Back to Journals » Clinical Ophthalmology » Volume 15
Intra-Operative Discomfort in Photorefractive Keratectomy
Authors Philbrick SM, Bennion JL ![]()
Received 3 July 2021
Accepted for publication 9 September 2021
Published 13 October 2021 Volume 2021:15 Pages 4121—4130
DOI https://doi.org/10.2147/OPTH.S327057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Samuel M Philbrick,1 John L Bennion2
1Department of Operational and Readiness Medicine, Joint Base Elmendorf-Richardson Hospital, Elmendorf, AK, USA; 2Department of Ophthalmology, Saint Alphonsus Health System, Boise, ID, USA
Correspondence: Samuel M Philbrick Email [email protected]
Purpose: Photorefractive keratectomy (PRK) remains a viable, safe, and efficacious option for patients wishing to correct refractive errors. One of its most significant drawbacks is pain. While post-operative pain has been well studied with different management options, intra-operative pain has been less well defined. The purpose of this study was to characterize intra-operative pain during PRK in regard to eye operated on, gender, excimer platform used, surgeon, and age.
Patients and Methods: A total of 134 patients (264 eyes) were prospectively randomized to undergo bilateral PRK of either the right eye first or the left eye first followed immediately by the fellow eye. In the immediate post-operative period they were surveyed using an 11-point Numeric Rating Scale regarding intra-operative pain or discomfort experienced in each eye. Resultant pain scores were then analyzed via two sample z-test and analysis of variance (ANOVA) to characterize pain overall as well as comparing first versus second eye operated on, right versus left eye, male versus female, excimer platform used, inter-surgeon variability, and age.
Results: Of 264 eyes surveyed the mean pain experienced on a 0– 10 pain scale was 1.13 (minimal discomfort). There was no statistically significant difference in pain or discomfort when comparing first versus second eye operated on, right versus left eye, male versus female, excimer platform used, operating surgeon, or age.
Conclusion: Intra-operative pain or discomfort experienced by patients is minimal. The absence of statistically significant differences in pain scores studied implies that standard of care procedures achieve adequate analgesia in PRK.
Keywords: corneal refractive surgery, CRS, myopia, VISX, EX500, military medicine, inter-surgeon variability, order effect, PRK, laser in situ keratomileusis, LASIK, laser assisted sub-epithelial keratectomy, LASEK, z-test, pain, anesthetic, analgesia
Introduction
Photorefractive Keratectomy (PRK) remains a viable option for patients considering corneal refractive surgery (CRS). In the United States military, PRK has been and remains the most common CRS procedure, more common than Laser In Situ Keratomileusis (LASIK) or small incision lenticule extraction (SMILE).1–3 While PRK does have distinct advantages it also has disadvantages, namely slower visual rehabilitation and post-operative discomfort.4,5 Well studied post-operative pain management strategies have helped to mitigate this disadvantage although pain remains a major obstacle for patients choosing PRK. Consequently, patients often inquire as to what to expect intra-operatively.
The cornea is a densely innervated tissue that responds well to topical anesthetics. Topical tetracaine and proparacaine have demonstrated efficacy for mitigating discomfort in various eye procedures including CRS.6 While this application of topical anesthesia generally allows patients to tolerate CRS without issue, from patient feedback at our center we anecdotally noted a varied response to the level of pain or discomfort experienced when comparing the first eye treated versus the second. This led us to question whether it is possible to identify measurable differences in pain levels experienced when comparing laterality, gender, excimer laser platform, operating surgeon, or age. To our knowledge, there are no studies that specifically attempt to characterize and quantify pain or discomfort experienced during PRK.
Methods
One hundred and thirty-seven subjects undergoing bilateral PRK at the Joint Warfighter Refractive Surgery center at Wilford Hall Ambulatory Surgical Center (WHASC) in San Antonio, Texas between June 2014 and May 2015 were studied. PRK was performed with either the VISX CustomVue STAR S4 IR (Abbott Medical Optics, Santa Ana, CA, USA) or WaveLight EX500 (Alcon Inc., Fort Worth, TX, USA) excimer laser machine at the surgeon’s discretion.
To be included in the study, patients needed to qualify for bilateral PRK and be at least 21 years old. Patients were excluded if they were pregnant, basic military trainees, prisoners, detainees, did not meet criteria for CRS, if they were receiving treatment on one eye, or if they were undergoing monovision PRK. Upon inclusion in the study cohort, patients were randomized to receive PRK in either the right or left eye first using the Research Randomizer tool (www.randomizer.org).
Pre-Operative Counseling and Management
As standard of care, all persons undergoing refractive surgery are brought together for a group educational meeting regarding refractive surgery. At this meeting patients are informed about WHASC standard of care procedures for pain management and about the risks and benefits of refractive surgery, including risk for intra-operative discomfort or pain. During the study period, individuals planning on undergoing PRK were notified of the opportunity to participate in this study and informed that their pain management would not be altered if they chose to participate or not to participate. Interested potential participants received a verbal and written explanation of the pain scale. The 0–10 Numeric Rating Scale (NRS) was employed to measure pain (Figure 1). This scale was selected for its established validity in a variety of settings and simplicity of use compared against Visual Analogue Scale (VAS) and other modalities.7–9 Pre-operative benzodiazepines and oral NSAIDs are not part of WHASC’s standard of care protocol for PRK and were not evaluated in this study.
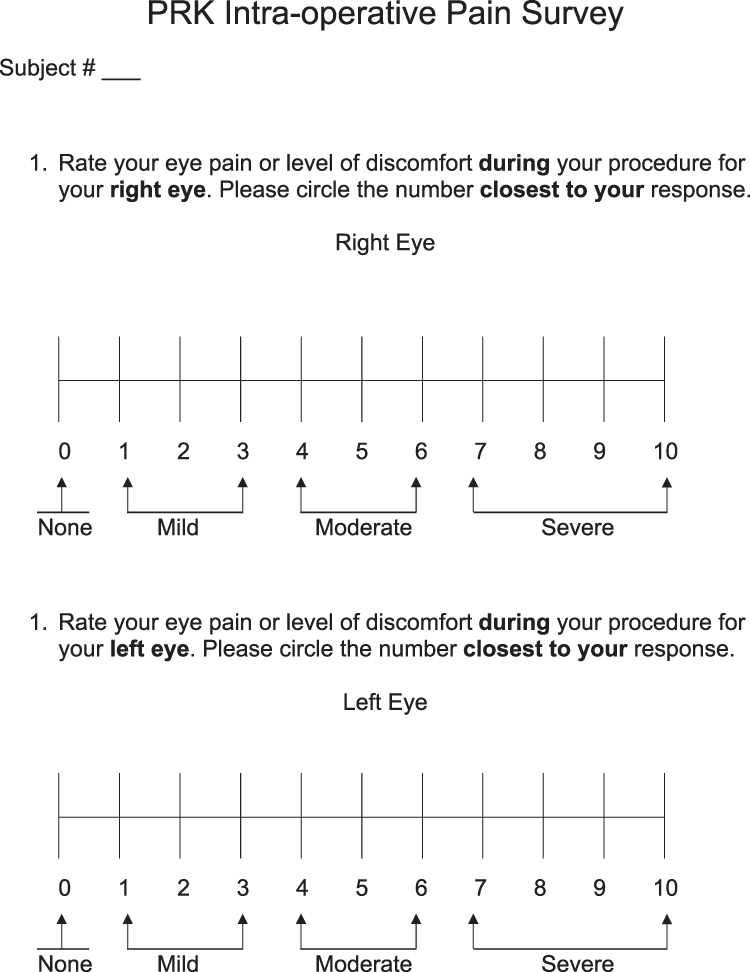 |
Figure 1 Pain numeric rating scale (NRS). This pain scale was completed by each subject on completion of PRK. |
Operative Management
Photorefractive keratectomy was performed in the usual fashion except for the fact that it is typical to operate on the right eye first, and half of the patients had their left eye treated first. Perioperative pain management and refractive surgery were accomplished in accordance with the WHASC institutional standard of care by one of four attending surgeons. Anesthesia was achieved by administration of several drops of 0.5% proparacaine hydrochloride (Bausch and Lomb, Inc.) before entering the operating suite, and by administration of one additional drop to the eye undergoing PRK immediately before removal of the corneal epithelium. The corneal epithelial layer was removed mechanically with an Amoils rotary brush (Innovative Excimer Solutions, Inc.). Following laser ablation of corneal stroma the ocular surface was irrigated with chilled BSS. One drop of topical prednisolone acetate 1% and one drop of moxifloxacin were then instilled in the treated eye. A bandage contact lens was then applied. Topical NSAIDs were not administered post-operatively nor were bandage contact lenses soaked in NSAID as these treatments were not part of the WHASC institutional standard of care. Mitomycin C 0.02% pledgets were applied to the treated area per surgeon discretion. Immediately following the procedure, while in the surgical suite, patients were asked to rate their pain during the procedure in each eye.
The survey ranked pain with the following prompts (Figure 1):
- Rate your eye pain or level of discomfort during your procedure for your right eye. Please circle the number closest to your response.
- Rate your eye pain or level of discomfort during your procedure for your left eye. Please circle the number closest to your response.
Ethical Standards
The WHASC Institutional Review Board reviewed and approved the study protocol in accordance with the tenets of the Declaration of Helsinki. Subjects had a minimum of 24 h to review informed consent and HIPAA authorization forms. Administration of peri-operative analgesia was neither modified nor restricted. To avoid conflict of interest, presentation of the study and recruitment to the prospective cohort was done by an investigator who would not be the operating surgeon for the recruited patient.
Statistical Analysis
Ophthalmologists aim for zero intra-operative pain in PRK, though some patients experience moderate or severe discomfort. While the mode reported pain on a 0–10 scale may be “0” and the median near-zero for a given cohort of patients, outliers are expected despite appropriate application of analgesia. Therefore, the distribution of pain scores given by patients for this procedure was expected to skew towards 0 and to have a single tail. Sample variance was defined by analysis of pain scores from the 268 eyes studied and that variance was used to perform a two sample z-test at α=0.05 looking for statistically significant difference between the mean pain scores of the first and second eye treated. Likewise, mean pain score differences were analyzed for statistical significance with a z-test at α=0.05 comparing the ablative laser platform used (VISX and EX500), gender, age group (age <40 and age ≥40). When pain scores could not be paired due to an unequal number of subjects in compared groups, difference scores between reported pain and a hypothesized median difference score of 0 were used. Differences in mean pain scores between operating surgeons were analyzed by single-factor analysis of variance (ANOVA).
The primary outcome measure was difference in perceived intra-operative pain or discomfort between the first-eye and second-eye surgeries, measured by a 0–10 NRS. Secondary outcome measures were differences in perceived pain comparing gender, age, laser platform used, and operating surgeon.
Results
The study enrolled 137 patients. Three were excluded because they elected for monovision treatment. Entities studied were 268 eyes from the remaining 134 patients, 110 (82%) female, 105 (78%) younger than 40. Number of eyes operated on by surgeons 1–4 were 80, 72, 28, and 88, respectively. Seventy-eight eyes were treated with the EX500 laser, and 190 with the VISX. Sixty-seven patients were randomized to group 1 (right eye treated first) and 67 to group 2 (left eye treated first).
Among the 268 eyes that received treatment the minimum reported pain or discomfort was 0; maximum reported pain was 8. The mean pain across all eyes was 1.13 (95% CI = 0.95–1.30), and the mode was 0. Twenty-six of 134 patients (19.4%) reported zero pain in one eye and the presence of discomfort in the contralateral eye. Of these patients with pain in only one eye, 25 (96%) reported mild pain (pain level: 1–3) and one patient reported moderate pain (pain level: 4). Out of the whole study group, only 2 patients (1.5%) reported severe (7–10) pain. One reported pain or discomfort of 6 and 8, the other reported pain of 7 in both eyes. Statistical analysis comparing first-eye discomfort to second-eye discomfort failed to reject the null hypothesis, with mean pain in the first eye of 1.01 (95% CI = 0.81–1.22) and mean pain in the second eye 1.25 (95% CI = 1.04–1.46); P = 0.09 (Figure 2). These data do not imply a statistically significant difference in pain levels between the first and second eye undergoing PRK.
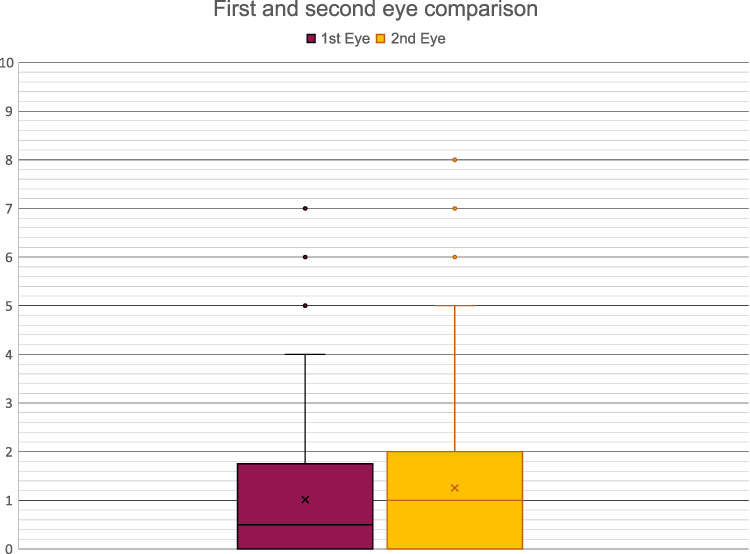 |
Figure 2 First and second eye comparison. Scores for first-eye and second-eye pain are reflected in this box plot. In the first eye, mean pain (“x”) was 1.01, interquartile range (inclusive) was 0–1.75, median pain (crossbar) was 0.5, and the mode was 0. In the second eye, mean pain was 1.25 (“x”), interquartile range (inclusive) was 0–2, median pain was 0, and the mode was 0. Outlier data points are plotted with single dots. For these data, P=0.09. |
Covariate analysis likewise did not show a statistically significant difference between groups. Mean right eye pain was 1.04 (95% CI = 0.84–1.24), mean left eye pain was 1.22 (95% CI = 1.01–1.44); P = 0.15 (Figure 3). Males reported mean pain of 1.15 (95% CI = 0.81–1.48), females reported mean pain 1.13 (95% CI = 0.97–1.29); P = 0.47 (Figure 4). Patients who received treatment with the EX500 laser reported mean discomfort 1.24 (95% CI = 0.93–1.55), the mean for those treated with the VISX platform was 1.09 (95% CI = 0.92–1.25); P = 0.11 (Figure 5). For patients aged 40 years or more mean pain was 0.95 (95% CI = 0.62–1.27), and mean pain was 1.19 (95% CI = 1.02–1.35) for patients younger than 40; P = 0.14 (Figure 6). Regarding inter-surgeon analysis, mean reported pain scores were: Surgeon 1 = 1.44 (95% CI = 1.09–1.78), Surgeon 2 = 0.92 (95% CI = 0.70–1.13), Surgeon 3 = 1.04 (95% CI = 0.67–1.40), and Surgeon 4 = 1.07 (95% CI = 0.83–1.31). The differences between these surgeons’ mean pain scores did not achieve statistical significance (P = 0.14) (Figure 7). A comparison of difference between subject’s first and second eye pain scores and subject’s average pain score had a Spearman rho of 0.08 (P = 0.18), which did not imply a correlation between patients’ average pain and whether they experienced an order effect in eye pain (Figure 8).
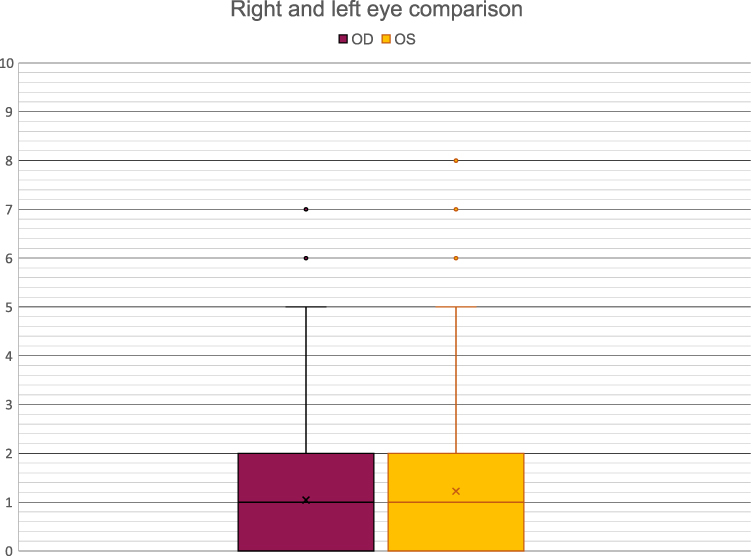 |
Figure 3 Right and left eye comparison. Scores for right and left eye pain are reflected in this box plot. In the right eye, mean pain (“x”) was 1.04, interquartile range (inclusive) was 0–2, median pain was 1 (crossbar), and the mode was 0. In the left eye, mean pain was 1.22, interquartile range (inclusive) was 0–2, median pain was 1, and the mode was 0. Outlier data points are plotted with single dots. For these data, P=0.15. |
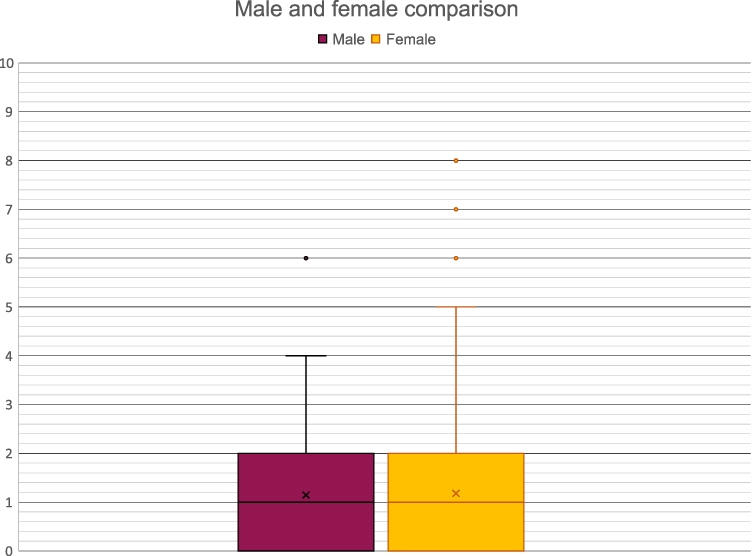 |
Figure 4 Male and female comparison. Scores reported by men and women are reflected in this box plot. For men, mean pain (“x”) was 1.15, interquartile range (inclusive) was 0–2, median pain was 1 (crossbar), and the mode was 0. For women, mean pain was 1.13, interquartile range (inclusive) was 0–2, median pain was 1, and the mode was 0. Outlier data points are plotted with single dots. For these data, P=0.47. |
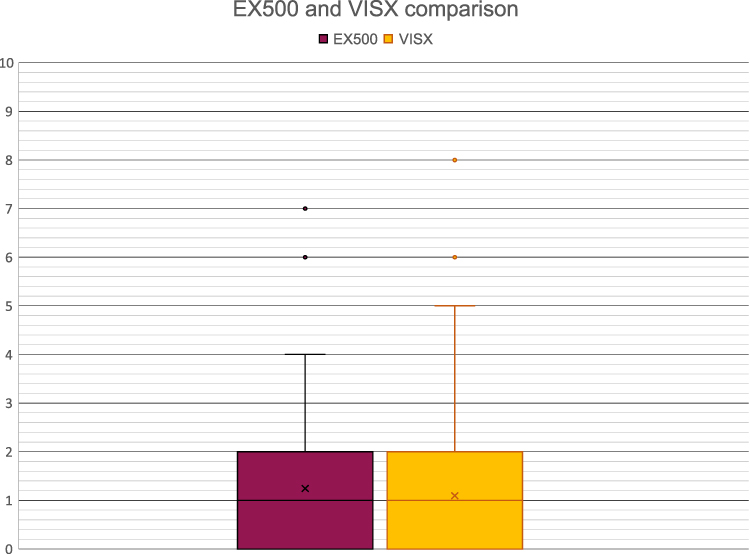 |
Figure 5 EX500 and VISX comparison. Scores reported for eyes undergoing PRK with EX500 and VISX excimer lasers are reflected in this box plot. For the EX500, mean pain (“x”) was 1.24, interquartile range (inclusive) was 0–2, median pain was 1 (crossbar), and the mode was 0. For the VISX, mean pain was 1.09, interquartile range (inclusive) was 0–2, median pain was 1, and the mode was 0. Outlier data points are plotted with single dots. For these data, P=0.11. |
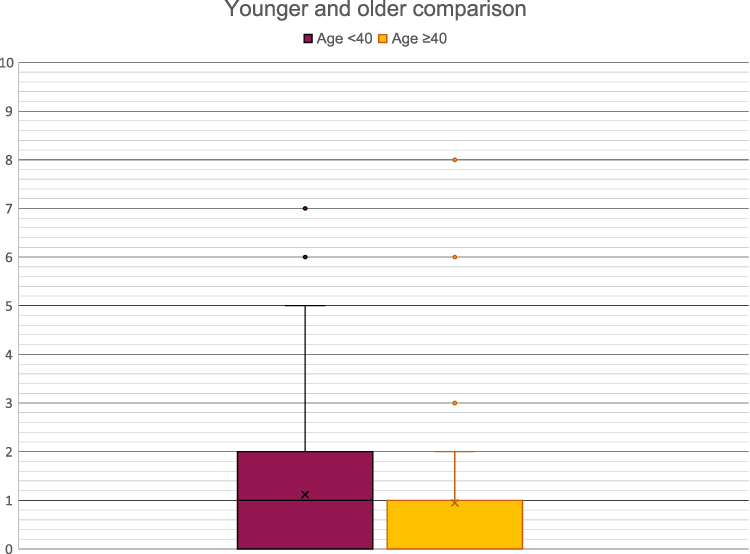 |
Figure 6 Age-based comparison. Scores reported by patients younger than 40 and by patients aged 40 years or more are reflected in this box plot. For patients younger than 40, mean pain (“x”) was 1.19, interquartile range (inclusive) was 0–2, median pain was 1 (crossbar), and the mode was 0. For patient’s older than 40, mean pain was 0.95, interquartile range (inclusive) was 0–1, median pain was 0, and the mode was 0. Outlier data points are plotted with single dots. For these data, P=0.14. |
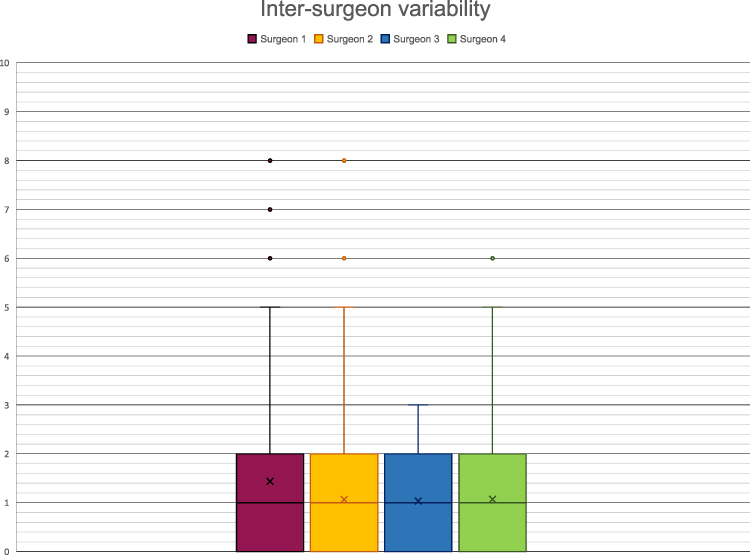 |
Figure 7 Inter-surgeon variability. Scores reported for surgeons are reflected in this box plot. For surgeon 1, mean pain (“x”) was 1.43, interquartile range (inclusive) was 0–2, median pain was 1 (crossbar), and the mode was 0. For surgeon 2, mean pain was 1.07, interquartile range (inclusive) was 0–2, median pain was 1, and the mode was 0. For surgeon 3, mean pain was 1.04, interquartile range (inclusive) was 0–2, median pain was 1, and the mode was 0. For surgeon 2, mean pain was 1.07, interquartile range (inclusive) was 0–2, median pain was 1, and the mode was 0. Outlier data points are plotted with single dots. For these data, P=0.14. |
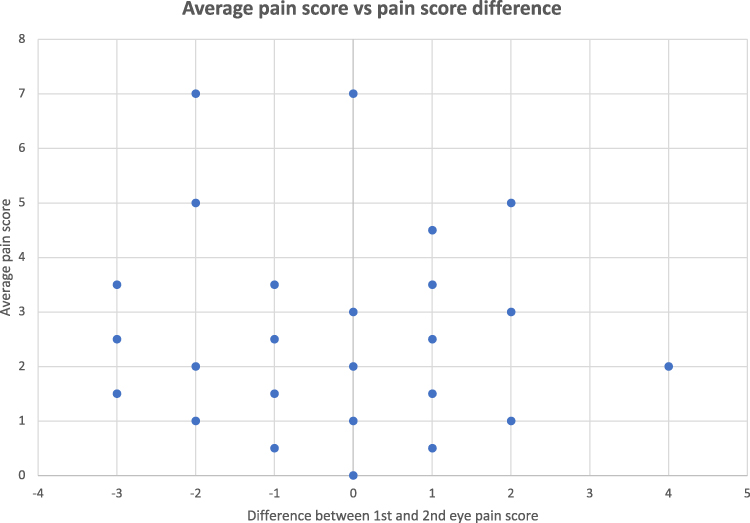 |
Figure 8 Average pain score vs pain score difference. Scattergram plot of the difference between the first and second pain scores and the average pain score of first and second eye pain scores. A strong correlation could indicate if patients who tended to rank pain more highly were also more sensitive to an “order effect,” experiencing more pain in the second eye undergoing PRK. However there is no strong correlation between average pain score and whether subjects ranked pain as higher in the first or second eye undergoing PRK. Spearman rho=0.08; P=0.18. |
Discussion
Photorefractive keratectomy and LASIK are favored as a corrective interventions for many patients with low-to-moderate myopia, low hyperopia, and astigmatism given their long-term efficacy improving visual acuity.10 LASIK has grown in popularity and been approved across the spectrum of Air Force occupations. However, recent studies and systematic reviews comparing LASIK and PRK, and their variants aided by wavefront technologies have not proved significant differences in outcomes with respect to visual acuity, spherical aberration (SA), or higher-order aberrations (HOAs).11–17 As such, PRK is likely to remain a popular choice for refractive surgery in the Air Force. Reducing intra-operative discomfort would further optimize this therapy that improves warfighting readiness and quality of life. This study looked for a change in perceived pain in the first or second eye undergoing PRK. Evidence suggesting an order effect in perceived pain could more effectively guide administration of intra-operative analgesia.
An order effect was observed by Cheng et al when comparing perceived pain between first-eye and second-eye LASIK surgeries, but only at the stages of speculum placement and microkeratome pass.18 Subsequently Rami et al noted an increase in reported pain for the second eye treated with LASIK; however, pain was measured during suction-ring placement, a step that does not occur in PRK.19 Sharma et al and Nijkamp et al compared first-eye and second-eye cataract surgeries and did not find a statistically significant difference in perceived pain.20,21 In keeping with these findings, Moshirfar et al analyzed data comparing proparacaine and tetracaine in 128 patients undergoing CRS and found a slight first-eye preference that did not achieve statistical significance.6 This study likewise demonstrated an increase in mean second-eye pain that was not statistically significant.
Regarding sample size and power, this study is comparable to the aforementioned reports. One hundred and thirty-seven patients were initially recruited to this study, and 134 included after application of exclusion criteria. Moshirfar et al enrolled 128, Sharma et al enrolled 127, Nijkamp et al enrolled 128, Rami et al enrolled 154, and Cheng et al enrolled 50 patients. In this study, the difference in mean pain score between the first eye and second eye was 0.24, and to show a difference in mean pain scores of 0.23 or more was statistically significant at α=0.05, an enrollment of 300 patients—more than twice as many as were recruited in a 1.5 year period—would have been needed. Even if a statistically significant difference had been observed, it is not clear that the difference would have been clinically significant.
This study was limited by several factors. First, the pain scale employed may have measured discomfort imperfectly. Investigators employed an NRS for pain with 4 labeled categories (none, mild, moderate, and severe). A variety of NRSs are used to measure discomfort, each with slight variations in “anchor” words used to guide patients’ understanding. The degree to which these anchor words skew pain scores has been evaluated but is not fully understood.8 The word “discomfort” was employed in the survey to counteract potential skew towards “0” scores as some patients might consider the PRK procedure “painless” but admit experiencing some level of discomfort. In support of using the NRS, this scale is thought to be sensitive to changes within individuals, and less affected by patient age and non-pain intensity factors such as pain beliefs and pain catastrophizing.22–25 Future research seeking accurate measures of non-intensity pain factors, such as pain unpleasantness, could consider other pain scales, especially the Faces Pain Scale-Revised (FPS-R).23
Additionally, the enrolled subjects were predominantly younger than 40 (78%) and female (82%). If statistically significant results had been observed, then applying those observations to inform treatment of older patients or male patients would have been more challenging. Future studies comparing first-eye and second-eye pain during ophthalmic procedures could consider seeking greater enrollment to gain statistical power. It will remain pertinent to describe when patients report pain, especially if it is during (and at which step), or after the procedure.
The mode pain or discomfort score of zero, together with statistical analyses of pain scores reinforce that following standard of care procedures for PRK may be trusted to minimize intra-operative pain. Data gathered do not imply a benefit to modifying analgesia for the second eye treated in PRK.
Abbreviations
FPS-R, Faces Pain Scale-Revised; LASEK, laser epithelial keratomileusis; LASIK, laser in situ keratomileusis; NRS, Numeric Rating Scale; PRK, photorefractive keratectomy; VRS, Verbal Rating Scale; WHASC, Wilford Hall Ambulatory Surgical Center.
Acknowledgments
Surgeries followed in this study were performed by Vasudah Panday, Robert Smith, Walter Steigleman, and James Richard Townley. Dr Matthew Caldwell advised as an associate investigator. Research optometrist Douglas Apsey assisted with statistical analysis. Kathleen Dinan served as the ophthalmic technician for patients enrolled in the study.
Funding
This investigation required no supplementary funding from Graduate Medical Education or extramural sources.
Disclosure
The authors have no conflicts of interest to disclose relating to this work.
References
1. Panday VA, Reilly CD. Refractive surgery in the United States air force. Curr Opin Ophthalmol. 2009;20:242–246. doi:10.1097/ICU.0b013e32832a6f5a
2. Cousineau-Krieger C, Caldwell M, Panday VA, Apsey D, Reilly C. Infection following photorefractive keratectomy. Ophthalmology. 2012;120(3):642. doi:10.1016/j.ophtha.2012.10.013
3. Stanley PF, Tanzer DJ, Schallhorn SC. Laser refractive surgery in the United States Navy. Curr Opin Ophthalmol. 2008;19:321–324. doi:10.1097/ICU.0b013e3283009ee3
4. Shetty R, Dalal R, Nair AP, Khamar P, D’Souza S, Vaishnav R. Pain management after photorefractive keratectomy. J Cataract Refract Surg. 2019;45(7):972–976. doi:10.1016/j.jcrs.2019.01.032
5. Caldwell M, Reilly C. Effects of topical nepafenac on corneal epithelial healing time and postoperative pain after PRK: a bilateral, prospective, randomized, masked trial. J Refract Surg. 2008;24(4):377–382.
6. Moshirfar M, Mifflin MD, McCaughey MV, Gess AJ. Prospective, randomized contralateral eye comparison of tetracaine and proparacaine for pain control in laser in situ keratomileusis and photorefractive keratectomy. Clin Opth. 2014;8:1219–1231.
7. Karcioglu O, Topacoglu H, Dikme O, Dikme O. A systematic review of the pain scales in adults: which to use? Am J Emerg Med. 2018;36:707–714. doi:10.1016/j.ajem.2018.01.008
8. Hjermstad MJ, Fayers PM, Haugen DF, et al. Studies comparing numerical rating scales, verbal rating scales, and visual analogue scales for assessment of pain intensity in adults: a systematic literature review. J Pain Symptom Manage. 2011;41(6):1073–1093. doi:10.1016/j.jpainsymman.2010.08.016
9. Bendinger T, Plunkett N. Measurement in pain medicine. BJA Educ. 2016;16(9):310–315. doi:10.1093/bjaed/mkw014
10. Godwalla RY, Magone MT, Kaupp SB, Jung H, Cason JB. Long-term outcomes of refractive surgery performed during the military. Mil Med. 2019;184:e808–e812. doi:10.1093/milmed/usz096
11. Lee MD, Chen LY, Tran EM, Manche EE. A prospective comparison of wavefront-guided LASIK versus wavefront-guided PRK after previous keratorefractive surgery. Clin Ophthalmol. 2020;14:3411–3419. doi:10.2147/OPTH.S276381
12. Ryan DS, Sia RK, Rabin J, et al. Contrast sensitivity after wavefront-guided and wavefront-optimized PRK and LASIK for myopia and myopic astigmatism. J Refract Surg. 2018;34(9):590–596. doi:10.3928/1081597X-20180716-01
13. Barreto J, Barboni MTS, Feitosa-Santana C, et al. Intraocular straylight and contrast sensitivity after contralateral wavefront-guided LASIK and wavefront-guided PRK for myopia. J Refract Surg. 2010;26(8):588–593. doi:10.3928/1081597X-20090930-01
14. Jahadi Hosseini SH, Abtahi SM, Khalili MR. Comparison of higher order aberrations after wavefront-guided LASIK and PRK: one year follow-up results. J Ophthalmic Vis Res. 2016;11(4):350–357. doi:10.4103/2008-322X.194069
15. Shortt AJ, Allan DS, Evans JR. Laser-assisted in-situ keratomileusis (LASIK) versus photorefractive keratectomy (PRK) for myopia. Cochrane Database Syst Rev. 2013;1:CD005135.
16. Settas G, Settas C, Minos E, Yeung YL. Photorefractive keratectomy (PRK) versus laser assisted in situ keratomileusis (LASIK) for hyperopia correction. Cochrane Database Syst Rev. 2012;6:CD007112.
17. Li SM, Kang MT, Wang NL, Abariga SA. Wavefront excimer laser refractive surgery for adults with refractive errors. Cochrane Database Syst Rev. 2020;12:CD012687.
18. Cheng AC, Young AL, Law RW, Lam DS. Prospective randomized double-masked trial to evaluate perioperative pain profile in different stages of simultaneous bilateral LASIK. Cornea. 2006;25(8):919–922. doi:10.1097/01.ico.0000226363.19054.2a
19. El Rami H, Fadlallah A, Fahd D, Fahed S. Patient-perceived pain during laser in situ keratomileusis: comparison of fellow eyes. J Cataract Refract Surg. 2012;38(3):453–457. doi:10.1016/j.jcrs.2011.10.028
20. Sharma NS, Ooi JL, Figueira EC, et al. Patient perceptions of second eye clear corneal cataract surgery using assisted topical anaesthesia. Eye. 2008;22(4):547–550. doi:10.1038/sj.eye.6702711
21. Nijkamp MD, Kenens CA, Dijker AJ, Ruiter RA, Hiddema F, Nuijts RM. Determinants of surgery related anxiety in cataract patients. Br J Ophthalmol. 2004;88(10):1310–1314. doi:10.1136/bjo.2003.037788
22. Safikhani S, Gries KS, Trudeau JJ, et al. Response scale selection in adult pain measures: results from a literature review. J Patient Rep Outcomes. 2018;2:40. doi:10.1186/s41687-018-0053-6
23. Thong ISK, Jensen MP, Miró J, Tan G. The validity of pain intensity measures: what do the NRS, VAS, VRS, and FPS-R measure? Scand J Pain. 2018;18(1):99–107. doi:10.1515/sjpain-2018-0012
24. Jensen MP, Tomé-Pires C, de la Vega R, Galán S, Solé E, Miró J. What determines whether a pain is rated as mild, moderate, or severe? The importance of pain beliefs and pain interference. Clin J Pain. 2017;33(5):414–421. doi:10.1097/AJP.0000000000000429
25. Gagliese L, Weizblit N, Ellis W, Chan VWS. The measurement of postoperative pain: a comparison of intensity scales in younger and older surgical patients. Pain. 2005;117(3):412–420. doi:10.1016/j.pain.2005.07.004
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.