seated upright, the ToriCam smartphone app was used to identify the horizontal axis as a reference point, and the limbus was marked with a fine marking pen. The ToriCam reference points were then used during surgery to mark the cornea with the final calculated axis of the IOL with the Mendez marker intraoperatively. Digital tracking was performed using the VERION Image Guided System (Alcon Vision, LLC). The toric IOL was placed on the digital Verion axis using the heads up display to align the lens. Final IOL power, cylinder power, and axis of placement was confirmed with the Optiwave Refractive Analysis (ORA) System with Verifeye (Alcon Vision, LLC), however the IOL was always placed on the digital marker axis. The intraoperative photographic images were obtained for all patients, and the difference in angle and direction was recorded by comparing the Mendez marks to the digital marking axis. All subjects were implanted with Clareon monofocal toric IOLs (CCWOTx), and returned for a postoperative day 1 visit and a second postoperative visit between postoperative week 4 and 8. Postoperative photos were obtained at each visit using slit lamp photography. These images were then digitally compared to the reference images obtained by the Argos to measure any cyclotorsion at each follow up visit.
The primary outcome measure was the difference in degrees between the digital marker and the manual marker intraoperatively. Secondary endpoints were the percentage of eyes with residual astigmatism ≤ 0.25 D, ≤ 0.50 D, ≤ 0.75 D, ≤ 1.00 D, and ≤ 1.25 D. Exploratory endpoints included postoperative IOL rotation, absolute prediction error (APE), monocular uncorrected visual acuity at distance (UDVA) and near (UNVA), and monocular corrected distance visual acuity (CDVA). Spherical APE was calculated as the absolute difference between predicted spherical equivalent and the postoperative spherical equivalent. Cylinder APE was calculated as the absolute difference between predicted cylinder and the postoperative manifest cylinder. Back-calculations were also performed to determine the residual astigmatism had the IOL been implanted according to the manual marking. As the toric power was the same in both groups and the only difference between groups was the axis orientation, the residual astigmatism due to axis misalignment was back-calculated as the toric power at the spectacle plane (using a vertex distance of 13.75 mm) multiplied by sin(2 * absolute angle difference between digital and manual markings).5
It was estimated that 30 eyes would be needed to detect a difference of 0.20 between the percentage of eyes with postoperative residual astigmatism 0.5 D or less (85% compared to 65%), power of 85%, correlation between paired observations 0.80, and a two-sided significance of 5%.8,10 To account for dropout, a sample size of at least 35 eyes were targeted. Normality was verified using the Shapiro–Wilk test. A t-test was used to compare parametric data, while the Wilcoxon Signed Rank test was used for non-parametric data. The McNemar test was used to compare the percentage of eyes with postoperative residual astigmatism. All statistical analyses were performed using the software R (version 4.4.2; The R Foundation for Statistical Computing, Vienna, Austria). A fixed sequence methodology was used to evaluate the primary and secondary endpoints, in the following sequence: difference in degrees between manual and digital marking methods, percentage of eyes with cylinder ≤ 0.50 D, percentage of eyes with cylinder ≤ 0.25 D, percentage of eyes with cylinder ≤ 0.75 D, percentage of eyes with cylinder ≤ 1.00 D, and percentage of eyes with cylinder ≤ 1.25 D. The first endpoint in the sequence was tested at the full alpha level and testing stopped if an endpoint was not significant. A p < 0.05 was considered significant.
Results
A total of 41 eyes of 41 patients completed the study. Table 1 summarizes patient demographics and preoperative data. No adverse events occurred during the study that were related to the surgery or IOL.
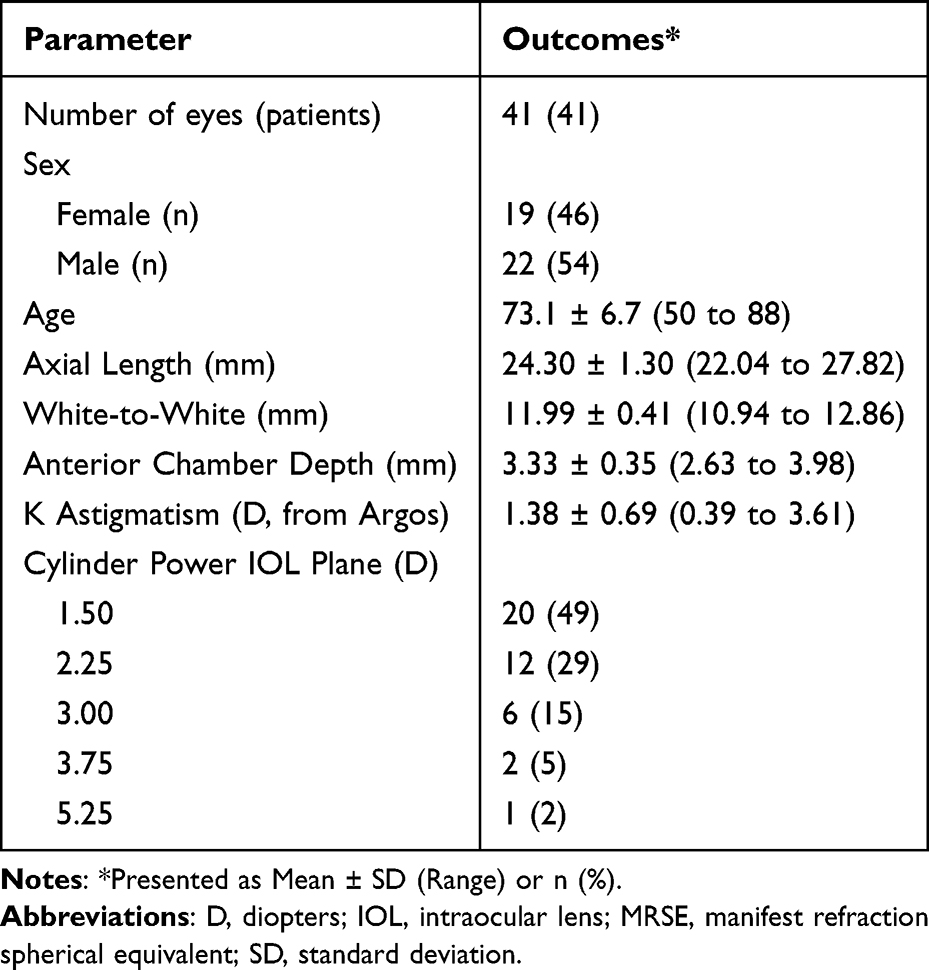 |
Table 1 Preoperative Data and Patient Demographics |
The directional difference in degrees between the digital and manual marking methods was −3.4 ± 7.7 (range −22.5 to 9.0), indicating a slight counterclockwise bias. The absolute difference in degrees between the digital and manual marking methods was 6.6 ± 5.2 (range 0.0 to 22.5). In addition, the absolute difference was 1 degree or less in 7% of eyes (3/41), 5 degrees or less in 51% of eyes (21/41), and 10 degrees or less in 80% of eyes (33/41). The absolute difference in degrees between the digital and manual marking methods in right eyes was 7.8 ± 5.9 compared to 4.5 ± 2.8 in left eyes (p = 0.02). The mean absolute IOL rotation in degrees between day 1 and the second postoperative visit was 3.5 ± 2.9 (range 0.3 to 14.8).
Table 2 summarizes the refractive outcomes. Back-calculated residual astigmatism was the theoretical residual astigmatism had the IOL been implanted according to the manual axis marking. Mean postoperative residual astigmatism was 0.24 ± 0.24 D, compared to 0.74 ± 0.53 D for back-calculated residual astigmatism (p < 0.001). In addition, 95% of eyes (39/41) had ≤ 0.5 D of postoperative residual astigmatism, compared to 37% (15/41) for back-calculated residual astigmatism (p < 0.001). Statistical significance was also observed for the percentages of eyes with residual astigmatism ≤ 0.25 D (p < 0.001), ≤ 0.75 D (p < 0.001), ≤ 1.00 D (p = 0.001), and ≤ 1.25 D (p = 0.02). Double angle vector plots for preoperative and postoperative astigmatism are shown in Figure 1.
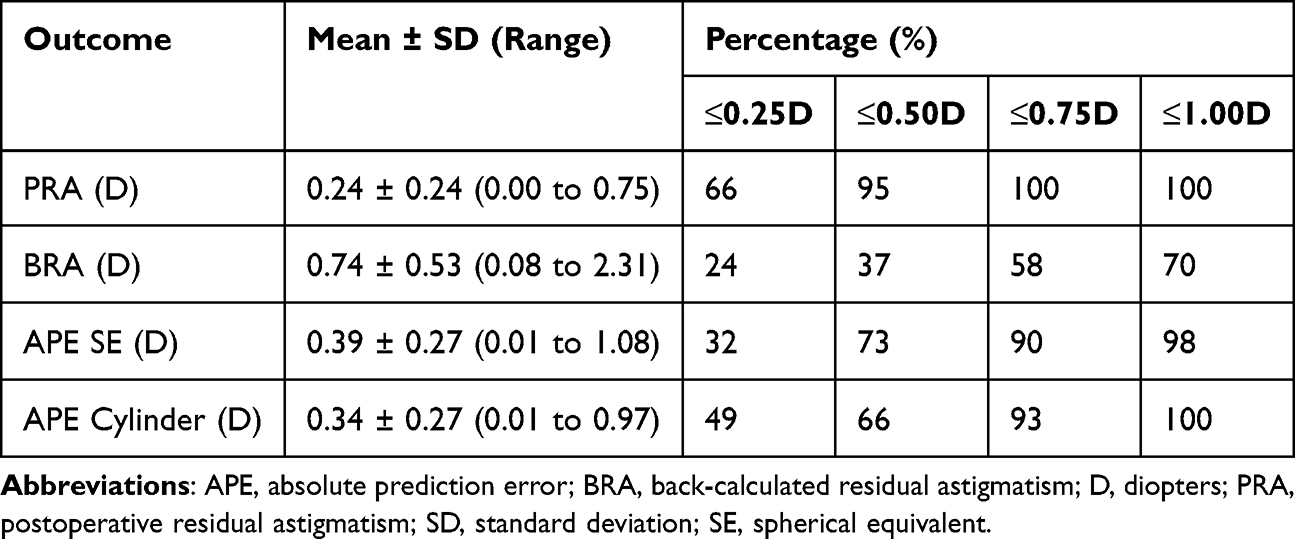 |
Table 2 Postoperative Actual and Theoretical Refractive Outcomes (n=41 Eyes) |
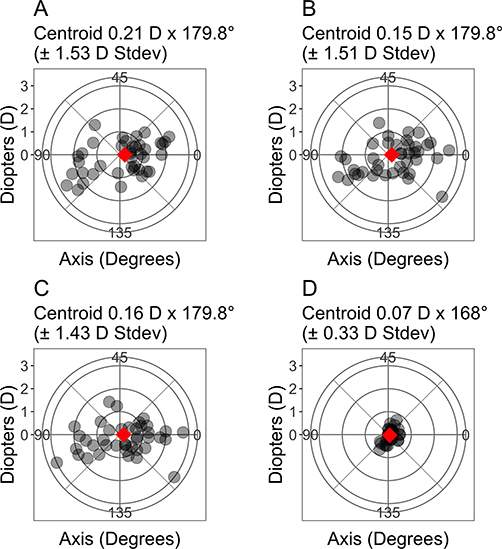 |
Figure 1 Preoperative Double Angle Vector Plots for (A) Argos, (B) Topography, (C) Keratometry, and (D) Postoperative Manifest Refraction. |
Visual outcomes are summarized in Table 3. A mixture of plano and myopia targets were included in the dataset, and have been summarized separately. However, overall postoperative mean monocular corrected distance visual acuity (CDVA) was 0.02 ± 0.05 logMAR, and 92% of eyes (38/41) were 20/25 or better.
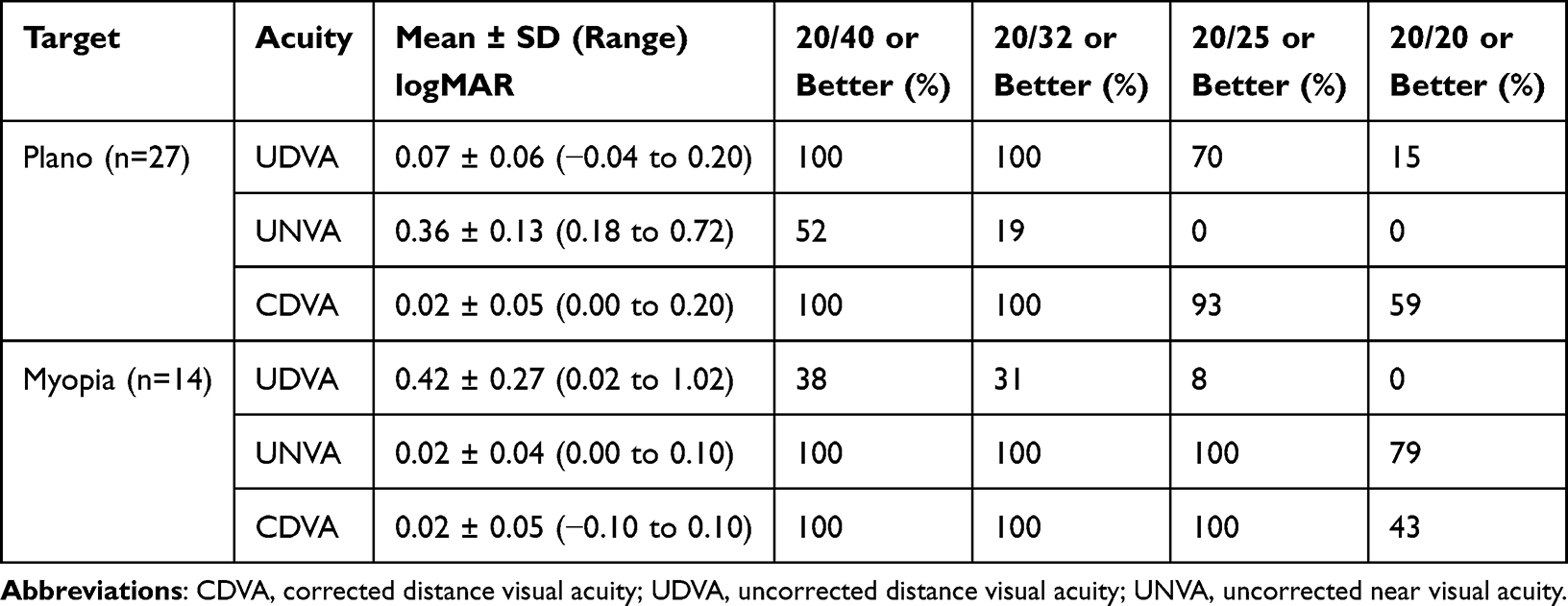 |
Table 3 Postoperative Visual Outcomes |
Discussion
To maximize postoperative outcomes for patients following cataract surgery, residual astigmatism should be minimized. It has been estimated that every diopter of postoperative residual astigmatism reduces distance visual acuity by 0.15 logMAR.11 Toric IOL alignment is a critical factor which can be done with manual or digital marking. In this study, we evaluated the postoperative refractive accuracy of the common toric manual marking method when compared to Argos combined with a digital marker microscope. To the best of our knowledge, this is the first report of outcomes with manual marking compared to Argos combined with a digital marker microscope.
In our study, the average absolute difference between the manual and digital marking methods was 6.6°. We are not aware of other studies that have reported specific differences between manual and digital marking. Generally, other studies report misalignment, which is a combination of missing the intended axis and IOL rotation. Nevertheless, it is worthwhile to compare our results to the misalignment results reported by other studies. Webers et al8 observed a difference in misalignment of 1.5° (p < 0.05) between manual and digital marking (VERION) methods, after 1 hour postoperatively, also in a randomized controlled trial. Elhofi and Helaly9 reported a difference in misalignment of 1.9° (p = 0.003) between manual and digital marking (VERION) methods, after 3 to 5 weeks postoperatively, in a randomized controlled trial. In addition, Shin et al7 observed a difference in misalignment of 2.6° (p < 0.001) between manual and digital marking (VERION) methods, after 1 hour postoperatively, in a retrospective study. In contrast, other studies have reported no significant differences in misalignment between digital (VERION) and manual marking methods, in a randomized controlled trials.10,12 It is also worth noting that other studies comparing manual marking to other digital marking systems have observed higher misalignment with manual marking.13–16
We back-calculated the residual astigmatism (BRA, manifest) had the toric IOL been aligned with the manual marking, and compared to the actual residual astigmatism (PRA, manifest). Mean PRA was significantly lower compared to BRA (0.24 D compared to 0.74 D) and the percentages of eyes with 0.5 D of astigmatism or less was significantly higher (95% compared to 37%). Kodavoor et al10 reported that the residual astigmatism was lower in the digital marking group (0.29 D) compared to the manual marking group (0.50 D). However, most other studies report no significant differences in residual astigmatism between digital (VERION) and manual marking.7–9,12 Differences between our study and others may be explained by the study design, patient populations, and the back-calculated values used in our study.
As the manual marking methods using weighted markers/ToriCAM or other bedside devices are acquired in the separate encounter from the patient’s preoperative reference images, we theorize that intrinsic variations in patient incline, cyclotorsion, and convergence results in a difference in toric alignment marks between the two modalities. The digital and manual marking methods are acquired in a different setting and the calculated intended toric axis is based on the preoperative image obtained by the Argos Biometer. Therefore simulating those exact conditions and reproducing the same reference marks is a challenge, and we theorize may lead to the difference we observed between digital and manual marking.
An interesting finding of our study was the dissimilarity between right and left eyes for the absolute difference between the manual and digital marking methods. However, a study by Rozema et al17 reported no differences in IOL rotation between right and left eyes. It is likely that differences in incisional behavior between right and left eyes may explain the disparity observed in our study.18
The main difference between our study and previous studies is that our study used subjects as their own controls, whereas previous studies used two independent groups. Using two independent groups does offer advantages, such as when comparing visual and refractive outcomes, and we acknowledge this is a limitation in our study. However, our study design allowed for a direct comparison of the difference in degrees between the digital and manual marking methods, without the confounding factor of IOL rotation. Another limitation of this study was the relatively short follow up time (56 days), which hinders our ability to draw long term conclusions about rotational stability and refractive outcomes.
Conclusions
The results of this study suggest good postoperative refractive accuracy was achieved using Argos combined with a digital marker microscope. In addition, the manual marking was significantly misaligned compared to the digital marking, which may cause significant postoperative residual astigmatism.
Data Sharing Statement
Data are not available for sharing.
Acknowledgments
This paper was presented at the 2024 and 2025 American Society of Cataract and Refractive Surgery (ASCRS) Annual Meeting as a conference talk with interim findings.
Funding
This study was supported with an investigator-initiated study grant (92162521) from Alcon Vision, LLC, Fort Worth, TX, USA.
Disclosure
Rom Kandavel reports that he has received consulting fees from Alcon Laboratories. Brad Hall reports independent contractor fees from Topcon Healthcare Inc. The authors report no other conflict of interest in this work.
References
1. Schallhorn SC, Hettinger KA, Pelouskova M, et al. Effect of residual astigmatism on uncorrected visual acuity and patient satisfaction in pseudophakic patients. J Cataract Refract Surg. 2021;47(8):991–7. doi:10.1097/j.jcrs.0000000000000560
2. Budak K, Friedman NJ, Koch DD. Limbal relaxing incisions with cataract surgery. J Cataract Refract Surg. 1998;24(4):503–508. doi:10.1016/S0886-3350(98)80292-7
3. Nubile M, Carpineto P, Lanzini M, et al. Femtosecond laser arcuate keratotomy for the correction of high astigmatism after keratoplasty. Ophthalmology. 2009;116(6):1083–1092. doi:10.1016/j.ophtha.2009.01.013
4. Mozayan E, Lee JK. Update on astigmatism management. Current Opinion in ophthalmology. 2014;25(4):286–290. doi:10.1097/ICU.0000000000000068
5. Ma JJ, Tseng SS. Simple method for accurate alignment in toric phakic and aphakic intraocular lens implantation. J Cataract Refract Surg. 2008;34(10):1631–1636. doi:10.1016/j.jcrs.2008.04.041
6. Terauchi R, Horiguchi H, Ogawa T, Shiba T, Tsuneoka H, Nakano T. Posture-related ocular cyclotorsion during cataract surgery with an ocular registration system. Sci Rep. 2020;10(1):2136. doi:10.1038/s41598-020-59118-9
7. Shin DE, Lee JM, Kim T-I, Seo KY, Koh K. Efficacy of the image-guided alignment system for a four-haptic hydrophobic monofocal toric intraocular lens. Eye & Contact Lens. 2022;48(9):396–402. doi:10.1097/ICL.0000000000000901
8. Webers VSC, Bauer NJC, Visser N, Berendschot TTJM, van den Biggelaar FJHM, Nuijts RMMA. Image-guided system versus manual marking for toric intraocular lens alignment in cataract surgery. J Cataract Refract Surg. 2017;43(6):781–788. doi:10.1016/j.jcrs.2017.03.041
9. Elhofi AH, Helaly HA. Comparison between digital and manual marking for toric intraocular lenses: a randomized trial. Medicine. 2015;94(38):e1618. doi:10.1097/MD.0000000000001618
10. Kodavoor SK, Divya J, Dandapani R, Ramamurthy C, Ramamurthy S, Sachdev G. Randomized trial comparing visual outcomes of toric intraocular lens implantation using manual and digital marker. Indian J Ophthalmol. 2020;68(12):3020–3024. doi:10.4103/ijo.IJO_465_20
11. Wolffsohn JS, Bhogal G, Shah S. Effect of uncorrected astigmatism on vision. J Cataract Refract Surg. 2011;37(3):454–460. doi:10.1016/j.jcrs.2010.09.022
12. Barberá-Loustaunau E, Basanta I, Vázquez J, et al. Time-efficiency assessment of guided toric intraocular lens cataract surgery: pilot study. J Cataract Refract Surg. 2021;47(12):1535–1541. doi:10.1097/j.jcrs.0000000000000688
13. Ding N, Wang X, Song X. Digital versus slit-beam marking for toric intraocular lenses in cataract surgery. BMC Ophthalmol. 2022;22(1):323. doi:10.1186/s12886-022-02548-y
14. Kim EC, Hwang KY, Lim SA, Yi R, Joo C-K. Accuracy of toric intraocular lens implantation using automated vs manual marking. BMC Ophthalmol. 2019;19(1):169. doi:10.1186/s12886-019-1175-1
15. Mayer WJ, Kreutzer T, Dirisamer M, et al. Comparison of visual outcomes, alignment accuracy, and surgical time between 2 methods of corneal marking for toric intraocular lens implantation. J Cataract Refract Surg. 2017;43(10):1281–1286. doi:10.1016/j.jcrs.2017.07.030
16. Titiyal JS, Kaur M, Jose CP, Falera R, Kinkar A, Bageshwar LM. Comparative evaluation of toric intraocular lens alignment and visual quality with image-guided surgery and conventional three-step manual marking. Clin Ophthalmol. 2018;12:747–753. doi:10.2147/OPTH.S164175
17. Rozema JJ, Gobin L, Verbruggen K, Tassignon MJ. Changes in rotation after implantation of a bag-in-the-lens intraocular lens. J Cataract Refract Surg. 2009;35(8):1385–1388. doi:10.1016/j.jcrs.2009.03.037
18. Alpins N, Ong JK, Stamatelatos G. Asymmetric corneal flattening effect after small incision cataract surgery. J Refract Surg. 2016;32(9):598–603. doi:10.3928/1081597X-20160608-01
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.