Back to Journals » Clinical Ophthalmology » Volume 17
Intraocular Pressure and Medication Changes Associated with Xen Gel Stent: A Systematic Review of the Literature
Authors Panarelli JF, Vera V, Sheybani A, Radcliffe N ![]() , Fiscella R, Francis BA, Smith OU, Noecker RJ
, Fiscella R, Francis BA, Smith OU, Noecker RJ
Received 6 October 2022
Accepted for publication 19 December 2022
Published 5 January 2023 Volume 2023:17 Pages 25—46
DOI https://doi.org/10.2147/OPTH.S390955
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Joseph F Panarelli,1 Vanessa Vera,2 Arsham Sheybani,3 Nathan Radcliffe,4 Richard Fiscella,2 Brian A Francis,5 Oluwatosin U Smith,6 Robert J Noecker7,8
1Department of Ophthalmology, New York University, New York, NY, USA; 2Allergan, an AbbVie Company, Dublin, Ireland; 3Department of Ophthalmology and Visual Sciences, Washington University in St. Louis School of Medicine, St. Louis, MO, USA; 4Department of Ophthalmology, New York Eye and Ear Infirmary, New York, NY, USA; 5Department of Ophthalmology, Doheny Eye Institute, University of California Los Angeles, Los Angeles, CA, USA; 6Glaucoma Associates of Texas, Dallas, TX, USA; 7Department of Ophthalmology and Visual Science, Yale School of Medicine, New Haven, CT, USA; 8Ophthalmic Consultants of Connecticut, Fairfield, CT, USA
Correspondence: Joseph F Panarelli, Department of Ophthalmology, New York University, 222 E 41st St, 3rd Floor, New York, NY, 10017, USA, Email [email protected]
Abstract: The Xen gel stent (Allergan Inc, an AbbVie company; Dublin, Ireland) was conceived as an option for patients requiring modest IOP reduction but for whom trabeculectomy was not yet indicated. As with any glaucoma surgery, establishing criteria for patient selection and identifying factors that contribute to a high likelihood of success are important. To help guide clinical decision-making, a systematic review of published studies on the gel stent was performed, with the goal of understanding postoperative outcomes based on clinical and patient factors. Results were organized around a series of pertinent clinical questions based on scenarios encountered in clinical practice. Criteria for including studies were intentionally broad, with the objective of simulating the diverse population of glaucoma patients encountered in real-world practice. Outcomes for IOP and medication reduction postoperatively were assessed in various analyses, including in eyes with various glaucoma types and severity; in eyes naïve to surgery as well as those with a history of prior incisional glaucoma surgery; and when surgery was performed as a standalone procedure or at the time of cataract surgery. The results of each of the various analyses were consistent in demonstrating that successful gel stent surgery achieved a postoperative IOP of approximately 14.0 mm Hg and reduction to fewer than 1 glaucoma medication. Additional data are shown on outcomes by method of implant (ab interno vs ab externo); intraoperative use of antifibrotics; and rates of needling in published studies.
Keywords: glaucoma, glaucoma surgery, bleb, Xen, gel stent
Introduction
The Xen gel stent (Allergan Inc, an AbbVie company) is a 6-mm-long hydrophilic tube composed of porcine gelatin crosslinked with glutaraldehyde that facilitates an outflow path to the subconjunctival space with minimal conjunctival trauma during the surgery.1 The blebs formed after the gel stent implantation are distinct in appearance compared to trabeculectomy blebs.2 When it is placed in the eye, the implant swells to become a tissue-conforming, non-migrating channel.3 By connecting the anterior chamber and subconjunctival space to direct aqueous drainage, the gel stent does not rely on the conventional outflow pathway.4 The implant was originally studied using an ab interno approach for implantation, although more recently, some authors have proposed an ab externo implantation technique.5,6
Laminar flow through the gel stent can be predicted using the Hagen-Poissuielle formula, which states that outflow resistance of a medium with a known viscosity at a given flow rate is the result of the ratio of the lumen diameter to its length. Three gel stents, all 6-mm in length but with different internal lumen diameters, were initially designed: ~45 µm (Xen45), ~63 µm (Xen63), and ~140 µm.5 All three devices have been subjected to preclinical and clinical testing, but currently only the Xen45 is commercially available. With a 6-mm length and 45-µm internal lumen, the dimensions of Xen45 provide 6 to 8 mm Hg of flow resistance, assuming a 1.2 µL/min flow rate and normal aqueous viscosity.7 These characteristics restrict the outflow of aqueous humor, thereby mitigating the risk of hypotony. In flow model testing, the 45-µm gel stent was found to reach steady-state pressure of 8.9 mm Hg at a flow rate of 2 µL/min,8 which approximates aqueous humor production in the human eye.9 The 45-µm device received a CE Mark for approval in Europe in 2013 and was granted an indication for use in refractory glaucoma by the US Food and Drug Administration in 2016.4
The safety of the 45-µm device has been confirmed in prospective and retrospective studies, consistently demonstrating postoperative IOP in the mid-to-low teens with a high probability of reducing medication burden in numerous settings, across diverse populations, and in varying degrees of glaucoma severity.5,10–12 A lack of standardized definitions for postoperative complications has been noted as a complicating factor in assessing the safety of new glaucoma devices in clinical trials.13,14 In a pivotal prospective clinical trial, the most commonly reported adverse events in the postoperative period after gel stent surgery were needling (32.3%), hypotony (24.6%), IOP increase greater than 10 mm Hg from baseline (21.5%), anterior chamber tap (9.2%), and wound leak/dehiscence (9.2%).15 Schlenker et al reported a more favorable safety profile with the gel stent compared to trabeculectomy in an international, multicenter, retrospective interventional cohort study of 509 eyes of 432 patients.16 Lenzhofer et al found no device-related risks for loss of best-corrected visual acuity (BCVA) among eyes with primary open-angle glaucoma undergoing standalone or combination procedures.17 Long-term safety with the device has also been confirmed with up to 3 years of follow-up.12
To further guide clinical decision-making, this systematic review of the literature was performed to describe effectiveness outcomes in terms of the most likely IOP response and potential to reduce medication burden after gel stent surgery, either alone or combined with cataract surgery, across a broad range of patient types, in varying degrees of glaucoma severity, and according to a variety of clinical and patient factors.
Methods
The primary intent of this systematic review was to determine the most likely IOP lowering and medication reduction associated with the gel stent in a wide assortment of patient types and settings. To further facilitate decision-making, results are organized according to a series of pertinent clinical questions most likely to be encountered in real-world clinical practice.
After excluding case studies and case series, a total of 111 studies reporting outcomes on the Xen45 gel stent that were published through June 30, 2021, were screened for this review, encompassing studies describing outcomes associated with the gel stent as an active comparator or as a control group compared to other interventions, as well as studies describing gel stent outcomes in studies without a control arm. After data from all studies were reviewed, 35 were excluded that did not report on IOP and medication outcomes, and 3 were excluded that did not report reliable data on IOP and medication use. To avoid ambiguity, a study that reported outcomes in bilateral simultaneous gel stent implantation was excluded.18 Three additional studies were excluded because the design and/or intent of the study introduced potential bias; excluding these studies assured consistency among included studies.
Partial data were included from select studies. Two studies reported outcomes of ab interno and ab externo surgeries;19,20 to ensure consistency with other studies in the systematic review, only the ab interno cohorts were included in the analysis, while outcomes from the ab externo group were summarized in a separate data table herein. Another study comparing outcomes between a first and second gel stent implant surgery in the fellow eye was included, but only data from the first-operated eye were considered.21 For two studies, data from individual study groups were included [studies compared primary open-angle glaucoma (POAG) versus pseudoexfoliative glaucoma (PEXG)].11,22 Data from each study group were included separately in the systematic analysis, and the data are also summarized in a data table.
IOP lowering and medication reduction were selected as the primary focus of this systematic review for three reasons. First, these are the most widely reported efficacy outcome values in published studies, and thus provide a basis for comparing results across studies with different methodologies. Second, change in IOP (and/or final target pressure achieved) and medication use from baseline are frequently used in clinical practice to make evidence-based decisions. Third, as these are commonly used outcome variables in both clinical trials and real-world practice, there is consensus on how these values should be reported. By comparison, this review will not discuss surgical success rates (inclusive of complete, partial, and qualified success) or failure rates, as the definitions of these values are not standardized in the literature. Safety outcomes associated with the gel stent and recommendations for managing intra- and postoperative complications have been reported elsewhere.5,23
Microsoft Excel was used to calculate all statistics used in this study. Weighted mean averages were calculated based on the number of eyes enrolled in each study. When information was available on the number of eyes remaining at various timepoints, that variable was used for calculating the weighted mean average—for example, when calculating the weighted mean average for 12-month outcomes, remaining eyes under evaluation at that timepoint were used for weighting the mean average. A similar schema was used when considering outcomes at 24 or 36 months.
Efficacy Outcomes
What are the Most Likely Outcomes for IOP and Medication Reduction Following Gel Stent Implantation?
We identified 59 studies for use in an overall analysis, in which the weighted mean average for IOP and medication use was based on reporting at the conclusion of the study, irrespective of length of follow-up. Similar analyses were performed to determine outcomes at 12 months based on 45 studies, at 24 months based on 17 studies, and at 36 months based on 6 studies. Weighted mean for IOP and medication use were also determined from 18 studies that followed patients prospectively and from 41 studies that collected data retrospectively. A summary of our various analyses is shown in Table 1.
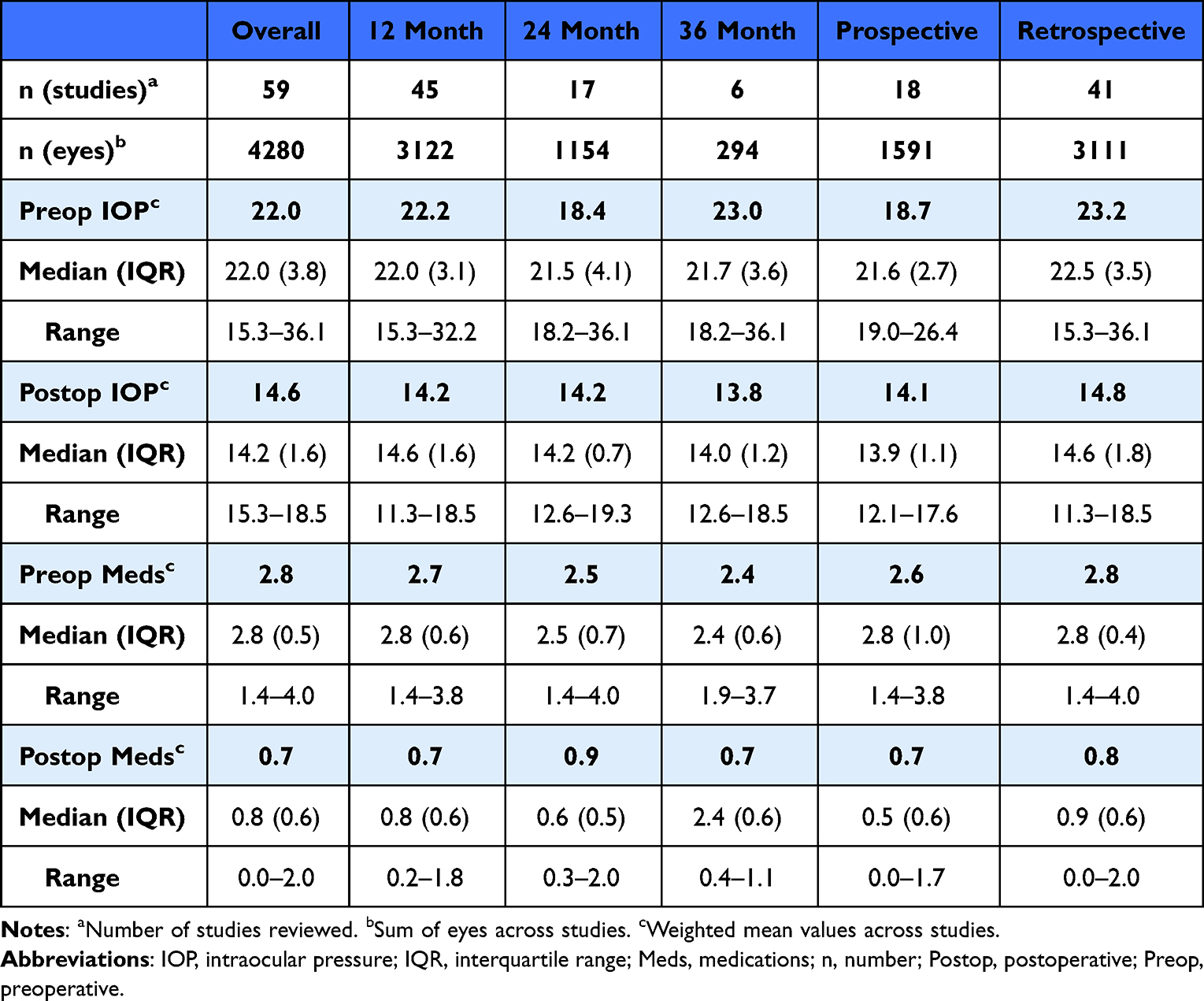 |
Table 1 Summary of IOP and Medication Reduction Across Various Study Types According to Weighted Mean Average |
A total of 59 studies representing 4280 total eyes reporting complete pre- and postoperative data on IOP and medication use were included in the overall analysis of change in IOP and medication use from baseline to the end of the study (regardless of timepoint).4,5,10–12,15,16,19–22,24–72 These studies followed a median 50 eyes (range, 12–242) of patients with a median age of 72.1 years (range, 53.4–80.9) for a median 12 months (range, 6–36). The weighted mean preoperative IOP was 22.0 mm Hg on 2.8 glaucoma medications, and the weighted mean postoperative IOP at last follow-up was 14.6 mm Hg on 0.7 glaucoma medications.
Forty-five studies (n = 3122 total eyes) reported 12-month outcomes with complete pre- and postoperative IOP and medication use.4,5,10–12,15,19,20,25,27–33,35–40,42–48,51–53,55,57–60,62–68 In these studies, the median number of eyes followed was 52 (range, 12–242) and median age was 72.2 years (range, 53.4–80.9). The weighted mean preoperative IOP was 22.2 mm Hg on 2.5 glaucoma medications, and the weighted mean postoperative IOP was 14.2 mm Hg on 0.7 glaucoma medications.
Follow-up to 24 months was reported in 17 studies (n = 1154 eyes).12,21,22,32–34,36,37,49–52,56–58,60,65 The weighted mean preoperative IOP was 18.4 mm Hg on 2.5 medications and the weighted mean postoperative IOP was 14.2 mm Hg on 0.9 medications. Follow-up to 36 months was reported in 6 studies (n = 294 eyes).12,32,34,37,51,56 The weighted mean preoperative IOP was 23.0 mm Hg on 2.4 medications and the weighted mean postoperative IOP was 13.8 mm Hg on 0.7 medications.
We sought to understand if there were any meaningful differences between studies following patients prospectively and retrospectively. In 18 prospective studies representing a total of 1591 eyes, a median of 53 eyes (range, 12–221) were followed for a median of 12 months (range, 8–36).5,10,11,15,21,22,29,31,37,40,43,44,50,54,55,58,63,69 In 41 retrospective studies representing 3111 total eyes, a median of 52 eyes (range, 13–242) were followed for a median of 12 months (range, 6–36).4,12,16,19,20,24–28,30,32–36,38,39,41,42,45–49,51–53,56–62,64,66–68,70,72 Prospective studies had a lower weighted mean average preoperative IOP (18.7 mm Hg) relative to retrospective studies (23.2 mm Hg), but the weighted mean averages for postoperative IOP, as well as pre- and postoperative medication use, were similar (Table 1).
We assessed IOP and medication use outcomes in selected studies that reported the number of eyes at enrollment and at the various timepoints through the follow-up period (Table 2). A difference in any variable when the mean average was weighted according to eyes at enrollment versus eyes at follow-up might indicate that eyes lost to follow-up, for whatever reason, might bias the data. However, the analysis demonstrated similar weighted mean averages for pre- and postoperative IOP, as well as pre- and postoperative medication use, in studies reporting data at end of follow-up (overall), at 12 months, and at 24 months, suggesting that study attrition was not a factor in reported outcomes. Furthermore, none of the weighted mean averages was notably different than findings in other analyses for this study, thus providing greater confidence in the accuracy of the outcomes reported herein.
 |
Table 2 Attrition Analysis |
Data from studies reporting IOP values at interim study visits were used to compile information about the expected IOP and IOP change from baseline at day 1 and week 1, and at months 1, 3, 6, 12, 24, and 36 (Figure 1). Available mean IOP values were tightly clustered at all time points (Figure 1B). IOP values from follow-up study visits were used to calculate median difference from baseline (Figure 2). The gel stent has been compared to other glaucoma surgeries in a few studies. An overview of outcomes from eight studies reporting IOP medication reduction from baseline to end of follow-up is shown in Table 3.16,51,64,67,73–76
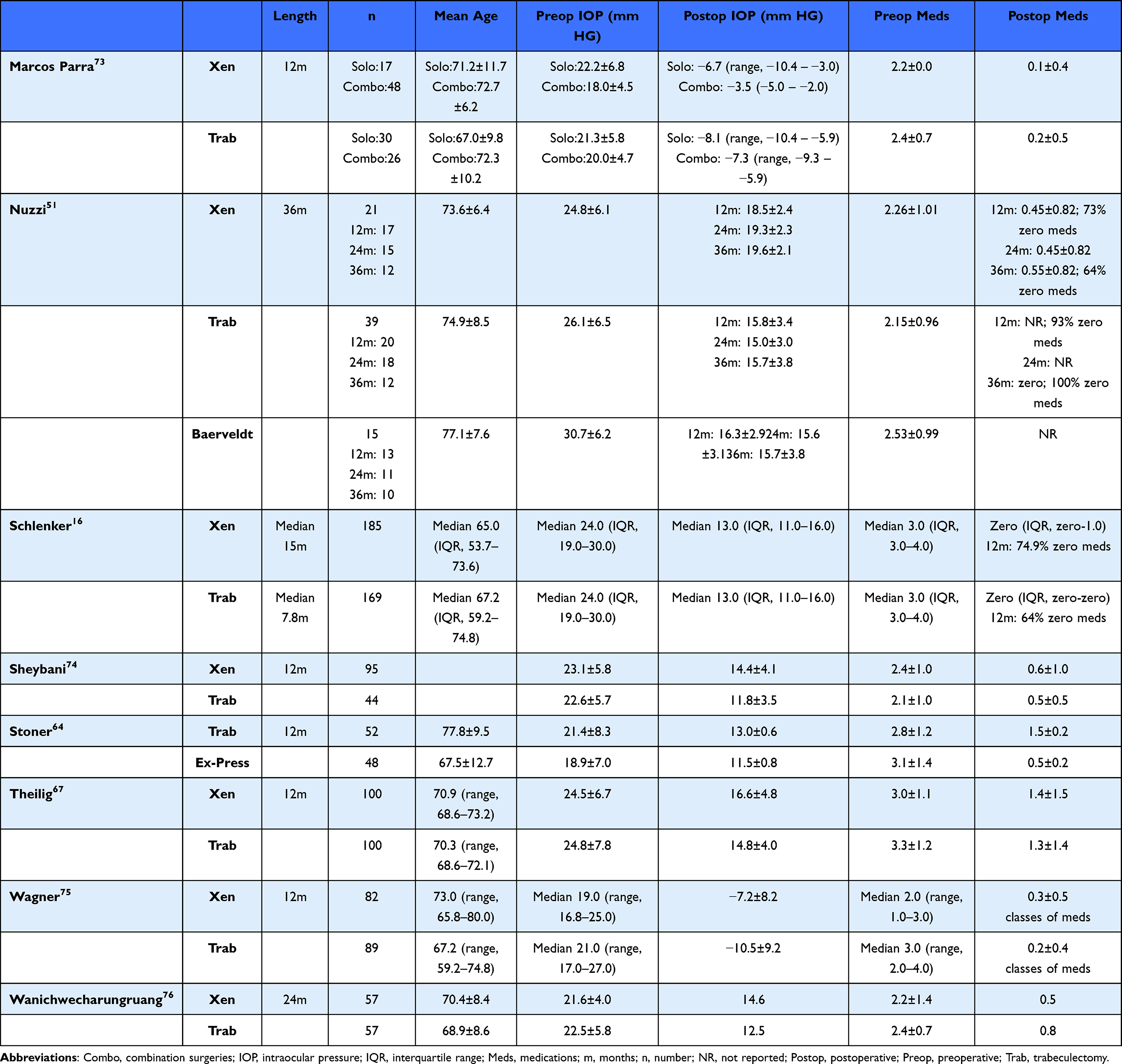 |
Table 3 Studies in Which Gel Stent Was Compared with Another Glaucoma Surgery |
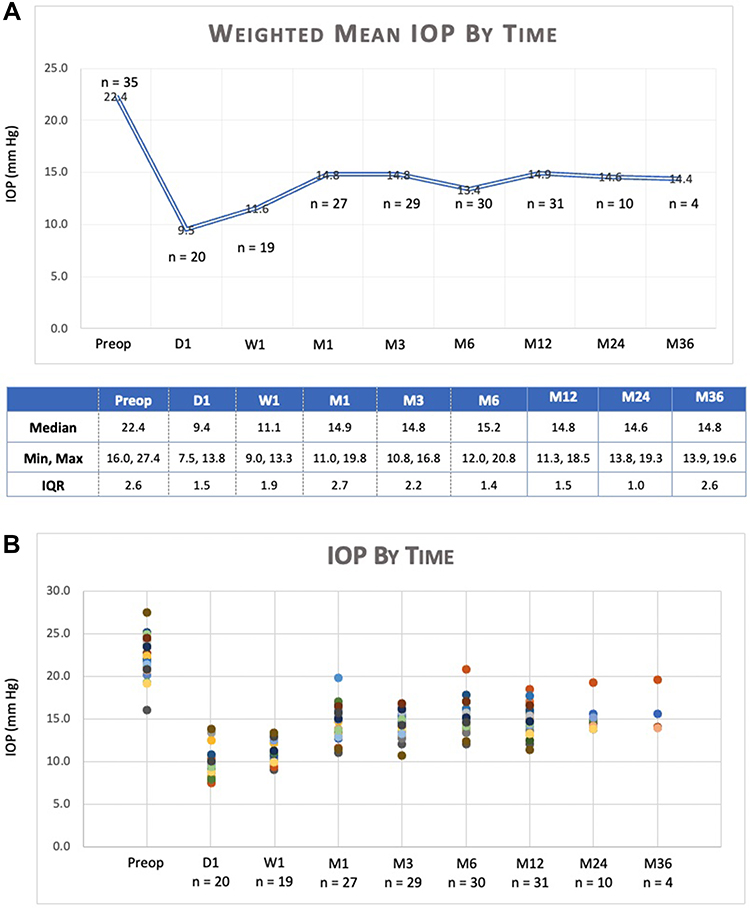 |
Figure 1 Two graphical depictions of weighted mean IOP over time after gel stent implantation among studies reporting data at baseline and at 12 months, as well as one additional interim time point. A line graph (A) shows the weighted mean IOP among qualifying studies at baseline and at day 1, week 1, and at months 1, 3, 6, 12, 24, and 36 (“n” represents the number of studies reporting data for the given time point and the number at each time points is the weighted mean IOP; additional data is shown in the accompanying table). As shown in a scatter plot (B), IOP outcomes among studies reporting baseline and 12-month data, as well as at least one additional time point, was consistent. |
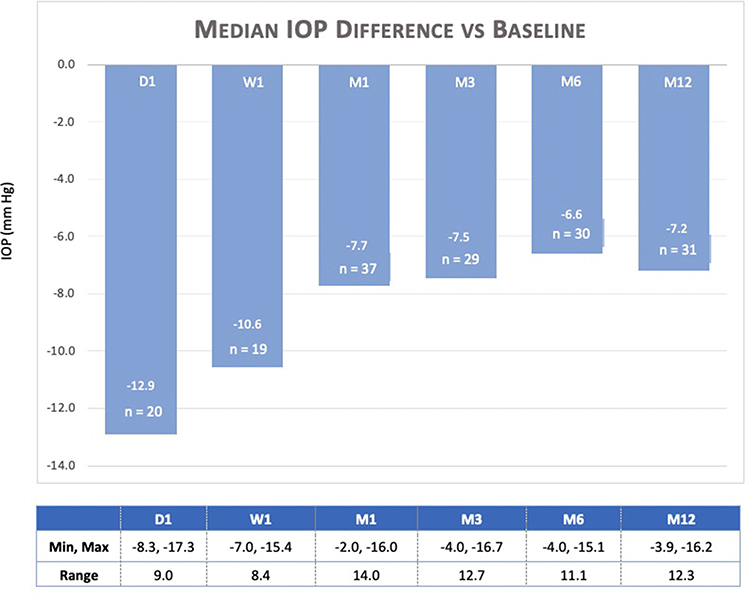 |
Figure 2 Median difference in IOP from baseline to day 1, to week 1, and to months 1, 3, 6, and 12 among studies reporting data at baseline and at 12 months, as well as one additional interim time point. On the graph, “n” represents the number of studies reporting data for the given time point and the number at each time points is the median difference in IOP from baseline to that time point. Additional data is provided in the accompanying table. |
Interpretations
Our various analyses show consistent and predictable IOP lowering with corresponding reduction in medication use after gel stent surgery across studies with varying length of follow-up and in studies with differing methodology and study design (Table 1). Taken together, the expected postoperative IOP after gel stent implantation is approximately 14.0 mm Hg on fewer than one ocular medication. After an initial decrease to around 9.0 mm Hg on day 1, IOP begins to stabilize around month 1, and then remains in the low-to-mid-teens through month 12; in successful eyes, the pressure remains consistent through longer-term follow-up of 24 and 36 months (Figure 1).
Our findings may have value for decision-making in the setting of real-world glaucoma practice. Our various analyses included studies with a wide assortment of glaucoma types, different degrees of glaucoma severity, and a range of baseline IOP. Additionally, certain studies enrolled patients who failed prior surgical interventions or were progressing despite use of medication, and in others, the prognosis was less guarded, but patients were nevertheless projected to benefit from pressure reduction and/or ability to reduce or discontinue use of pressure-reducing medications. Furthermore, our review also included gel stent implantation in standalone and combination procedures. The aggregated study population thus mimics an all-comers analysis, and it may be useful as guidance among the diverse array of patients encountered in daily practice.
In the Advanced Glaucoma Intervention Study, IOP that was consistently below 18 mm Hg yielded almost zero risk of progression over 6 years of follow-up.77 Long-term fluctuation of IOP is associated with visual field deterioration.78 Furthermore, in the Early Manifest Glaucoma Trial, risk of progression decreased by 8% for each mm Hg reduction in pressure from baseline, but there was a 13% increase in risk of progression for each mm Hg higher than baseline.79 In the same population of patients, elevated mean IOP over time was a risk factor for glaucomatous progression, with the hazard ratio rising by 11% for every mm Hg of higher IOP.80 An increase in the average IOP over time has also been correlated with deterioration on visual field.77,81 Taken together, achieving consistently low target pressure post-intervention, preferably ≤18 mm Hg, reduces risk of progression and portends a more favorable prognosis for visual function. In at least one study, filtration surgery was found to yield greater diurnal IOP control than maximum tolerated medical therapy,82 and in severe OAG, medication use is associated with more progressive visual field loss and less IOP lowering than surgery, as well as a higher risk of treatment failure.83
The limitations of including an intentionally wide assortment of studies in our analyses should be acknowledged. The wide variety of inclusion and exclusion criteria of the various studies, the differing methodologies, and the distinct study populations each introduce confounding variables that limit the ability to draw definitive conclusions. Since nonrandomized data were included in the analysis, the potential that confounding by indication influenced data reporting cannot be ruled out. However, taken together, the various studies included in this report include a representative sample of the variety of patients seen by the ophthalmologist in everyday clinical practice, and our findings provide a reasonable barometer of likely IOP and medication outcomes during the postoperative period at different timepoints.
Do Baseline Factors Influence Outcomes After Gel Stent Implantation?
Our analysis collected sufficient data to assess IOP outcomes and impact on medication according to mean baseline IOP (Table 4) and by mean baseline age (Table 5). There was insufficient data to properly review other baseline factors.
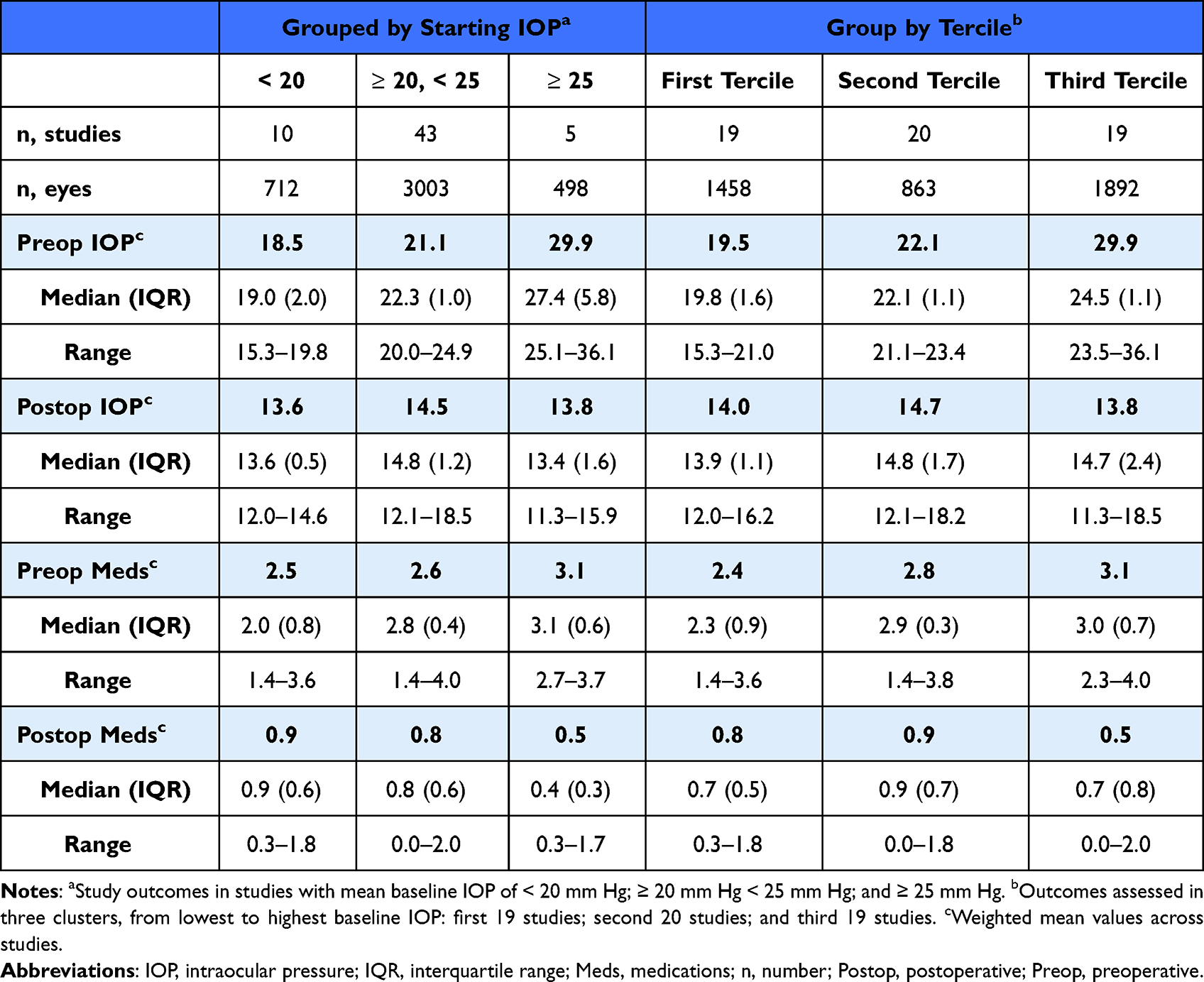 |
Table 4 IOP and Medication Reduction According to Starting IOP |
 |
Table 5 IOP and Medication Outcomes by Mean Age at Study Enrollment |
Among 58 studies that recorded a minimum of 12 months of follow-up, the postoperative weighted mean IOP was 13.6 mm Hg, 14.5 mm Hg, and 13.8 mm Hg in studies with a baseline IOP below 20 mm Hg, between 20 and 25 mm Hg, and over 25 mm Hg, respectively.4,5,12,15,16,19–22,24–70,72 In all three groups of studies, the weighted mean average number of postoperative medications was less than 1. The results were similar for a second analysis in which studies were clustered in terciles from lowest mean baseline IOP to highest: First 19 studies (range, 15.3–21.0 mm Hg),4,10,12,21,22,26,32,35,37,41,46–48,50,54,60,61,65,68 second 20 studies (range, 21.1–23.4 mm Hg),24,28,30,31,33,34,38,40,42–45,53,55,57,58,62–64,69 and third 19 studies (range, 23.5–36.1 mm Hg).5,15,16,19,20,25,27,29,36,39,49,51,52,56,59,66,67,70,72
There were 49 studies (n = 3587 eyes) available for an analysis of outcomes by mean baseline age.4,5,10,11,15,16,19–22,24–30,32–44,46,47,49–53,55,59,61–68,72 The weighted mean average postoperative IOP was 14.3 mm Hg, 15.1 mm Hg, and 14.0 mm Hg among studies with a baseline age younger than 70 years,16,20,25,26,28,39,40,49,52,55,60,65 between 70 and 74.9 years,5,10,11,15,19,22,24,27,29,30,32–36,38,41,46,47,50,51,59,61,63,66–68,72 and older than 75 years, respectively.4,10,21,22,37,42–44,53,62,64 Outcomes were similar in a second analysis in which studies were clustered in terciles from youngest reported age to oldest reported age: The first 18 studies had an age range from 53.4 to 70.5 years,15,16,20,25,26,28,39,40,49,52,55,59,63,65,66 the second 17 studies had a range from 70.6 to 74.0 years,5,10,19,22,24,27,30,32–36,41,47,51,67,68,72 and the third 18 studies had an age range of 74.3 to 80.9 years.4,10,11,21,22,29,37,38,42–44,46,50,53,61,62,64
Due to limitations in data reporting across studies, we could not properly address whether prior therapy or surgery affects postoperative IOP and medication use. Nevertheless, findings from some of the studies in our analysis are illustrative. In a series of 259 eyes, 91 of which were followed to 12 months, there was similar efficacy in IOP reduction among eyes with or without prior glaucoma filtration surgery, and no difference in number of medications used postoperatively, rates of bleb management, or rates of adverse events.84 Laborda-Guirao et al found greater IOP reduction in eyes with previous surgery (32.3%) compared to eyes without (24.3%), although the difference was not statistically significant.47 In the latter, there was also no difference in outcomes among implants placed in the inferior quadrants versus superior, suggesting the ability to use the gel stent in eyes where the superior quadrants are unsuitable for conjunctival manipulation due to a previous filtration surgery. Hengerer et al compared the effectiveness of the gel stent in 45 eyes with no prior glaucoma intervention and 103 eyes which previously failed a prior glaucoma intervention (trabeculectomy [n = 31], micro-bypass stent [n = 31], cyclophotocoagulation [n = 24], phacoemulsification [n = 11], and laser [n = 6]). In that study, IOP was reduced in eyes without and with prior interventions from 36.0±10.7 mm Hg on 3.6±0.8 medications and 31.6±8.9 mm Hg on 3.0 ± 1.0 medications at baseline, respectively, to 14.2 ± 3.4 mm Hg on 0.3±0.7 medications and 14.3±4.2 mm Hg on 0.3±0.7 medications at 12 months, respectively.85 Widder et al compared outcomes in a group of eyes receiving a gel stent after previous failed trabeculectomy (Group 1; n = 30) and a group of eyes with no previous surgery (Group 2; n = 60). In that study, preoperative IOP was 24.6±4.7 mm Hg and 24.3±6.2 mm Hg in Group 1 and Group 2, respectively; postoperative IOP was 13.7±5.0 mm Hg and 14.2±3.7 mm Hg in Group 1 and Group 2, respectively. Medication use was reduced from 2.9±1.1 at baseline in Group 1 to 0.5± 1.1 postoperatively, and from 2.7±1.2 at baseline in Group 2 to 0.3±0.6 postoperatively.70 Karimi et al reviewed outcomes in 17 eyes receiving a gel stent after a prior failed trabeculectomy. IOP was reduced from 21.5±2.4 mm Hg preoperatively to 13.6±3.4 mm Hg at month 12 (P < 0.05), and medication use was reduced from 2.8±0.6 at baseline to 1.0±1.3 at month 12 (P < 0.05).45
Interpretations
Neither baseline IOP or age at enrollment influenced postoperative IOP or postoperative medication use. A history of prior intervention does not appear to influence outcomes after gel stent implantation. Our analyses by baseline factors align with the outcomes from analyses at 12, 24, and 36 months of follow-up and among prospective and retrospective studies. Nevertheless, more data among these subpopulations would be helpful in predicting likely outcomes after gel stent surgery.
Our analyses could not identify any other meaningful predictors of postoperative IOP and medication use. For example, only a few studies assessed outcomes in non-Caucasian populations,28,48 and one additional study noted that stratification by ethnicity had no impact on either diurnal IOP reduction or achieving 20% or greater IOP reduction on the same or fewer medications.15 On the other hand, Schlenker found that white ethnicity was associated with a decreased rate of failure (crude hazard ratio [HR], 0.49; 95% CI, 0.30–0.81; adjusted HR, 0.49; 95% CI, 0.25–0.96).16 Based on the limited information available, we are not able to draw conclusions about outcomes according to ethnicity.
Is There Any Evidence of a Difference in Outcomes in Standalone versus Combination Procedures?
To ensure a balanced analysis of outcomes in combined and standalone gel stent surgeries, we restricted the analysis to 10 studies reporting complete pre- and postoperative IOP and medication use in standalone gel stent implantation, in combination with cataract surgery, and in the overall population.5,17,19,30,47,53,54,56,64,83 Outcomes with respect to IOP lowering and reduction in medication use were consistent with other analyses performed in this systematic review (Table 6).
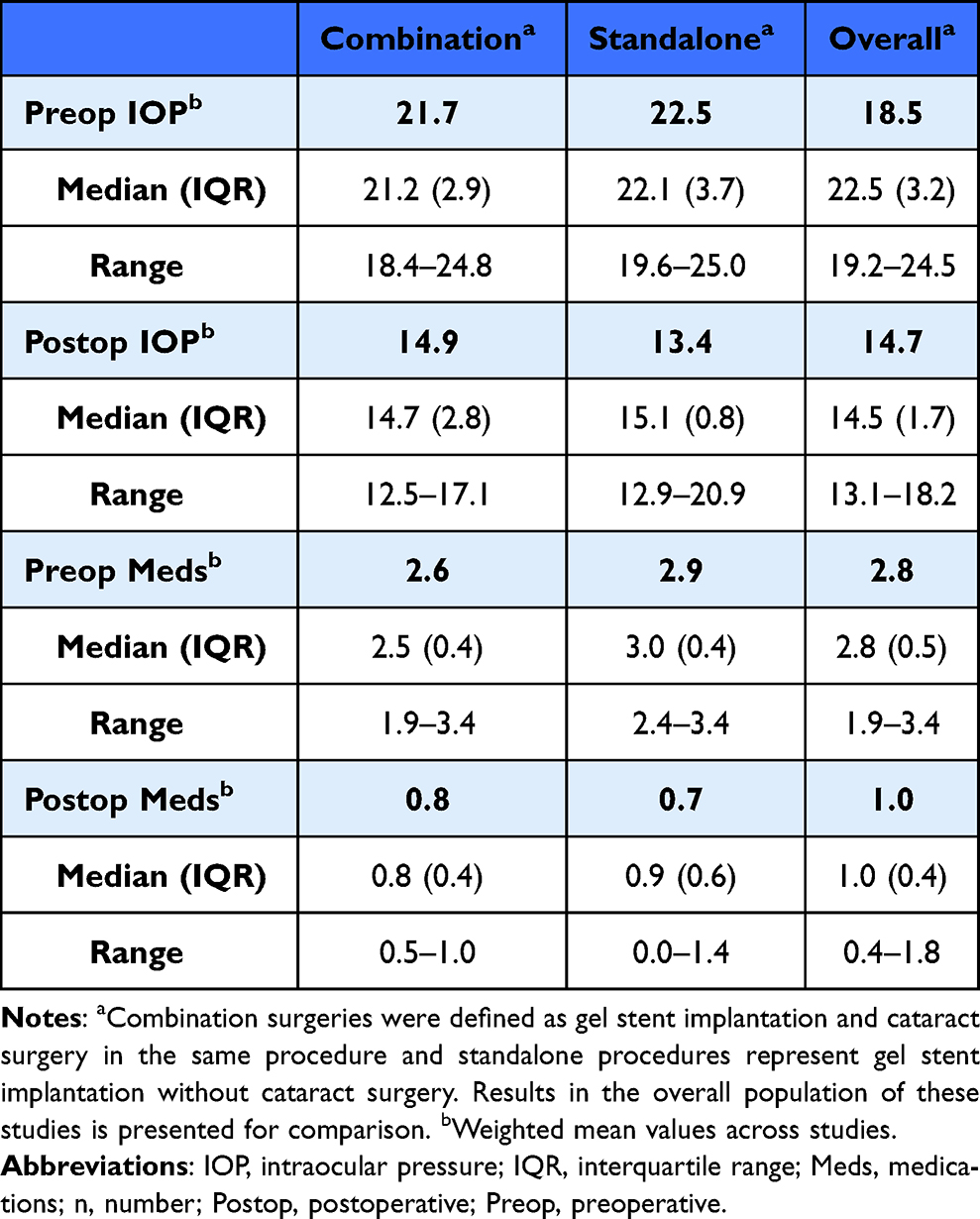 |
Table 6 Summary of Median Outcomes for Postoperative IOP and Medication Use Among 11 Studies Reporting Outcomes in the Overall Population, as Well as in Combination and Standalone Surgeries |
Interpretations
The available evidence suggests that surgeons can choose to use the gel stent as a standalone procedure or in combination with cataract extraction.
While we found little difference in studies comparing standalone and combination procedures, some authors have reported better success rates associated with standalone gel stent procedures.5,10,70 Fea et al reported lower week 1 IOP among standalone procedures, but no difference at any other timepoint, as well as greater mean IOP and medication reduction from baseline to final follow-up among standalone compared to combination procedures.5 In a retrospective case series, compared to combined procedures, standalone procedures yielded lower IOP and a greater percentage of patients achieving ≤18 mm Hg, ≤15 mm Hg, and ≤12 mm Hg at 12 months; however, intergroup differences were not statistically significant.4 Karimi reported a higher percentage of patients using zero medications after standalone procedures (53.4%) compared to combined gel stent and cataract surgery (41.1%), but no difference in mean IOP or number of glaucoma medications after 18 months of follow-up.46 A larger IOP-lowering effect associated with standalone compared to combination procedures was found in two studies.10,47 By comparison, Barao et al reported a non-statistically significant trend for greater IOP-lowering and medication-sparing effects in combination procedures compared to standalone.24 Other studies, however, noted no difference between groups of patients after standalone or combination procedures.46,58,86
Information on need for reoperation is available from a few select studies. In a study of 171 eyes, Fea et al found that the need for secondary surgical intervention (SSI) was low overall (12%) and numerically higher in a group of eyes after standalone gel stent surgery (n = 8) versus combination surgery group (n = 4).5 Lenzhofer noted five patients requiring SSI (7%) among those undergoing standalone procedures and zero in those undergoing combination procedures (P = 0.058).17 Reitsamer found a numerically higher survival probability in maintaining overall success (defined as ≥20% IOP reduction from medicated baseline without need for a second surgery, clinical hypotony, or topical IOP-lowering medications) at 3 years associated with standalone compared to combination procedures.12 Mansouri et al reported 5 eyes in a standalone group and 12 eyes in a combination group (P = 0.63) as total failures, defined as the need for reoperation due to uncontrolled IOP (n = 16) or persistent bleb leak (n = 1).10 Poelman et al found no difference in SSI rates between eyes undergoing solo or combination procedures.54
The minimal differences noted in our aggregate analysis are not entirely unsurprising considering how the gel stent directs aqueous flow dynamics. Cataract surgery is well known to have positive benefits for lowering IOP.87 While the exact IOP-lowering mechanism is unknown, cataract surgery is understood to improve trabecular outflow in some manner. Such changes in outflow facility may be irrelevant after placement of a gel stent, as outflow is intended to bypass the conventional outflow pathway structures. Because of its similar outflow mechanism, outcomes from trabeculectomy with or without cataract surgery might provide some insight. According to a Consensus Report from the World Glaucoma Association, phacotrabeculectomy appears to be less effective at reducing IOP than trabeculectomy alone in OAG.88
Does IOP Response or Effect on Postoperative Medication Use Differ According to Glaucoma Type?
A limited number of studies reported outcomes among eyes diagnosed with POAG compared to PEXG (Table 7).11,22,36,89,90 Similarly, data are limited but nonetheless encouraging in the setting of uveitic glaucoma. Qureshi et al reported outcomes in an observational case series of 37 eyes with medically uncontrolled glaucoma secondary to uveitis. Mean IOP was reduced from 36.1±9.6 mm Hg on 3.69±0.46 glaucoma medications at baseline to 12.63±4.13 mm Hg on 0.62±1.1 glaucoma medications at 12 months.56 In an exploratory prospective case series of gel stent implantation in 24 eyes to treat uncontrolled uveitic glaucoma, mean IOP was 30.5±9.8 mm Hg at baseline and mean glaucoma medication use 3.3±0.8; at 12 months, mean IOP was 12.2±3.1 mm Hg, and mean glaucoma medication use was 0.4±0.9.91
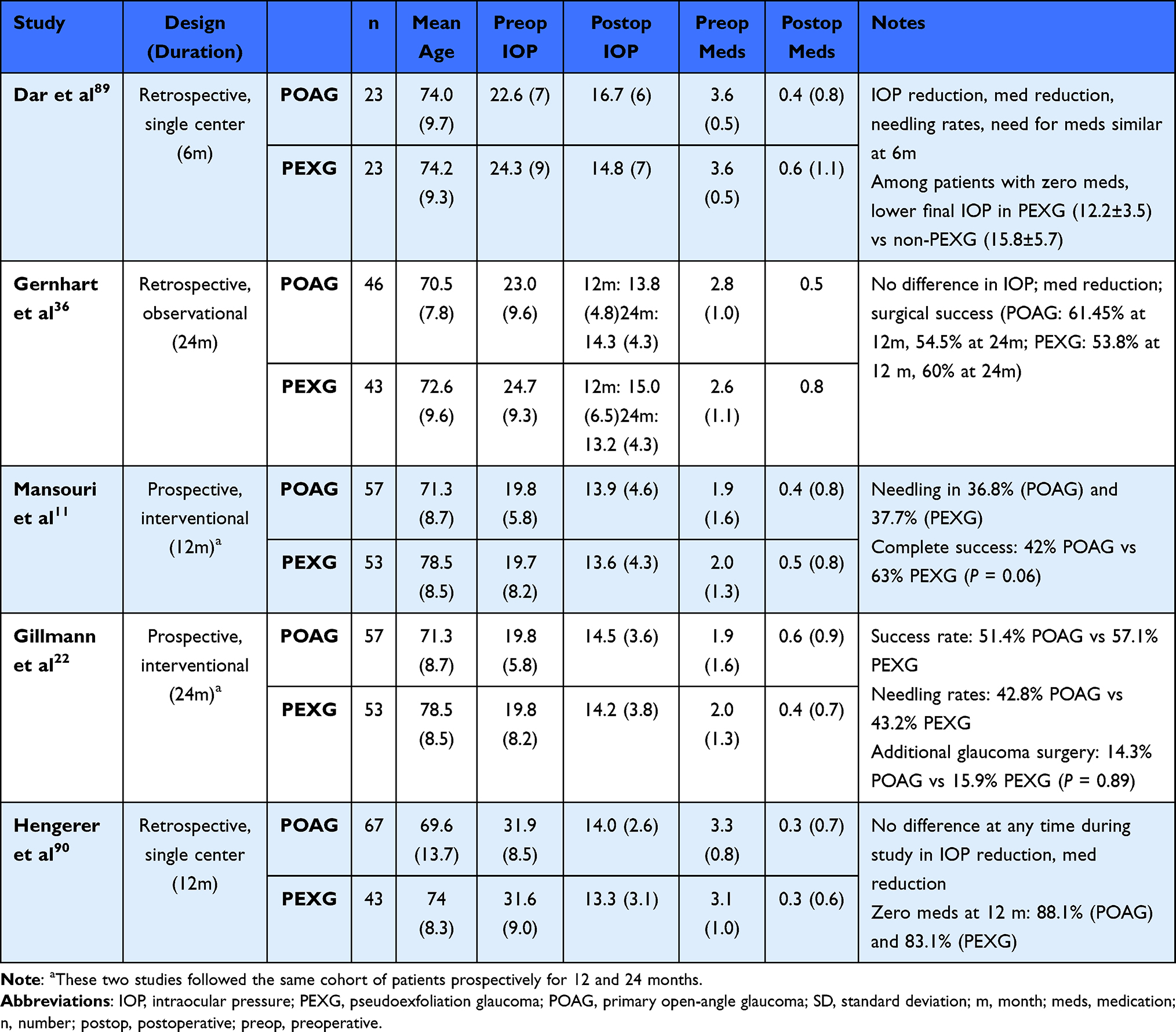 |
Table 7 Studies Reporting Outcomes in Eyes with POAG and PEXG |
Interpretations
The available evidence supports the use of the gel stent in patients with both primary and secondary OAG. Given that pseudoexfoliation is a risk factor for rapid glaucomatous progression,92 more data on the gel stent in this glaucoma subtype are needed. A higher success rate in POAG eyes compared to PEXG eyes was found in one study, but the results were not statistically significant.27 Other studies have reported no difference in success rates.25,36,57
In a study reporting outcomes after a single gel stent implant in different types of primary and secondary glaucomas, Schargus et al reported reduction in mean IOP and medication use across all treatment groups from baseline to 12 months: POAG (22.8±6.5 mm Hg and 2.5±1.2 medications to 15.1±4.6 mm Hg and 0.8±1.3 medications); normal-tension glaucoma (16.6±3.4 mm Hg and 2.6± 0.9 medications to 11.6±2.2 mm Hg and 0.6±0.9 medications); PEXG (28.0±7.9 mm Hg and 2.9±1.2 medications to 17.1±6.6 mm Hg and 1.0±1.3 medications); and secondary glaucoma (28.9±13.9 mm Hg and 2.7±0.9 medications to 15.5±6.9 mm Hg and 0.9±1.4 medications).59
The positive effect of gel stent in differing glaucoma subtypes is perhaps unsurprising given its intended mechanism of directing aqueous drainage. Similar to trabeculectomy, the gel stent creates a non-physiological pathway that bypasses traditional outflow, albeit with a more favorable safety profile. As a consequence, the gel stent consistently achieves sustained IOP in the mid-to-low teens,58 which is lower than the expected outcome after MIGS options targeting the trabecular meshwork and/or Schlemm canal.93–96 Intuitively, the gel stent should achieve these effects regardless of the glaucoma etiology.
Does Use of an Ab Interno or Ab Externo Approach, or Employment of Open (Subtenon) versus Closed Conjunctiva (Subconjunctival) Placement, Affect IOP Response and Medication Reduction Postoperatively?
At the time of our systematic review, there were two studies that compared outcomes after ab externo versus ab interno delivery of the implant19,20 and one study that compared outcomes after gel stent implantation in eyes operated with an open (subtenon) or closed (subconjunctival) technique.97 There were two retrospective analyses of outcomes with an open technique (subtenon placement) published after the cutoff date for the current review.98,99 As these data pertain to a key clinical question on the use of the gel stent in clinical practice, findings from the one study comparing open (subtenon) versus closed conjunctiva (subconjunctival) gel stent placement are reviewed below, while select findings from the other four studies are shown in Table 8. In addition, the authors are aware of one additional study reporting 12-month outcomes after ab externo delivery, but it was unavailable at the time of our systematic analysis.100
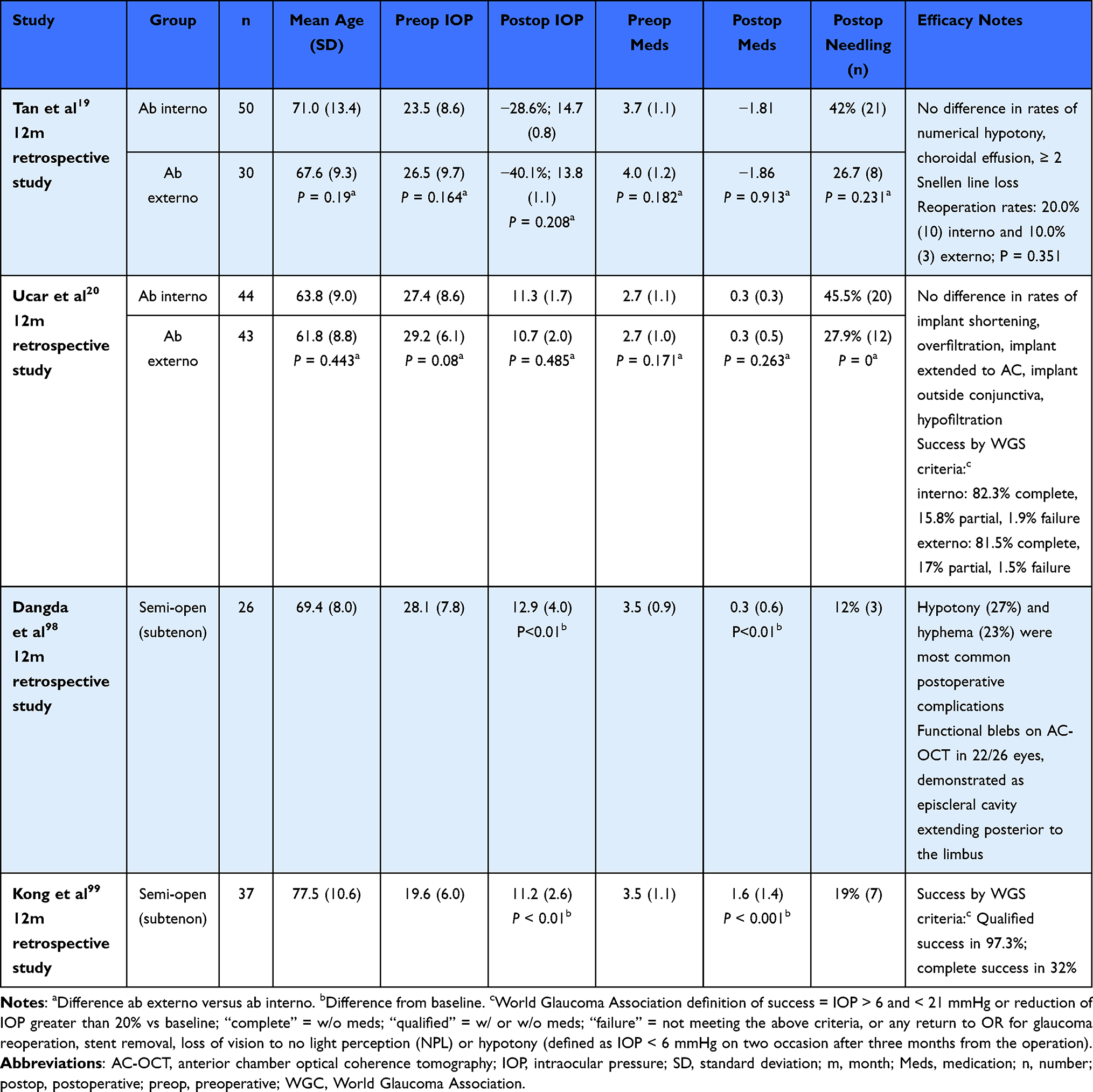 |
Table 8 Key Outcomes in Studies Reviewing Ab Interno versus Ab Externo Surgeries and Semi-Open (Subtenon) Placement |
Do et al compared outcomes after gel stent implantation in eyes operated with an open (subtenon) or closed (subconjunctival) technique. Preoperative IOP was statistically significantly higher in the open group (n = 76; 26.4±8.6 mm Hg) compared to the closed group (n = 61; 23.0±7.8 mm Hg; P = 0.01), and the former was more likely to have had a prior incisional glaucoma surgery (20% vs 5%; P = 0.01). Preoperative medication use was similar, 3.6±0.11 in the open group 3.6±0.14 in the closed group. The 12-month postoperative IOP in the closed group (n = 26) was 17.0±9.5 mm Hg on 1.8±1.6 glaucoma medications. In the open group, the 12-month postoperative IOP was 13.6±6.3 mm Hg on 0.9±1.4 glaucoma medications (P = 0.02 vs closed group). Compared to the closed group, the open group had significantly greater percent IOP reduction from baseline (24.8% vs 43.1%; P = 0.02) and required fewer medications at 3 months (1.2 vs 0.6, P = 0.02) and 12 months (1.8 vs 0.9, P = 0.02). The open technique was also associated with a lower rate of postoperative needling (11.8%) compared to the closed technique (36.1%; P = 0.001). The authors speculated that opening the conjunctiva, coupled with the more extensive dissection of Tenon, allowed for more consistent placement of the gel stent implant, which in turn resulted in reduced risk for intra- and postoperative occlusion.97
Interpretations
At the current time, there is not enough evidence to clearly state that an open approach is favorable compared to a closed, and longer-term follow-up from the study mentioned above is forthcoming. The ability to utilize various techniques (open versus closed, ab interno vs ab externo) permits surgeons greater flexibility in determining an appropriate surgical plan for the individual patient.
There are some theoretical advantages in using an ab externo approach: The target area for implantation is expanded, corneal incisions are not required, viscoelastic use is optional, intraocular maneuvers are minimized, the learning curve is shorter, and there is less chance the distal end of the implant will become embedded in the Tenon layer.101 Ab externo placement may be performed with or without opening of the conjunctiva.6
While surgical approach is important, the overall goal of a gel stent surgery is to achieve proper placement of the device to optimize outflow performance. According to the manufacturer, 1-2-3 positioning with a free and mobile stent is most likely to achieve the desired outflow postoperatively: The proximal end of the implant should extend 1.0 mm into the anterior chamber, 2.0 mm of the implant should reside in the scleral tunnel, and the distal end should be 3.0 mm into the subconjunctival space.102 Optimal results can be achieved when the device is patent, well-positioned, and no viscoelastic is retained in the anterior chamber.29 Primary needling at the time of gel stent implantation may be beneficial in leading to a free and mobile implant, with one study showing that it substantially reduced the need for postoperative needling (3.9% vs 25.7%; P = 0.003).103
Is There Any Consensus on Optimal Use of Anti-Metabolites in Conjunction with Gel Stent Implantation?
We were able to calculate the absolute mean dose of mitomycin C (MMC) based on full reporting of dosage used in 37 studies that also recorded pre- and postoperative IOP and medication use. Among 14 studies using an absolute dose of 10 µg, the weighted mean average IOP was reduced from 24.4 mm Hg on 2.7 medications at baseline to 15.2 mm Hg on 0.7 medications at the end of follow-up.5,24,26,28–30,32–36,89,104 Among 21 studies using an absolute dose of 20 µg, the weighted mean average IOP was reduced from 21.6 mm Hg on 2.7 medications at baseline to 14.4 mm Hg on 0.8 medications at the end of follow-up.5,10,15,21,24,28,33,34,44–48,50,54–56,60,63,65,68 Only two studies were available with a calculated mean dose of 40 µg; due to the paucity of data, these data are not shown.49,62 Additional studies using other absolute mean doses were identified: ~25 µg and 30 µg; however, due to incomplete data reporting, these studies were not included in this analysis. Among the group of studies with a calculated absolute dose of 10 µg, 10 also reported the needling rate; the range of reported needling rates was 2.5%30 to 62.0%.57 Among studies with a calculated absolute dose of 20 µg, all 21 also reported the needling rate; the range of reported needling rates was 8.8%47 to 46.2%.5
Interpretation
There is no consensus on optimal use of anti-metabolites in conjunction with gel stent implantation; however, there appears to be a trend between the use of mitomycin and postoperative IOP. A more complete discussion of needling rates is included in the following section.
What is the Available Evidence on the Need for Needling Following Gel Stent Surgery?
A wide range of needling rates has been reported in the literature, as low as 2.5%30 to as high as 67%.49 In 59 studies reporting needling rates, the median needling rate was 34%. There was notable heterogeneity in the timing to first needling, how the procedure was performed (including use of antifibrotic), and whether and how frequently needling was repeated. Most interventions occur within the first 1–3 months after the initial surgery.4,10,11,25,27,35,38–40,44,46,57,58 Repeated needling in the same eye was consistently reported.5,27 Use of a 27- or 30-gauge needle for the procedure is typically preferred.10,11,35,46,86 Across studies, various other nuances of needling were described, including approaches with and without antifibrotics; use of pharmacologic measures for bleb revision as an alternative to needling; varied use of adjuncts (MMC, fluorouracil [5-FU], bevacizumab, other); and different settings for performing needling (ie, in the clinic vs repeat visits to the operating room).
Interpretations
The available data support adopting a low barrier for initiating needling in clinical practice, and whether and how many times it is repeated should be dictated by the individual patient’s clinical profile and the surgeon’s judgment. In our review, most needling interventions were performed in the first 1 to 3 months postoperatively, although some studies reported needling 12 or 17 months after the initial surgery.24,25 By comparison, time to needling following trabeculectomy is about 4.5 months.105,106 Across studies, needling was usually performed only once; however, multiple needling interventions in the same eye were consistently reported. Studies in eyes following trabeculectomy have found that an increased number of needlings was associated with surgical failure, presumably due to increased risk for scarring and fibroblastic proliferation.107 Whether these findings are applicable for gel stent blebs is not clear, although it is likely that repeated needling of gel stent blebs contributes a similar risk for scarring.
Whether the requirement for needling in the postoperative period is considered a complication of surgery is controversial. Some authors contend that needling of a scarred filtering bleb is the preferred first-line approach to rescue failing blebs and delay additional surgery, and therefore should not be considered a complication.10,16,38 In the context of incisional surgery, the American Academy of Ophthalmology Preferred Practice Patterns state that bleb needling is part of periopostoperative care to improve aqueous flow and lower IOP as necessary, based on the physician’s assessment of bleb function.108 Furthermore, needling post-trabeculectomy has been found to be effective in lowering IOP at 12 months, and needling with adjunctive use of 5-FU is more effective than medical treatment in lowering IOP at 12 months.109 Similar findings have been found after needling revision following gel stent implantation, with most studies noting that the procedure is relatively safe and associated with low risk of implant amputation and hypotony. When successful, needling optimizes outflow dynamics, yielding up to 40% IOP lowering compared with preneedling values.84
Data on alternative options to needling are limited. In a retrospective study of 5-FU used alone as an alternative to needling in 39 eyes, Walek et al reported a 69% unqualified success rate (postoperative IOP < 18 mm Hg and >20% reduction from baseline without any antiglaucoma medication use and no evidence of progression); however, the low number of patients and a lack of a comparison group suggest that more data are needed.69 One retrospective study found more favorable survival rates and lower reintervention rates associated with open filtering bleb revision compared to needling; however, high patient attrition and nonstandardized methodology hamper the ability to make definitive comparisons.110 In a retrospective series of 151 eyes, 13.9% (n = 21) underwent revision surgery for a persistently elevated bleb. Among eyes followed after revision surgery for 1 year, 16 patients had a mean IOP of 26.1±8.3 mm Hg on 2.0 drops prerevision and a mean IOP of 16.3±3.7 mm Hg on 0.7 drops after 12 months of follow-up.111 In a separate prospective case series of 221 eyes, postoperative needling was not performed, and instead patients were subjected to a second surgery in which the conjunctiva of the bleb area was opened, followed by mechanical removal of all tissue adhesions.54 In our opinion, the latter exposes patients to new intra- and postoperative risks that can be avoided with needling.
Taken together, there is no consensus on the expected rate of needling in the gel stent postoperative period. Furthermore, needling is associated with a favorable risk-benefit ratio, with a low potential for adverse outcomes and a high probability of improving the clinical course. The data suggest a reasonable probability that needling will be required after gel stent implantation, but the number of needlings is variable and contextual. Because elevated IOP secondary to an encapsulated bleb contributes to a vicious cycle of ever-increasing IOP, needling may be considered an expected part of postoperative management to decrease the potential for surgical failure. Given the suggestion of benefit, primary needling at the time of gel stent implantation should be considered, as it is associated with a significant reduction in the need for postoperative needling and postoperative clinic visits,103 especially in eyes at risk for postoperative bleb failure or occlusion of the stent.84
Conclusions
This systematic review of the literature demonstrates consistent IOP of around 14.0 mm Hg with use of around 1 glaucoma medication after successful gel stent surgery in studies reporting outcomes in a wide range of glaucoma types and severity at 12, 24, and 36 months of follow-up; in both prospective and retrospective study designs; regardless of baseline age or baseline; irrespective of whether the procedure was performed in a standalone setting or combined with cataract surgery; and in cases where either an ab interno or ab externo surgical technique was employed. It provides additional evidence to support the use of anti-metabolites at the time of surgery to reduce the risk of postoperative fibrosis and to promote healing; however, data are inconclusive on ideal dosing and delivery. The perception of postoperative needling has evolved, from once being considered a safety consideration in US registration clinical trials to being deemed part of periopostoperative care to improve aqueous flow and lower IOP as necessary as per real-world practices.
Precis
A systematic review of published studies on the Xen45 gel stent suggests a high likelihood of achieving postoperative IOP of approximately 14.0 mm Hg with requirement for fewer than 1 supplemental glaucoma medication.
Abbreviations
5-FU, Fluorouracil; HR, hazard ratio; MMC, mitomycin; POAG, primary open-angle glaucoma; PEXG, pseudoexfoliative glaucoma; SSI, secondary surgical intervention.
Data Sharing Statement
Data used for the research described herein was acquired by the authors by searches on publicly available online libraries.
Ethics Approval and Informed Consent
This formulation of this manuscript did not involve research on humans or animals.
Consent for Publication
Consent is not required to publish any information herein.
Acknowledgments
Editorial assistance in the preparation of this article was provided by Bryan Bechtel of Bryn Mawr Communications, LLC. Support for this assistance was funded by Allergan, an AbbVie Company.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This review was supported by Allergan plc, Dublin, Ireland (prior to its acquisition by AbbVie Inc.). The sponsor participated in the writing, reviewing, and approval of the final version of the manuscript. Neither honoraria nor payments were made for authorship.
Disclosure
Richard Fiscella is an employee of AbbVie, Inc. and may hold AbbVie stock. Brian A. Francis is a consultant for Allergan/AbbVie, Bausch & Lomb, BVI Endo Optiks, IStar, Ivantis, Iridex, MST, Thea; Speaker for Aerie. Robert J. Noecker reports consulting Fee from Alcon, Aerie, Allergan, Alimera, Beaver-Visitec, Glaukos, Iridex, Ocular Therapeutics, Santen, Thea, Kala, New World Medical, Oysterpoint, Sight Sciences, Science Branding, iStar, MST; Speakers Bureau for Allergan, Alcon, Beaver-Visitec, Iridex, Quantel, Imprimis, Kala, Nova Medical, Sight Sciences; Contracted Research for Allergan, Glaukos, Nova Medical; Equity Owner of Ocular Therapeutics, Tula Medical, ISP Surgical, Mati. Joseph F. Panarelli reports personal fees from AbbVie, Aerie, CorneaGen, Glaukos, Santen, New World Medical, Allergan, Nova Eye Medical, AOI Ophthalmics. Nathan Radcliffe reports personal fees from Alderya, AbbVie, Alcon, Allergan, Alimera, Aerie, Avellino, Bausch & Lomb, Beaver Visitec, Belkin, CATS, Carl Zeiss Meditec, Elios Vision, Equinox, Eyenovia, Eyepoint, Expert Opinion, Glaukos, Imprimis, Iridex, Ivantis, IrisVision, Lumenis, New World Medical, Novartis, Ocular Therapeutix, Regeneron, Reichert, Shire, Sight Sciences, SpyGlass, Tarsus, Thea, Tearclear, ViaLase. Arsham Sheybani is a consultant for Allergan/AbbVie, Alcon, Nova Eye, Santen, New World Medical. Oluwatosin U. Smith is a consultant for Alcon, Allergan, Iridex, Santen, New World Medical, Glaukos; Speaker & consultant for Aerie, Bausch & Lomb; Stocks from Nova Eye Medical. Vanessa Vera is an employee of AbbVie, Inc. and may hold AbbVie stock. The authors report no other conflicts of interest in this work.
References
1. Sheybani A, Lenzhofer M, Hohensinn M, Reitsamer H, Ahmed II. Phacoemulsification combined with a new ab interno gel stent to treat open-angle glaucoma: pilot study. J Cataract Refract Surg. 2015;41(9):1905–1909. doi:10.1016/j.jcrs.2015.01.019
2. Lenzhofer M, Strohmaier C, Hohensinn M, et al. Longitudinal bleb morphology in anterior segment OCT after minimally invasive transscleral ab interno Glaucoma Gel Microstent implantation. Acta Ophthalmol. 2019;97(2):e231–e237. doi:10.1111/aos.13902
3. Shaarawy TM, Moschos MM, Sherwood MB. New glaucoma surgical alternatives. In: Shaarawy TM, Sherwood MB, Hitchings RA, Crowston JG, editors. Glaucoma.
4. Rather PA, Vold S, McFarland M. Twelve-month outcomes of an ab interno gelatin stent combined with cataract surgery or as a standalone procedure in pseudophakic eyes with open-angle glaucoma. J Cataract Refract Surg. 2020;46(8):1172–1177. doi:10.1097/j.jcrs.0000000000000286
5. Fea AM, Bron AM, Economou MA, et al. European study of the efficacy of a cross-linked gel stent for the treatment of glaucoma. J Cataract Refract Surg. 2020;46(3):441–450. doi:10.1097/j.jcrs.0000000000000065
6. Panarelli JF, Yan DB, Francis B, Craven ER. XEN gel stent open conjunctiva technique: a practical approach paper. Adv Ther. 2020;37(5):2538–2549. doi:10.1007/s12325-020-01278-1
7. Lewis RA. Ab interno approach to the subconjunctival space using a collagen glaucoma stent. J Cataract Refract Surg. 2014;40(8):1301–1306. doi:10.1016/j.jcrs.2014.01.032
8. Sheybani A, Reitsamer H, Ahmed II. Fluid dynamics of a novel micro-fistula implant for the surgical treatment of glaucoma. Invest Ophthalmol Vis Sci. 2015;56(8):4789–4795. doi:10.1167/iovs.15-16625
9. McLaren JW. Measurement of aqueous humor flow. Exp Eye Res. 2009;88(4):641–647. doi:10.1016/j.exer.2008.10.018
10. Mansouri K, Guidotti J, Rao HL, et al. Prospective evaluation of standalone XEN gel implant and combined phacoemulsification-XEN gel implant surgery: 1-year results. J Glaucoma. 2018;27(2):140–147. doi:10.1097/ijg.0000000000000858
11. Mansouri K, Gillmann K, Rao HL, Guidotti J, Mermoud A. Prospective evaluation of XEN gel implant in eyes with pseudoexfoliative glaucoma. J Glaucoma. 2018;27(10):869–873. doi:10.1097/ijg.0000000000001045
12. Reitsamer H, Vera V, Ruben S, et al. Three-year effectiveness and safety of the XEN gel stent as a solo procedure or in combination with phacoemulsification in open-angle glaucoma: a multicentre study. Acta Ophthalmol. 2022;100(1):e233–e245. doi:10.1111/aos.14886
13. Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–814.e1. doi:10.1016/j.ajo.2011.10.024
14. Zahid S, Musch DC, Niziol LM, Lichter PR. Risk of endophthalmitis and other long-term complications of trabeculectomy in the Collaborative Initial Glaucoma Treatment Study (CIGTS). Am J Ophthalmol. 2013;155(4):674–680, 680.e1. doi:10.1016/j.ajo.2012.10.017
15. Grover DS, Flynn WJ, Bashford KP, et al. Performance and safety of a new ab interno gelatin stent in refractory glaucoma at 12 months. Am J Ophthalmol. 2017;183:25–36. doi:10.1016/j.ajo.2017.07.023
16. Schlenker MB, Gulamhusein H, Conrad-Hengerer I, et al. Efficacy, safety, and risk factors for failure of standalone ab interno gelatin microstent implantation versus standalone trabeculectomy. Ophthalmology. 2017;124(11):1579–1588. doi:10.1016/j.ophtha.2017.05.004
17. Lenzhofer M, Strohmaier C, Hohensinn M, et al. Change in visual acuity 12 and 24 months after transscleral ab interno glaucoma gel stent implantation with adjunctive Mitomycin C. Graefes Arch Clin Exp Ophthalmol. 2019;257(12):2707–2715. doi:10.1007/s00417-019-04452-6
18. Urcola A, Garay-Aramburu G. Safety and efficacy of bilateral simultaneous XEN implant surgery: a pilot study. Int Ophthalmol. 2021;41(3):859–866. doi:10.1007/s10792-020-01640-w
19. Tan NE, Tracer N, Terraciano A, Parikh HA, Panarelli JF, Radcliffe NM. Comparison of safety and efficacy between ab interno and ab externo approaches to XEN gel stent placement. Clin Ophthalmol. 2021;15:299–305. doi:10.2147/opth.s292007
20. Ucar F, Cetinkaya S. Xen implantation in patients with primary open-angle glaucoma: comparison of two different techniques. Int Ophthalmol. 2020;40(10):2487–2494. doi:10.1007/s10792-020-01427-z
21. Gillmann K, Bravetti GE, Rao HL, Mermoud A, Mansouri K. Bilateral XEN stent implantation: a long-term prospective study of the difference in outcomes between first-operated and fellow eyes. J Glaucoma. 2020;29(7):536–541. doi:10.1097/ijg.0000000000001520
22. Gillmann K, Bravetti GE, Mermoud A, Rao HL, Mansouri K. XEN gel stent in pseudoexfoliative glaucoma: 2-year results of a prospective evaluation. J Glaucoma. 2019;28(8):676–684. doi:10.1097/ijg.0000000000001295
23. Vera V, Shah M. Navigating challenges after xen. Curr Trends Ophthalmol. 2021;4(1):17. doi:10.18314/ctoy.v4i1.2078
24. Barão RC, José P, Teixeira FJ, Ferreira NP, Sens P, Pinto LA. Automated gonioscopy assessment of XEN45 gel stent angle location after isolated XEN or combined phaco-XEN procedures: clinical implications. J Glaucoma. 2020;29(10):932–940. doi:10.1097/ijg.0000000000001582
25. Başer EF, Seymenoğlu RG. Results of fluorouracil-augmented Xen45 implantation in primary open-angle and pseudoexfoliation glaucoma. Int Ophthalmol. 2021;41(3):945–955. doi:10.1007/s10792-020-01650-8
26. Buffault J, Graber M, Bensmail D, et al. Efficacy and safety at 6 months of the XEN implant for the management of open angle glaucoma. Sci Rep. 2020;10(1):4527. doi:10.1038/s41598-020-61319-1
27. Busch T, Skiljic D, Rudolph T, Bergström A, Zetterberg M. Learning curve and one-year outcome of XEN 45 gel stent implantation in a Swedish population. Clin Ophthalmol. 2020;14:3719–3733. doi:10.2147/opth.s267010
28. Chao YJ, Ko YC, Chen MJ, Lo KJ, Chang YF, Liu CJ. XEN45 Gel Stent implantation in eyes with primary open angle glaucoma: a study from a single hospital in Taiwan. J Chin Med Assoc. 2021;84(1):108–113. doi:10.1097/jcma.0000000000000430
29. Cutolo CA, Iester M, Bagnis A, et al. Early postoperative intraocular pressure is associated with better pressure control after XEN implantation. J Glaucoma. 2020;29(6):456–460. doi:10.1097/ijg.0000000000001501
30. De Gregorio A, Pedrotti E, Russo L, Morselli S. Minimally invasive combined glaucoma and cataract surgery: clinical results of the smallest ab interno gel stent. Int Ophthalmol. 2018;38(3):1129–1134. doi:10.1007/s10792-017-0571-x
31. Fea AM, Spinetta R, Cannizzo PML, et al. Evaluation of bleb morphology and reduction in IOP and glaucoma medication following implantation of a novel gel stent. J Ophthalmol. 2017;2017:9364910. doi:10.1155/2017/9364910
32. Fernández-García A, Zhou Y, García-Alonso M, Andrango HD, Poyales F, Garzón N. Medium-term clinical outcomes following Xen45 device implantation. Int Ophthalmol. 2020;40(3):709–715. doi:10.1007/s10792-019-01232-3
33. Gabbay IE, Allen F, Morley C, Pearsall T, Bowes OM, Ruben S. Efficacy and safety data for the XEN45 implant at 2 years: a retrospective analysis. Br J Ophthalmol. 2020;104(8):1125–1130. doi:10.1136/bjophthalmol-2019-313870
34. Gabbay IE, Goldberg M, Allen F, et al. Efficacy and safety data for the Ab interno XEN45 gel stent implant at 3 years: a retrospective analysis. Eur J Ophthalmol. 2021;11206721211014381. doi:10.1177/11206721211014381
35. Galal A, Bilgic A, Eltanamly R, Osman A. XEN glaucoma implant with mitomycin C 1-year follow-up: result and complications. J Ophthalmol. 2017;2017:5457246. doi:10.1155/2017/5457246
36. Gernhart M, Hohberger B, Laemmer R. Two-Year Follow-Up: therapeutic Success with Respect to Axial Length of Stand-Alone Xen45 Gel Stent Implantation and Combined Procedures. Einfluss der Achsenlänge auf die 2-Jahres-Erfolgsrate der Stand-alone- und mit Phako/HKL kombinierten Xen45-Gel-Stent implantation. Klin Monbl Augenheilkd. 2021;238(11):1240–1247. doi:10.1055/a-1328-2847
37. Gillmann K, Bravetti GE, Rao HL, Mermoud A, Mansouri K. Combined and stand-alone XEN 45 gel stent implantation: 3-year outcomes and success predictors. Acta Ophthalmol. 2021;99(4):e531–e539. doi:10.1111/aos.14605
38. Heidinger A, Schwab C, Lindner E, Riedl R, Mossböck G. A retrospective study of 199 Xen45 stent implantations from 2014 to 2016. J Glaucoma. 2019;28(1):75–79. doi:10.1097/ijg.0000000000001122
39. Hengerer FH, Kohnen T, Mueller M, Conrad-Hengerer I. Ab interno gel implant for the treatment of glaucoma patients with or without prior glaucoma surgery: 1-year results. J Glaucoma. 2017;26(12):1130–1136. doi:10.1097/ijg.0000000000000803
40. Hong K, Lind J, Sheybani A. Safety and efficacy outcomes of the Xen45 gel stent use for refractory glaucoma: a surgery series from surgeon trainees at a tertiary teaching hospital. Eye Vis. 2020;7:5. doi:10.1186/s40662-019-0171-0
41. Hu JY, Ang BCH, Yip LW. Efficacy of the XEN gel stent on intraocular pressure lowering in East Asian eyes. Int Ophthalmol. 2020;40(5):1191–1199. doi:10.1007/s10792-020-01284-w
42. Ibáñez-Muñoz A, Soto-Biforcos VS, Chacón-González M, et al. One-year follow-up of the XEN® implant with mitomycin-C in pseudoexfoliative glaucoma patients. Eur J Ophthalmol. 2019;29(3):309–314. doi:10.1177/1120672118795063
43. Ibáñez-Muñoz A, Soto-Biforcos VS, Rodríguez-Vicente L, et al. XEN implant in primary and secondary open-angle glaucoma: a 12-month retrospective study. Eur J Ophthalmol. 2020;30(5):1034–1041. doi:10.1177/1120672119845226
44. Kalina AG, Kalina PH, Brown MM. XEN(®) gel stent in medically refractory open-angle glaucoma: results and observations after one year of use in the United States. Ophthalmol Ther. 2019;8(3):435–446. doi:10.1007/s40123-019-0192-8
45. Karimi A, Hopes M, Martin KR, Lindfield D. Efficacy and safety of the ab-interno xen gel stent after failed trabeculectomy. J Glaucoma. 2018;27(10):864–868. doi:10.1097/ijg.0000000000001044
46. Karimi A, Lindfield D, Turnbull A, et al. A multi-centre interventional case series of 259 ab-interno Xen gel implants for glaucoma, with and without combined cataract surgery. Eye. 2019;33(3):469–477. doi:10.1038/s41433-018-0243-8
47. Laborda-Guirao T, Cubero-Parra JM, Hidalgo-Torres A. Efficacy and safety of XEN 45 gel stent alone or in combination with phacoemulsification in advanced open angle glaucoma patients: 1-year retrospective study. Int J Ophthalmol. 2020;13(8):1250–1256. doi:10.18240/ijo.2020.08.11
48. Laroche D, Nkrumah G, Ng C. Real-world retrospective consecutive study of ab interno XEN 45 gel stent implant with mitomycin C in black and Afro-Latino patients with glaucoma: 40% required secondary glaucoma surgery at 1 year. Middle East Afr J Ophthalmol. 2019;26(4):229–234. doi:10.4103/meajo.MEAJO_126_19
49. Lewczuk K, Konopińska J, Jabłońska J, et al. XEN glaucoma implant for the management of operated uncontrolled glaucoma: results and complications during a long-term follow-up. J Ophthalmol. 2021;2021:2321922. doi:10.1155/2021/2321922
50. Mansouri K, Bravetti GE, Gillmann K, Rao HL, Ch’ng TW, Mermoud A. Two-year outcomes of XEN gel stent surgery in patients with open-angle glaucoma. Ophthalmol Glaucoma. 2019;2(5):309–318. doi:10.1016/j.ogla.2019.03.011
51. Nuzzi R, Gremmo G, Toja F, Marolo P. A retrospective comparison of trabeculectomy, baerveldt glaucoma implant, and microinvasive glaucoma surgeries in a three-year follow-up. Semin Ophthalmol. 2021;36(8):839–849. doi:10.1080/08820538.2021.1931356
52. Olgun A, Aktas Z, Ucgul AY. XEN gel implant versus gonioscopy-assisted transluminal trabeculotomy for the treatment of open-angle glaucoma. Int Ophthalmol. 2020;40(5):1085–1093. doi:10.1007/s10792-019-01271-w
53. Pérez-Torregrosa VT, Olate-Pérez Á, Cerdà-Ibáñez M, et al. Combined phacoemulsification and XEN45 surgery from a temporal approach and 2 incisions. Cirugía combinada mediante facoemulsificación e implante XEN45 con acceso temporal y 2 únicas incisiones. Arch Soc Esp Oftalmol. 2016;91(9):415–421. doi:10.1016/j.oftal.2016.02.006
54. Poelman HJ, Pals J, Rostamzad P, Bramer WM, Wolfs RCW, Ramdas WD. Efficacy of the XEN-implant in glaucoma and a meta-analysis of the literature. J Clin Med. 2021;10(5):1118. doi:10.3390/jcm10051118
55. Post M, Lubiński W, Śliwiak D, Podborączyńska-Jodko K, Mularczyk M. XEN Gel Stent in the management of primary open-angle glaucoma. Doc Ophthalmol. 2020;141(1):65–76. doi:10.1007/s10633-020-09753-4
56. Qureshi A, Jones NP, Au L. Urgent management of secondary glaucoma in uveitis using the Xen-45 gel stent. J Glaucoma. 2019;28(12):1061–1066. doi:10.1097/ijg.0000000000001389
57. Rauchegger T, Angermann R, Willeit P, Schmid E, Teuchner B. Two-year outcomes of minimally invasive XEN Gel Stent implantation in primary open-angle and pseudoexfoliation glaucoma. Acta Ophthalmol. 2021;99(4):369–375. doi:10.1111/aos.14627
58. Reitsamer H, Sng C, Vera V, Lenzhofer M, Barton K, Stalmans I. Two-year results of a multicenter study of the ab interno gelatin implant in medically uncontrolled primary open-angle glaucoma. Graefes Arch Clin Exp Ophthalmol. 2019;257(5):983–996. doi:10.1007/s00417-019-04251-z
59. Schargus M, Theilig T, Rehak M, Busch C, Bormann C, Unterlauft JD. Outcome of a single XEN microstent implant for glaucoma patients with different types of glaucoma. BMC Ophthalmol. 2020;20(1):490. doi:10.1186/s12886-020-01764-8
60. Scheres LMJ, Kujovic-Aleksov S, Ramdas WD, et al. XEN(®) Gel Stent compared to PRESERFLO™ MicroShunt implantation for primary open-angle glaucoma: two-year results. Acta Ophthalmol. 2021;99(3):e433–e440. doi:10.1111/aos.14602
61. Sharpe R, Pham G, Chang P. Comparison of ab interno XEN gelatin stent vs trabeculectomy with mitomycin C: a retrospective study. J Curr Glaucoma Pract. 2020;14(3):87–92. doi:10.5005/jp-journals-10078-1287
62. Smith M, Charles R, Abdel-Hay A, et al. 1-year outcomes of the Xen45 glaucoma implant. Eye. 2019;33(5):761–766. doi:10.1038/s41433-018-0310-1
63. Sng CCA, Chew PTK, Htoon HM, Lun K, Jeyabal P, Ang M. Case series of combined XEN implantation and phacoemulsification in Chinese eyes: one-year outcomes. Adv Ther. 2019;36(12):3519–3529. doi:10.1007/s12325-019-01127-w
64. Stoner AM, Capitena Young CE, SooHoo JR, et al. A comparison of clinical outcomes after XEN gel stent and EX-PRESS glaucoma drainage device implantation. J Glaucoma. 2021;30(6):481–488. doi:10.1097/ijg.0000000000001823
65. Subaşı S, Yüksel N, Özer F, Yılmaz Tugan B, Pirhan D. A retrospective analysis of safety and efficacy of XEN 45 microstent combined cataract surgery in open-angle glaucoma over 24 months. Turk J Ophthalmol. 2021;51(3):139–145. doi:10.4274/tjo.galenos.2020.47629
66. Tan SZ, Walkden A, Au L. One-year result of XEN45 implant for glaucoma: efficacy, safety, and postoperative management. Eye. 2018;32(2):324–332. doi:10.1038/eye.2017.162
67. Theilig T, Rehak M, Busch C, Bormann C, Schargus M, Unterlauft JD. Comparing the efficacy of trabeculectomy and XEN gel microstent implantation for the treatment of primary open-angle glaucoma: a retrospective monocentric comparative cohort study. Sci Rep. 2020;10(1):19337. doi:10.1038/s41598-020-76551-y
68. Theillac V, Blumen-Ohana E, Akesbi J, et al. Cataract and glaucoma combined surgery: XEN® gel stent versus nonpenetrating deep sclerectomy, a pilot study. BMC Ophthalmol. 2020;20(1):231. doi:10.1186/s12886-020-01492-z
69. Wałek E, Przeździecka-Dołyk J, Helemejko I, Misiuk-Hojło M. Efficacy of postoperative management with 5-fluorouracil injections after XEN Gel Stent implantation. Int Ophthalmol. 2020;40(1):235–246. doi:10.1007/s10792-019-01168-8
70. Widder RA, Lappas A, Rennings C, Hild M, Dietlein TS, Roessler GF. Primary versus posttrabeculectomy XEN45 gel stent implantation: comparison of success rates and intraocular pressure-lowering potential in pseudophakic eyes. J Glaucoma. 2020;29(12):1115–1119. doi:10.1097/ijg.0000000000001649
71. Wilkins M, Indar A, Wormald R. Intra-operative mitomycin C for glaucoma surgery. Cochrane Database Syst Rev. 2005;2005(4):Cd002897. doi:10.1002/14651858.CD002897.pub2
72. Widder RA, Dietlein TS, Dinslage S, Kühnrich P, Rennings C, Rössler G. The XEN45 Gel Stent as a minimally invasive procedure in glaucoma surgery: success rates, risk profile, and rates of re-surgery after 261 surgeries. Graefes Arch Clin Exp Ophthalmol. 2018;256(4):765–771. doi:10.1007/s00417-018-3899-7
73. Marcos Parra MT, Salinas López JA, López Grau NS, Ceausescu AM, Pérez Santonja JJ. XEN implant device versus trabeculectomy, either alone or in combination with phacoemulsification, in open-angle glaucoma patients. Graefes Arch Clin Exp Ophthalmol. 2019;257(8):1741–1750. doi:10.1007/s00417-019-04341-y
74. Sheybani A. Prospective, randomized, multicenter, open-label, 12-month evaluation of the effectiveness and safety of the gel stent vs trabeculectomy: the Gold Standard Pathway Study (GPS).
75. Wagner FM, Schuster AK, Emmerich J, Chronopoulos P, Hoffmann EM. Efficacy and safety of XEN®-implantation vs. trabeculectomy: data of a “real-world” setting. PLoS One. 2020;15(4):e0231614. doi:10.1371/journal.pone.0231614
76. Wanichwecharungruang B, Ratprasatporn N. 24-month outcomes of XEN45 gel implant versus trabeculectomy in primary glaucoma. PLoS One. 2021;16(8):e0256362. doi:10.1371/journal.pone.0256362
77. The AGIS Investigators. The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol. 2000;130(4):429–440. doi:10.1016/s0002-9394(00)00538-9
78. Caprioli J, Coleman AL. Intraocular pressure fluctuation a risk factor for visual field progression at low intraocular pressures in the advanced glaucoma intervention study. Ophthalmology. 2008;115(7):1123–1129.e3. doi:10.1016/j.ophtha.2007.10.031
79. Leske MC, Heijl A, Hyman L, Bengtsson B, Dong L, Yang Z. Predictors of long-term progression in the early manifest glaucoma trial. Ophthalmology. 2007;114(11):1965–1972. doi:10.1016/j.ophtha.2007.03.016
80. Bengtsson B, Leske MC, Hyman L, Heijl A. Fluctuation of intraocular pressure and glaucoma progression in the early manifest glaucoma trial. Ophthalmology. 2007;114(2):205–209. doi:10.1016/j.ophtha.2006.07.060
81. Kim JH, Rabiolo A, Morales E, et al. Risk factors for fast visual field progression in glaucoma. Am J Ophthalmol. 2019;207:268–278. doi:10.1016/j.ajo.2019.06.019
82. Konstas AG, Topouzis F, Leliopoulou O, et al. 24-hour intraocular pressure control with maximum medical therapy compared with surgery in patients with advanced open-angle glaucoma. Ophthalmology. 2006;113(5):761–5.e1. doi:10.1016/j.ophtha.2006.01.029
83. Burr J, Azuara-Blanco A, Avenell A, Tuulonen A. Medical versus surgical interventions for open angle glaucoma. Cochrane Database Syst Rev. 2012;(9):Cd004399. doi:10.1002/14651858.CD004399.pub3
84. Midha N, Gillmann K, Chaudhary A, Mermoud A, Mansouri K. Efficacy of needling revision after XEN gel stent implantation: a prospective study. J Glaucoma. 2020;29(1):11–14. doi:10.1097/ijg.0000000000001394
85. Hengerer FH, Auffarth G, Conrad-Hengerer I. Comparison of minimally invasive XEN45 gel stent implantation in glaucoma patients without and with prior interventional therapies. Ophthalmol Ther. 2019;8(3):447–459. doi:10.1007/s40123-019-0193-7
86. Hohberger B, Welge-Lüßen UC, Lämmer R. MIGS: therapeutic success of combined Xen Gel Stent implantation with cataract surgery. Graefes Arch Clin Exp Ophthalmol. 2018;256(3):621–625. doi:10.1007/s00417-017-3895-3
87. Berdahl JP. Cataract surgery to lower intraocular pressure. Middle East Afr J Ophthalmol. 2009;16(3):119–122. doi:10.4103/0974-9233.56222
88. Weinreb RN, Ramulu P, Topouzis F, et al. 11th Consensus Meeting: Glaucoma Surgery. Kugler Publications; 2019. WGA Consensus Series.
89. Dar N, Sharon T, Hecht I, Kalev-Landoy M, Burgansky-Eliash Z. Efficacy and safety of the ab interno gelatin stent in severe pseudoexfoliation glaucoma compared to non-pseudoexfoliation glaucoma at 6 months. Eur J Ophthalmol. 2020;30(5):1028–1033. doi:10.1177/1120672119848277
90. Hengerer FH, Auffarth GU, Yildirim TM, Conrad-Hengerer I. Ab interno gel implant in patients with primary open angle glaucoma and pseudoexfoliation glaucoma. BMC Ophthalmol. 2018;18(1):339. doi:10.1186/s12886-018-0989-6
91. Sng CC, Wang J, Hau S, Htoon HM, Barton K. XEN-45 collagen implant for the treatment of uveitic glaucoma. Clin Exp Ophthalmol. 2018;46(4):339–345. doi:10.1111/ceo.13087
92. Chan TCW, Bala C, Siu A, Wan F, White A. Risk factors for rapid glaucoma disease progression. Am J Ophthalmol. 2017;180:151–157. doi:10.1016/j.ajo.2017.06.003
93. Grieshaber MC, Peckar C, Pienaar A, Koerber N, Stegmann R. Long-term results of up to 12 years of over 700 cases of viscocanalostomy for open-angle glaucoma. Acta Ophthalmol. 2015;93(4):362–367. doi:10.1111/aos.12513
94. Lewis RA, von Wolff K, Tetz M, et al. Canaloplasty: three-year results of circumferential viscodilation and tensioning of Schlemm canal using a microcatheter to treat open-angle glaucoma. J Cataract Refract Surg. 2011;37(4):682–690. doi:10.1016/j.jcrs.2010.10.055
95. Pfeiffer N, Garcia-Feijoo J, Martinez-de-la-casa JM, et al. A randomized trial of a schlemm’s canal microstent with phacoemulsification for reducing intraocular pressure in open-angle glaucoma. Ophthalmology. 2015;122(7):1283–1293. doi:10.1016/j.ophtha.2015.03.031
96. Samuelson TW, Katz LJ, Wells JM, Duh YJ, Giamporcaro JE. Randomized evaluation of the trabecular micro-bypass stent with phacoemulsification in patients with glaucoma and cataract. Ophthalmology. 2011;118(3):459–467. doi:10.1016/j.ophtha.2010.07.007
97. Do A, McGlumphy E, Shukla A, et al. Comparison of clinical outcomes with open versus closed conjunctiva implantation of the XEN45 gel stent. Ophthalmol Glaucoma. 2021;4(4):343–349. doi:10.1016/j.ogla.2020.12.003
98. Dangda S, Radell JE, Mavrommatis MA, et al. Open conjunctival approach for sub-Tenon’s xen gel stent placement and bleb morphology by anterior segment optical coherence tomography. J Glaucoma. 2021;30(11):988–995. doi:10.1097/ijg.0000000000001929
99. Kong YXG, Chung IY, Ang GS. Outcomes of XEN45 gel stent using posterior small incision sub-tenon ab interno insertion (Semi-open) technique. Eye. 2021;36:1456–1460. doi:10.1038/s41433-021-01635-6
100. Gallardo MJ, Vincent LR, Porter M. Comparison of clinical outcomes following gel stent implantation via ab-externo and ab-interno approaches in patients with refractory glaucoma. Clin Ophthalmol. 2022;16:2187–2197. doi:10.2147/OPTH.S354038
101. Vera V, Gagne S, Myers JS, Ahmed IIK. Surgical approaches for implanting xen gel stent without conjunctival dissection. Clin Ophthalmol. 2020;14:2361–2371. doi:10.2147/opth.s265695
102. Vera V, Ahmed IIK, Stalmans I, Reitsamer H. Gel stent implantation—recommendations for preoperative assessment, surgical technique, and postoperative management. Touch Ophthalmol. 2018;11(1):38–46. doi:10.17925/USOR.2018.11.1.38
103. Kerr NM, Lim S, Simos M, Ward T. Primary needling of the ab interno gelatin microstent reduces postoperative needling and follow-up requirements. Ophthalmol Glaucoma. 2021;4(6):581–588. doi:10.1016/j.ogla.2021.02.004
104. Eraslan M, Özcan AA, Dericioğlu V, Çiloğlu E. Multicenter case series of standalone XEN implant vs. combination with phacoemulsification in Turkish patients. Int Ophthalmol. 2021;41(10):3371–3379. doi:10.1007/s10792-021-01899-7
105. Laspas P, Culmann PD, Grus FH, et al. Revision of encapsulated blebs after trabeculectomy: long-term comparison of standard bleb needling and modified needling procedure combined with transconjunctival scleral flap sutures. PLoS One. 2017;12(5):e0178099. doi:10.1371/journal.pone.0178099
106. Rotchford AP, King AJ. Needling revision of trabeculectomies bleb morphology and long-term survival. Ophthalmology. 2008;115(7):1148–1153.e4. doi:10.1016/j.ophtha.2007.10.023
107. Tsai AS, Boey PY, Htoon HM, Wong TT. Bleb needling outcomes for failed trabeculectomy blebs in Asian eyes: a 2-year follow up. Int J Ophthalmol. 2015;8(4):748–753. doi:10.3980/j.issn.2222-3959.2015.04.19
108. Gedde SJ, Vinod K, Wright MM, et al. Primary open-angle glaucoma preferred practice pattern®. Ophthalmology. 2021;128(1):80. doi:10.1016/j.ophtha.2020.10.022
109. Suzuki R, Susanna R. Early transconjunctival needling revision with 5-fluorouracil versus medical treatment in encapsulated blebs: a 12-month prospective study. Clinics. 2013;68(10):1376–1379. doi:10.6061/clinics/2013(10)14
110. Steiner S, Resch H, Kiss B, Buda D, Vass C. Needling and open filtering bleb revision after XEN-45 implantation-A retrospective outcome comparison. Graefes Arch Clin Exp Ophthalmol. 2021;259(9):2761–2770. doi:10.1007/s00417-021-05204-1
111. Linton E, Au L. Technique of xen implant revision surgery and the surgical outcomes: a retrospective interventional case series. Ophthalmol Ther. 2020;9(1):149–157. doi:10.1007/s40123-020-00234-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Update on Surgical Techniques Best Practices to Optimize Outcomes Following Gel Stent Implantation

Vera V, Sheybani A, Panarelli JF, Grover DS, Lee J, Craven ER, Samuelson TW, Ahmed IIK
Clinical Ophthalmology 2025, 19:325-347
Published Date: 31 January 2025
A Comparison of the Efficacy and Safety of Modified Baerveldt Drainage Implants versus Ahmed Glaucoma Valves After 1 Year of Follow-Up
Davis KL, Christensen QH, VandeLune JA, Pellack DR, Donegan PJ, Meyer MD, Singh RS, Al-Kaylani HM, Boese EA, Pouw AE
Clinical Ophthalmology 2026, 20:588163
Published Date: 8 July 2026