Back to Journals » Clinical Ophthalmology » Volume 19
Intraocular Pressure Spikes Following Cataract Extraction: Hydrophobic vs Hydrophilic Acrylic Lenses
Authors Micheletti E, Khan AJ
Received 16 June 2025
Accepted for publication 10 November 2025
Published 3 December 2025 Volume 2025:19 Pages 4387—4395
DOI https://doi.org/10.2147/OPTH.S544933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Eleonora Micheletti,1,2 Abdul Jabbar Khan1
1Department of Ophthalmology, Lincolnshire United Hospitals NHS Trust, Lincoln, UK; 2Moorfields Eye Hospital NHS Foundation Trust, London, UK
Correspondence: Eleonora Micheletti, Moorfields Eye Hospital NHS Foundation Trust, 162 City Road, London, EC1V 2PD, UK, Email [email protected]
Purpose: To investigate the intraocular pressure (IOP) changes after cataract extraction (CE) with an acrylic hydrophobic EyeCee One versus a hydrophilic Akreos MI60 intraocular lens (IOL) implant.
Methods: All patients who underwent CE with acrylic EyeCee One IOL implant and Akreos MI60 IOL implants were included. Parameters such as age, sex, history of glaucoma or ocular hypertension (OHT), IOP, axial length (AXL), anterior chamber depth (ACD) and type of IOL implant were measured.
Results: A total of 193 eyes of 193 patients were included. Of them, 115 eyes underwent CE with EyeCee One IOL, while 78 eyes underwent CE with Akreos MI60 IOL. Mean age (± SD) was 76.1 (± 9.4). A preoperative diagnosis of open-angle glaucoma (OAG) and ocular hypertension (OHT) was found in 10.9% and 3.6%, respectively. Mean pre-operative IOP was 16.8 ± 4.1. Mean IOP reduction at 2 months follow-up after CE was 2.8 ± 3.7 mmHg in the Akreos group and 0.3 (± 4.3) in the Eye Cee One group (< 0.001). Five patients who underwent EyeCee One IOL implant had IOP rise ≥ 10 mmHg at 2 months follow-up, whereas none of the patients in the Akreos MI60 group had IOP spikes. Age and type of IOL implant were associated with greater IOP reduction in both univariable and multivariable analyses.
Conclusion: CE with acrylic hydrophobic EyeCee One IOL implant was associated with more IOP spikes compared to the acrylic hydrophilic Akreos MI60 IOL implant. Further studies are warranted to clarify the association between IOP and IOL implants.
Keywords: intraocular pressure, intraocular lens, cataract surgery, hydrophobic, hydrophilic
Introduction
Intraocular lenses (IOLs) are a fundamental component of cataract surgery and are commonly implanted as an artificial replacement for the natural crystalline lens.1 Various designs and materials of IOLs are currently in the market, which ultimately aim to optimize short and long-distance visual acuity. An ophthalmologist can choose the most appropriate IOL considering the clinical circumstances, with an emphasis on how different materials and shapes have various refractive indexes and a different likelihood of complications post-operatively. For accurate decision making, it is essential to acknowledge the qualities and limitations of each IOL.1 Over the years various IOL materials have been introduced into the market. This ranges from the first ever material used in cataract surgery - polymethylmethacrylate (PMMA), to the use of more modern IOLs such as acrylic hydrophilic and hydrophobic IOLs. Such materials can be classified based on the various properties they have, including but not limited to Abbe number, hydrophobicity, biocompatibility, and refractive index.2 Although all cataract procedures are associated with a risk of developing complications, certain complications are seen more commonly in specific types of IOLs in comparison with others. A common postoperative complication is posterior capsule opacification (PCO) formation, which studies have shown to be more prevalent in acrylic hydrophilic than hydrophobic IOLs.3,4
Although it has been reported that IOP decreases in some patients after CE with IOL implant,5,6 IOP spikes have also been reported among the most common cataract surgery complications.7 These IOP spikes after cataract surgery have been associated with topical steroid use,8 concomitant glaucoma,9 resident-performed surgeries.10 IOP spikes in the postoperative period can have negative effects, especially in eyes with glaucoma or other ocular comorbidities, causing additional VF defects, severe discomfort, and complications such as ischemic optic neuropathy.10 However, there is still room for more evidence to investigate the association between IOP spikes and the type of IOL implant.
On January 26th, 2023, the Medicines and Healthcare products Regulatory Agency (MHRA) issued a Device Safety Information (DSI) alert (DSI/2023/001), mandating the immediate cessation of use and quarantine of all preloaded EyeCee One IOLs following reports of IOP spikes. The underlying cause of these IOP elevations has not yet been determined, and further investigations are ongoing in collaboration with the manufacturer. In May 2023, the Royal College of Ophthalmologists published a report looking at 820 eyes of 758 patients, in which 6.2% of all eyes had IOP spikes at the first postoperative follow-up.11
However, IOP spikes can occur with various types of IOL implants, and it remains unclear whether they are more frequent with hydrophobic IOLs compared to hydrophilic ones.
Our comparative study aims to evaluate the post-operative IOP changes after cataract surgery with the use of hydrophobic IOL implant (EyeCee One, Bausch & Lomb) compared with the hydrophilic implant (Akreos MI60, Bausch & Lomb) at 2 months follow-up.
Materials and Methods
This is a retrospective case-control study of all patients who underwent cataract extraction with EyeCee One (Bausch & Lomb, Canada) IOL implant and Akreos MI60 (Bausch & Lomb, Canada) IOL implant between January 2022 and January 2023 at the United Lincolnshire Hospital NHS Trust.
The study adhered to the tenets of the Declaration of Helsinki, and Institutional review board approval was obtained from the United Lincolnshire Hospital NHS Trust Research and Innovation. Informed consents were obtained from all individual participants included in the study.
All patients were required to have at least one pre-operative examination and one postoperative examination at 2 months including IOP measurement. Exclusion criteria included angle closure or angle closure suspect, brunescent and white cataracts, history of other surgical interventions, laser procedures, intravitreal injections and changes of glaucoma medications for other reasons during the follow-up period. Patients who experienced cataract surgery complications, including posterior capsular tear, vitreous loss and other conditions associated with IOP fluctuations were also excluded.
Demographics for each patient were collected through electronic health record (EHR), including parameters such as age, gender, history of diabetes, history of glaucoma, ocular hypertension or other ocular comorbidities, use of IOP-lowering medication, use of systemic medications affecting IOP including systemic steroids, and smoking history. Data encompassed pre-operative and post-operative best corrected distant visual acuity (BCDVA), axial length (AXL), anterior chamber depth (ACD), white-to-white (WTW), type and power of IOL implant, pre- and post-operative IOP. IOP was measured using Goldmann Applanation Tonometry (GAT) by a trained specialist nurse or an ophthalmic surgeon. IOP reduction was measured as an absolute number. Gonioscopy was performed before the surgery by a consultant ophthalmic surgeon. BCVA was measured using a LogMAR chart. Optical Biometry (IOL-Master 500) was utilized to capture data on parameters including AXL, ACD, and WTW measurements.
All surgeries were carried out by three surgeons, who followed a standard protocol for phacoemulsification cataract surgery. All surgeries were performed using a standardized phacoemulsification technique under topical anesthesia. A 2.2 mm clear corneal incision was created, followed by the instillation of a cohesive ophthalmic viscosurgical device (OVD, Provisc, Alcon) to maintain anterior chamber stability. A continuous curvilinear capsulorhexis (approximately 5.5 mm) was performed, followed by standard hydrodissection and hydrodelineation. Nucleus removal was carried out using the stop-and-chop technique with the same phacoemulsification machine and settings in all cases. Residual cortical material was aspirated, and the assigned intraocular lens (hydrophobic or hydrophilic acrylic) was implanted in the capsular bag using a preloaded injector. The OVD was thoroughly removed from the anterior chamber, and incisions were hydrated to ensure watertight closure. All patients in the study received the same postoperative medications including chloramphenicol 0.5% four times daily for one week and Dexamethasone 0.1% four times daily for two weeks, followed by twice daily for two weeks.
IOP was measured preoperatively and postoperatively at week 8 using Goldmann applanation tonometry. IOL material, model, and power were recorded for each patient.
Statistical Analysis
Comparison of the baseline characteristics and IOP between the acrylic hydrophobic EyeCee One IOL group and acrylic hydrophilic Akreos MI60 group were performed using the independent t test and the paired t test for continuous variables and the χ 2 test for categorical variables. Regression analysis was performed to identify the factors associated with greater IOP reduction at 2 months after CE with IOL implant. The multivariate model was made solely including the variables that hold statistical significance and/or clinical relevance. The statistical analysis was performed using Statistical analysis software (SPSS 18.0; SPSS Inc., Chicago, IL; P<0.050 were considered statistically significant.
Results
A total of 414 eyes were initially enrolled. Two hundred two eyes (126 eyes receiving EyeCee One IOL and 95 receiving Akreos MI60 IOL) were excluded due to missing data, resulting in 115 eyes who underwent CE with EyeCee One IOL implant and 78 eyes who underwent CE with Akreos IOL implant.
Patients’ demographics including all patients are shown in Table 1. Mean age (± SD) was 76.1 (± 9.4). A preoperative diagnosis of OAG was found in 21/193 (10.9%) and 7 (3.6%) of ocular hypertension (OHT). Mean AXL was 23.4 (± 1.4) mm, mean ACD was 3.0 (± 0.5) mm, mean WTW was 11.7 (± 1.1) mm. Mean pre-operative IOP was 16.8 ± 4.1 mmHg. Mean IOP reduction at 2 months follow-up after CE was 2.8 ± 3.7 mmHg in the Akreos group and 0.3 (± 4.3) mmHg in the Eye Cee One group (<0.001).
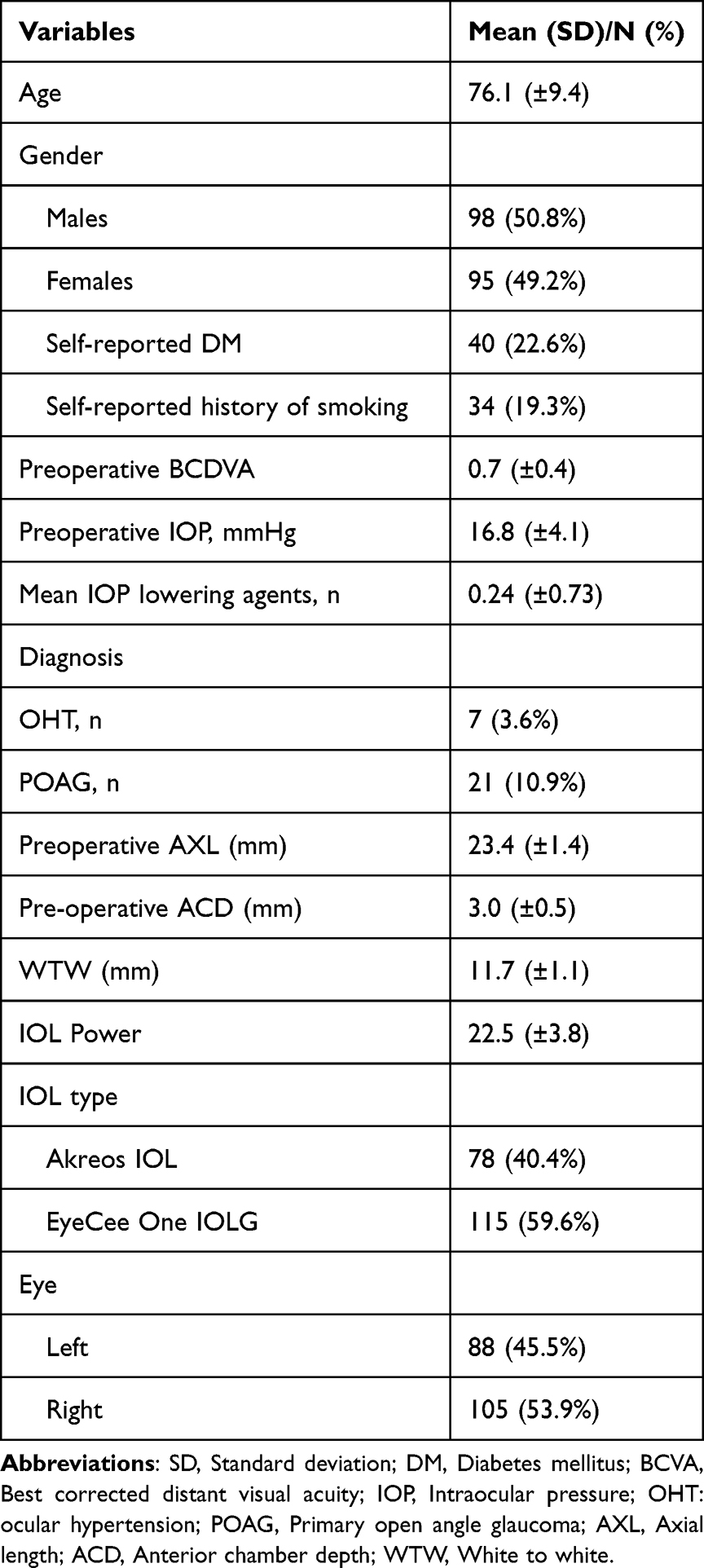 |
Table 1 Patient Demographics Characteristic Including the Entire Patients Cohort (n=193) |
Pre-operative IOP, diagnosis of OAG, AXL, ACD, were not significantly associated with IOP reduction. Five patients who underwent Eye Cee one IOL implant had IOP rise ≥10 mmHg at 2 months follow-up, whereas none of the patients in the Akreos group had IOP spikes.
Table 2 shows demographic and clinical characteristics in the Eye Cee One group compared to the Akreos group. There is no significant difference between the two groups in terms of age (P = 0.801), gender (P = 0.061), diagnosis of OAG (p = 0.098) and ocular hypertension (P=0.839). Self-reported diabetes mellitus and history of smoking did not differ between the two groups (P= 0.672 and P= 0.921, respectively).
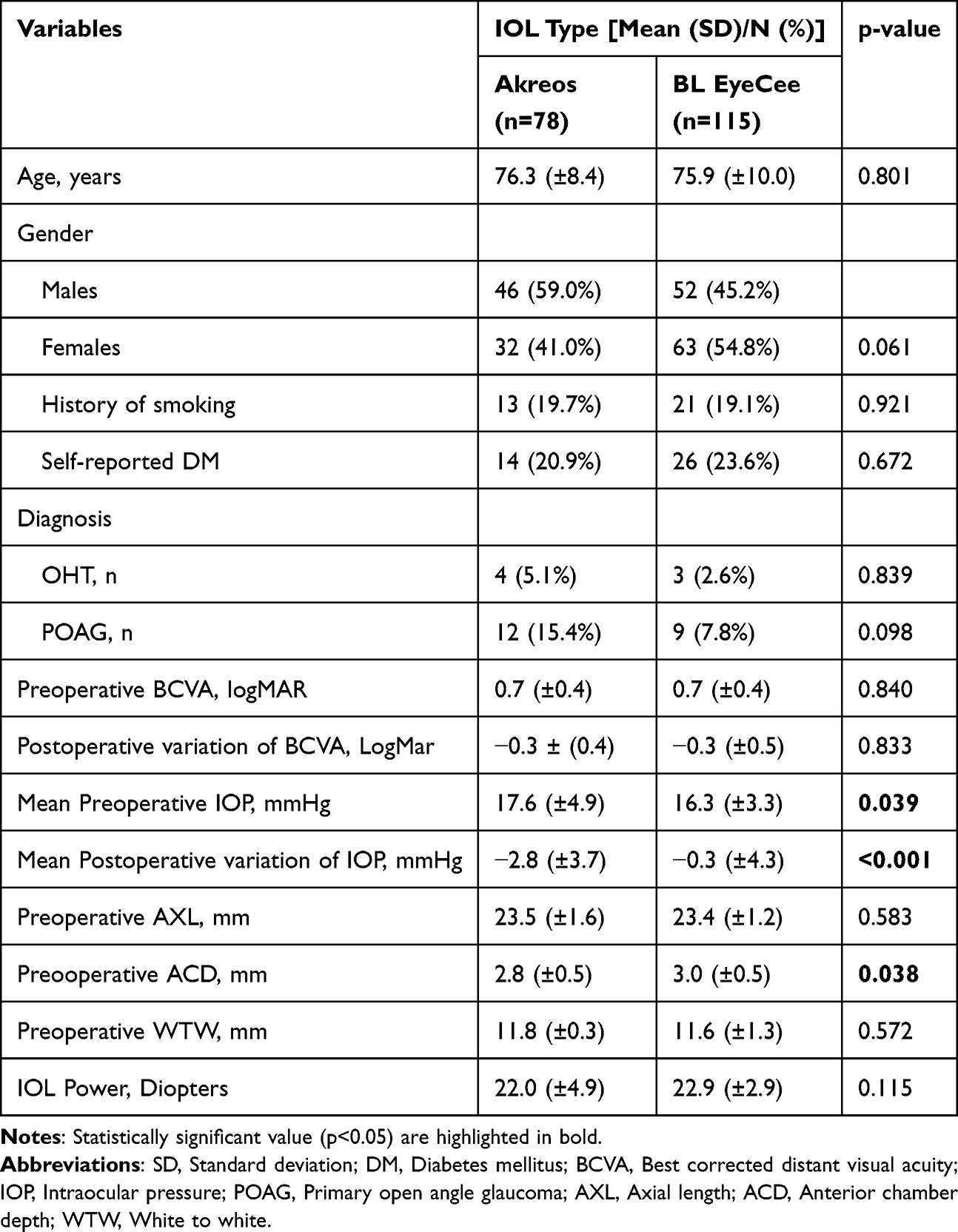 |
Table 2 Patients Demographics of Patients in the Akreos Versus EyeCee One IOL Groups |
The mean pre-operative IOP was 17.6 ± 4.9 mmHg in the Akreos group, and 16.3 ± 3.3 mmHg in the EyeCee One group. The IOP change after CE with IOP implant −2.8 ± 3.7 mmHg in the None of the patients in the Eye Cee One group, and five patients in the Eye Cee Light group, developed IOP spikes greater than 10 mmHg that required IOP-lowering medications or selective laser trabeculoplasty.
Only one of the 5 patients who experienced IOP spikes had a pre-operative diagnosis of OAG.
With respect to posterior capsular opacification (PCO), one patient in the Akreos group developed early PCO, whereas no cases of significant early PCO were observed in the EyeCee One group at the 2-month follow-up.
Table 3 shows the factors associated with greater IOP changes after CE with IOP implant considering the entire cohort of patients. The IOL type was significantly associated with greater IOP changes in both the univariate and multivariate analyses (ß coefficient: 2.65 (0.74; 4.56) (P=0.007)). Age was also associated with greater IOP reduction in both univariable and multivariable analysis (ß coefficient: 0.15 (0.05; 0.25) (P=0.003).
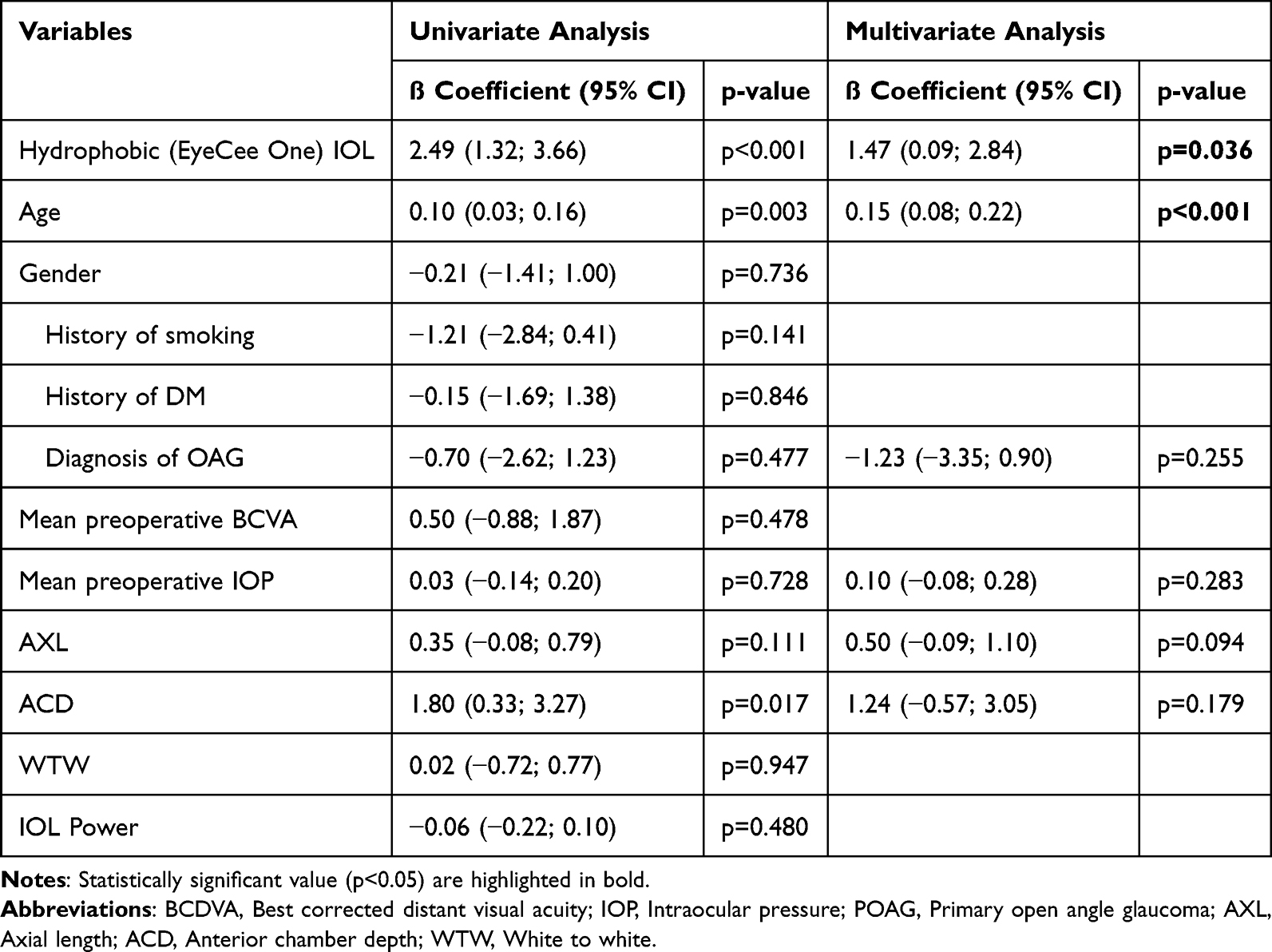 |
Table 3 Factors Associated with IOP Changes After Cataract Surgery |
Pre-operative ACD was significantly associated with greater IOP changes in the univariable analysis (ß coefficient: 1.80 (0.33; 3.27) (P=0.002), but the association was not significant in the multivariable analysis (P=0.132). Pre-operative IOP, pre-operative BCVA, diagnosis of OAG, AXL and WTW were not significantly associated with IOP reduction.
Discussion
The present study showed that IOP spikes occurred in eyes receiving acrylic hydrophobic EyeCee One IOL implant, whereas none of the eyes who underwent CE with acrylic hydrophilic Akreos MI60 IOL implant experienced IOP spikes. Our study also showed that IOL type and patients’ age were significantly associated with IOP changes after CE with IOL implant, suggesting that these factors might affect IOP after cataract surgery.
Raised IOP is a common complication following cataract surgery.12 The causes are multifactorial, with factors including retained ophthalmic viscoelastic devices (OVD), surgical technique, prior ocular trauma, vitreous loss at surgery, pre-existing glaucoma, and unexperienced surgeon, commonly associated with greater spikes.8,10,12 Seol at al. reported IOP spikes in less than 5% of both normal tension glaucoma (NTG) and healthy eyes, with most of spikes occurring over the first 3 days postoperatively. Only 1 out 149 NTG eye had persistent postoperative IOP spikes >10 mmHg at 4 weeks follow-up.13 A recent study by Rees showed that increased LT and a lower number of preoperative medications were significant predictors of increased IOP after cataract surgery.14 Another study in glaucoma eyes found that higher baseline IOP, male sex, glaucoma, Black race, older age, and complex cataract coding were associated with early postoperative IOP spike, whereas diabetes and postoperative aphakia were protective against a spike after stand-alone phacoemulsification.15
In the present study, 4.3% of eyes who underwent CE with the acrylic hydrophobic EyeCee IOL implant experienced IOP spikes greater than 10 mmHg at 2 months follow up, whereas none of the eyes who underwent CE with hydrophilic Akreos MI60 IOL implant showed any spikes. One of the 5 patients had a preoperative diagnosis of glaucoma, whereas four patients had no comorbidities or risk factors that could explain the expectedly raised IOP. Most of the eyes who had IOP spikes (4/5) were managed with medications and strict follow-up, while one case required additional selective laser trabeculoplasty.
Our findings confirm those of a recent report published by the Royal College of Ophthalmologists found 51/820 eyes (6.2%) who had EyeCee One IOL implant, had an IOP of ≥ 30mmHg at their first postoperative visit. Out of 51, 14 eyes were previously diagnosed with OHT, open-angle and angle closure glaucoma and 5 eyes had a combined pars plana vitrectomy (PPV) and phacoemulsification using EyeCee One IOL implant. As reported by the authors, the vast majority of these eyes were managed medically with topical or systemic IOP lowering medications, whereas three cases required surgical intervention to control IOP, including one case of IOL exchange with PPV after MHRA DSI/2023/001 was issued.11 It should be noted that the study period partly predates this alert and therefore does not establish causality. Although the underlying reasons remain unclear, we speculate that either the IOL material or aspects of the manufacturing process may have contributed to anatomical or inflammatory changes, potentially resulting in uncontrolled IOP after cataract surgery. Alternatively, factors unrelated to the IOL itself—such as postoperative inflammation, residual lens material, the use of topical steroids, or improper administration of glaucoma medications—could also explain the observed IOP spikes. One possible explanation is that acrylic IOLs adhere more firmly to the posterior capsule, reducing the space between the IOL and capsule, which may alter aqueous dynamics or trap viscoelastic material, contributing to IOP elevation. Another potential mechanism is that hydrophobic IOLs have a more lipophilic surface, which can promote protein adsorption and cellular adhesion, potentially leading to increased fibrin formation, accumulation of cellular debris in the anterior chamber, or transient trabeculitis, all of which may trigger IOP spikes.
Bojikian et al reported that 2.1% of nonglaucomatous eyes and 8.4% of glaucomatous eyes were diagnosed as steroid responders following cataract surgery, with steroid response associated with longer axial length in both groups and with greater numbers of preoperative medications in glaucoma patients.16 Furthermore, an experimental study17 demonstrated that residual OVD retained in the capsular bag after irrigation/aspiration was significantly greater in eyes with single-piece IOLs compared with three-piece IOLs, suggesting that IOL material may also influence OVD retention.
Nonetheless, these considerations remain speculative, as no evidence or established pathophysiological mechanism currently explains a direct relationship. The role of IOL hydrophobicity in postoperative IOP elevation remains uncertain, and further research is warranted to clarify this possible association and its underlying mechanisms.
EyeCee One is a preloaded monofocal hydrophobic acrylic IOL manufactured by Bausch and Lomb (Quebec, Canada). It has a negative aspheric optic, 360-degree posterior square edge, and modified L-loop haptics design features. The material specifications include UV and blu-light filters, a dense polymetric network that is produced by a double-polymerisation manufacturing process and has a refractive index of 1.52. (B+L, 2022) The study by Lantham et al showed excellent post-operative visual acuity and refractive outcomes in eyes after EyeCee One implantation with no intra-operative complications. Only 1.3% of patients reported complications 2 weeks post-operatively, including allergic conjunctivitis, entropion, acute vision loss at 2 weeks, which are not attributed to cataract surgery. No cases of IOP elevation were reported.18 A recent randomized controlled trial by Palsson investigated the inflammatory response in patients implanted with either EyeCee One hydrophobic or Akreos MI60 hydrophilic IOLs. The study found no significant differences between the two groups in terms of postoperative inflammation, cystoid macular edema, or visual acuity. However, intraocular pressure outcomes were not reported.19
The present study also showed that older age was significantly associated with greater IOP reduction. In agreement with our study, Leal I. et al found a significant association between older age and higher IOP reduction.5 This IOP reduction may reflect the phacodynamic effect of a larger mature lens in IOP drainage dynamics.20 Previous studies also showed that shallower ACD was significantly associated with percentage of IOP decrease after cataract surgery.21 The present study showed that a deeper AC was significantly associated with greater IOP reduction. However, this association was not confirmed in the multivariate model.
There are only a few studies which observed a relationship between the design and material of IOLs, and the post-operative IOP. A study by Alzafiri et al has shown that there were no differences in mean IOP or IOP spikes between foldable acrylic and rigid PMMA IOLs for combined phacoemulsification and trabeculectomy.21 With the same combined procedure, R Braga-Mele et al found that IOP control was similar in patients with foldable silicone IOLs versus PMMA IOLs.22 However, these studies focused exclusively on cataract surgery combined with trabeculectomy and may not be directly applicable to our work. To date, no studies have specifically evaluated IOP changes following cataract surgery alone in relation to IOL material or design, nor whether either factor is directly associated with IOP spikes.
The present study has several limitations. The retrospective nature of the study limits control over confounders and introduces selection bias. Prospective studies are required to provide stronger evidence. Prospective studies are required to provide stronger evidence. Secondly, a considerable number of patients were excluded due to missing preoperative or postoperative data. In fact, most patients were followed by local opticians and referred back to the surgeons only in cases of complications. Patients who attended follow-up were predominantly those with ocular comorbidities, such as glaucoma or age-related macular degeneration, which may influence IOP through different mechanisms. Although the proportion of comorbidities did not differ between the EyeCee One and Akreos groups, the exclusion of such a large number of patients due to missing data remains a potential source of bias.
Third, all cataract surgeries were performed by three different consultants. Differences in surgical techniques among surgeons may have contributed to IOP spikes, and this inter-surgeon variability could have affected our findings. Fourth, the choice of intraocular lens was guided by the surgeons’ preferences and lens availability in the Hospital Trust. As a result, there is a possibility of an allocation bias that could have influenced the outcomes of our study. Fifth, although IOP typically normalizes within one to four weeks after discontinuing topical steroids,23 the postoperative use of steroids may still have influenced our results. All patients in the study received the same regimen (Dexamethasone 0.1% four times daily for two weeks, followed by twice daily for two weeks); however, the presence of steroid responders could have led to significant IOP fluctuations that may have affected our findings. Sixth, it is worth noting that the IOP measurements were conducted during morning or early afternoon sessions at an outpatient clinic. Given the known circadian variations in IOP that tend to affect individuals with glaucoma more significantly than those with healthy eyes,24,25 the timing of our measurements could potentially have influenced our outcomes. For future investigations, it would be prudent to standardize the time of day for IOP measurements in order to mitigate the potential impact of circadian rhythms on the results. Seventh, Preoperative IOP was significantly higher in the Akreos group, while ACD was deeper in the EyeCee group. These imbalances could independently affect IOP changes, irrespective of IOL type. For example, some recent studies14 demonstrated that IOP spikes following cataract surgery were associated with anterior segment anatomy, including lens thickness and axial length. Other studies21 also found that higher preoperative IOP, ACD, axial length and lens thickness were associated with greater IOP decrease after cataract surgery. Multivariable adjustment may therefore not fully remove this bias, as the model only included variables deemed statistically significant or clinically relevant, potentially overlooking hidden confounders. Furthermore, no formal correction for multiple comparisons was applied and that the findings should therefore be interpreted with appropriate caution. Finally, the definitions of IOP spikes varies widely across the different studies. These differing definitions limit direct comparison across studies.
To conclude, the present study showed that cataract surgery with IOL implant can significantly reduce IOP levels at 2 months follow-up. However, IOP spikes requiring medications or laser treatment were observed in eyes who received Eye Cee One IOL implant. These findings suggest that IOL materials and designs can negatively affect IOP after cataract surgery. Further investigations on the underlying causes need to be carried out to reduce the rates of these sight threatening complications and protect our patients’ vision.
Acknowledgments
No sponsor or funding organization had role in this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Zvornicanin J, Zvornicanin E. Premium intraocular lenses: the past, present and future. J Curr Ophthalmol. 2018;30(4):287–296. doi:10.1016/j.joco.2018.04.003
2. Vacalebre M, Frison R, Corsaro C, et al. Current state of the art and next generation of materials for a customized intraocular lens according to a patient-specific eye power. Polymers. 2023;15(6):1590. doi:10.3390/polym15061590
3. Grzybowski A, Zemaitiene R, Markeviciute A, Tuuminen R. Should we abandon hydrophilic intraocular lenses? Am J Ophthalmol. 2022;237:139–145. doi:10.1016/j.ajo.2021.11.021
4. Zhao Y, Yang K, Li J, Huang Y, Zhu S. Comparison of hydrophobic and hydrophilic intraocular lens in preventing posterior capsule opacification after cataract surgery: an updated meta-analysis. Medicine. 2017;96(44):e8301. doi:10.1097/MD.0000000000008301
5. Leal I, Chu CJ, Yang YY, Manasses DM, Sebastian RT, Sparrow JM. Intraocular pressure reduction after real-world cataract surgery. J Glaucoma. 2020;29(8):689–693. doi:10.1097/IJG.0000000000001527
6. Poley BJ, Lindstrom RL, Samuelson TW, Schulze R Jr. Intraocular pressure reduction after phacoemulsification with intraocular lens implantation in glaucomatous and nonglaucomatous eyes: evaluation of a causal relationship between the natural lens and open-angle glaucoma. J Cataract Refract Surg. 2009;35(11):1946–1955. doi:10.1016/j.jcrs.2009.05.061
7. Grzybowski A, Kanclerz P. Early postoperative intraocular pressure elevation following cataract surgery. Curr Opin Ophthalmol. 2019;30(1):56–62. doi:10.1097/ICU.0000000000000545
8. Pleyer U, Ursell PG, Rama P. Intraocular pressure effects of common topical steroids for post-cataract inflammation: are they all the same? Ophthalmol Ther. 2013;2(2):55–72. doi:10.1007/s40123-013-0020-5
9. Levkovitch-Verbin H, Habot-Wilner Z, Burla N, et al. Intraocular pressure elevation within the first 24 hours after cataract surgery in patients with glaucoma or exfoliation syndrome. Ophthalmology. 2008;115(1):104–108. doi:10.1016/j.ophtha.2007.03.058
10. Kim JY, Jo MW, Brauner SC, et al. Increased intraocular pressure on the first postoperative day following resident-performed cataract surgery. Eye (Lond). 2011;25(7):929–936. doi:10.1038/eye.2011.93
11. Wang H, Jong JLZ, Chiu SJ, Kay WL, Tan JHY. Evaluation of raised intraocular pressure post EyeCee One preloaded intraocular lenses implantation. Eye (Lond). 2023;37:3293–3294. doi:10.1038/s41433-023-02487-y
12. Mackner AJ. Ups and downs in cataract surgery complications; 2019. Available from: https://collaborativeeye.com/articles/2019-oct/ups-and-downs-in-cataract-surgery-complications/.
13. Seol BR, Shin JY, Choi S, Kang TG, Jeoung JW, Park KH. Intraocular pressure (IOP) change and frequency of IOP spike after cataract surgery in normal-tension glaucoma: a case-control study. J Glaucoma. 2019;28(3):201–206. doi:10.1097/IJG.0000000000001172
14. Rees JP, Khuu TH, Sanchez FG, et al. Anterior segment parameters are associated with intraocular pressure spikes following cataract surgery in glaucoma patients. J Glaucoma. 2025;34(8):637–643. PMID: 40340970. doi:10.1097/IJG.0000000000002589
15. Lidder AK, Vanner EA, Chang TC, Lum F, Rothman AL. Intraocular pressure spike following stand-alone phacoemulsification in the IRIS® Registry (intelligent research in sight). Ophthalmology. 2024;131(7):780–789. PMID: 38246424. doi:10.1016/j.ophtha.2024.01.022
16. Bojikian KD, Nobrega P, Roldan A, Forrest SL, Tsukikawa M, Chen PP. Incidence of and risk factors for steroid response after cataract surgery in patients with and without glaucoma. J Glaucoma. 2021;30(4):e159–e163. PMID: 33428351. doi:10.1097/IJG.0000000000001785
17. Oki T, Horiguchi H, Terauchi R, Gunji H, Nakano T. Comparison of the residual amount of an ophthalmic viscosurgical device among different types of intraocular lens implants in vitro. Clin Ophthalmol. 2024;18:1083–1091. PMID: 38659426; PMCID: PMC11041993. doi:10.2147/OPTH.S458348
18. Latham SG, Carr F, Ali H, Gangwani V. Clinical safety and efficacy of a preloaded monofocal hydrophobic acrylic intraocular lens in a real-world population. BMC Ophthalmol. 2021;21(1):379. doi:10.1186/s12886-021-02142-8
19. Pålsson S, Schuborg C, Sterner B, Andersson Grönlund M, Zetterberg M. Hydrophobic and hydrophilic IOLs in patients with uveitis - a randomised clinical trial. Clin Ophthalmol. 2025;19:373–383. PMID: 39926313; PMCID: PMC11806708. doi:10.2147/OPTH.S493398
20. Hsu CH, Kakigi CL, Lin SC, Wang YH, Porco T, Lin SC. Lens position parameters as predictors of intraocular pressure reduction after cataract surgery in nonglaucomatous patients with open angles. Invest Ophthalmol Vis Sci. 2015;56(13):7807–7813. doi:10.1167/iovs.15-17926
21. Alzafiri Y, Harasymowycz P. Foldable acrylic versus rigid polymethylmethacrylate intraocular lens in combined phacoemulsification and trabeculectomy. Can J Ophthalmol. 2004;39(6):609–613. doi:10.1016/S0008-4182(04)80025-5
22. Braga-Mele R, Cohen S, Rootman DS. Foldable silicone versus poly(methyl methacrylate) intraocular lenses in combined phacoemulsification and trabeculectomy. J Cataract Refract Surg. 2000;26(10):1517–1522. doi:10.1016/S0886-3350(00)00478-8
23. Phulke S, Kaushik S, Kaur S, Pandav SS. Steroid-induced glaucoma: an avoidable irreversible blindness. J Curr Glaucoma Pract. 2017;11(2):67–72. PMID: 28924342; PMCID: PMC5577123. doi:10.5005/jp-journals-l0028-1226
24. Sacca SC, Rolando M, Marletta A, Macri A, Cerqueti P, Ciurlo G. Fluctuations of intraocular pressure during the day in open-angle glaucoma, normal-tension glaucoma and normal subjects. Ophthalmologica. 1998;212(2):115–119. doi:10.1159/000027290
25. Mansouri K, Tanna AP, De Moraes CG, Camp AS, Weinreb RN. Review of the measurement and management of 24-hour intraocular pressure in patients with glaucoma. Surv Ophthalmol. 2020;65(2):171–186. doi:10.1016/j.survophthal.2019.09.004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.