Back to Journals » Journal of Multidisciplinary Healthcare » Volume 9
Interprofessional teamwork innovations for primary health care practices and practitioners: evidence from a comparison of reform in three countries
Authors Harris M, Advocat J, Crabtree B, Levesque J, Miller W, Gunn J, Hogg W, Scott C, Chase S, Halma L, Russell G ![]()
Received 29 September 2015
Accepted for publication 27 November 2015
Published 29 January 2016 Volume 2016:9 Pages 35—46
DOI https://doi.org/10.2147/JMDH.S97371
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Mark F Harris,1 Jenny Advocat,2 Benjamin F Crabtree,3 Jean-Frederic Levesque,1,4 William L Miller,5 Jane M Gunn,6 William Hogg,7 Cathie M Scott,8 Sabrina M Chase,9 Lisa Halma,10 Grant M Russell11
1Center for Primary Health Care and Equity, University of New South Wales, Sydney, NSW, 2Southern Academic Primary Care Research Unit, School of Primary Health Care, Monash University, Notting Hill, VIC, Australia; 3Department of Family Medicine and Community Health, Rutgers Robert Wood Johnson Medical School, New Brunswick, NJ, USA; 4Bureau of Health Information, NSW Government, Sydney, NSW, Australia; 5Department of Family Medicine, Lehigh Valley Health Network, Allentown, PA, USA; 6Department of General Practice, The University of Melbourne, Melbourne, VIC, Australia; 7The CT Lamont Primary Care Research Center, The University of Ottawa, Ottawa, ON, 8Alberta Centre for Child, Family, and Community Research, University of Calgary, AB, Canada; 9Rutgers University, Rutgers School of Nursing, Rutgers, NJ, USA; 10Alberta Health Services, Lethbridge, AB, Canada; 11School of Primary Health Care, Monash University, Notting Hill, VIC, Australia
Context: A key aim of reforms to primary health care (PHC) in many countries has been to enhance interprofessional teamwork. However, the impact of these changes on practitioners has not been well understood.
Objective: To assess the impact of reform policies and interventions that have aimed to create or enhance teamwork on professional communication relationships, roles, and work satisfaction in PHC practices.
Design: Collaborative synthesis of 12 mixed methods studies.
Setting: Primary care practices undergoing transformational change in three countries: Australia, Canada, and the USA, including three Canadian provinces (Alberta, Ontario, and Quebec).
Methods: We conducted a synthesis and secondary analysis of 12 qualitative and quantitative studies conducted by the authors in order to understand the impacts and how they were influenced by local context.
Results: There was a diverse range of complex reforms seeking to foster interprofessional teamwork in the care of patients with chronic disease. The impact on communication and relationships between different professional groups, the roles of nursing and allied health services, and the expressed satisfaction of PHC providers with their work varied more within than between jurisdictions. These variations were associated with local contextual factors such as the size, power dynamics, leadership, and physical environment of the practice. Unintended consequences included deterioration of the work satisfaction of some team members and conflict between medical and nonmedical professional groups.
Conclusion: The variation in impacts can be understood to have arisen from the complexity of interprofessional dynamics at the practice level. The same characteristic could have both positive and negative influence on different aspects (eg, larger practice may have less capacity for adoption but more capacity to support interprofessional practice). Thus, the impacts are not entirely predictable and need to be monitored, and so that interventions can be adapted at the local level.
Keywords: interprofessional care, primary health care, teamwork, research synthesis
Introduction
Enhancing interprofessional team care has been a key element of primary health care (PHC) reform in many countries.1,2 Team-related reforms have been built in the recognition that care is becoming increasingly complex for populations affected by multimorbidity and long-term physical and psychological conditions. More comprehensive care can be provided by health professionals from multiple disciplines working together as a team.3 Team-based care is also a critical element of the patient-centered medical home model.4
Interprofessional team-based care has been demonstrated to improve quality of care and outcomes in patients with chronic disease in primary care.5–8 Teamwork may also reduce costs and improve care coordination for PHC organizations and enhance job satisfaction among health professionals.9,10
International surveys conducted by the Commonwealth Fund and other bodies have demonstrated considerable intercountry variability in the implementation of interprofessional team care in PHC.11 However, the impacts of policies that aim to improve team care within PHC organizations have not been intensively studied, and the degree to which it is possible to transfer research into the implementation of teamwork across jurisdictional boundaries and contexts is unclear.
Interprofessional teamwork may be considered as “a dynamic process involving two or more health care professionals with complementary backgrounds and skills, sharing common health goals and exercising concerted, physical and mental effort in assessing, planning, or evaluating patient care.”12 This study aimed to describe how interventions and reform policies to enhance teamwork impacted on communication, relationships, role definition, and work satisfaction in PHC.
Methods
Our approach13 draws upon the principles of participatory action research14 and narrative, meta-narrative, and realist synthesis15–17 using an open system approach.18 Participatory action research seeks to integrate participatory interaction and the lived experience into the research process. In our approach, established investigators were brought together as active observers and participants in a deliberative iterative process of sharing, reflection, and synthesis. Deliberative process allows a group of participants to receive and exchange information, to critically examine an issue, and to come to consensus agreement. Specifically, an analytic-deliberative approach was used that combines technical and content expertise with the values and experiences and investigators. A distinctive feature of our approach is that a group of researchers from different contexts reflect together over a prolonged time frame to actively reinterpret findings from their own published research as well as raw data. In this way, the authors of original research papers become active participants in the process and use the collective studies of the collaborative group to explore and challenge each other’s published findings, underlying assumptions, and personal experiential knowledge. The shared understandings that emerge draw on principles of realist evaluation to focus attention on ways in which contexts and mechanisms could be identified as impacting on study outcomes.
Ethical considerations
The original studies were conducted with the approval of the Ethics Committees of the authors’ respective institutions. The synthesis work was approved by the Human Research Ethics Committee of the University of Monash University Human Ethics Committee (MHHREC CF10/1766-2010000910).
Participants
Investigators were brought together with the support of an international team Catalyst Grant: Primary and Community-Based Health Care from the Canadian Institutes of Health Research. Funding supported virtual and face-to-face engagement between 12 investigators. All the investigators were major contributors to primary care practice-based qualitative and quantitative studies from three countries (Australia, the USA, and Canada, including three Canadian provinces: Alberta, Ontario, and Quebec). The team comprised five academic family physicians, three sociologists, a medical anthropologist, a public health physician, and an epidemiologist. Three of the team had direct policy-making responsibilities. A total of 12 studies provided cross-jurisdictional comparisons of interventions on primary practices, practitioners, and patients. These interventions were either generated by changes in primary care policy or through controlled interventions. We drew upon published accounts and secondary reflection and analysis of primary data from each study to generate a cross-context synthesis of peer-reviewed manuscripts and additional unpublished data from 12 mixed methods studies (Table 1).
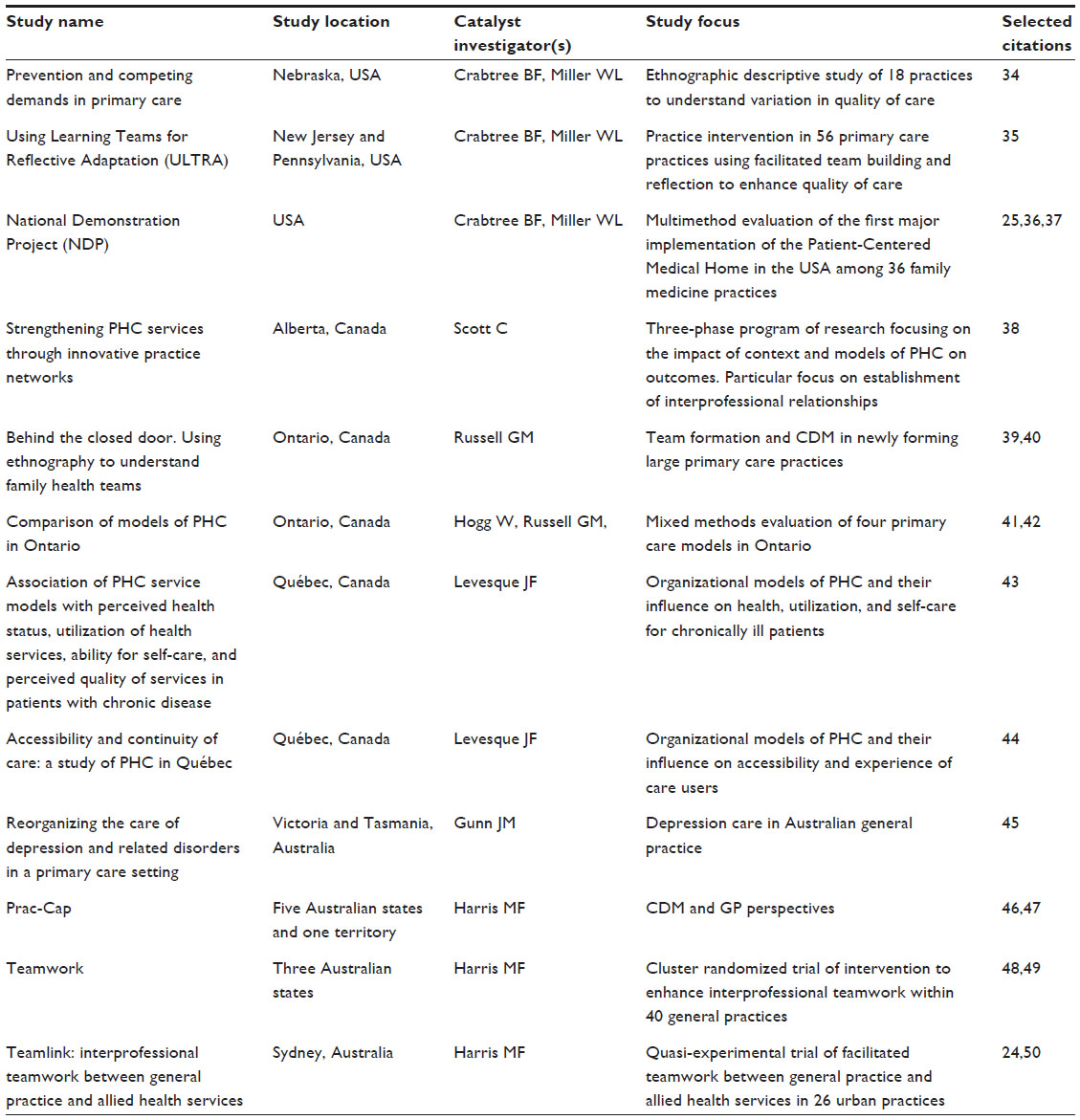 | Table 1 The studies |
Analysis
The methodology involved four stages: 1) selecting, extracting, and classifying original published studies from each participant’s program of research; 2) re-extracting and analyzing broader study materials and unpublished information from each study and program of research; 3) absorbing and reinterpreting knowledge from other studies that the investigators were aware of; and 4) reflecting and integrating insights from individual and group experiential reflections.
This iterative process of reviewing and synthesizing was accomplished using a combination of monthly teleconferences and four face-to-face retreats conducted between 2010 and 2012. The original broad aim was “To perform a synthesis of comparable studies to better understand the impact of primary health care reform on the organization, routines and relationships within primary care practices in different health care settings.”19 During the second stage, the focus shifted to a more specific question related to teamwork: “In what way do primary care reforms influence the development of teamwork in primary care practices.”
With this focus, the participants went back to the published studies and reanalyzed the data, some of which was not necessarily published previously, to gain insights into the new research question. We used matrices to thematically arrange data on the implementation of teamwork innovations from each of the different studies. A context matrix involved three main sections: the broad organization of primary care in each setting (largely based on investigator’s perceptions of the drivers of primary care reform and timing in each setting); environmental and structural factors, drawn from a published conceptual framework for understanding the influences on primary care service delivery;20 and a section related specifically to teamwork. We extracted data to inform the findings matrix through an iterative, emergent process. First, the lead investigator developed preliminary themes by grouping broad findings from a comprehensive, Ontario-based evaluation of multidisciplinary practices.17 These categories were then used as a starting point for other investigators to extract key, relevant findings from their own studies and then refined as analysis progressed (Table S1). We considered the variation in these responses according to the intensity of teamwork involved, the existing organizational culture, decision-making processes, and the size and structure of the service. We used our meetings to explore and challenge each other’s research findings and reflexively analyze how our findings were constructed.
There was variation between studies among the different jurisdictions. Thus, in our findings, we make reference to these jurisdictions (eg, Australia, USA, Alberta), although it is not necessarily the case that all the findings observed in the studies can be generalized across the whole jurisdiction (as they may not, eg, have covered all types of geographic areas).
Findings
There were major interventions and reforms implemented in all jurisdictions over the decade, which directly and indirectly aimed to enhance interprofessional teamwork (Table 2). As a result, there was evidence of changes in interprofessional processes of care both within PHC services and with health professionals outside of them. Improvements in interprofessional care processes included the following:
- Improved organization of chronic disease and preventive care (USA, Alberta, and Ontario)
- Increases in referral rates between clinicians (Australia)
- Patient-assessed quality of care (Australia)
- More frequent planned and guideline-based care for the management of chronic conditions (Australia, USA, Ontario, and Quebec).
 | Table 2 Changes to interprofessional teamwork studied in five jurisdictions |
The impacts on communication, relationships, roles, and work satisfaction were all variable within jurisdictions (Table 3).
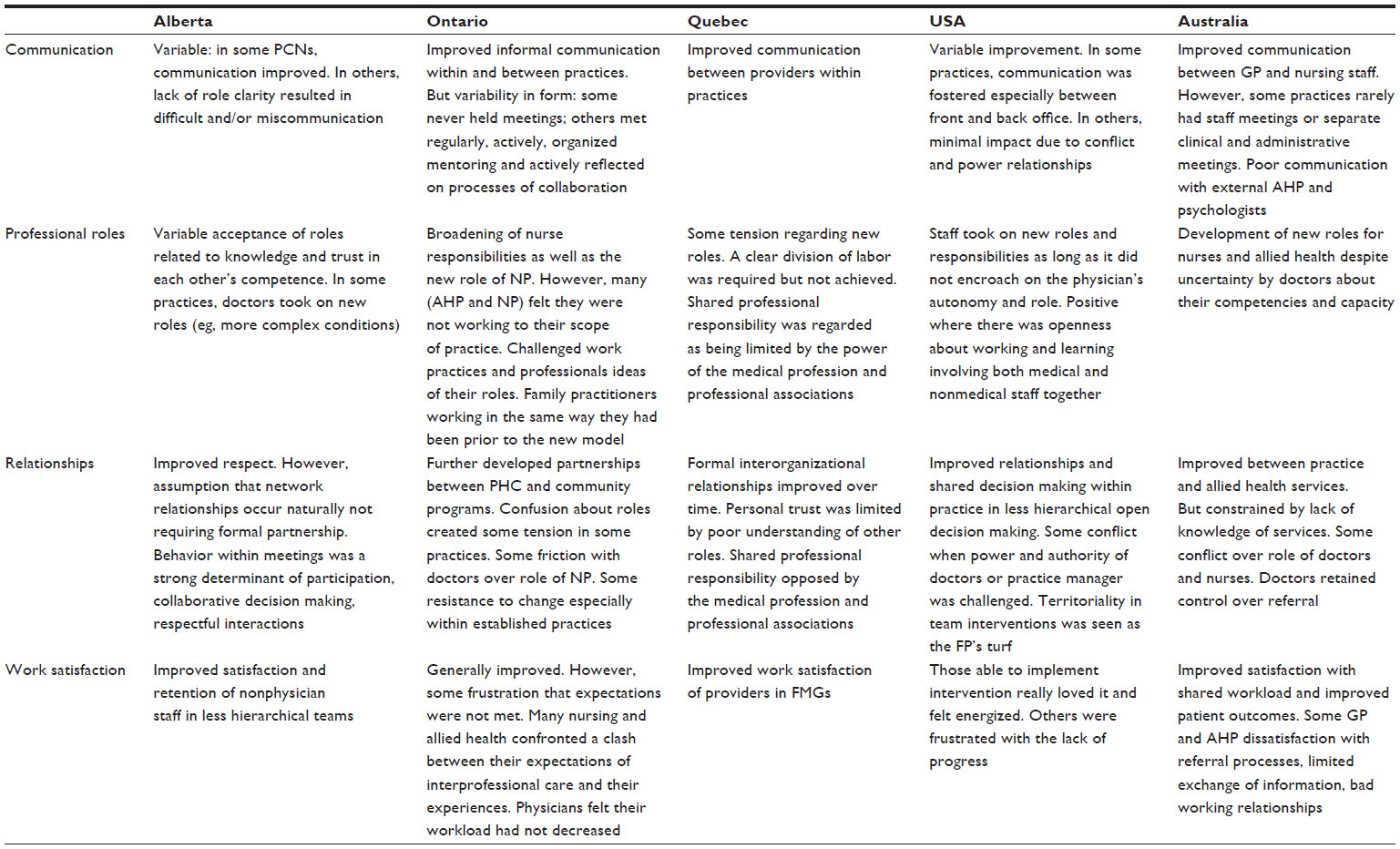 | Table 3 Impacts of interprofessional team interventions and policies on communication, relationships, roles and satisfaction of PHC providers by jurisdictions |
Impacts
Communication
Improved communication among members of the primary care practice was a universally intended objective of interprofessional team policies or interventions. However, there was considerable variation in the form and quality of communication resulting from specific interventions and policies. Some practices did not hold regular team meetings involving different practitioners and those who did sometimes encountered difficulties due to power dynamics within practices (USA, Alberta, Ontario, and Quebec). In Ontario, one family health team (FHT) never held meetings between administrative and clinical staff working in the organization, and all decisions were made by a group of FHT owners. By contrast, in other FHTs, staff met regularly, actively organized mentoring, and actively reflected on processes of collaboration.
The successful implementation of intrapractice teamwork implies bridging of the traditional communication gap between reception (front office) and clinicians (back office) to office workflow and patient flow.21 There was little consistency in the content, conduct, or timing of communication between front and back office. Much communication was informal – associated with the transfer (charting, details of next appointment, etc) or seeking of information (the best specialist to refer to, getting sign-offs on prescription renewals, new scripts, etc).
Relationships
In all jurisdictions, there were some improvements in interorganizational relationships and partnerships. The traditional loose federation of autonomous physicians was simply not consistent with the sharing and ongoing learning required for continually improving patient-centered care (USA). However, the links between primary care organizations and other community-based organizations remained weak (Ontario) except in Quebec where PHC reform was embedded in a broader reform of locally organized hospital- and community-based care networks.22
At an interprofessional level within practices, there were generally improved relationships. However, this was constrained in some practices by hierarchical decision making about roles and responsibilities and other providers’ lack of knowledge (USA, Australia, and Ontario). Physically isolated providers found it hard to integrate with their colleagues and were less able to give others an idea of their skills and potential contributions (Ontario).
At the beginning [the] GP did not entirely trust allied health professionals [dieticians] to treat the patient as he wanted them treated, so he was doing all the work himself. Now he is [referring to] dieticians and can see the value of their participation … [Nurse facilitator, Australia]23
Role change
There was adaptation to extended roles for nonphysician staff within practices across jurisdictions. In some practices, clear roles emerged and strong support for different professionals was evident.
Teamwork makes general practice sustainable. It means not everything is on the GP’s shoulders. It also means everyone in the team is valued for what they do and this engenders happiness amongst the staff. [Physician, Australia]24
However, a clear division of roles was not always achieved with some confusion about roles, which created tension in some practices (Ontario, Alberta, and Quebec). Conflict emerged as some providers felt their power was challenged (USA). This led to dissatisfaction with communication, and the processes for sharing care and changes were met with resistance, disengagement, or conflict (Australia, USA, Ontario, and Quebec).
One pharmacist said that physicians did not always understand the
value that the pharmacist can provide to their patients. They’re … very receptive to the idea of working with … a pharmacist … but it’s kind of, ‘Alright, you know we’re really glad to have you here. This is great, but what do we do with you?’ [Ontario]39
Sometimes the lead physicians, managers, or CEOs did not necessarily know the skills, knowledge, or experience possessed by other members of their team (Australia and Ontario). Other barriers to a more comprehensive scope of practice included doctors’ discomfort with what allied health professionals could do, lack of trust and lack of time to write medical directives, and change and uncertainty about their scope of practice (Australia and Ontario). Nurses seeking an expanded role were particularly frustrated with these hurdles:
There’s frustration that what we have been asked to do is … more an administrative role, in terms of filling out lab requisitions for the doctors, calling patients back with abnormal test results, and things like that. And that is not … purposeful use of our time, that … in terms of working to maximum scope, there’s lots more that we can do. [RN, Ontario]39
Change created uncertainty about what their responsibilities were and how best to respond to a new set of circumstances (Australia, Alberta, and Ontario). This situation was applied not only to clinical staff but also to administrative staff who were sometimes uncertain about what procedures they should follow especially in engaging other staff in management. For example, in some practices, there needed to be a change in practitioner routines, so that the new activities could fit into existing responsibilities and their sequencing (eg, a nurse arranging to see a patient for care planning both before and after the patient’s GP appointment) (Australia). Some identified roles that they had not previously perceived that they had. For example, reception and nursing staff played roles in triage, support, advocacy, and listening. These “shadow” team roles often went unacknowledged (Australia).
In all jurisdictions, redefinition of roles challenged the way health care providers (especially doctors) thought about their professional identity and autonomy. Adopting team care challenged some physicians who had deeply held beliefs that the role of the family physician was grounded in a strong, trusting relationship between the patient and physician. Permitting other practice staff to have meaningful patient interactions for team care meant expanding that special relationship and required an identity shift. Physicians who had deeply held beliefs about the centrality of the doctor–patient relationship found permitting other practice staff into that relationship particularly difficult as it required a shift in their identity (USA).
Readiness for change
There was evidence that although many clinicians were ready to change (prompted at least in part by a degree of work dissatisfaction), this needed to be adapted to the individual practice context and culture (Australia, USA, Alberta, and Ontario). In some practices, the changes were viewed as increasing the burden on the organization (eg, with increased paper work) and stretching capacity (eg, by increasing the workload of some health professionals) or, conversely, not drawing sufficiently upon staff to work to the full scope of their practice (Australia, USA, Alberta, Ontario, and Quebec). Practice leadership was often seen as important in facilitating readiness to change (Ontario and USA). Our findings on leadership are described later.
Work satisfaction
In all jurisdictions, there were improvements to work satisfaction where teamwork was purposefully implemented.
Doing stuff in the context of a team is so much better than trying to do it all myself. It’s just such a relief. All I can say is, everything is more doable and more enjoyable with a team. [Physician, USA]25
These improvements made attracting new staff easier and could be part of a virtuous cycle where the climate of teamwork was in turn attractive to staff who were committed to working in an interprofessional environment (Quebec). There was a complex association between changed teamwork and work satisfaction. Those staff members who were somewhat more dissatisfied with their current work situation were more ready to change their team roles, and they were more likely to actively participate in the change (Australia and Ontario).
Once teamwork innovations were introduced, this raised expectations that nonphysician roles would be extended. If these were met, work satisfaction improved. There was increased work satisfaction of nonphysician staff in less hierarchical or less physician-centric teams (Alberta), and this was associated with greater retention of nonphysician staff. However, if these expectations were not met and they were unable to extend their scope of practice, this could lead to staff member frustration and dissatisfaction. Where staff felt disempowered or not encouraged to participate in decision making, there was a higher incidence of staff feeling undervalued, underutilized, and dissatisfied (Ontario).
Influence of local factors
Variations in these impacts on practitioner communication, relationships, roles, readiness to change, and work satisfaction were mediated by a range of local contextual issues, including the type and size of practice, location and organization of teams, and leadership.
Types of practices
The influence of type of practice was complex. In Ontario, Alberta, and Quebec, different types of practices seemed to respond to teamwork in different ways. For example, Community Health Centers in Ontario, Family Medicine Groups in Quebec, and Primary Care Networks in Alberta, tended to involve other professionals in a broader scope of practice than traditional general practices, including in chronic disease management. In Australia, while larger practices were able to incorporate a broader range of health professionals in care, smaller practices found the introduction of new roles easier than larger practices:
It is really important to have open lines of communication with everybody, especially when there is more than one GP. The more people you have in your practice the more systems you need. [Practice manager, Australia]
Many interventions involved the addition of new types of employees (administrative, nursing, allied health, and social work) (Australia, Alberta, Ontario, and Quebec), which changed and complicated clinical governance and the way health professionals worked and interacted with practices, at least initially.
Colocation
Colocation facilitated getting to know one another, building trust, and establishing new practice patterns. Trust, in turn, made developing shared goals possible.
The GP gets to know allied health professionals personally. He only uses allied health professionals that he knows well. [RN, Australia]23
However, colocation itself did not always ensure effective interprofessional working relationships. In Alberta, effective communication strategies, whether face to face or virtual, were recognized as being essential if trust, respect, and common understanding were to be achieved. Without these, colocation alone did not achieve desired outcomes. For example, in other contexts, while psychologists and allied health were colocated with some practices, they were often in reality only “renting a room” and were not a “part” of the team (Australia).
Space
The organization of physical space within practices influenced the extent to which communication and shared care processes could be effectively established (Alberta and Ontario). Some practices took initial steps by creating stable physician–medical assistant teams and locating physicians and medical assistants in the same work area (USA). However, in some instances, space was used to reinforce the hierarchy already present. One example of how this happened emerged where allied health professionals were required to ask permission to use rooms that “belonged” to physicians (Ontario). In this example, allied health professionals spent much of their time seeking space to use for consultations. Space concerns were also found relating to privacy issues that were apparent in the way that physical space was organized – for example, no private space was allotted for “distressed” patients waiting for an appointment, which burdened reception staff with the need to identify this issue and attempt to “make do” within their physical space limitations (Australia).
Leadership
Leadership style set the tone for the culture of teamwork. Physician support was important in achieving and maintaining changes to team roles. Consistent and clear leadership increased resilience among individuals and the team and mediated the negativity of the challenges they experienced as they worked to develop new working relationships. In Ontario, a balance between clinical and nonclinical leadership seemed necessary to allow practices to maximize the benefits of interprofessional teamwork. A vacuum in clinical leadership left staff feeling undervalued, underutilized, and dissatisfied with the current situation.
Some teams were built on physician leads, while others developed leadership roles for other professionals. However, in most cases, the viability of programs or policies depended on physician support, at the very least. Hierarchical teams were more likely to report frustration of expectations and dissatisfaction (USA).
Discussion
Our study found considerable similarities between jurisdictions in the impacts of PHC teamwork innovations on quality and form of communication, changes to scope of practice, conflict, and work satisfaction. As others have, we found that the impacts of teamwork varied, being modified by intrapractice contextual factors including practice model, colocation of services, leadership style, and space.26,27 Our multijurisdictional comparison showed how the differences within the jurisdictions studied were often greater than those existing between jurisdictions. Although the extent of intrajurisdictional variation has been documented in some cross-national comparative surveys, our methods allowed us to understand the origin of this variability.28
Teamwork innovations can promote better communication, better relationships, and greater satisfaction of the workforce. However, they can also contribute to conflict if professionals have poor understanding of each other’s roles.12 Roles need to be clearly articulated and negotiated if team innovations are to have the desired effects.29
Some practitioners were challenged by changes in roles – relating to skills and capacities of staff and confusion over work practices (such as what to do with patients when they present to reception staff). However, role boundaries and power and autonomy were the key factors. In particular, teamwork challenged the autonomy and decision making of physicians, especially in the USA. Staff in hierarchical, physician-centric practices tended to respond most negatively. The influence of hierarchy and professional power on linkages between general practices and other providers have been previously described in Australian, Canadian, and UK general practice.30–32
Staff in services where practitioners were able to develop confidence in each other’s roles and in which roles and tasks could be assigned on the basis of skill and capacity rather than power responded more positively. The development of interprofessional teamwork required clinical leadership that was both able to make decisions (physician support was important here) and empowered all staff members to collaborate and develop flexible roles. This was especially important in the management of chronic illness in PHC.33
In some cases, the interventions or reforms examined here had a focus on teamwork, but not all studies did. Collaborative synthesis allowed investigators to reanalyze data from completed studies that had already been published and look at that data through a new lens, in this case teamwork. Original findings from these studies were not revised; instead, new insights were developed through reanalysis of the data against similar studies from other jurisdictions. While any one study may have concluded an impact of teamwork, the strength of this study is through the comparison across contexts.
There are a number of limitations to this study. The studies in this synthesis were conducted throughout the first decade of this century covering most of the significant innovations in teamwork in primary care across three countries during this period. However, there were other changes and they built on changes in the previous decade. Furthermore, our synthesis integrated findings from studies that were conducted at various stages of these reforms. The reforms and interventions evaluated in these studies were variable, ranging from discrete interventions to naturalistic evaluations of the introduction of new policies within a jurisdiction. In addition, these impacts were observed in only a sample of practices in each jurisdiction. It should be noted that the methodology described here is innovative and not yet tested more broadly. However, it builds on established methods and adds to them the important element of reflexivity, an essential and established element of all qualitative research and often lacking from other approaches that combine findings from published research. Experienced researchers who are thoroughly knowledgeable about their own work might benefit from this interactive process for systematic reflection and synthesis. The strength of this study is that we now better understand the impact of teamwork reforms across jurisdictions. These should incorporate the patient viewpoint, which most of these studies only addressed in a minor way.
Conclusion
Key findings were that although the impacts of the reforms and interventions designed to enhance interprofessional teamwork were generally positive, they did vary under the influence of professional and organizational contexts, especially, the model of practice. However, differences in impact were greater within than between jurisdictions. Leadership hierarchies and lack of knowledge of other team members’ roles challenged the adoption of new configurations of team-based practice. To avoid negative impacts and achieve their desired goals, policy makers need to be aware of the complexity of the PHC context into which reforms are introduced and the consequent variation in impacts and responses. This leads to some important implications. First, leadership at the practice level matters with collaborative decision making about roles needing to be facilitated rather than being expected to emerge. Second, some flexibility for local adaptation is needed with mechanisms established to monitor the impacts across different contexts and models of practice.
Acknowledgments
This study was funded by a Catalyst Grant from the Canadian Institutes of Health Research (Grant No 212271). Dr Crabtree’s time was supported in part by a Senior Investigator Award from the National Cancer Institute (K05 CA140237). Dr Levesque was supported through a career award Chercheur-boursier clinicien – junior 1 from the Fonds recherche Québec – Sante (FRQ-S).
Author contributions
Mark F Harris and Jenny Advocat contributed to the conception, analysis, and interpretation of the data and drafting and revision of the manuscript. Benjamin F Crabtree, Jean-Frederic Levesque, William L Miller, Jane M Gunn, William Hogg (co-chief investigator), Cathie M Scott, Sabrina M Chase, and Lisa Halma contributed to the conception, analysis, and interpretation of the data and critical revision of the manuscript.
Grant M Russell was co-chief investigator, coordinated the project, and contributed to the conception, analysis, and interpretation of the data and critical revision of the manuscript. All authors have given final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure
The authors declare no conflicts of interest.
References
Grumbach K, Bodenheimer T. Can health care teams improve primary care practice? JAMA. 2004;291(10):1246–1251. | |
Bodenheimer T, Ghorob A, Willard-Grace R, et al. The 10 building blocks of high-performing primary care. Ann Fam Med. 2014;12(2):166–171. | |
Wagner EH, Austin BT, Von Korff M. Organizing care for patients with chronic illness. Milbank Q. 1996;74(4):511–544. | |
Nutting PA, Crabtree BF, Miller WL, et al. Transforming physician practices to patient-centered medical homes: lessons from the National Demonstration Project. Health Aff. 2011;30(3):439–445. | |
Renders C, Valk G, Griffin S, et al. Interventions to improve the management of diabetes in primary care, outpatient, and community settings. Diabetes Care. 2001;24(10):1821–1833. | |
de Sonnaville JJ, Bouma M, Colly LP, et al. Sustained good glycaemic control in NIDDM patients by implementation of structured care in general practice: 2-year follow-up study. Diabetologia. 1997;40(11):1334–1340. | |
Temkin-Greener H, Gross D, Kunitz SJ, et al. Measuring interdisciplinary team performance in a long-term care setting. Med Care. 2004;42(5):472–481. | |
Mickan SM, Rodger SA. Effective health care teams: a model of six characteristics developed from shared perceptions. J Interprof Care. 2005;19(4):358–370. | |
Mickan SM. Evaluating the effectiveness of health care teams. Aust Health Rev. 2005;29(2):211–217. | |
Harris M, Proudfoot J, Jayasinghe U, et al. The job satisfaction of general practice staff and the team environment. Med J Aust. 2007;186:570–572. | |
Schoen C, Osborn R, Doty MM, et al. A survey of primary care physicians in eleven countries, 2009: perspectives on care, costs, and experiences. Health Aff (Millwood). 2009;28(6):w1171–w1183. | |
Xyrichis A, Lowton K. What fosters or prevents interprofessional teamworking in primary and community care? A literature review. Int J Nurs Stud. 2008;45(1):140–153. | |
Crabtree B, Miller W, Gunn J, et al. Uncovering the Wisdom Hidden Between the Lines: The Collaborative Reflexive Deliberative Approach. 2015. [Under Review]. | |
Baum F, MacDougall C, Smith D. Participatory action research. J Epidemiol Community Health. 2006;60(10):854–857. | |
Barnett-Page E, Thomas J. Methods for the synthesis of qualitative research: a critical review. BMC Med Res Methodol. 2009;9:59. | |
Pawson R, Greenhalgh T, Harvey G, et al. Realist review – a new method of systematic review designed for complex policy interventions. J Health Serv Res Policy. 2005;10(Suppl 1):21–34. | |
Greenhalgh T, Robert G, Macfarlane F, et al. Storylines of research in diffusion of innovation: a meta-narrative approach to systematic review. Soc Sci Med. 2005;61(2):417–430. | |
Scott RW. Organizations: Rational, Natural, and Open Systems. Upper Saddle River: Prentice Hall; 2003. | |
Hogg W, Russell G, Crabtree B, et al. Shifting Ground, Common Ground – Understanding the Evolving Primary Care Practice. Canadian Institutes of Health Research Catalyst Grant. Sydney, NSW: Primary and Community-Based Healthcare; 2010–2011. | |
Hogg W, Rowan M, Russell G, et al. Framework for primary care organizations: the importance of a structural domain. Int J Qual Health Care. 2008;20(5):308–313. | |
Crabtree B, McDaniel R, Nutting P, et al. Closing the physician-staff divide: a step toward creating the medical home. Fam Pract Manag. 2008;15:20–24. | |
Breton M, Pineault R, Levesque JF, et al. Reforming healthcare systems on a locally integrated basis: is there a potential for increasing collaborations in primary healthcare? BMC Health Serv Res. 2013; 8(13):262. | |
Chan B, Proudfoot J, Zwar N, et al. Satisfaction with referral relationships between general practice and allied health professionals in Australian primary health care. Aust J Prim Health. 2011;17(3):250–258. | |
Chan BC, Perkins D, Wan Q, et al. Finding common ground? Evaluating an intervention to improve teamwork among primary health-care professionals. Int J Qual Health Care. 2010;22(6):519–524. | |
Nutting PA, Crabtree BF, Miller WL, et al. Journey to the patient-centered medical home: a qualitative analysis of the experiences of practices in the National Demonstration Project. Ann Fam Med. 2010;8(Suppl 1):S45–S56; S92. | |
Sicotte C, D’Amour D, Moreault MP. Interdisciplinary collaboration within Quebec Community Health Care Centres. Soc Sci Med. 2002; 55(6):991–1003. | |
Swerissen H, Macmillan J, Biuso C, et al. Community health and general practice: the impact of different cultures on the integration of primary health care. Aust J Prim Health. 2001;7(1):65–70. | |
Osborn R, Moulds D, Squires D, et al. International survey of older adults finds shortcomings in access, coordination, and patient-centered care. Health Aff. 2014;33(12):2247–2255. | |
Mitchell G, Tieman J, Shelby-James T. Multidisciplinary care planning and teamwork in primary care. Med J Aust. 2008;188(8):S61–S64. | |
McDonald J, Jayasuriya R, Harris M. The influence of power dynamics and trust on multidisciplinary collaboration: a qualitative case study of type 2 diabetes mellitus. BMC Health Serv Res. 2012;12(1):63. | |
Charles-Jones H, Latimer J, May C. Transforming general practice: the redistribution of medical work in primary care. Sociol Health Illn. 2003;25(1):71–92. | |
Gaboury I, Bujold M, Boon H, et al. Interprofessional collaboration within Canadian integrative healthcare clinics: key components. Soc Sci Med. 2009;69(5):707–715. | |
Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness: the chronic care model, part 2. JAMA. 2002;288(15):1909–1914. | |
Crabtree BF, Miller WL, Tallia AF, et al. Delivery of clinical preventive services in family medicine offices. Annals of family medicine. 2005;3(5):430–435. | |
Balasubramanian BA, Chase SM, Nutting PA, et al. Using Learning Teams for Reflective Adaptation (ULTRA): insights from a team-based change management strategy in primary care. Annals of family medicine. 2010;8(5):425–432. | |
Nutting PA, Crabtree BF, Stewart EE, et al. Effect of facilitation on practice outcomes in the National Demonstration Project model of the patient-centered medical home. Annals of family medicine. 2010;8 Suppl 1:S33–S44; s92. | |
Nutting PA, Miller WL, Crabtree BF, Jaen CR, Stewart EE, Stange KC. Initial lessons from the first national demonstration project on practice transformation to a patient-centered medical home. Annals of family medicine. 2009;7(3):254–260. | |
Scott C, Hofmeyer A. Networks and social capital: a relational approach to primary healthcare reform. Health Res Policy Syst. 2007;5:9. | |
Russell G, Geneau R, Farrell B. Behind the Closed Door: Using Ethnography to Understand Family Health Teams (FHT) Phase II Toronto, ON: Ministry of Health and Long-term Care, 2009. | |
Russell G, Advocat J, Geneau R, Farrell B, Thille P, Ward N, Evans S. Examining organizational change in primary care practices: experiences from using ethnographic methods. Fam Pract. 2012;29(4):455–461. | |
Russell G, Dahrouge S, Tuna M, Hogg W, Geneau R, Gebremichael G. Getting it all done. Organizational factors linked with comprehensive primary care. Family practice. 2010;27(5):535–541. | |
Russell GM, Dahrouge S, Hogg W, Geneau R, Muldoon L, Tuna M. Managing chronic disease in ontario primary care: the impact of organizational factors. Annals of family medicine. 2009;7(4):309–318. | |
Levesque JF, Feldman DE, Lemieux V, Tourigny A, Lavoie JP, Tousignant P. Variations in patients’ assessment of chronic illness care across organizational models of primary health care: a multilevel cohort analysis. Healthc Policy. 2012;8(2):e108–123. | |
Pineault R, Levesque JF, Roberge D, Hamel M, Lamarche P, Haggerty J. Accessibility and continuity of care: a study of primary healthcare in Québec. Québec; 2009. Available from: https://www.inspq.qc.ca/pdf/publications/813_ResumeServicesPremLigneAng.pdf. Accessed December 31, 2015. | |
Gunn JM, Palmer VJ, Dowrick CF, et al. Embedding effective depression care: using theory for primary care organisational and systems change. Implement Sci. 2010;5:62. | |
Oldroyd J, Proudfoot J, Infante FA, et al. Providing healthcare for people with chronic illness: the views of Australian GPs. Medical J Aust. 2003;179(1):30–33. | |
Proudfoot J, Infante F, Holton C, et al. Organisational capacity and chronic disease care: an Australian general practice perspective. Aust Fam Physician. 2007;36(4):286–288. | |
Harris MF, Jayasinghe UW, Taggart JR, et al. Multidisciplinary Team Care Plans in the management of patients with chronic disease in Australian general practice. Med J Aust. 2011;194(5):236–239. | |
Christl B, Harris MF, Jayasinghe UW, et al. Readiness for organisational change among general practice staff. Qual Saf Health Care. 2010;19(5):e12. | |
Harris MF, Chan BC, Daniel C, Wan Q, Zwar N, Davies GP. Development and early experience from an intervention to facilitate teamwork between general practices and allied health providers: the Team-link study. BMC Health Serv Res. 2010;10:104. |
Supplementary material
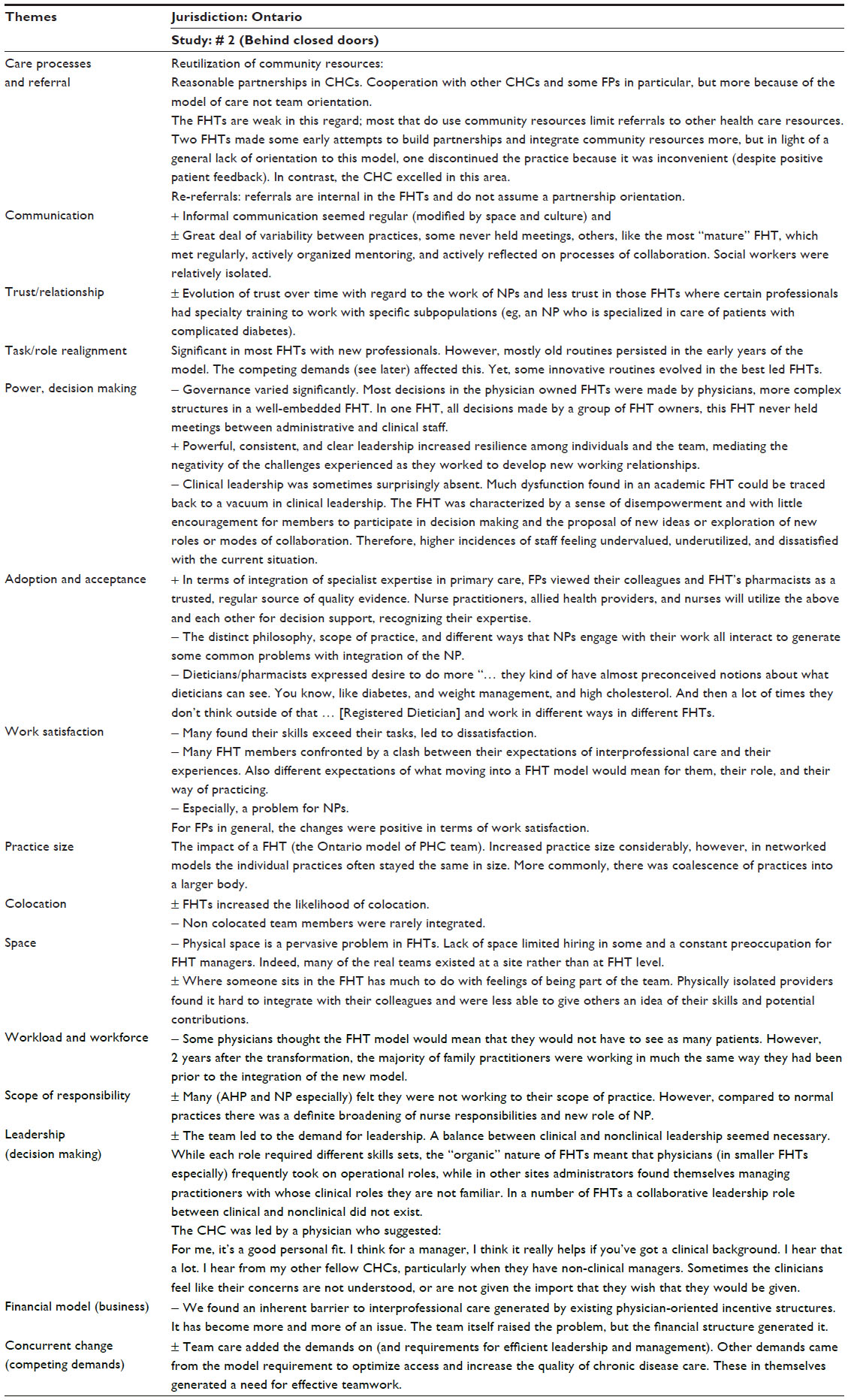 | Table S1 Example of summary matrix used to compare impacts across studies and jurisdictions |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.