Back to Journals » Journal of Asthma and Allergy » Volume 19
Intranasal Corticosteroids Versus Second-Generation Antihistamines for Allergic Rhinitis in Adolescents: A Prospective Cohort Study of Quality of Life and School Attendance
Authors Irmak S ![]() , Dedeoglu S
, Dedeoglu S ![]() , Toprak SF, Sırma E, Samancı S, Kozan G
, Toprak SF, Sırma E, Samancı S, Kozan G ![]()
Received 3 March 2026
Accepted for publication 22 May 2026
Published 11 June 2026 Volume 2026:19 606463
DOI https://doi.org/10.2147/JAA.S606463
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Luis Garcia-Marcos
Siraç Irmak,1 Serkan Dedeoglu,1 Serdar Ferit Toprak,2 Enes Sırma,1 Serhat Samancı,3 Günay Kozan4
1Department of Otorhinolaryngology, University of Health Sciences Gazi Yaşargil Training and Research Hospital, Diyarbakır, Turkey; 2Department of Audiology, Artuklu University, Mardin, Turkey; 3Department of Pediatrics, Diyarbakır Children Hospital, Diyarbakır, Turkey; 4Department of Otorhinolaryngology and Head and Neck Surgery, Faculty of Medicine, Dicle University, Diyarbakır, Turkey
Correspondence: Serkan Dedeoglu, Department of Otorhinolaryngology, University of Health Sciences Gazi Yaşargil Training and Research Hospital, Diyarbakır, Turkey, Tel +90 5325999729, Email [email protected]
Purpose: Allergic rhinitis (AR) in adolescents can negatively affect daily functioning, sleep, and school performance. This observational, non-randomized prospective cohort study compared the real-world effectiveness of intranasal corticosteroids (INCS) and second-generation oral antihistamines (OAH) on disease-specific quality of life and school attendance.
Patients and Methods: This observational, non-randomized prospective cohort study included 80 adolescents aged 12– 18 years with moderate-to-severe allergic rhinitis who were followed for one school term. Participants received either INCS monotherapy or OAH monotherapy according to routine clinical practice; treatment allocation was not randomized. Specific drug selection within each treatment class was determined by the treating clinician and was not fully standardized, reflecting real-world treatment heterogeneity. Primary outcomes were changes in Pediatric Rhinoconjunctivitis Quality of Life Questionnaire (PRQLQ) scores and school absenteeism. Secondary outcomes included classroom productivity, sleep quality (Pittsburgh Sleep Quality Index), daytime sleepiness (Epworth Sleepiness Scale), adherence, and adverse events. Between-group comparisons and multivariable analyses were performed.
Results: Both treatments were associated with improvement, but the magnitude of improvement was greater in the INCS group. Mean PRQLQ scores decreased by – 1.0± 0.4 in the INCS group and – 0.6± 0.5 in the OAH group; the between-group difference in mean change was – 0.4 (95% confidence interval [CI], – 0.7 to – 0.1; p = 0.01). Clinically meaningful QoL improvement (≥ 0.5 reduction) occurred in 65.0% of INCS users versus 37.5% of OAH users (p = 0.02). Median school absenteeism decreased in the INCS group (change, – 2 days) but not in the OAH group (change, 0 days; between-group p = 0.03). INCS users also reported greater improvements in classroom productivity and sleep quality, and fewer participants had ESS scores ≥ 10 at follow-up (3% vs 18%).
Conclusion: In this real-world adolescent cohort, INCS use was associated with greater short-term improvement in quality-of-life and school-attendance outcomes than OAH use. However, because the study was observational and non-randomized, and because treatment heterogeneity existed within both treatment groups, these findings should be interpreted as associations rather than definitive causal effects. The infographic compares intranasal corticosteroids (INCS) and second-generation antihistamines (OAH) for treating allergic rhinitis in adolescents. It is based on a prospective cohort study involving 80 adolescents. The comparison covers three areas: Quality of Life (PRQLQ), School Absenteeism and Sleep & Alertness. INCS shows greater improvement in quality of life, fewer missed school days and better sleep with less daytime sleepiness. In contrast, OAH results in moderate improvement in quality of life, more missed school days and more daytime sleepiness. The conclusion states that intranasal corticosteroids are superior for quality of life and school attendance.Image of a prospective cohort study comparing intranasal corticosteroids with second-generation oral antihistamines in eighty adolescents with allergic rhinitis. Intranasal corticosteroids are associated with greater improvement in quality of life, fewer missed school days, better sleep, and less daytime sleepiness than oral antihistamines, which show moderate improvement and more daytime sleepiness.
Keywords: allergic rhinitis, adolescent, intranasal corticosteroid, antihistamine, quality of life, school attendance
Introduction
Allergic rhinitis (AR) is a common chronic inflammatory disease of the nasal mucosa and represents a substantial health burden during childhood and adolescence. Beyond nasal symptoms, AR may impair sleep quality, daily functioning, school attendance, classroom productivity, and overall quality of life. AR is a prevalent chronic illness among adolescents, with prevalence estimates of approximately 20% to 40% in this age group. Urbanisation, environmental change, and lifestyle factors are likely contributing to this rising burden. In adolescents, AR is not a trivial condition; it commonly presents with chronic nasal congestion, rhinorrhoea, sneezing, and ocular pruritus, all of which can disturb sleep, reduce daytime alertness, and impair psychological well-being. Many adolescents report that symptoms interfere with academic performance, sports, and social activities, and they often perceive their overall health to be poorer than that of their non-allergic peers. Although intranasal corticosteroids and second-generation oral antihistamines are widely used in adolescents with AR, comparative prospective real-world evidence evaluating their effects on both disease-specific quality of life and educational outcomes remains limited.
The educational consequences of AR have attracted increasing attention. Previous literature has shown that allergic rhinitis and allergic rhinoconjunctivitis are associated with increased school absenteeism, reduced classroom productivity, and poorer self-reported academic performance. In a United Kingdom case-control study, adolescents sitting national examinations during symptomatic seasonal AR achieved significantly lower grades than matched peers without active symptoms, suggesting a potential effect on high-stakes academic outcomes. Other studies have linked AR to poorer cognitive performance, including reduced attention, slower psychomotor speed, and impaired memory, particularly during periods of uncontrolled symptoms. Sleep disruption may be an important mediator, as nocturnal nasal obstruction and related arousals can lead to non-restorative sleep, daytime sleepiness, and difficulty concentrating in class.
Current pharmacological options for allergic rhinitis include intranasal corticosteroids, oral antihistamines, intranasal antihistamines, leukotriene receptor antagonists, and allergen immunotherapy, with treatment selection guided by symptom severity, dominant symptom profile, patient preference, adherence considerations, and comorbid disease. Intranasal antihistamines, such as azelastine or olopatadine, provide topical H1-receptor antagonism and may offer rapid relief of sneezing, itching, rhinorrhoea, and nasal congestion. They therefore represent an important alternative to oral antihistamines in selected patients, particularly when local nasal symptom control is desired.
For patients with moderate-to-severe allergic rhinitis or inadequate control with monotherapy, fixed intranasal corticosteroid–intranasal antihistamine combination therapy, such as fluticasone plus azelastine, is also an important option within the current therapeutic landscape. Such combination therapy targets both nasal mucosal inflammation and histamine-mediated symptoms and may provide greater symptom control than either component alone in selected patients. Although these therapies are clinically relevant, the present study compared only intranasal corticosteroid monotherapy with second-generation oral antihistamine monotherapy; intranasal antihistamines and fixed intranasal combination therapy were not included as comparator arms.
International guidelines emphasise that AR affects not only nasal symptoms but also sleep, daily functioning, and co-morbid asthma. AR is driven by IgE-mediated inflammation after allergen exposure, with mast-cell activation, mediator release, and subsequent recruitment of inflammatory cells to the nasal mucosa; this pathophysiology provides the rationale for anti-inflammatory treatment. ARIA and related practice recommendations identify intranasal corticosteroids and second-generation oral antihistamines as first-line pharmacotherapies in adolescents, while discouraging routine use of sedating first-generation antihistamines. Intranasal corticosteroids are generally considered the most effective treatment for moderate-to-severe AR, particularly for nasal obstruction. Oral antihistamines are effective for sneezing, itching, and rhinorrhoea and are convenient once-daily treatments; however, even second-generation agents may cause mild drowsiness or cognitive slowing in susceptible individuals. In addition, intranasal antihistamines and combination intranasal corticosteroid–antihistamine therapy are increasingly recognised options within the therapeutic landscape, particularly for patients requiring rapid symptom relief or escalation beyond monotherapy.
Disease-specific quality-of-life instruments such as the Pediatric Rhinoconjunctivitis Quality of Life Questionnaire provide a sensitive way to capture the multidimensional burden of AR on daily activities, emotions, sleep, and school life. The PRQLQ has been validated in children and adolescents and has an established minimal clinically important difference of approximately 0.5 points on its 0–6 scale. Despite the availability of such tools, relatively few studies have evaluated how common AR therapies affect both quality of life and educational outcomes in adolescents in real-world settings. Many clinical trials enrol mixed age groups, focus primarily on symptom scores, and are conducted under tightly controlled conditions, which may not reflect variability in adolescent adherence or the realities of school calendars and examination periods. Comparative prospective real-world evidence focused specifically on adolescents remains limited.
The present prospective cohort study was designed to address this evidence gap by comparing the real-world effectiveness of intranasal corticosteroids and second-generation oral antihistamines on disease-specific quality of life and school attendance among adolescents with moderate-to-severe allergic rhinitis during one academic term. Our primary hypothesis was that INCS therapy, through broader anti-inflammatory control of nasal mucosal inflammation, would be associated with greater improvement in PRQLQ scores and larger reductions in school absenteeism than OAH monotherapy. Secondary outcomes included classroom productivity, sleep quality, daytime sleepiness, adherence, and adverse events.
Materials and Methods
Study Design and Setting
We conducted a single-centre, prospective cohort study over a 4-month period corresponding to one academic term. Participants were recruited from the otorhinolaryngology and allergy clinics of a tertiary training and research hospital in Diyarbakır, Turkey, and from neighbouring schools that collaborated in the project. The study was designed to reflect routine clinical practice rather than a tightly controlled trial, while maintaining structured follow-up and standardised outcome measurement.
The research protocol was approved by the Ethics Committee of Artuklu University Medical Faculty Hospital (approval number: 2025/9-37; dated September 9, 2025) and complied with the Declaration of Helsinki. Written informed consent was obtained from parents or legal guardians, and assent was obtained from adolescents before enrolment. Permission to access school attendance records was granted by school administrations and local educational authorities.
Participants
Adolescents aged 12 to 18 years with a diagnosis of AR were considered for inclusion. Diagnosis was established by an otorhinolaryngologist or allergist according to ARIA criteria, based on a compatible clinical history of nasal and/or ocular symptoms related to allergen exposure and objective evidence of sensitisation (positive skin prick test or serum specific IgE to relevant aeroallergens).1,2 We included students with at least moderate severity of AR, defined as symptoms on most days during the relevant season or throughout the year that interfered with daily activities or sleep and required regular pharmacotherapy.
Key inclusion criteria were: (i) enrolment in middle or high school (grades 6–12) with electronic attendance tracking; (ii) ability to complete questionnaires in Turkish; and (iii) no change in long-term AR medication during the preceding 4 weeks. Exclusion criteria were: (i) severe or uncontrolled asthma (Global Initiative for Asthma step 4 or above) requiring frequent systemic corticosteroids; (ii) chronic rhinosinusitis with or without nasal polyps; (iii) prior or current allergen immunotherapy within the last 12 months; (iv) use of systemic corticosteroids within the previous month; (v) use of first-generation (sedating) antihistamines more than occasionally; (vi) any chronic disease likely to influence school attendance (for example epilepsy, severe eczema or inflammatory bowel disease); and (vii) inability or unwillingness to participate in follow-up visits.
Treatment Groups and Clinical Management
This was an observational, non-randomized real-world cohort study. Treatment allocation and drug selection reflected routine clinical practice rather than a fully standardized protocol. Participants in the INCS group received a commercially available intranasal corticosteroid preparation, such as fluticasone or mometasone, at standard product-label doses. Participants in the OAH group received a second-generation oral antihistamine, such as loratadine, desloratadine, or fexofenadine, also according to usual once-daily product-label dosing. The specific agent within each treatment class was selected by the treating physician according to symptom profile, prior treatment response, tolerance, availability, expected adherence, and patient/family preference.Because different agents were pooled within each treatment class, the study should be interpreted as a pragmatic class-level comparison rather than a head-to-head comparison of individual drugs. No product-specific efficacy inference was intended.Participants prescribed intranasal corticosteroids formed the INCS group. They received a commercially available aqueous nasal spray, such as fluticasone furoate or mometasone furoate, at a standard once-daily dose according to product labelling. The usual regimen was two sprays per nostril once daily in the morning, equivalent to a medium dose. The specific INCS preparation remained at the clinician’s discretion, reflecting real-world practice.
Participants prescribed second-generation oral antihistamines formed the OAH group. They received a once-daily oral antihistamine, usually loratadine 10 mg, desloratadine 5 mg, or fexofenadine 120 mg. The specific agent was selected according to prior tolerance, previous response, local availability, clinician judgement, and patient/family preference. Because the OAH group included agents with potentially different sedative profiles, class-level effects on daytime sleepiness were interpreted cautiously.
Treatment as monotherapy was encouraged. Regular combination therapy, such as daily INCS plus daily antihistamine, was avoided to preserve the contrast between groups. Short courses of additional symptomatic treatment, including saline nasal irrigation or occasional rescue antihistamine use during severe symptom flares, were permitted when clinically necessary and documented. No participant was scheduled to switch treatment during follow-up; any temporary deviations were recorded in the clinical file and considered when interpreting adherence and adverse events. The study was designed and analysed as a treatment-class comparison, not as a head-to-head comparison of individual drugs.2.4. Outcomes and Measurement Instruments.
Primary Outcomes
There were two primary outcomes.
Change in disease-specific QoL from baseline to 4 months, measured by the Pediatric Rhinoconjunctivitis Quality of Life Questionnaire. The PRQLQ is a 28-item instrument covering nose symptoms, eye symptoms, practical problems, activity limitation and emotional impacts.3 Items are rated on a 7-point scale (0 “not troubled” to 6 “extremely troubled”), and the overall score is the mean of all items, so higher scores indicate worse QoL. The questionnaire has been validated in children and adolescents and has an established minimal clinically important difference (MCID) of approximately 0.5 points.3,4 We used the Turkish adaptation following a standard translation and back-translation process where necessary.5,6
Change in school absenteeism, defined as the number of whole school days missed for any reason during the 4-month study term compared with the immediately preceding term. Official attendance records were obtained from school electronic systems. For descriptive purposes, absences recorded as due to illness (by parental note or school nurse report) were distinguished from other reasons when such documentation was available, although all missed days contributed to the primary absenteeism outcome.
Secondary Outcomes
Secondary outcomes reflected domains that are likely to mediate the impact of AR on school functioning. Classroom productivity was assessed using a pragmatic self-reported presenteeism question designed for this study. This measure was intended to capture perceived classroom functioning during the academic term; however, it was not a formally validated academic-performance or presenteeism instrument.
Presenteeism (in-class productivity): Students completed a brief 0–10 numerical rating scale asking “How much did your nose or eye symptoms interfere with your performance at school in the past two weeks?” (0 “not at all”, 10 “completely prevented me from performing”). This simple, face-valid measure was adapted from work productivity instruments and piloted in a small group of students for clarity; however, it was not a formally validated school-function instrument, and results should therefore be interpreted cautiously.
Sleep quality: The short form of the Pittsburgh Sleep Quality Index (PSQI) was used to assess subjective sleep quality over the previous month. Global scores range from 0 to 21, with higher scores indicating poorer sleep; a score above 5 is often taken to signify clinically relevant sleep disturbance.7,8
Daytime sleepiness: The Epworth Sleepiness Scale (ESS) was administered. Scores range from 0 to 24, and a threshold of 10 or higher is widely used to indicate significant excessive daytime sleepiness. Using this cut-off, we calculated the proportion of students with meaningful daytime somnolence before and after treatment.
Medication adherence: Adherence was assessed using a self-report medication diary and, when feasible, pill counts or assessment of remaining nasal spray doses at follow-up visits. For analysis, adherence was expressed as the percentage of prescribed doses taken over the 4-month period. Participants who took at least 80% of prescribed doses were classified as having “good adherence”, a threshold commonly used in chronic disease research.
Adverse events: At each visit, clinicians asked about side effects. Particular attention was paid to local nasal irritation or epistaxis in the INCS group, and to sedation, fatigue or reduced alertness in the OAH group.
Data Collection and Follow-Up Schedule
Baseline assessment (T0) occurred at the start of the school term. Demographic data (age, sex), clinical profile (duration of AR symptoms, seasonal versus perennial pattern, known allergen sensitisation) and co-morbidities, including asthma, were recorded. Baseline PRQLQ, presenteeism, PSQI and ESS questionnaires were administered at this visit. We then obtained absenteeism data for the previous term from school records, blind to subsequent treatment group.
Participants were followed at approximately 8 weeks (T1) and 16 weeks (T2). At T1, interim clinical status, adherence and any adverse events were reviewed. Short questionnaires (presenteeism, ESS) were repeated to provide interim safety information and to encourage adherence, but only T0 and T2 measurements were used in the primary analyses. At T2, all baseline questionnaires were repeated and absenteeism for the current term was extracted from school records.
To minimise recall bias, students were encouraged to bring their medication diaries to each visit. Where attendance records were unclear, school staff were contacted for clarification. Outcome assessors extracting school data were unaware of participants’ treatment groups.
Sample Size
Sample size calculations were based on detecting a between-group difference of at least 0.5 in mean PRQLQ change, corresponding to the MCID.3,4 Assuming a standard deviation of 0.8 for change scores, a two-sided alpha of 0.05 and 80% power, a minimum of 34 participants per group was required. Anticipating up to 15% loss to follow-up, we aimed to recruit 40 participants for each group, giving a total target sample size of 80 adolescents.
Statistical Analysis
Analyses were conducted using IBM SPSS Statistics version 27 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD) if approximately normally distributed or median with interquartile range (IQR) for skewed data. Normality was assessed using the Shapiro–Wilk test and inspection of histograms.
Between-group comparisons of baseline continuous variables used the independent-samples t-test or Mann–Whitney U-test, as appropriate. Within-group pre–post comparisons used paired t-tests or Wilcoxon signed-rank tests. Categorical variables were compared with chi-square or Fisher’s exact tests.
For the primary QoL outcome, the mean change in PRQLQ from T0 to T2 was compared between groups. The proportion of participants achieving a clinically meaningful improvement (≥0.5 reduction) was also compared using chi-square. For absenteeism, the change in number of missed days between the previous term and the study term was calculated for each participant; group differences in change were tested using Mann–Whitney U.
To explore independent predictors of QoL improvement, multivariable linear regression was performed with PRQLQ change score as the dependent variable. Candidate predictors included treatment group (INCS vs OAH), baseline PRQLQ score, presence of mild asthma, type of AR (seasonal vs perennial), good adherence (≥80% vs <80%) and a seasonal index (study term dominated by pollen season vs outside main season). Model assumptions were checked using residual plots and collinearity diagnostics.
All tests were two-sided and a p-value below 0.05 was considered statistically significant. Given the exploratory nature of secondary analyses, no formal adjustment for multiple comparisons was applied, but interpretation emphasised patterns rather than isolated marginal p-values. No formal adjustment for multiple comparisons was performed. Therefore, analyses of secondary outcomes were considered exploratory. The study was primarily powered for the PRQLQ outcome, and findings for secondary outcomes, including sleep quality, daytime sleepiness, classroom productivity, and adverse events, should be interpreted with caution.
Results
Participant Flow and Baseline Characteristics
Ninety-two adolescents were assessed for eligibility. Twelve were excluded: eight did not meet inclusion criteria (for example very mild intermittent symptoms, chronic sinusitis) and four declined participation. Eighty students consented and were enrolled. Treating clinicians prescribed intranasal corticosteroids for 40 participants and second-generation oral antihistamines for the remaining 40. All INCS participants and 38 of 40 OAH participants attended the final follow-up; two OAH students missed the T2 visit but had partial data available. Figure 1 summarises the flow of participants.
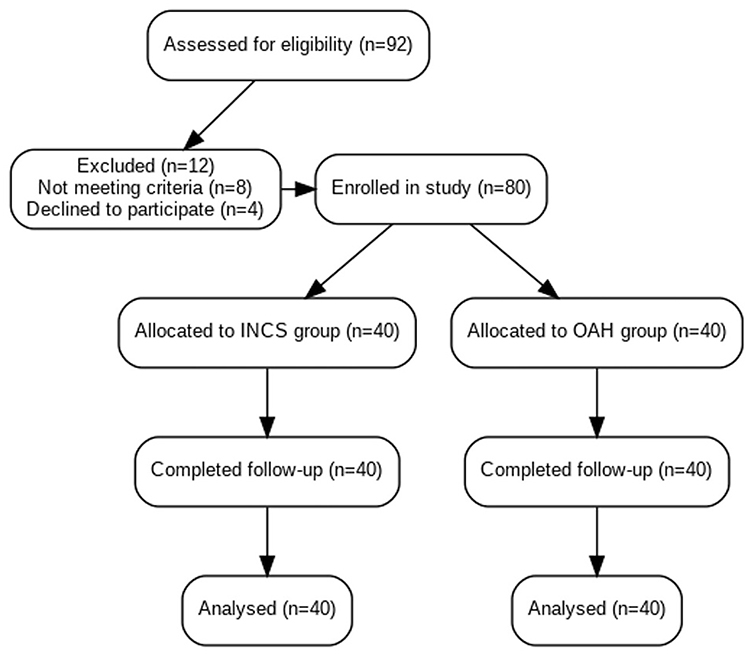 |
Figure 1 Flow diagram of study participation. Of 92 adolescents screened, 80 were enrolled. Forty received intranasal corticosteroid monotherapy and 40 received second-generation oral antihistamine monotherapy. All INCS participants completed the 4-month follow-up. Two OAH participants were lost to follow-up but had partial data; their available outcomes were included in intention-to-treat analyses. |
Baseline characteristics are shown in Table 1. The two treatment groups were broadly comparable in age, sex distribution, AR type, asthma comorbidity, baseline PRQLQ score, sleep quality, daytime sleepiness, and school absenteeism. However, because treatment allocation was observational and non-randomized, baseline comparability should not be interpreted solely on the basis of non-significant p-values. Small clinically relevant imbalances may have persisted and could have influenced treatment selection and outcomes. The mean age was 14.7 ± 1.6 years in the INCS group and 14.5 ± 1.8 years in the OAH group. Girls comprised 50% of each group. Seasonal AR was present in 60% of INCS and 57.5% of OAH participants. Sensitisation to at least one pollen allergen was common in both cohorts (75% and 70%, respectively). Mild asthma co-morbidity occurred in 15% of INCS and 17.5% of OAH participants. Baseline PRQLQ scores indicated moderate impairment in both groups (3.8 ± 0.7 vs 3.9 ± 0.8, p = 0.54). Median absenteeism during the previous term was 3 days in both groups. Baseline presenteeism, PSQI and ESS scores were comparable, and about one fifth of participants in each group had ESS values of 10 or more, suggesting meaningful daytime sleepiness at enrolment. Although no baseline difference reached statistical significance, the observational design means that small clinical imbalances cannot be excluded.
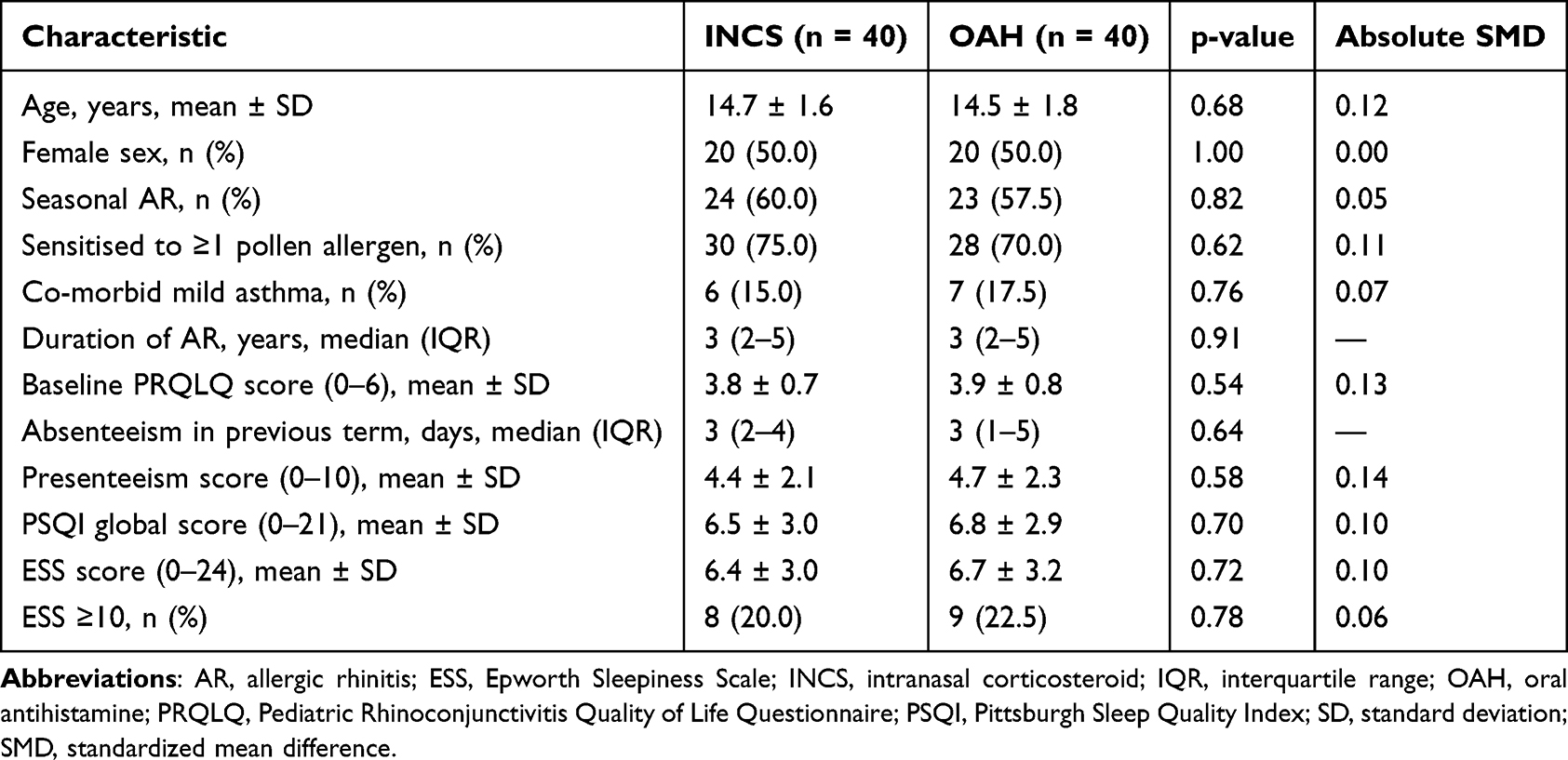 |
Table 1 Baseline Characteristics of Adolescents with Allergic Rhinitis According to Treatment Group |
Changes in Key Outcomes
Mean PRQLQ scores improved in both groups over 4 months. The mean change was greater in the INCS group than in the OAH group (–1.0±0.4 vs –0.6±0.5). The between-group difference in mean change was –0.4 points (95% CI, –0.7 to –0.1; p=0.01). Clinically meaningful improvement, defined as a reduction of at least 0.5 points in PRQLQ score, occurred in 65.0% of INCS users and 37.5% of OAH users (absolute difference, 27.5%; 95% CI, 6.2% to 48.8%; p=0.02).
Figure 2 illustrates the pattern of PRQLQ change in each group. The proportion of participants achieving a clinically important improvement (≥0.5 reduction) was 65% (26 of 40) in the INCS group, compared with 37.5% (15 of 40) in the OAH group (χ2 = 6.0, p = 0.02). Furthermore, 8 INCS users (20%) had near complete resolution of QoL impairment (PRQLQ < 1 at T2), whereas only 3 OAH users (7.5%) reached this threshold (p = 0.10). No INCS participant experienced a deterioration in PRQLQ, while three OAH participants had a slight increase in score, generally coinciding with marked seasonal pollen peaks.
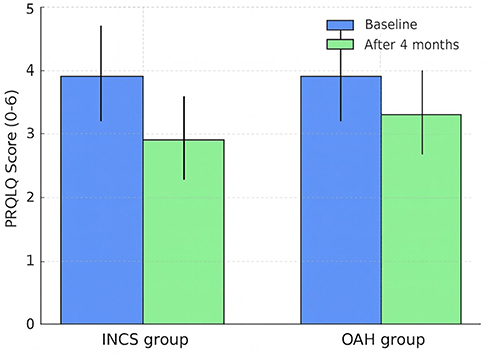 |
Figure 2 Change in PRQLQ scores over 4 months of treatment. Bar graph displays mean PRQLQ scores at baseline and 4 months for each group (INCS: 3.8 to 2.8; OAH: 3.9 to 3.3). Error bars show standard deviations, and the figure is intended as a simple visual summary of the primary outcome rather than a substitute for the full numerical data in Table 3. |
Subdomain analyses suggested that INCS treatment yielded larger improvements in nasal symptom and practical problem domains, whereas differences between groups for ocular and emotional domains were smaller. These patterns are consistent with the strong effect of intranasal steroids on nasal congestion and obstruction.9–11
School Absenteeism
Median school absenteeism decreased in the INCS group from 4 days at baseline to 2 days at follow-up, corresponding to a median change of –2 days. In the OAH group, median absenteeism changed from 4 days to 4 days, corresponding to a median change of 0 days. The between-group difference in absenteeism change was statistically significant (p=0.03). Because absenteeism was recorded as all-cause school absence rather than AR-specific absence, this finding should be interpreted as a functional educational outcome rather than as a direct disease-attributable absence measure.
More than half of INCS-treated students (22 of 40; 55%) had no absences recorded during the study term, compared with 12 of 40 (30%) in the OAH group (p = 0.02). Among those who remained absent, most episodes were documented as illness-related; colds, asthma exacerbations and severe allergy days were common reasons, but explicit attribution to AR was infrequent in school notes.
Presenteeism, Sleep and Daytime Sleepiness
Presenteeism scores improved in both groups but to a greater extent with INCS. At baseline, mean scores suggested moderate interference with school performance (4.4 ± 2.1 in INCS; 4.7 ± 2.3 in OAH). At 4 months, INCS participants reported mean scores of 2.4 ± 1.8 (mean change −2.0 ± 1.6; p < 0.001), whereas OAH participants reported 4.3 ± 2.1 (mean change −0.4 ± 1.5; p = 0.18). The between-group difference in change was significant (p < 0.01). Around 60% of INCS users reported an improvement of at least 2 points, compared with 25% of OAH users.
Sleep quality also improved over the study term. The INCS group showed a mean PSQI reduction from 6.5 ± 3.0 to 4.5 ± 2.6 (mean change −2.0 ± 2.1; p < 0.001). The OAH group improved from 6.8 ± 2.9 to 5.8 ± 2.8 (change −1.0 ± 2.0; p = 0.02). The difference in mean change between groups reached statistical significance (p = 0.04). The proportion of students with PSQI global scores above 5 declined from 60% to 35% in the INCS group, and from 65% to 50% in the OAH group.
Although follow-up ESS findings suggested less daytime sleepiness in the INCS group than in the OAH group, this result should be interpreted cautiously. The OAH group included different second-generation antihistamines with potentially different sedative profiles; therefore, the observed difference may partly reflect heterogeneous antihistamine exposure rather than a uniform class effect. Follow-up ESS scores suggested less daytime sleepiness in the INCS group than in the OAH group. However, because the OAH group included agents with potentially different sedative profiles, this finding should be interpreted cautiously and should not be attributed to a single antihistamine agent. Mean ESS scores decreased slightly in both groups (INCS: 6.4 ± 3.0 to 5.7 ± 2.6; OAH: 6.7 ± 3.2 to 6.4 ± 3.1), and between-group differences in mean change were not significant. However, the prevalence of ESS ≥ 10 at follow-up was 1 of 40 (3%) in the INCS group versus 7 of 40 (18%) in the OAH group (p = 0.03). Most OAH participants reporting daytime sleepiness also described feeling “sluggish” or “less focused” during classes. Given heterogeneity within the antihistamine group, these findings should be interpreted as observational class-level signals rather than definitive drug-specific effects.
Adherence and Adverse Events
Adherence was generally good in both groups. Mean adherence, calculated as the percentage of prescribed doses taken, was 85% ± 11% in the INCS group and 81% ± 14% in the OAH group (p = 0.21). Using the ≥80% threshold, 35 INCS participants (88%) and 33 OAH participants (82%) were considered good adherers (p = 0.47). Adolescents most commonly cited forgetfulness as the reason for missed doses; dislike of nasal spray sensation was an occasional complaint in the INCS group.
Adverse events were mild and infrequent. Four INCS users (10%) reported minor nasal irritation or transient epistaxis, which resolved with brief dose adjustment or technique correction. No participant discontinued INCS due to adverse events. In the OAH group, eight students (20%) reported subjective drowsiness or decreased alertness; seven of these had ESS scores ≥ 10 at follow-up. No serious systemic reactions occurred in either group.
Multivariable Analysis
Variables initially entered into the multivariable model included treatment group, baseline PRQLQ score, asthma comorbidity, AR type, adherence status, and seasonal timing. In the final model, INCS treatment and good adherence remained independently associated with greater PRQLQ improvement. INCS treatment was associated with a larger reduction in PRQLQ score compared with OAH treatment (B = −0.38; 95% CI, −0.62 to −0.14; standardized β = −0.46; p = 0.002). Good adherence was also associated with greater improvement (B = −0.24; 95% CI, −0.46 to −0.02; standardized β = −0.29; p = 0.030) Table 2). Because this was an observational, non-randomized cohort study, these adjusted findings should be interpreted as associations rather than causal effects.
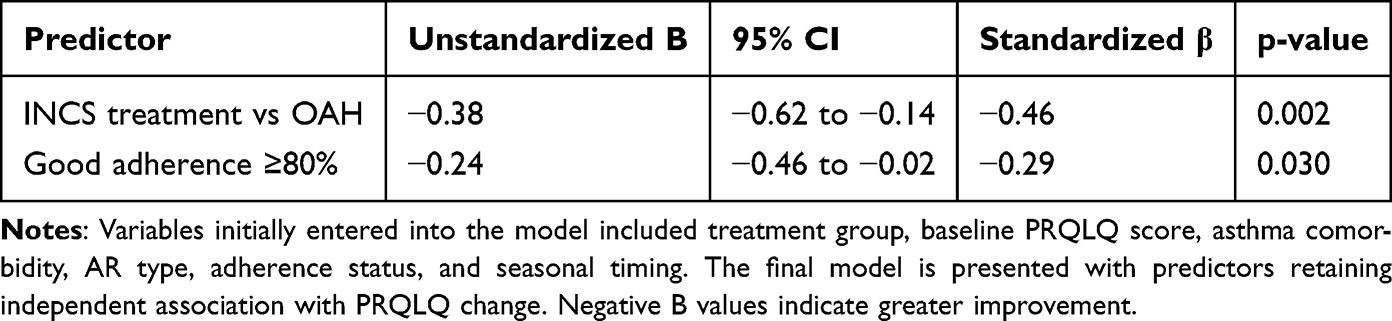 |
Table 2 Multivariable Linear Regression Analysis for Change in PRQLQ Score at 4 Months |
An exploratory negative binomial regression for change in absenteeism suggested a trend toward fewer missed days with INCS and with good adherence, although confidence intervals were wide and did not consistently exclude unity, reflecting the relatively small number of events and limited power.
The changes in the primary clinical and functional outcomes across the four-month follow up are summarised in Table 3. Adolescents treated with intranasal corticosteroids had a larger mean drop in PRQLQ scores and a greater decline in absence days than those taking oral antihistamines, and a higher proportion reached the minimal clinically meaningful improvement in quality of life. Improvements in classroom productivity and sleep quality also favoured the INCS group, although excessive daytime sleepiness at follow up was more frequent in the antihistamine group. Adherence rates were high and comparable between groups, therefore the variations seen in Table 3 are unlikely to be explained solely by differential compliance.
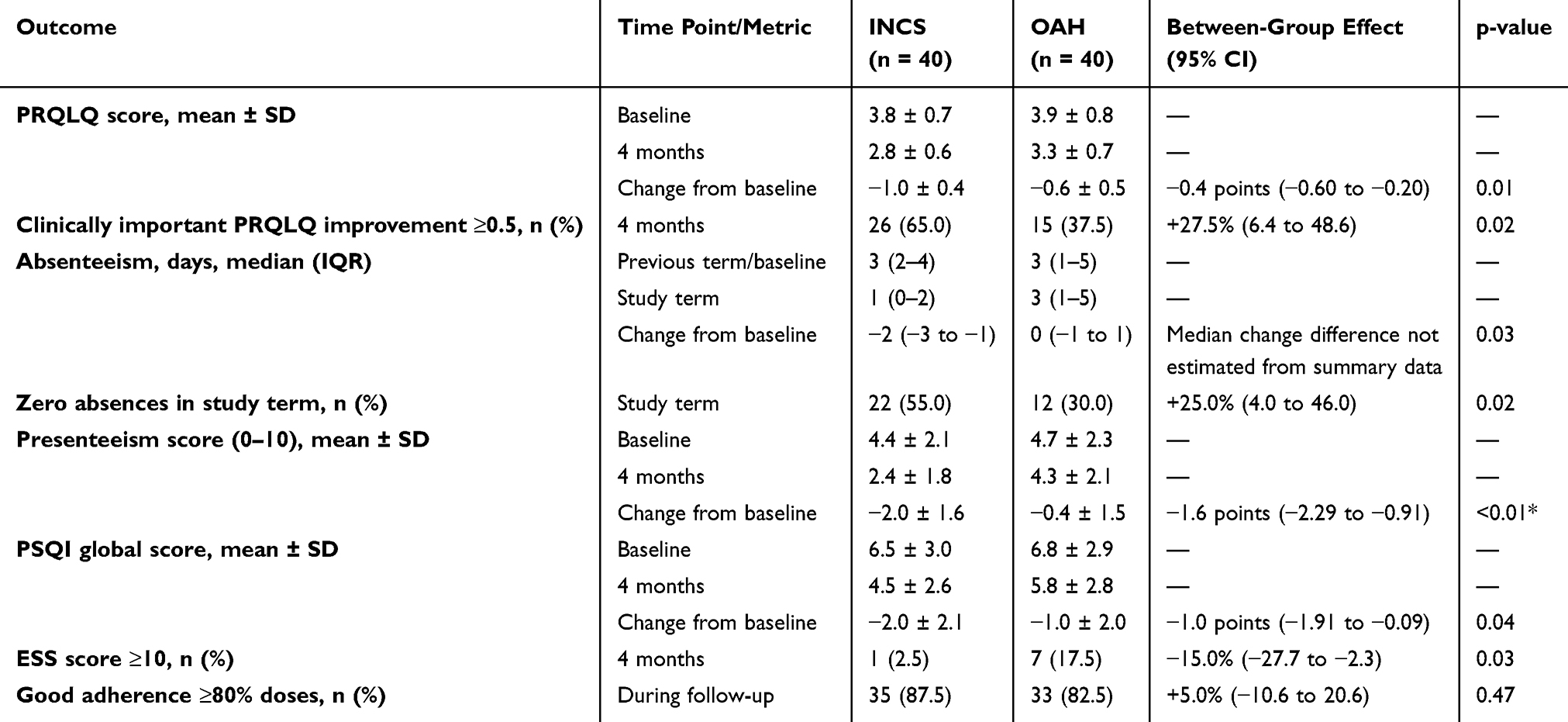 |
Table 3 Changes in Key Outcomes from Baseline to 4 Months According to Treatment Group |
Discussion
This prospective non-randomized cohort study examined the comparative real-world effectiveness of intranasal corticosteroids and second-generation oral antihistamines in adolescents with allergic rhinitis. Over the course of a single school term, both treatments were associated with improved symptoms and QoL, yet the magnitude of improvement was greater among adolescents treated with INCS. Better functional outcomes were also observed in the INCS group for absenteeism, classroom productivity, and sleep-related measures. Because this was a non-randomized observational cohort study, the findings should be interpreted as associations rather than definitive causal effects. Although INCS use was associated with greater improvement in PRQLQ scores and school-attendance outcomes, treatment allocation was determined by routine clinical decision making rather than random assignment. Therefore, residual confounding and confounding by indication cannot be excluded. Confounding by indication is particularly relevant in this study. Clinicians may have selected INCS or OAH according to dominant symptom profile, severity of nasal obstruction, sleep disturbance, prior treatment response, expected adherence, perceived need for anti-inflammatory control, and patient/family preference. These clinical factors may themselves be associated with treatment response and functional outcomes. Although multivariable analysis was used to adjust for selected baseline characteristics, unmeasured confounding may have remained.
Interpretation in Light of Existing Literature
The observed advantage of intranasal corticosteroids over oral antihistamines in controlling nasal symptoms and improving rhinitis-specific QoL is consistent with prior literature and current guideline preferences. Our findings extend this literature by focusing specifically on adolescents in routine practice and by incorporating school-related outcomes. At the same time, the real-world nature of the cohort is central to interpretation: the study was designed to reflect routine prescribing patterns rather than to test a tightly standardized efficacy model.
The educational implications of these differences are notable Previous work has shown that adolescents with AR may miss more school and report worse academic functioning than their non-allergic peers. Mechanisms likely include direct symptom burden, sleep fragmentation, and reduced concentration. However, because our absenteeism endpoint captured days missed for any reason, the present findings should be read as evidence of better overall school participation during follow-up rather than as proof that all prevented absences were directly attributable to AR control. The observed differences between groups, particularly for daytime sleepiness, should be interpreted in the context of the study’s real-world, non-randomized design. Because treatment selection was based on routine clinical decision making, the results may partly reflect drug selection bias or confounding by indication rather than true causal treatment-class effects.
Possible Mechanisms
Several mechanisms may explain the observed association between INCS use and better outcomes in this cohort. Intranasal steroids provide broad local anti-inflammatory effects throughout the nasal mucosa and are particularly effective for nasal obstruction, which may in turn improve sleep continuity and daytime functioning. These mechanisms remain biologically plausible hypotheses in the context of the present study, as we did not directly measure inflammatory biomarkers, airflow, or neurocognitive performance.
The side-effect profiles of the treatment classes may also contribute. Sedation and cognitive impairment are well recognised with first-generation antihistamines and have led to strong recommendations against their routine use in school-aged children. Second-generation antihistamines are much less sedating, yet some agents and some individuals remain susceptible to daytime drowsiness. Importantly, our OAH group included several antihistamines with potentially different sedative profiles; therefore, the ESS findings should not be overinterpreted as proving a uniform class effect.
Intranasal antihistamines and fixed intranasal corticosteroid–antihistamine combinations were not evaluated in this study, although both are increasingly relevant in contemporary AR care. Combination intranasal therapy can be more effective than monotherapy in selected patients, and omission of these comparator strategies limits the clinical scope of our conclusions. Accordingly, our findings should be interpreted specifically as a comparison between two common monotherapy approaches used in routine adolescent practice. The mechanisms underlying the observed associations should be considered hypothesis-generating. INCS may have been associated with greater improvement because of broader anti-inflammatory effects on the nasal mucosa, particularly in adolescents with nasal obstruction and sleep disturbance. Improved nasal airflow and reduced nocturnal symptoms may, in turn, have contributed to better sleep quality, reduced daytime impairment, and improved school participation. However, these pathways were not directly measured using inflammatory biomarkers, objective nasal airflow testing, or formal neurocognitive assessment. Therefore, these explanations should be interpreted as plausible mechanisms rather than confirmed causal pathways.
Adherence and Real-World Practice
A common concern is that adolescents may be reluctant to use nasal sprays regularly, preferring tablets. Interestingly, adherence in this study was high and similar between groups, perhaps owing to regular follow-up and clear education. Good adherence was independently associated with greater QoL improvement, although this should be interpreted cautiously because adherence assessment partly relied on self-report and simple dose-count methods rather than electronic monitoring. Adherence appeared to be associated with greater improvement, but this finding should also be interpreted cautiously. Adherence assessment relied partly on self-report, which may be affected by recall and social desirability bias. Therefore, although good adherence may have contributed to better clinical outcomes, the present data cannot fully separate the effect of adherence from patient motivation, family support, symptom severity, or other behavioural factors.
Because this was an observational study, treatment allocation reflected real-world decision making. Clinicians may have preferentially prescribed INCS to students perceived as having more severe nasal obstruction or greater overall burden, while oral medication may have been favoured when convenience or prior treatment preference was prominent. Although measured baseline variables appeared similar, confounding by indication cannot be excluded and remains an important alternative explanation for some between-group differences.
Treatment Heterogeneity and Comparator Limitations
Treatment heterogeneity may have influenced the observed results. Multiple intranasal corticosteroids and multiple second-generation oral antihistamines were grouped within broad treatment classes. This approach reflects routine practice but introduces pharmacological variability and limits the ability to attribute outcomes to specific drugs or even to fully homogeneous class effects. This limitation is particularly relevant for daytime sleepiness, because oral antihistamines may differ in their sedative potential.
Treatment heterogeneity should be considered when interpreting the present findings. Different intranasal corticosteroids and different second-generation oral antihistamines were pooled within broad treatment classes. Although this approach reflects routine clinical practice, it introduces pharmacological variability and reduces internal validity. Therefore, the findings should not be interpreted as evidence for the superiority of any individual intranasal corticosteroid or oral antihistamine agent.
Another important limitation is the absence of additional comparator arms. Intranasal antihistamines, such as azelastine or olopatadine, represent clinically relevant alternatives to oral antihistamines and may provide rapid topical relief of nasal symptoms. Fixed intranasal corticosteroid–intranasal antihistamine combination therapy, such as fluticasone plus azelastine, is also an important option in moderate-to-severe allergic rhinitis and in patients with inadequate response to monotherapy. Because intranasal antihistamine monotherapy and fixed intranasal combination therapy were not evaluated in this cohort, the findings should be interpreted only in relation to INCS monotherapy and second-generation OAH monotherapy, not the full therapeutic spectrum of allergic rhinitis treatment.
The absence of intranasal antihistamine monotherapy and fixed intranasal corticosteroid–intranasal antihistamine combination therapy as comparator arms also limits the clinical scope of the findings. Therefore, the present results should be interpreted only as a comparison between INCS monotherapy and second-generation OAH monotherapy, rather than as evidence covering the full therapeutic spectrum of moderate-to-severe allergic rhinitis.
The absence of additional comparator arms also limits clinical interpretation. Intranasal antihistamines and fixed intranasal corticosteroid–intranasal antihistamine combination therapy are clinically relevant options for moderate-to-severe allergic rhinitis, particularly when rapid symptom relief or escalation beyond monotherapy is required. Because these treatments were not included, the findings should not be generalized to the full therapeutic spectrum of allergic rhinitis management. The observed associations should be interpreted within the limits of the non-randomized observational design. Treatment allocation followed routine clinical practice rather than random assignment, and the findings may have been influenced by confounding by indication, treatment-selection bias, adherence patterns, and unmeasured clinical factors. Therefore, the present results should be considered real-world comparative evidence from one cohort rather than definitive causal proof of treatment superiority.
Strengths and Limitations
Several limitations should be acknowledged. First, the non-randomized design limits causal inference and leaves the possibility of residual confounding and confounding by indication. Second, this was a single-center study with a modest sample size, which may limit generalisability and statistical precision, particularly for secondary outcomes and subgroup analyses. Third, treatment heterogeneity existed within both groups, because different intranasal corticosteroids and different second-generation oral antihistamines were pooled at the treatment-class level. Fourth, classroom productivity was assessed using a pragmatic self-reported measure rather than a formally validated academic-performance instrument or teacher-rated assessment. Fifth, absenteeism was recorded as all-cause school absence rather than AR-specific absence, and therefore should be interpreted as a functional educational outcome rather than a direct disease-attributable measure. Sixth, adherence assessment relied partly on self-report. Finally, the 4-month follow-up period reflects short-term outcomes over one academic term and does not support conclusions regarding long-term effectiveness. Another limitation is that the study did not include intranasal antihistamine monotherapy or fixed intranasal corticosteroid–intranasal antihistamine combination therapy as comparator arms. Therefore, the findings should be interpreted only in relation to the two treatment strategies evaluated—INCS monotherapy and second-generation OAH monotherapy—and should not be generalized to the full therapeutic spectrum of moderate-to-severe allergic rhinitis. Several additional limitations should be considered. Classroom productivity was assessed using a pragmatic self-reported measure rather than a validated presenteeism or academic-performance instrument. No formal adjustment for multiple comparisons was performed, and secondary outcomes were therefore exploratory. The modest sample size limited statistical power for secondary outcomes and subgroup analyses. Finally, the 4-month follow-up period corresponds to one academic term and supports only short-term conclusions; it does not allow assessment of long-term treatment effectiveness, adherence sustainability, or seasonal variability over multiple years.
Overall, these data are plausible and consistent with known pharmacological differences between treatment strategies, but the interpretation remains limited by the observational design, treatment heterogeneity, possible drug selection bias, and the absence of additional comparator arms.
Clinical and Policy Implications
Despite these caveats, the present study offers practical messages for clinicians, families and educators. For clinicians, the data suggest that prioritising intranasal corticosteroids as first-line therapy for adolescent AR, particularly when symptoms affect sleep or school activities, may be associated with better short-term functional outcomes than reliance on oral antihistamine monotherapy alone. However, treatment choice should remain individualised, and options such as intranasal antihistamines or fixed combination intranasal therapy may be appropriate in selected patients.
For families, the findings emphasise that effective management of AR is not merely about reducing sneezing. Appropriate therapy has the potential to improve sleep, mood, and the ability to participate fully in school and extracurricular activities. Engaging adolescents in conversations about their goals and concerns, including academic ambitions, may improve motivation to adhere to therapy.
From an educational perspective, collaboration between healthcare providers and schools could be beneficial. School nurses and teachers who are aware that AR can impair attendance and concentration might be more proactive in identifying students with persistent symptoms and encouraging them to seek medical review.12,13 Policies that facilitate access to medication at school, permit reasonable adjustments during examination periods and support healthy sleep routines may help mitigate the impact of AR on learning.
Conclusion
In this real-world cohort of adolescents with moderate-to-severe allergic rhinitis, INCS monotherapy was associated with greater short-term improvements in disease-specific quality of life and school-attendance outcomes compared with second-generation OAH monotherapy. These findings are consistent with current guideline preferences for INCS in moderate-to-severe allergic rhinitis; however, the observational, non-randomized design, treatment heterogeneity, and absence of intranasal antihistamine and fixed intranasal combination-therapy comparator arms limit causal inference and generalisability. Larger randomized or multicenter studies are needed to confirm these associations and to compare broader treatment strategies in adolescent populations.
Data Sharing Statement
The data are not publicly available due to privacy concerns. However, data are available from the corresponding author upon reasonable request.
Ethics Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Artuklu University Medical Faculty Hospital (approval #2025/9-37, dated September 9, 2025).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brożek JL, Bousquet J, Agache I, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines-2016 revision. J Allergy Clin Immunol. 2017;140(4):950–14. doi:10.1016/j.jaci.2017.03.050
2. Seidman MD, Gurgel RK, Lin SY, et al. Clinical practice guideline: allergic rhinitis. Otolaryngol Head Neck Surg. 2015;152(1 Suppl):S1–43. doi:10.1177/0194599814561600
3. Juniper EF, Howland WC, Roberts NB, Thompson AK, King DR. Measuring quality of life in children with rhinoconjunctivitis. J Allergy Clin Immunol. 1998;101(2 Pt 1):163–170. doi:10.1016/s0091-6749(98)70380-x
4. Juniper EF, Thompson AK, Ferrie PJ, Roberts JN. Validation of the standardized version of the rhinoconjunctivitis quality of life questionnaire. J Allergy Clin Immunol. 1999;104(2 Pt 1):364–369. doi:10.1016/s0091-6749(99)70380-5
5. Izci B, Ardic S, Firat H, Sahin A, Altinors M, Karacan I. Reliability and validity studies of the Turkish version of the epworth sleepiness scale. Sleep and Breathing. 2008;12(2):161–168. doi:10.1007/s11325-007-0145-7
6. Johns MW. A new method for measuring daytime sleepiness: the epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
7. Rosario CS, Murrieta-Aguttes M, Rosario NA. Allergic rhinits: impact on quality of life of adolescents. Eur Ann Allergy Clin Immunol. 2021;53(6):247–251. doi:10.23822/EurAnnACI.1764-1489.176
8. D’Elia C, Gozal D, Bruni O, Goudouris E, Meira ECM. Allergic rhinitis and sleep disorders in children - coexistence and reciprocal interactions. J Pediatr. 2022;98(5):444–454. doi:10.1016/j.jped.2021.11.010
9. Meltzer EO. Quality of life in adults and children with allergic rhinitis. J Allergy Clin Immunol. 2001;108(1 Suppl):S45–53. doi:10.1067/mai.2001.115566
10. Sousa-Pinto B, Vieira RJ, Brozek J, et al. Intranasal antihistamines and corticosteroids in allergic rhinitis: a systematic review and meta-analysis. J Allergy Clin Immunol. 2024;154(2):340–354. doi:10.1016/j.jaci.2024.04.016
11. Kennedy R. Mechanisms and comparative treatments of allergic rhinitis including phototherapy. Allergies. 2024;4(1):17–29. doi:10.3390/allergies4010002
12. Blaiss MS, Hammerby E, Robinson S, Kennedy-Martin T, Buchs S. The burden of allergic rhinitis and allergic rhinoconjunctivitis on adolescents: a literature review. Ann Allergy Asthma Immunol. 2018;121(1):43–52.e3. doi:10.1016/j.anai.2018.03.028
13. Jáuregui I, Mullol J, Dávila I, et al. Allergic rhinitis and school performance. J Investig Allergol Clin Immunol. 2009;19 Suppl 1:32–39.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.