Back to Journals » Clinical Ophthalmology » Volume 19
Intraocular Lens Position Stability During Phacovitrectomy with Air or Gas Tamponade
Authors Yoshikawa Y ![]() , Matsushima T, Takano S
, Matsushima T, Takano S ![]() , Makita J, Shinoda K
, Makita J, Shinoda K
Received 29 May 2025
Accepted for publication 5 August 2025
Published 15 August 2025 Volume 2025:19 Pages 2773—2783
DOI https://doi.org/10.2147/OPTH.S539958
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yuji Yoshikawa,1,2 Takashi Matsushima,2 Shunichiro Takano,1 Jun Makita,1 Kei Shinoda1
1Department of Ophthalmology, Saitama Medical University, Iruma, Saitama, Japan; 2Department of Ophthalmology, Tokai University School of Medicine, Kanagawa, Japan
Correspondence: Yuji Yoshikawa, Department of Ophthalmology, Saitama Medical University, 38, Morohongo, Iruma, Saitama, 350-0495, Japan, Tel/Fax +81-492-76-1250, Email [email protected]
Purpose: To evaluate the stability of different intraocular lenses (IOLs) after phacovitrectomy with air or gas tamponade.
Patients and Methods: This retrospective cross-sectional study included 28 patients who underwent phacovitrectomy with air or sulfur hexafluoride gas tamponade and postoperative anterior segment optical coherence tomography assessments. Patients who received any DIB00V (Johnson & Johnson Surgical Vision, Inc. Irvine, CA, USA), XY-1 (HOYA Surgical Optics Co. Chromos, Singapore), or NX70s (Santen Pharmaceutical Co. LTD, Osaka, Japan) IOL implantation were analyzed. The anterior chamber depth (ACD) and IOL position values at each measurement (100%, 50%, 0%) and between IOLs were compared. The IOL displacement force (mN) was measured with a verification experiment and recorded at each 0.1 mm anterior movement until anterior displacement reached 0.5 mm.
Results: The average patient age was 66 (59– 73) years. ACD values increased progressively as the postoperative gas decreased for all IOLs. Compared to the preoperative ACD, postoperative ACD was significantly greater at 50% and 0% gas for all IOLs. The DIB00V had significantly larger ACD values than the XY-1 at 100% gas or air (P = 0.023) and the NX70s at 0% gas or air (P = 0.008). The IOL position gradually shifted significantly posteriorly for all IOLs as the gas or air disappeared. No significant change was observed in the DIB00V and NX70s between the gas 50% and gas 0% conditions (DIB00VP = 0.019 with Bonferroni correction, NX70s; P = 0.148 with Bonferroni correction). The DIB00V were significantly more posterior than the XY-1at 100% (P = 0.046).
Conclusion: The DIB00V had greater IOL displacement force against push from the retinal surface compared to the XY-1 and NX70s and exhibited excellent z-axis stability in phacovitrectomy with air or gas tamponade.
Keywords: anterior chamber depth, displacement, postoperative, implantation, retinal surface
Introduction
Postoperative refractive error has long been of great interest to cataract surgeons aiming for superior postoperative visual function after cataract surgery. Although advancements in various formulas have improved the accuracy of postoperative refraction in cataract surgery alone, challenges persist, particularly in cases involving phacovitrectomy.1–5
One study suggests that simultaneous vitreous surgery does not change refractive error compared to cataract surgery alone,6 whereas others suggest that it causes myopia.7–9 Thus, managing postoperative refractive error in phacovitrectomy is more complex than in cataract surgery alone.
In particular, when gas tamponade is performed during vitrectomy, the postoperative anterior chamber depth (ACD) is shallower compared to cases without tamponade.8 Additionally, ACD increases with gas loss when gas tamponade is performed.10 A recent study has demonstrated that a myopic shift can occur when combined surgery is performed with gas tamponade, such as in eyes with retinal detachment.9 Furthermore, the myopic shift after vitrectomy for retinal detachment is more pronounced when the IOL is implanted primarily rather than secondarily.11 These findings are considered due to IOL anterior displacement caused by pressure from the intraocular gas.
Various intraocular lens (IOL) types, including one-piece, three-piece, 6 mm, and 7 mm lenses, exhibit different lens stability.12,13 IOL stability in the z-axis direction for gas tamponade may be one of the factors that influences postoperative refraction.
This study evaluated the stability of different IOLs after phacovitrectomy with air or gas tamponade.
Materials and Methods
Study Design
This retrospective cross-sectional study was approved by the Ethics Committee of Saitama Medical University, Iruma, Japan. (Application No. 2023-095) The study adhered to the tenets of the Declaration of Helsinki and opt-out informed consent was obtained from each participant.
Study Participants and Examinations
Twenty-eight patients who underwent phacovitrectomy with air or sulfur hexafluoride (SF6) gas tamponade at Saitama Medical University Hospital between January and July 2023 and underwent postoperative anterior segment optical coherence tomography assessments using CASIA2 (TOMEY, Inc., Nagoya, Japan), were included in the study.
Cataract surgery was performed through a 2.4 mm corneal incision, along with simultaneous 25- or 27-gauge pars plana vitrectomy by a retinal specialist. A continuous curvilinear capsulotomy was created to completely cover the IOL optics. The trocar was inserted into the vitreous cavity at an angle of 30° to the scleral surface, positioned 3.5 mm posterior to the corneal limbus. All patients underwent peripheral vitreous shaving and fluid-air exchange. The intraocular vitreous cavity was replaced with 20% SF6 from air, depending on intraoperative findings. Surgery was completed with the IOL and vitreous cavity filled with either air or 20% SF6.
The patients who received implantation with the DIB00V (a one-piece, 6 mm acrylic IOL manufactured by Johnson & Johnson Surgical Vision, Inc. Irvine, CA, USA), the XY-1 (a one-piece, 6 mm acrylic IOL manufactured by HOYA Surgical Optics Co., Chromos, Singapore), or the NX70s (a three-piece, 7 mm acrylic IOL with polyvinylidene fluoride haptics manufactured by Santen Pharmaceutical Co., LTD, Osaka, Japan) were included in the analyses.
CASIA 2 (TOMEY, Inc.) was used to measure ACD preoperatively, and at 100%, 50%, and 0% residual air or SF6 gas. To minimize the influence of preoperative ACD measurements when comparing postoperative ACDs among different IOLs, the IOL position was calculated as the ratio of the change in ACD before and after surgery to the preoperative lens thickness, defined as: (postoperative ACD − preoperative ACD) / preoperative lens thickness, as previously reported12 (Figure 1).
 |
Figure 1 Measurement of intraocular lens (IOL) position. The left images depict preoperative and postoperative CASIA 2 scans; the preoperative image is above and the postoperative image is below. The right image shows a superimposition of the preoperative and postoperative CASIA 2 images. The IOL position was measured as the ratio of the difference between the preoperative and postoperative anterior chamber depths (ACD) to the lens thickness, expressed as (postoperative ACD – preoperative ACD) versus the lens thickness. The corneal side was assigned a value of 0, and the retinal side was assigned a value of 1. |
A fundus examination was performed on the day after surgery and eyes in which the vitreous cavity was completely filled with air or gas were defined as “gas 100%”. Based on the fundus examination and wide-field fundus photography, eyes in which air or gas extended over the macular area were defined as “gas 50%”, and eyes in which gas had completely disappeared were defined as “gas 0%”.
The difference between the subjective refraction value at 0% gas and the preoperatively predicted refraction value, measured using OA2000 (TOMEY, Inc.) and CASIA 2 (TOMEY, Inc.), was defined as the refractive error. The ACD and IOL position values at each measurement time point were compared using the Wilcoxon signed-rank test with Bonferroni correction for each IOL. Comparisons of ACD and IOL position between IOLs at each time point were evaluated using the Steel–Dwass test.
All values are presented as medians with interquartile ranges. Statistical analyses were performed using JMP version 10.1 (SAS Institute, Cary, NC, USA).
A P value of < 0.05 was considered significant. However, for comparisons of ACD and IOL position at each time point, Bonferroni correction was applied, and the significance levels were set as: ACD P < 0.0083, IOL position P < 0.0167.
Verification Experiment
The IOL displacement force was measured as previously reported.12,13
All selected IOLs were +21 diopters. The IOLs were placed in a 10 mm diameter holder at room temperature (31 °C). To simulate the drag force produced when the IOL is pushed from the retinal surface side, the posterior side of the IOL was pushed by a digital micrometer head (3.0 mm diameter; Mitutoyo, Kawasaki, Japan) until they moved 0.5 mm anteriorly. The IOL displacement force (mN) was measured when the values were stabilized using an electronic balance (SHIMADZU, Kyoto, Japan) and recorded at each 0.1 mm anterior movement until the anterior displacement reached 0.5 mm (Figure 2A).
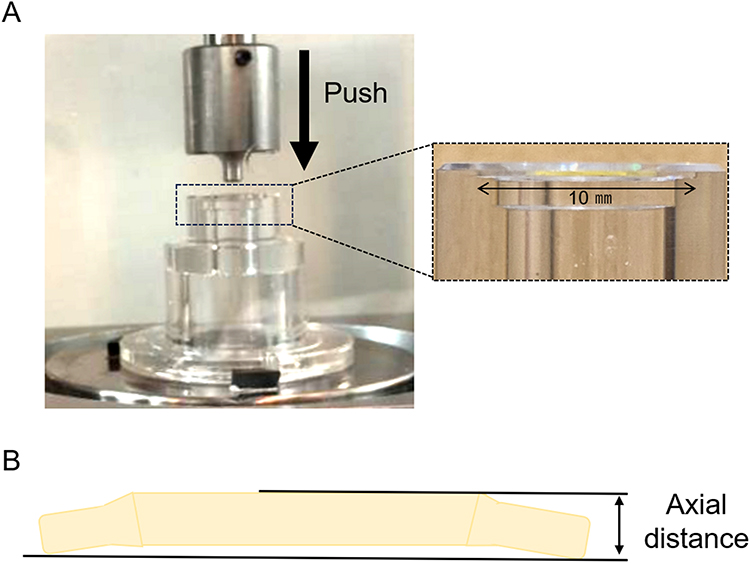 |
Figure 2 Measurement of intraocular lens (IOL) displacement force and reversibility. This figure illustrates the methods used to assess the displacement force and reversibility of IOLs, each with +21 diopters, placed in a 10 mm diameter holder at 31 °C. (A) Displacement force is evaluated by applying a digital micrometer head (diameter 3.0 mm; Mitutoyo, Kawasaki, Japan) to the posterior side of the IOL, gradually pushing it 0.5 mm anteriorly. The force required to stabilize the IOL at each 0.1 mm anterior movement is measured in mN using an electronic balance (SHIMADZU, Kyoto, Japan). (B) Reversibility is evaluated by recording the distance in the z-axis between the optics and haptics immediately after the IOL is pushed in 0.5 mm (0 h) and again 48 h later. The measured axial distance reflects the distance from the retinal surface side of the optics to the corneal surface side of the haptics. |
To further evaluate IOL reversibility, the axial-distance in the z-axis direction between the optics and haptics was measured immediately after the IOL was pushed 0.5 mm (0 h) and 48 h later. All distances were measured with the IOL removed from the fixture and the push-in was released (Figure 2B).
Results
The overall patient age was 66 (59, 73) (median [quartiles]) years. The median ages for the IOL groups were DIB00V (Johnson & Johnson Surgical Vision, Inc.) (n = 11) 67 (58, 76) years, NX70s (Santen Pharmaceutical Co., LTD) (n = 8) 66 (58, 77) years, and XY-1 (HOYA Surgical Optics Co.) (n = 9) 64 (59, 73) years; without significant differences between the IOLs. No significant differences in sex, axial length, lens thickness, ratio of air and SF6, or time to CASIA2 (TOMEY, Inc., Japan) examinations were observed (Table 1).
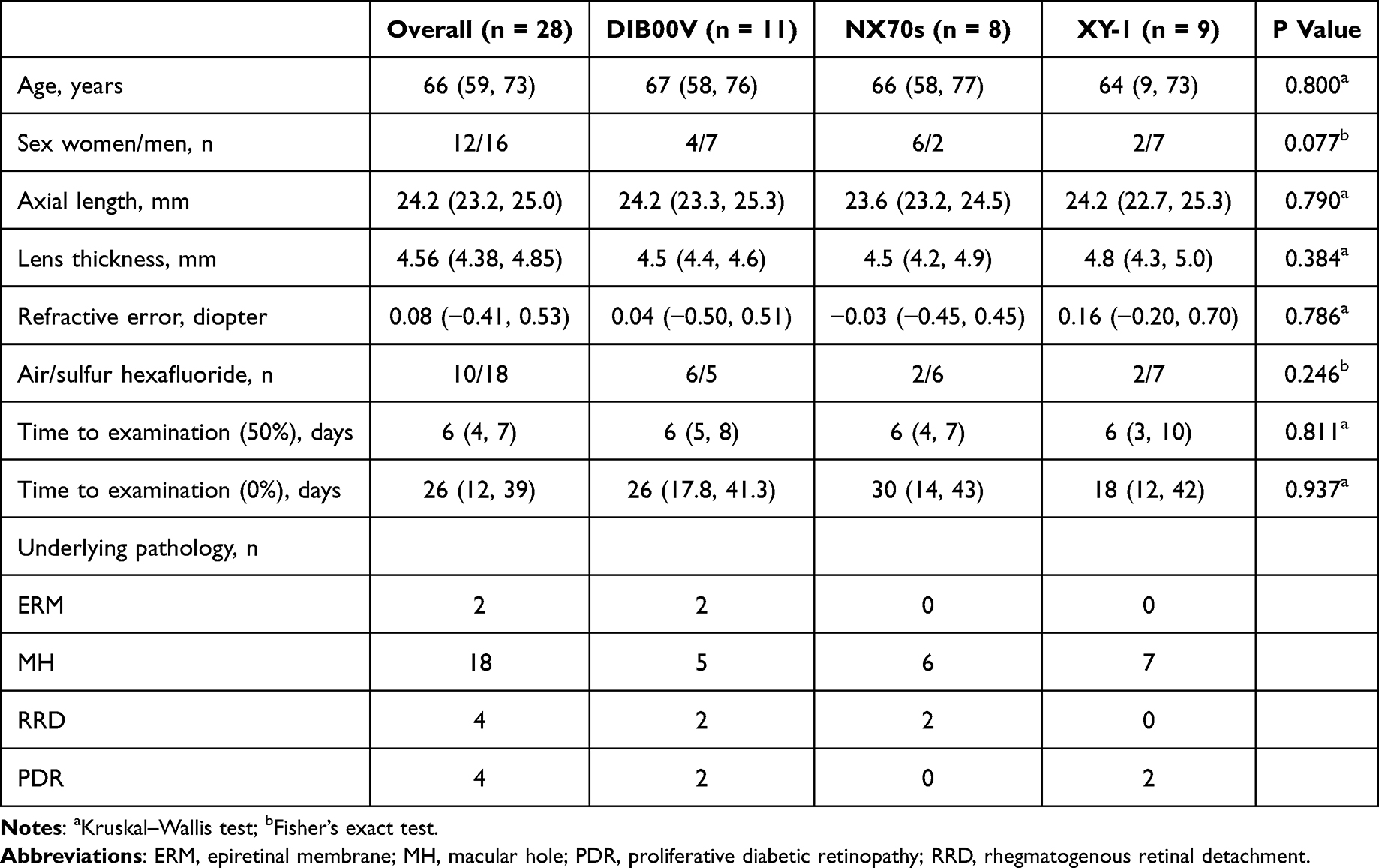 |
Table 1 Demographic and Clinical Characteristics of Each Intraocular Lens Group |
The refractive error values were 0.04 (−0.50, 0.51) diopters for DIB00V, −0.03 (−0.45, 0.45) diopters for NX70s, and 0.16 (−0.20, 0.70) diopters for XY-1, without significant differences observed between the three IOL groups.
As listed in Table 2, the ACD values increased progressively as the postoperative gas decreased for all IOLs. Compared to the preoperative ACD measurements, the postoperative ACD measurements were significantly greater at 50% and 0% gas for all IOLs. However, the XY-1 demonstrated no significant difference in ACD values between preoperative and 100% air or gas (P = 0.098 with Bonferroni correction); the DIB00V and NX70s showed no significant difference between 50% and 0% air or gas (DIB00V P= 0.019 with Bonferroni correction, NX70s; P = 0.117 with Bonferroni correction). Additionally, DIB00V had significantly larger ACD values compared to the XY-1 at 100% gas or air (P = 0.023) and NX70s at 0% gas or air (P = 0.008) (Table 2 and Figure 3).
 |
Table 2 Comparison of Anterior Chamber Depth Values for Each Intraocular Lens |
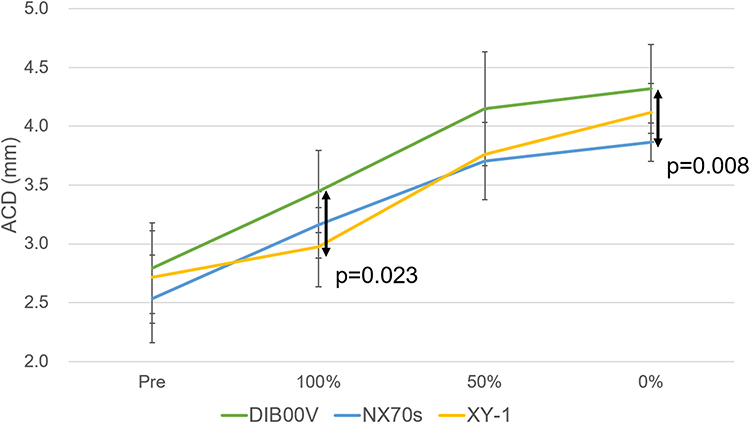 |
Figure 3 Temporal changes in anterior chamber depth (ACD) for different intraocular lenses (IOLs). This figure shows the changes in the ACD at different time points for each IOL. The DIB00V demonstrate significantly greater ACD compared to the XY-1 at 100% gas or air (P = 0.023) and compared to the NX70s at 0% gas or air (P = 0.008). |
As presented in Table 3, the IOL position gradually shifted significantly posteriorly for all IOLs as the gas or air disappeared. However, no significant change was observed in the DIB00V and NX70s between the 50% and 0% air or gas conditions (DIB00V P = 0.019 with Bonferroni correction, NX70s P = 0.148 with Bonferroni correction). IOL-by-IOL comparisons at each time point determined that the DIB00V were significantly more posterior than the XY-1 at 100% gas or air (P = 0.046) (Table 3 and Figure 4).
 |
Table 3 Comparison of Intraocular Lens Position Values for Each Intraocular Lens |
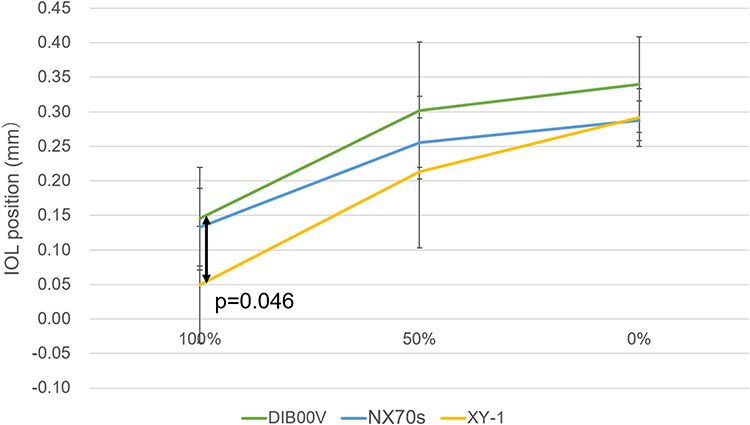 |
Figure 4 Temporal changes in intraocular lens (IOL) position. The figure illustrates the changes in IOL position for each IOL across time points. The DIB00V exhibit a significantly more posterior position compared to the XY-1 at 100% gas or air (P = 0.046), indicating greater posterior stability under full tamponade conditions. |
In the verification experiment, the DIB00V required a greater IOL displacement force against a push from the retinal surface compared to the XY-1 and NX70s (displacement force at 0.5 mm: DIB00V, 2.45 mN; XY-1, 1.04 mN; NS70s, 0.64 mN) (Figure 5).
 |
Figure 5 Intraocular lens (IOL) displacement force response to push. This figure demonstrates the relationship between IOL displacement force and IOL travel distance. For all IOLs, the displacement force increases with increasing IOL travel distance. The DIB00V show a greater displacement force in response to a push from the retinal surface side compared to the XY-1 and NX70s. The drag forces at 0.5 mm displacement are recorded as follows: DIB00V at 2.45 mN, XY-1 at 1.04 mN, and NX70s at 0.64 mN. |
The mean axial distances immediately after the 0.5 mm push (0 h) were 0.775 mm for the DIB00V, 0.441 mm for XY-1, and 1.213 mm for NX70s. After 48 h of 0.5 mm push, the mean axial distances were 0.770 mm for the DIB00V, 0.386 mm for XY-1, and 1.038 mm for the NX70s. The percentage change in axial distance was smallest for the DIB00V (0.65%), compared to 12.5% for the XY-1 and 14.4% for the NX70s (Figure 6).
 |
Figure 6 Reversibility of intraocular lens (IOL) shape after 48 h of compression. This graph shows the axial distance change in each IOL immediately after applying 0.5 mm of pressure (0 h) and after 48 h of compression. The percentage change in axial distance after 48 h is minimal for DIB00V (0.65%), compared to XY-1 (12.5%) and NX70s (14.4%), indicating that the DIB00V have greater resistance to deformation over time. |
A representative case is shown in Figure 7. With the one-piece IOLs (DIB00V, XY-1), the ACD deepenedand the IOL position shifted toward the retinal plane as the tamponade material decreased. In contrast, the three-piece IOL(NX70s) showed minimal changes in ACD and IOL position between 50% and 0% air or gas conditions. At all time points, the DIB00V were positioned closer to the retinal plane than the XY-1 and NX70s.
 |
Figure 7 Comparison of anterior chamber depth (ACD) and intraocular lens (IOL) positions in representative cases. This figure compares the changes in ACD and IOL position among different IOL types as the tamponade material diminishes. In the one-piece IOLs (DIB00V, XY-1), the ACD deepens, and the IOL position moves posteriorly toward the retinal plane as the tamponade material decreases. In contrast, the three-piece IOL(NX70s) show minimal change in both ACD and IOL position between 50% and 0% tamponade. Throughout all time points, the DIB00V consistently demonstrate a more posterior IOL position compared to the XY-1 and NX70s. |
Discussion
This study examined the z-axis stability of the one-piece DIB00V and XY-1and the three-piece NX70 IOLs under air or SF6 gas tamponade. In phacovitrectomy, three-piece IOLs and large-diameter IOLs are generally preferred because of their intracapsular stability and better fundus visibility through the IOL.14,15 However, in recent years, insertion of premium IOLs has been attempted in cases of epiretinal membrane.16,17 Given the importance of refractive correction in phacovitrectomy, there is a growing need for one-piece IOLs.
Previous studies have shown that when IOL optics are pushed in the z-axis from the posterior side, the stability of the NS60YG (NIDEK Co., LTD, Japan), YP2.2R (KOWA Co., LTD, Japan), and ZCB00V (Johnson & Johnson Surgical Vision, Inc.) is higher than that of the SN60WF (Alcon Laboratories Inc, USA), XY-1, and 255 (HOYA Surgical Optics Co.).13 Additionally, the NS60YG has demonstrated superior stability compared to X70 (Santen Pharmaceutical Co., LTD), which is a large aperture three-piece lens.12 In our clinical study, the DIB00V exhibited greater ACD and IOL position values at 100% gas or air than the XY-1. From the results of the validation experiments, the DIB00V was more resistant to IOL displacement forces than XY-1 and NX70s.
The DIB00V has the same lens design as the ZCB00V (TECNIS series, Johnson & Johnson), which has been reported to be more stable than the XY-1 against pressure loading from behind the IOL (in the z-axis direction) in an experimental system,13 as in this study. This indicates that the TECNIS series lens design has excellent z-axial stability.
For the one-piece lenses, the IOL position progressively shifted backward, and the IOL position value increased as the pressure load decreased due to the decrease in gas or air; however, the NX70s group showed no significant change from 50% to 0% air or gas. The ACD at 0% in the NX70s group was significantly smaller than that of the DIB00V group. The IOL position value was previously reported as approximately 0.35–0.36 for cataract surgery alone.8 In our study, the IOL position for the DIB00V at 0% was 0.35, indicating that, even with phacovitrectomy with tamponade, the DIB00V returned to the same IOL position with cataract surgery alone once the tamponade material disappeared. Conversely, for the NX70s, the IOL positions were more anterior than those reported for cataract surgery alone, without change in ACD or IOL positions from 50% to 0% air or gas. The validation experiments showed that 48 h of loading caused IOL deformation, particularly in the NX70s, which had the greatest deformation.
In the NX70s group, backward loading with air or gas in the z-axis direction may have caused IOL deformation, which resulted in the IOL position remaining fixed anteriorly after the tamponade material disappeared. Although there were no significant differences in refractive error among the three groups, the median values showed a shift toward hyperopia in the DIB00V and myopia for NX70s, suggesting an effect of the IOL position. However, this study could not identify the factors that influence reversibility of the lens position. IOL stability depends on the haptic junction area,13 number of haptics, and shape.18 The shape and material of the haptics may also influence IOL reversibility.
After cataract surgery, the IOL tends to shift anteriorly over time, resulting in a myopic shift.19 Some reports have suggested that the use of a capsular tension ring can suppress postoperative myopization by preventing ACD from becoming shallower through inhibition of capsular contraction.20 Therefore, in addition to tamponade, capsular contraction may be an important factor that influences postoperative IOL position and refractive change. Previous studies have reported that capsular contraction tends to occur after 3 weeks postoperatively.21 Since the average follow-up period after gas absorption in our study was 26 (12, 39) days, capsular contraction may have already occurred. Moreover, one-piece lenses are more prone to capsular contraction than three-piece lenses.21 In our study, both the DIB00V and XY-1 were one-piece lenses and may have been more susceptible to anterior displacement due to capsular contraction. However, our results showed that the DIB00V and XY-1 had greater ACD and IOL position values even after gas absorption compared to the NX70s, indicating that the one-piece IOLs were positioned more posteriorly. Therefore, even if capsular contraction occurred, its influence on the outcomes of this study is considered minimal.
Although a significant difference was observed in postoperative ACD and IOL position between the three IOLs, no significant difference was found in postoperative refractive error. This may be attributed to the absence of individualized A-constant optimization for each IOL, as well as variability among surgeons, both of which could have affected postoperative refractive outcomes. To assess refractive error more precisely after surgery, prospective studies that incorporate personalized A-constants and minimize surgeon variability are warranted.
This study has several limitations, including a small sample size, multiple surgeons, and the use of two tamponade materials. However, continuous curvilinear capsulorhexis provided complete coverage of the IOL optics in all surgeries, and the ratio of air to SF6 gas did not significantly differ among the three groups. The degree of peripheral vitreous shaving likely varies depending on the underlying disease. Careful vitreous dissection may have been performed, particularly in cases where NX70s were selected. When the most peripheral vitreous is shaved, the IOL should be shifted posteriorly due to the vulnerability of the ligament of Zinn.22 This study showed that the NX70s were more anteriorly positioned than other IOLs. Therefore, even if the NX70s group included more eyes with careful vitreous shaving, the ACD depth may have been underestimated; however, this would have had minimal impact on the study results. The clinical data in this study were obtained approximately 30 days postoperatively. The experimental data also evaluated lens shape recovery after 48 h and immediately after the release of compression. Therefore, long-term changes in IOL shape after the loss of air or gas could not be assessed. Additionally, postoperative positioning and resting periods may differ depending on the causative disease, and the degree of backward pressure on the IOL may differ depending on the postoperative positioning. However, these effects were not considered in the present study. Further validation is needed through conducting studies with larger sample sizes that focus on specific underlying diseases and gas types used.
Conclusion
In combined surgeries with gas tamponade, the DIB00V may offer greater stability against tamponade compared to the XY-1 and NX70s. Although its impact on postoperative refraction was minimal, the findings of this study are based on a small cohort and caution should be exercised in generalizing the results.
Abbreviations
ACD, anterior chamber depth; IOL, intraocular lens; SF6, sulfur hexafluoride.
Data Sharing Statement
The datasets used and/or analyzed during the current study available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This retrospective cross-sectional study was approved by the Ethics Committee of Saitama Medical University, Iruma, Japan. (Application No. 2023-095) The study adhered to the tenets of the Declaration of Helsinki and opt-out informed consent was obtained from each participant.
Acknowledgments
The authors thank Editage (https://www.editage.jp) for English language review. We also thank Shinji Nagasaka and colleagues at NIDEK Co., Ltd. for conducting the verification experiment. This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-5276306/v1.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not supported by any funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Retzlaff JA, Sanders DR, Kraff MC. Development of the SRK/T intraocular lens implant power calculation formula. J Cataract Refract Surg. 1990;16(3):333–340. doi:10.1016/s0886-3350(13)80705-5
2. Holladay JT, Prager TC, Chandler TY, Musgrove KH, Lewis JW, Ruiz RS. A three-part system for refining intraocular lens power calculations. J Cataract Refract Surg. 1988;14(1):17–24. doi:10.1016/s0886-3350(88)80059-2
3. Olsen T. Prediction of the effective postoperative (intraocular lens) anterior chamber depth. J Cataract Refract Surg. 2006;32(3):419–424. doi:10.1016/j.jcrs.2005.12.139
4. Barrett GD. An improved universal theoretical formula for intraocular lens power prediction. J Cataract Refract Surg. 1993;19(6):713–720. doi:10.1016/s0886-3350(13)80339-2
5. Ghoreyshi M, Khalilian A, Peyman M, Mohammadinia M, Peyman A. Comparison of OKULIX ray-tracing software with SRK-T and Hoffer-Q formula in intraocular lens power calculation. J Curr Ophthalmol. 2017;30(1):63–67. doi:10.1016/j.joco.2017.06.008
6. Sato T, Korehisa H, Shibata S, Hayashi K. Prospective comparison of intraocular lens dynamics and refractive error between phacovitrectomy and phacoemulsification alone. Ophthalmol Retina. 2020;4(7):700–707. doi:10.1016/j.oret.2020.01.022
7. Liu BS, Cui WN, Niu R, et al. Refractive outcomes after vitrectomy combined with phacoemulsification of idiopathic macular holes. Int J Ophthalmol. 2021;14(2):250–254. doi:10.18240/ijo.2021.02.11
8. Shiraki N, Wakabayashi T, Sakaguchi H, Nishida K. Effect of gas tamponade on the intraocular lens position and refractive error after phacovitrectomy: a swept-source anterior segment OCT analysis. Ophthalmology. 2020;127(4):511–515. doi:10.1016/j.ophtha.2019.10.021
9. Tanaka Y, Kamiya K, Igarahi A, et al. Evaluation of the accuracy of intraocular lens power calculation formulas in phacovitrectomy. Ophthalmol Ther. 2024;13(8):2197–2208. doi:10.1007/s40123-024-00971-6
10. Takahashi Y, Hirano T, Nakamura M, et al. Temporal change in anterior chamber depth after combined vitrectomy and cataract surgery using different sizes of intraocular lens. J Clin Med. 2022;11(21):6430. doi:10.3390/jcm11216430
11. Li Q, Yang Z, Liu R. Intraocular lens tilt and decentration after primary and delayed implantation in phacovitrectomy for macula-off rhegmatogenous retinal detachment repair. Indian J Ophthalmol. 2024;72(Suppl 5):S788–S794. doi:10.4103/IJO.IJO_3192_23
12. Akiyama A, Yokota H, Aso H, et al. Comparison of postoperative stability of intraocular lenses after phacovitrectomy for rhegmatogenous retinal detachment. J Clin Med. 2022;11(12):3438. doi:10.3390/jcm11123438
13. Mochiji M, Kaidzu S, Ishiba Y, Matsuda Y, Tanito M. Measurement of force required for anterior displacement of intraocular lenses and its defining parameters. Materials. 2020;13(20):4593. doi:10.3390/ma13204593
14. Borkenstein AF, Borkenstein EM. Efficacy of large optic intraocular lenses in myopic eyes with posterior segment pathology. Ophthalmol Ther. 2022;11(1):443–452. doi:10.1007/s40123-021-00433-3
15. Schrecker J, Seitz B, Langenbucher A. Performance einer neuen 7-mm-Intraokularlinse mit Nachbeobachtung über 1,5 Jahre [Performance of a unique 7 mm intraocular lens with follow-up over 1.5 years]. Ophthalmologe. 2022;119(4):367–373. German. doi:10.1007/s00347-021-01504-3
16. Jeon S, Choi A, Kwon H. Clinical outcomes after implantation of extended depth-of-focus AcrySof® Vivity® intraocular lens in eyes with low-grade epiretinal membrane. Graefes Arch Clin Exp Ophthalmol. 2022;260(12):3883–3888. doi:10.1007/s00417-022-05751-1
17. Kim H, Jeon S. Visual outcomes of epiretinal membrane removal after diffractive-type multifocal intraocular lens implantation. BMC Ophthalmol. 2022;22(1):423. doi:10.1186/s12886-022-02649-8
18. Hwang HS, Jee D. Effects of the intraocular lens type on refractive error following phacovitrectomy with gas tamponade. Curr Eye Res. 2011;36(12):1148–1152. doi:10.3109/02713683.2011.632107
19. Stifter E, Menapace R, Luksch A, Neumayer T, Sacu S. Anterior chamber depth and change in axial intraocular lens position after cataract surgery with primary posterior capsulorhexis and posterior optic buttonholing. J Cataract Refract Surg. 2008;34(5):749–754. doi:10.1016/j.jcrs.2007.12.035
20. Lin H, Zhang Y, Xie X, et al. Capsular tension ring implantation for intraocular lens position: a systematic review and meta-analysis. JAMA Ophthalmol. 2025. doi:10.1001/jamaophthalmol.2025.1623
21. Lin X, Ma D, Yang J. Exploring anterion capsular contraction syndrome in cataract surgery: insights into pathogenesis, clinical course, influencing factors, and intervention approaches. Front Med. 2024;11:1366576. doi:10.3389/fmed.2024.1366576
22. Ahfat FG, Yuen CH, Groenewald CP. Phacoemulsification and intraocular lens implantation following pars plana vitrectomy: a prospective study. Eye. 2003;17(1):16–20. doi:10.1038/sj.eye.6700232
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.