Back to Journals » International Journal of Women's Health » Volume 18
Intraoperative Collapse During First-Trimester Abortion: Hyperleukocytosis Crisis, Thrombotic Pulmonary Embolism, or Amniotic Fluid Embolism?
Authors Wen T ![]() , Zhang Y, Zhong Y, Song S
, Zhang Y, Zhong Y, Song S
Received 20 February 2026
Accepted for publication 7 July 2026
Published 14 July 2026 Volume 2026:18 604225
DOI https://doi.org/10.2147/IJWH.S604225
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Tingting Wen, Yu Zhang, Yushan Zhong, Shengwen Song
Department of Anesthesiology, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Tingting Wen, Department of Anesthesiology, The First Affiliated Hospital, Zhejiang University School of Medicine, 1367 West Wenyi Road, Hangzhou, Zhejiang, 310000, People’s Republic of China, Email [email protected]
Background: Hyperleukocytosis in patients with hematologic malignancies poses significant perioperative risks, including leukostasis, coagulopathy, tumor lysis syndrome and hyperinflammatory syndrome. Additionally, pregnancy and hyperleukocytosis predispose patients to a hypercoagulable state, increasing the risk of thrombosis. On the other hand, amniotic fluid embolism (AFE) is a rare but serious complication of pregnancy. Although distinct in etiology, thrombotic pulmonary embolism (PE), AFE, and hyperleukocytosis crisis can present with a strikingly similar clinical picture of pulmonary hypertension and respiratory failure, posing a significant diagnostic challenge in the perioperative setting.
Case Presentation: An 18-year-old female with chronic phase chronic myeloid leukemia and hyperleukocytosis (WBC > 100× 109/L) underwent medical termination of pregnancy followed by emergency dilation and curettage. Intraoperatively, she developed acute hypoxemia, hypotension, and cardiac arrest. Resuscitation was successful, but she exhibited severe pulmonary hypertension, respiratory failure and DIC. The initial diagnosis of large thrombotic pulmonary and AFE was ultimately reconsidered in favor of a hyperleukocytosis crisis, based on three key observations: pulmonary angiography revealed no central, lobar, or segmental filling defects, the resolution of pulmonary hypertension closely paralleled a reduction in leukocyte count two weeks later, and there was an absence of uterine atony and massive uterine bleeding despite profound DIC. Though histopathological confirmation is lacking, pulmonary leukostasis remains the most likely explanation for the patient’s cardiopulmonary collapse. The patient survived after prolonged intensive care unit care, including mechanical ventilation, renal replacement therapy, and cytoreductive treatment.
Conclusion: Anesthesia and surgical interventions in patients with hyperleukocytosis pose a formidable challenge, which could cause life threatening complications and need vigilance care. Given hyperleukocytosis crisis can present with clinical features indistinguishable from thrombotic pulmonary embolism and AFE, recognizing this distinction is critical for guiding appropriate treatment and optimizing perioperative outcomes.
Keywords: hyperleukocytosis, leukostasis, pulmonary hypertension, pulmonary embolism, amniotic fluid embolism
Introduction
Patients with hematological malignancies represent a high-risk population for perioperative complications, particularly those presenting with hyperleukocytosis—commonly defined as a white blood cell (WBC) count exceeding 100×109/L.1 This condition predisposes patients to several life-threatening complications, the most common of which include leukostasis, coagulopathy, and tumor lysis syndrome. In chronic-phase chronic myeloid leukemia (CML) (blast cells <10%), however, overt leukostasis is relatively uncommon, likely because mature myeloid cells are smaller and more deformable.2 Nevertheless, a white blood cell (WBC) count above 100 × 109/L is per se a well-recognized risk factor for leukostasis in CML.3 Kurosawa et al reported 21 leukostasis events in 192 chronic-phase CML children,4 and several case reports have documented similar presentations.5–7 Rarely, hyperinflammatory syndrome can also be seen. Early recognition and proactive management of these potential crises are essential in the perioperative care of such patients.
Pregnancy induces a progressive hypercoagulable state that begins as early as 5 weeks after pregnancy. This state is driven by a rise in procoagulant factors (including fibrinogen, factors V, VII, VIII, X, XII, and von Willebrand factor), an increase in plasminogen activator inhibitors (PAI-1 and PAI-2) that impair fibrinolysis, and a concomitant decrease in free protein S along with the development of acquired activated protein C resistance.8,9 Although thrombotic pulmonary embolism (PE) in early pregnancy is rare, hyperleukocytosis—an independent thrombotic risk factor—may substantially amplify the overall prothrombotic burden.10
Amniotic fluid embolism (AFE) is a rare but serious complication of pregnancy with an incidence of 0.8–7.7 in every 100000 pregnancies and with a maternal mortality of 10–17%.11 The entry of amniotic fluid and fetal debris into the maternal circulation serves as both a mechanical insult and a potent initiator of an anaphylactoid-like response.12 This reaction rapidly unleashes a cascade of proinflammatory mediators and pro-coagulants, resulting in multisystem organ failure and severe coagulopathy. It is characterized by sudden cardiovascular collapse, respiratory distress, and disseminated intravascular coagulation (DIC).13
We report a case of a patient with newly diagnosed chronic phase CML who most likely experienced an intraoperative hyperleukocytosis crisis during a first-trimester termination of pregnancy. She presented with acute pulmonary hypertension, hemodynamic collapse and DIC. This report aims to elucidate the distinct pathophysiology of thrombotic PE, AFE, and hyperleukocytosis crisis, and to outline the essential perioperative management strategies specific to patients with extreme leukocytosis.
The case report was approved by the institutional ethics committee of the First Affiliated Hospital, Zhejiang University School of Medicine (IIT Ethics Approval No. 0156). Written informed consent for the publication of this case report was obtained from the patient.
Case Presentation
Preoperative Course
An 18-year-old female, gravida 3 para 1 at 8 weeks of gestation, was admitted to hematology with a 7-day history of fever and an initial leukocyte count of 280 x 109/L. Bone marrow aspiration investigations confirmed the diagnosis of BCR-ABL positive CML in chronic phase with 3% of blasts, and the patient presented with significant leukocytosis (WBC 245 x 109/L), anemia (hemoglobin 76 g/L), and thrombocytosis (platelet 939 x 109/L). She was otherwise healthy and asymptomatic. After initial management with hydroxyurea, flumatinib for 6 days, her leukocyte count decreased to 118 x 109/L. Due to the teratogenic risk of ongoing CML therapy, a medical termination of pregnancy was initiated at 10 weeks with mifepristone and misoprostol. Due to incomplete expulsion of products of conception, an emergency dilation and curettage (D and C) was scheduled at 10 week and 1 day of pregnancy.
Intraoperative Crisis
Upon arrival in the operating room, her vital signs were stable with non-invasive blood pressure (BP) of 110/63 mmHg, heart rate (HR) of 80 bpm, and saturation of peripheral oxygen (SpO2) was 97% on room air. The electrocardiogram (ECG) was normal. Anesthesia was induced with 0.5 mg of hydromorphone and 100 mg propofol. She was then maintained by propofol infusion. Approximately 10 minutes after anesthesia induction, immediately following completion of the curettage, she developed acute hypoxemia (SpO2 65%) and severe hypotension (BP 45/22 mmHg), rapidly progressing to ventricular tachycardia and fibrillation. Cardiopulmonary resuscitation, endotracheal intubation, and adrenaline administration was started, with return of spontaneous circulation after 10 minutes. Following resuscitation, invasive hemodynamic monitoring was established. A notably elevated central venous pressure of 25 mmHg was recorded via the internal jugular line. Concurrently, the initial arterial blood gas analysis yielded the following values: pH 6.943, pCO2 37.4 mmHg, K⁺ 5.7 mmol/L, Ca2⁺ 1.75 mmol/L, lactate 12.1 mmol/L, glucose 18.3 mmol/L, base excess −24 mmol/L. Point-of-care echocardiography revealed right ventricular dilatation with a D-shaped septum (Figure 1A), severe biventricular akinesia, and a tricuspid regurgitation velocity of 3.17 m/s (Figure 1B), yielding an estimated pulmonary artery pressure of 65 mmHg, raising suspicion for PE. Meanwhile, bilateral lower extremity venous ultrasound was negative for deep vein thrombosis by point of care ultrasound in the operating room. She was then transferred to the hybrid operating room for possible thrombolysis or mechanical thrombectomy. Pulmonary angiography showed no obvious central, lobar, or segmental intraluminal filling defects but noted hypoperfusion in the right middle and upper lung fields (Figure 1C). Thus, large vessel thrombotic PE was considered unlikely as the direct cause of the collapse. Though subsegmental PE could not be excluded since computed tomography pulmonary angiography (CTPA) was not performed for this patient. No intervention was considered feasible by the surgical team. Coagulation studies were sent to the lab and returned approximately 30 minutes later, revealing severe coagulopathy: APTT 99s, PT 30s, INR 3.0, and fibrinogen 0.72 mg/L. D-dimer levels also increased and peaked at 5 hours after collapse (88,000 mg/L). Amniotic fluid embolism was then suspected at this time. An estimated 200 mL of blood was lost during the 3 hours’ time in the operating room.
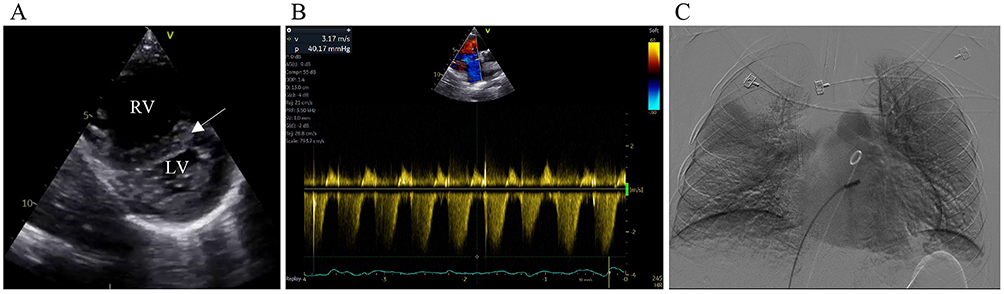 |
Figure 1 Perioperative echocardiographic and angiographic findings. (A) Transthoracic echocardiography showing right ventricular dilatation with a D-shaped septum (arrow), indicative of RV pressure overload. (B) Continuous-wave Doppler echocardiography across the tricuspid valve revealing a peak tricuspid regurgitation velocity of 3.17 m/s. Based on the simultaneously measured central venous pressure of 25 mmHg, the estimated pulmonary artery systolic pressure was approximately 65 mmHg. (C) Pulmonary angiography demonstrating hypoperfusion in the right middle and upper lung fields, without evidence of obvious central embolic masses. Abbreviations: RV, right ventricle; LV, left ventricle. |
Postoperative Course
The patient was transferred to the ICU in critical condition with multi-organ dysfunction syndrome (MODS). Her clinical manifestations encompassed encephalopathy (Glasgow coma scale score: E1VTM1), myocardial injury with troponin I elevation, hepatic injury with marked alanine aminotransferase (ALT) and aspartate aminotransferase elevation, and acute kidney injury necessitating continuous renal replacement therapy (CRRT). Laboratory investigations revealed a marked leukocytosis, with a peak WBC count of 346 x 109/L (Figure 2A). Because progression from chronic phase to accelerated or blast phase typically takes months to years, repeat marrow examination during the short postoperative period was not clinically indicated. Additionally, there was a significant cytokine surge, characterized by markedly elevated levels of IL-8, IL-1β, IL-6, and IL-10, while levels of TNF-α, IFN-α, IFN-γ, IL-17A, IL-2, IL-4, and IL-5 remained within the normal range.
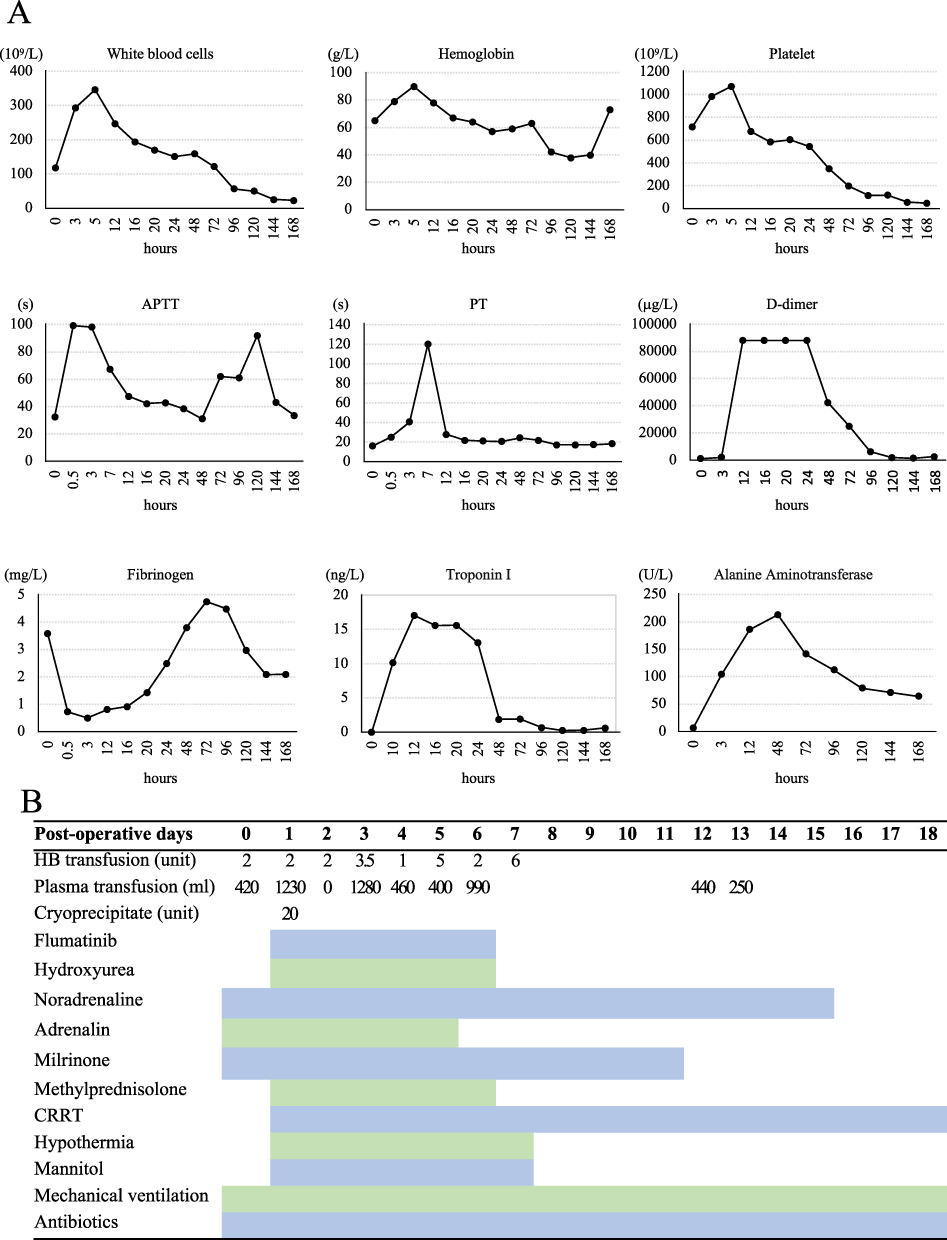 |
Figure 2 Postoperative trends of laboratory parameters and major therapeutic interventions. (A) Serial changes in white blood cell count (WBC), hemoglobin (Hb), platelet count (PLT), activated partial thromboplastin time (APTT), prothrombin time (PT), fibrinogen, D‑dimer, cardiac troponin I (TnI), and alanine aminotransferase (ALT) measured from immediately after surgery to 168 hours postoperatively. The x‑axis is shown in hours, with each parameter plotted on its own scale. (B) Timeline of key therapeutic strategies administered during the acute intensive care phase from post-operative day (POD) 0 to 18. The shaded background indicates the duration of intensive care support. The specific interventions comprised: transfusion of packed red blood cells, fresh frozen plasma, and cryoprecipitate for correction of coagulopathy; neuroprotective measures including therapeutic hypothermia, mannitol for intracranial pressure reduction, and corticosteroids; continuous renal replacement therapy (CRRT); mechanical ventilation. Note that the x‑axis in Panel B is truncated at POD 18 for clarity; however, the actual durations of CRRT, mechanical ventilation extended to POD 38 and POD 31, respectively. |
A multidisciplinary team was gathered for her condition, and her intensive care management was multifaceted. Underlying leukemia and hyperleukocytosis were managed with continued aggressive hydroxyurea and flumatinib treatment, as leukapheresis was precluded by hemodynamic instability. Notably, her complicating pulmonary hypertension resolved as her leukocyte count fell below 25×109/L after two weeks. At this point, this constellation of findings suggested a diagnosis of a hyperleukocytosis crisis complicated by pulmonary leukostasis, a systemic hyperinflammatory syndrome, and DIC. Pulmonary leukostasis was most likely responsible for her intraoperative collapse.
For hemodynamic support, she required prolonged infusion of milrinone (11 days), noradrenaline (15 days), and adrenaline (5 days). Coagulopathy was managed with substantial blood product replacement (Figure 2B). Despite the severity of DIC, uterine bleeding was not excessive, totaling approximately 550 mL within the first 48 hours and ceasing by postoperative day 7 (POD 7).
Cerebral CT revealed diffuse brain edema on postoperative day 1, which was most likely attributed to cardiopulmonary collapse with resultant hypoxic-ischemic encephalopathy. To mitigate neurological injury, mild therapeutic hypothermia (34–35°C), a cooling helmet, and corticosteroids were used. The patient regained consciousness on POD 15.
She also experienced two episodes of respiratory infection from POD 6–8 and POD 19–24. Sputum next generation sequencing detected Ureaplasma urealyticum. Blood cultures at POD 26 yielded Abiotrophia defectiva. Antibiotic therapy was escalated accordingly, and the patient subsequently made a full clinical recovery from infection.
She was successfully extubated following 31 days of mechanical ventilation, and was discharged from the ICU after a 37-day stay. With a total hospitalization of 99 days, she was ultimately discharged without neurological sequelae but with renal failure requiring hemodialysis.
Discussion
Determining the etiology of acute perioperative cardiorespiratory collapse poses a significant diagnostic challenge. We report a challenging case that was difficult to initially differentiate among a thrombotic PE, hyperleukocytosis crisis and AFE. This diagnostic uncertainty forms the basis of the following discussion, which will compare the pathophysiology, clinical features, and management strategies of these conditions.
Pathophysiology of Hyperleukocytosis Crisis for Our Patient
CML is a myeloproliferative neoplasm mostly driven by the Philadelphia chromosome—a reciprocal translocation t(9;22)(q34;q11) that generates the BCR::ABL1 fusion oncogene.14 The resulting constitutively active tyrosine kinase promotes uncontrolled myeloid proliferation, reduced apoptosis, and altered cell adhesion, primarily within the bone marrow. While modern tyrosine kinase inhibitors effectively target this pathway and normalize leukocyte counts, perioperative risks in CML patients remain clinically significant.15
The pathophysiology of leukostasis is characterized not only by high leukocyte counts but also by increased adhesion of these cells to the endothelium.16 The resulting hyperviscosity impairs microcirculatory flow, leading to tissue hypoxia and organ dysfunction—most notably in the lungs, central nervous system, kidneys, and heart.
Surgery and general anesthesia introduce multiple superimposed stresses that can significantly amplify the risk of microvascular leukostasis, even at WBC counts that might otherwise be tolerated. Preoperative fasting and fluid restriction inevitably lead to reduced intravascular volume and increased blood viscosity. This is particularly critical because vigorous hydration is a primary therapeutic measure for managing hyperleukocytosis—withholding it effectively negates one of the key protective interventions. Anesthesia-related hypoxemia promotes pulmonary vasoconstriction and slows microcirculatory flow, while hypotension reduces perfusion pressure. Both conditions prolong the transit time of leukemic blasts through the pulmonary microvasculature and increase the likelihood of adhesion and occlusion. Tissue injury and catecholamine release further activate endothelial cells, upregulating adhesion molecules and promoting leukocyte-endothelial interaction.17 Another factor that could amplify these risks is postoperative infection, which activates leukocytes.18 Nevertheless, no evidence-based guideline currently defines a clearly “safe” WBC count for elective surgery in patients with hyperleukocytosis.
For our patient, we propose the following sequence of events: Pre-existing subclinical leukostasis and increased metabolic demand from proliferating leukemic cells reduced the patient’s pulmonary oxygen reserve. Anesthesia-induced hypotension and hypoxemia then exacerbated leukocyte sludging and pulmonary vasoconstriction, precipitating acute pulmonary hypertension and subsequent right heart failure. This underscores the importance of maintaining normovolemia, adequate perfusion pressure, and oxygenation throughout the perioperative period.
Pulmonary leukostasis-induced pulmonary hypertension, which aligns with group 4.2 PH according to the 7th World Symposium on Pulmonary Hypertension,19 remains largely underinvestigated. Not all patients with pulmonary leukostasis develop pulmonary hypertension;20,21 its occurrence likely correlates with the acuteness of onset, the extent of pulmonary vascular occlusion and the severity of microvascular involvement. Autopsy findings of pulmonary leukostasis reveal extensive leukocyte infiltration in pulmonary arteries, arterioles, capillaries, and venules.22
Hyperleukocytosis itself is a well-known risk factor for DIC and the risk of DIC is even higher in leukostasis.23 Although the mechanism was mostly studied in AML and acute promyelocytic leukemia (APL), the fundamental pathways are likely applicable to condition with massive leukemic cell burden and turnover. Specifically, high cell turnover releases abundant tissue factor from leukemic blasts and activated leukocytes.24 Tissue factor activates the extrinsic pathway via factor VII, leading to thrombin generation, platelet and coagulation factor consumption, and microvascular fibrin deposition. In addition, cytokines (eg, IL-1β, IL-6, TNF-α) and enzymes released from leukemic cells promote hemorrhage by disrupting endothelial integrity.25 Hyperfibrinolysis is also common in hyperleukocytosis due to elevated plasminogen activator and reduced plasminogen activator inhibitor activity.23
The patient’s impaired consciousness was most likely due to hypoxic-ischemic encephalopathy. This is distinct from the classic cerebral leukostasis, which typically presents as focal hemorrhage and carries the highest mortality among all hyperleukocytosis-related complications.26 The patient regained consciousness at postoperative day 15 and discharged without neurological sequalae. Meanwhile, her renal failure was multifactorial, with possible contributions from renal leukostasis, severe cardiopulmonary collapse causing renal hypoperfusion, high-dose vasopressor support, massive cytokine release, postoperative infection, and the use of multiple antibiotics.
Differential Diagnosis of Hyperleukocytosis Crisis: Thrombotic PE and Amniotic Fluid Embolism
Initially, the patient’s intraoperative collapse raised strong concern for thrombotic PE, prompting transfer to the hybrid operating room for possible endovascular or surgical intervention. However, angiography revealed no central, lobar, or segmental filling defects. Moreover, subsegmental thrombi—even if angiographically occult—cannot explain the severity of her hemodynamic collapse, particularly in the absence of baseline dyspnea or hypoxemia. This clinical-radiological discordance, together with her dramatic improvement after leukoreduction, effectively excludes massive or submassive thrombotic PE as the primary cause.
While AFE more commonly occurs in full-term deliveries, it rarely can occur following abortion.27 It remained a leading diagnostic consideration for our patient given the obstetric setting and the presentation of acute respiratory and circulatory failure, pulmonary hypertension, and DIC. A report on pregnancy-related mortality in the United States (2011–2013) documented 111 deaths attributed to AFE, including one case following abortion;28 other case reports have similarly described AFE occurring in the first or second trimester. The definitive diagnosis of AFE relies on the postmortem identification of fetal debris (eg, squamous cells, mucin, lanugo hair) in the maternal pulmonary circulation. In surviving patients, however, the diagnosis is clinical and based on exclusion—much like the diagnosis of pulmonary leukostasis in our patient, which also lacks a definitive antemortem test.
Although the clinical presentation in this case was consistent with AFE, the following two key observations strongly support the diagnosis of hyperleukocytosis crisis. First, resolution of pulmonary hypertension paralleled leukocyte count reduction. The patient’s pulmonary hypertension resolved gradually only as her white blood cell count decreased below 25×109/L, a pattern not typical of AFE, in which pulmonary hypertension usually improves more rapidly—often within days—independent of cytoreduction. Second, the patient had severe DIC without severe hemorrhage. Even though 9.5 units of red blood cells were transfused in the first three days to our patient, the reduced blood hemoglobin level is a result of both uterine hemorrhage and, to a greater extent, chemotherapy-induced myelosuppression.
This case highlights that disseminated intravascular coagulation (DIC) alone does not fully explain massive hemorrhage during abortion or amniotic fluid embolism (AFE). Although the patient met laboratory criteria for severe DIC, significant bleeding—particularly uterine hemorrhage—was not a prominent feature. In contrast, DIC in AFE is typically accompanied by profuse hemorrhage resulting from combined coagulopathy and uterine atony.29 Thus, uterine atony appears to be a key contributor to uterine bleeding in AFE. Consistent with our findings, several reports have demonstrated a strong association between uterine atony and AFE, mediated by mast cell-derived mediators (histamine, bradykinin, and cytokines) that cause uterine muscle edema and impair myometrial contraction.11,30,31 The concept that DIC results in excessive bleeding after delivery in AFE should also be challenged. We propose that this anaphylactoid reaction is organ-specific, predominantly involving the pulmonary vasculature, coagulation system, and uterus, with potential involvement of the cardiac and cerebral systems as well. Early recognition of uterine atony constitutes a critical component of AFE care and warrants more proactive intervention.
This report has several limitations. First, as a single case report, the generalizability of the findings is inherently limited. Definitive diagnoses of AFE and pulmonary leukostasis would require histopathological confirmation, which was not available. Tryptase and complement levels for AFE diagnosis were also not measured.32 Furthermore, thrombotic PE—particularly at the subsegmental level—cannot be completely excluded. Therefore, we present hyperleukocytosis crisis as the most clinically plausible diagnosis rather than a definitive one. A comparative table (Table 1) has been included to help readers distinguish among the three entities.
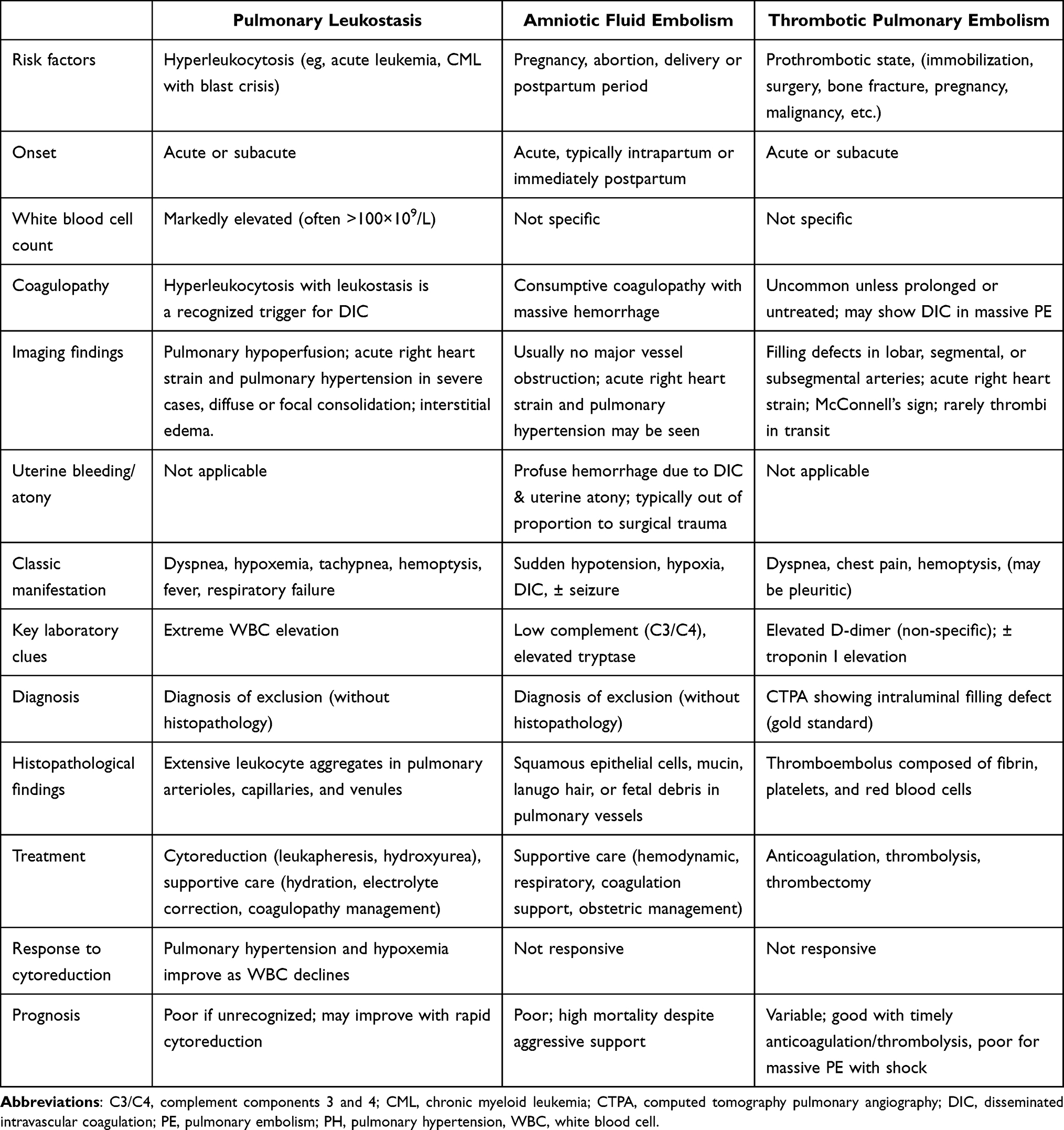 |
Table 1 Differential Diagnosis of Pulmonary Leukostasis, Amniotic Fluid Embolism and Thrombotic Pulmonary Embolism |
Conclusion
Patients with hyperleukocytosis are at exceptionally high risk during anesthesia and surgery, requiring heightened vigilance due to life-threatening complications. Although histopathological confirmation is lacking—thrombotic PE and AFE cannot be definitely excluded—pulmonary leukostasis remains the most clinically plausible explanation for the patient’s intraoperative collapse. Hyperleukocytosis crisis can mimic thrombotic PE and AFE through overlapping symptoms of pulmonary hypertension, systemic inflammation, and coagulopathy. Recognizing the pathophysiological distinction is essential for guiding appropriate perioperative management in this high-risk patient population.
Data Sharing Statement
Data is provided within the manuscript.
Ethics Approval and Informed Consent
The case report was approved by the institutional ethics committee of the First Affiliated Hospital, Zhejiang University School of Medicine (IIT Ethics Approval No. 0156).
Consent for Publication
Informed consent for the publication of this case report was obtained from the patient.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests in this work.
References
1. Macaron W, Sargsyan Z, Short NJ. Hyperleukocytosis and leukostasis in acute and chronic leukemias. Leuk Lymphoma. 2022;63(8):1780–9. doi:10.1080/10428194.2022.2056178
2. Lichtman MA, Rowe JM. Hyperleukocytic leukemias: rheological, clinical, and therapeutic considerations. Blood. 1982;60(2):279–283. doi:10.1182/blood.V60.2.279.279
3. Ali AM, Mirrakhimov AE, Abboud CN, Cashen AF. Leukostasis in adult acute hyperleukocytic leukemia: a clinician’s digest. Hematol Oncol. 2016;34(2):69–78. doi:10.1002/hon.2292
4. Kurosawa H, Tanizawa A, Tono C, et al. Leukostasis in children and adolescents with chronic myeloid leukemia: japanese pediatric leukemia/lymphoma study group. Pediatr Blood Cancer. 2016;63(3):406–411. doi:10.1002/pbc.25803
5. Jeon WJ, Dalal S, Moon JH, et al. Leukostasis with isolated central nervous system involvement in chronic phase of chronic myelogenous leukemia. J Hematol. 2023;12(4):187–196. doi:10.14740/jh1150
6. Raghuwanshi B, Chouhan S, Jain A. Leukocytapheresis in chronic myeloid leukemia with leukostasis. Cureus. 2020;12(12):e12375. doi:10.7759/cureus.12375
7. Takahashi N, Sano H, Mochizuki K, Kobayashi S, Ohara Y, Kikuta A. Intracranial hemorrhage in a pediatric patient with chronic myeloid leukemia in chronic phase: a case report. Case Rep Oncol. 2021;14(1):525–530. doi:10.1159/000515011
8. Rosenkranz A, Hiden M, Leschnik B, et al. Calibrated automated thrombin generation in normal uncomplicated pregnancy. Thromb Haemost. 2008;99(2):331–337. doi:10.1160/TH07-05-0359
9. Brenner B. Haemostatic changes in pregnancy. Thromb Res. 2004;114(5–6):409–414. doi:10.1016/j.thromres.2004.08.004
10. Castelli R, Ferrari B, Cortelezzi A, Guariglia A. Thromboembolic complications in malignant haematological disorders. Curr Vasc Pharmacol. 2010;8(4):482–494. doi:10.2174/157016110791330799
11. Mazza GR, Youssefzadeh AC, Klar M, et al. Association of pregnancy characteristics and maternal mortality with amniotic fluid embolism. JAMA Network Open. 2022;5(11):e2242842. doi:10.1001/jamanetworkopen.2022.42842
12. Tamura N, Farhana M, Oda T, Itoh H, Kanayama N. Amniotic fluid embolism: pathophysiology from the perspective of pathology. J Obstet Gynaecol Res. 2017;43(4):627–632. doi:10.1111/jog.13284
13. Clark SL, Romero R, Dildy GA, et al. Proposed diagnostic criteria for the case definition of amniotic fluid embolism in research studies. Am J Obstet Gynecol. 2016;215(4):408–412. doi:10.1016/j.ajog.2016.06.037
14. Kamizela AE, Leongamornlert D, Williams N, et al. Timing and trajectory of BCR::ABL1-driven chronic myeloid leukaemia. Nature. 2025;640(8060):982–990. doi:10.1038/s41586-025-08817-2
15. Guilhot F, Hehlmann R. Long-term outcomes of tyrosine kinase inhibitors in chronic myeloid leukemia. Blood. 2025;145(9):910–920. doi:10.1182/blood.2024026311
16. Röllig C, Ehninger G. How I treat hyperleukocytosis in acute myeloid leukemia. Blood. 2015;125(21):3246–3252. doi:10.1182/blood-2014-10-551507
17. Fan X, Yang G, Yang Z, et al. Catecholamine induces endothelial dysfunction via Angiotensin II and intermediate conductance calcium activated potassium channel. Biomed Pharmacother. 2024;177:116928. doi:10.1016/j.biopha.2024.116928
18. Hidou M, Caramella JP, Deletang D, Claude E, Strouk R. Poumon hyperleucocytaire postopératoire responsable d’une détresse respiratoire fatale [Postoperative pulmonary leukostasis responsible for fatal respiratory distress]. Ann Fr Anesth Reanim. 1990;9(4):390–392. doi:10.1016/s0750-7658(05)80254-0
19. Kovacs G, Bartolome S, Denton CP, et al. Definition, classification and diagnosis of pulmonary hypertension. Eur Respir J. 2024;64(4):2401324. doi:10.1183/13993003.01324-2024
20. Snyder AB, Barone JG, DiGiacomo JC, Barone JE. Postoperative pulmonary leukostasis. Crit Care Med. 1990;18(1):116–117. doi:10.1097/00003246-199001000-00024
21. Pryds K, Rasmussen LE, Andersen NH. Fatal right-sided heart failure due to leukostasis in a patient with leukemic transformation of myelodysplastic syndrome. Clin Case Rep. 2018;7(1):115–119. doi:10.1002/ccr3.1929
22. Kaminsky DA, Hurwitz CG, Olmstead JI. Pulmonary leukostasis mimicking pulmonary embolism. Leuk Res. 2000;24(2):175–178. doi:10.1016/s0145-2126(99)00162-9
23. Franchini M, Di Minno MN, Coppola A. Disseminated intravascular coagulation in hematologic malignancies. Semin Thromb Hemost. 2010;36(4):388–403. doi:10.1055/s-0030-1254048
24. Dicke C, Amirkhosravi A, Spath B, et al. Tissue factor-dependent and -independent pathways of systemic coagulation activation in acute myeloid leukemia: a single-center cohort study. Exp Hematol Oncol. 2015;4(1):22. doi:10.1186/s40164-015-0018-x
25. Stefanidakis M, Karjalainen K, Jaalouk DE, et al. Role of leukemia cell invadosome in extramedullary infiltration. Blood. 2009;114(14):3008–3017. doi:10.1182/blood-2008-04-148643
26. Owattanapanich W, Auewarakul CU. Intracranial hemorrhage in patients with hematologic disorders: prevalence and predictive factors. J Med Assoc Thai. 2016;99(1):15–24.
27. Bridwell RE, Long B, Montrief T, Gottlieb M. Post-abortion complications: a narrative review for emergency clinicians. West J Emerg Med. 2022;23(6):919–925. doi:10.5811/westjem.2022.8.57929
28. Creanga AA, Syverson C, Seed K, Callaghan WM. Pregnancy-related mortality in the United States, 2011-2013. Obstet Gynecol. 2017;130(2):366–373. doi:10.1097/AOG.0000000000002114
29. Matsuda Y, Kamitomo M. Amniotic fluid embolism: a comparison between patients who survived and those who died. J Int Med Res. 2009;37(5):1515–1521. doi:10.1177/147323000903700529
30. Tamura N, Nagai H, Maeda H, et al. Amniotic fluid embolism induces uterine anaphylaxis and atony following cervical laceration. Gynecol Obstet Invest. 2014;78(1):65–68. doi:10.1159/000360537
31. Gentilomo A, Tambuzzi S, Gentile G, Boracchi M, Andreola S, Zoia R. Post-mortem diagnosis of amniotic fluid embolism. Autops Case Rep. 2024;14:e2024472. doi:10.4322/acr.2024.472
32. Benson MD. Current concepts of immunology and diagnosis in amniotic fluid embolism. Clin Dev Immunol. 2012;2012:946576. doi:10.1155/2012/946576
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.