Back to Journals » Clinical Ophthalmology » Volume 20
Interocular Axial Length Asymmetry and Postoperative Refractive Error After Bilateral Cataract Surgery: A Retrospective Comparative Study
Authors Ouchi M, Takehara C
Received 27 February 2026
Accepted for publication 20 May 2026
Published 18 June 2026 Volume 2026:20 603474
DOI https://doi.org/10.2147/OPTH.S603474
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Bharat Gurnani
Masayuki Ouchi, Chika Takehara
Department of Ophthalmology, Masayuki Ouchi Eye Clinic, Kyoto, Japan
Correspondence: Masayuki Ouchi, Department of Ophthalmology, Masayuki Ouchi Eye Clinic, 9 Nishikujo Ohkuni-cho, Minami-ku, Kyoto, 601-8449, Japan, Email [email protected]
Purpose: To evaluate whether interocular axial length (AL) asymmetry is associated with postoperative refractive error, independent of absolute AL.
Patients and Methods: This retrospective comparative study included 42 patients (84 eyes) who underwent bilateral cataract surgery. Within-patient comparisons were performed between longer-AL and shorter-AL eyes, and longer-AL eyes were also compared with an AL-matched control group. Postoperative spherical equivalent (SE) at 1 month was compared with predicted SE using the Barrett Universal II and SRK/T formulas. Multivariable regression analysis was performed.
Results: Mean postoperative refractive error (mean ± SD) was − 0.20 ± 0.63 D in the longer-AL group vs 0.02 ± 0.50 D in the shorter-AL group (BU, p = 0.01), and − 0.41 ± 0.84 D vs − 0.05 ± 0.53 D (SRK/T, p = 0.02). Longer-AL eyes showed a significantly greater myopic shift than shorter-AL and control eyes. Interocular AL difference remained independently associated with postoperative refractive error.
Conclusion: Interocular AL asymmetry was associated with postoperative myopic shift, even after adjustment for axial length and other covariates.
Keywords: asymmetry, postoperative refractive error, Barrett Universal II, SRK/T
Introduction
Advances in ocular biometry and intraocular lens (IOL) power calculation formulas have substantially improved the accuracy of refractive outcomes after cataract surgery. The Barrett Universal II (BU) formula demonstrates high predictive accuracy;1–3 however, its performance may be less reliable in eyes with atypical geometry, such as those with long or short axial lengths (ALs).4 Even among eyes with comparable ALs, refractive prediction errors are more likely to occur when ocular dimensions are disproportionate, particularly when the ratio between the AL and the corneal curvature radius is mismatched.5,6 In cases of interocular differences in AL, the proportional relationships between the ocular components may differ between eyes, suggesting that such cases cannot necessarily be managed in the same manner as those with symmetrical ALs. However, previous studies have primarily focused on the effect of absolute axial length,4 and the impact of interocular asymmetry itself has not been fully investigated.
Therefore, in this study, we investigated the postoperative refractive error in cataract surgery cases involving interocular differences in AL.
Materials and Methods
This retrospective study included 42 patients (84 eyes) who underwent bilateral cataract surgery with an interocular AL difference of ≥0.5 mm. Patients with ocular comorbidities including posterior staphyloma or intraoperative complications were excluded. All surgeries were performed by a single surgeon using a 2.4-mm clear corneal incision, phacoemulsification, and in-the-bag IOL implantation.
The same IOL model was implanted in both eyes of each patient. The IOL models used were as follows: CNA0T0 (Alcon) in 8 cases (16 eyes), AU00T0 (Alcon) in 18 cases (36 eyes), ZCB00V (J&J Vision) in 9 cases (18 eyes), XC-1 and YA-BBR (HOYA) in 4 cases (8 eyes), and W-60R (Santen) in 3 cases (6 eyes).
Biometric Measurements
Ocular biometry, including AL, keratometry, and anterior chamber depth, was performed twice using IOLMaster 700 (Carl Zeiss Meditec AG), with the second measurement used for analysis. Measurements were performed by three trained examiners in a random manner. Each parameter was measured twice, and a third measurement was obtained only when a discrepancy was observed between the initial two measurements.
For each patient, the eye with the longer AL was classified into the longer-AL group, and the shorter eye was classified into the shorter-AL group. In addition, a control group comprising 42 consecutive eyes whose age and AL values fell within the mean ± 2 SD range of the longer-AL group from patients who underwent cataract surgery at our clinic between January 2022 and December 2023 was included for comparison. These cases were matched based on age and AL within two standard deviations of the mean AL in the longer-AL group. Postoperative refractive errors in the control group were compared with those in the previously defined longer-AL group.
Intraocular Lens Calculation
IOL power was calculated using the Barrett Universal II formula. Except for a limited number of cases, the target refraction was set at emmetropia for the shorter-AL group and between −2.5 and −3.0 D for the longer-AL group.
The selection of the IOL model was based on standard clinical practice, taking into account surgical conditions such as eyelid anatomy, lens nucleus hardness, and maximum pupil dilation, as well as surgeon preference.
Outcome Measurements
Visual acuity was measured using a Space-Saving Chart (SSC-370; NIDEK Co., Ltd). Objective refraction was initially obtained using an autorefractor keratometer (ARK-1; NIDEK Co., Ltd.) and subsequently refined by subjective manifest refraction. Predicted postoperative refraction was calculated using the BU and SRK/T formulas. The postoperative refractive error was defined as the difference between the postoperative subjective spherical equivalent (SE) at 1 month and the predicted SE (negative values indicating a myopic shift).
Statistical Analyses
Statistical analyses were performed using R software. To account for potential inter-eye correlation,comparisons between longer-AL and shorter-AL eyes were performed using the Wilcoxon signed-rank test, whereas comparisons between longer-AL and control eyes were performed using the Mann–Whitney U-test. In addition, multivariate linear regression analysis was performed to evaluate factors associated with postoperative refractive error. The dependent variable was postoperative refractive error, and the independent variables included axial length, interocular axial length difference, keratometry, anterior chamber depth, age and a binary variable indicating longer-AL eyes. Subgroup analyses were also conducted based on axial length (eg, AL < 26 mm vs ≥ 26 mm).A p-value < 0.05 was considered statistically significant.
This study was a retrospective observational study based on existing clinical data obtained during routine cataract surgery. It did not constitute a clinical trial, did not involve investigational drugs or medical devices, and was not conducted for regulatory approval purposes. No additional interventions or procedures were performed for research purposes, and no additional risks were imposed on the patients.
The study protocol was reviewed and approved by the Ethics Committee of Masayuki Ouchi Eye Clinic, Kyoto, Japan (Approval No. 10). The study adhered to the tenets of the Declaration of Helsinki.
Written informed consent for the use of anonymized clinical data for research purposes was obtained from all patients prior to surgery. Due to the retrospective nature of the study, the requirement for additional informed consent was waived by the ethics committee.
Results
Table 1 summarizes the preoperative demographic characteristics of the three groups, and Figure 1 illustrates the AL distributions. The mean AL was 25.79 ± 2.02 mm (range: 22.06–30.59 mm) in the longer-AL group, 24.65 ± 1.75 mm (range: 20.69–29.37 mm) in the shorter-AL group, and 26.04 ± 1.97 mm (range: 22.56–30.82 mm) in the control group. Postoperative uncorrected distance visual acuity (UDVA) was significantly better in the longer-AL group than in the shorter-AL group (0.91 ± 0.24 vs 0.23 ± 0.34, p < 0.001), whereas no significant difference was observed in best-corrected distance visual acuity (CDVA) between the two groups (−0.00 ± 0.23 vs 0.01 ± 0.18, p = 0.74).
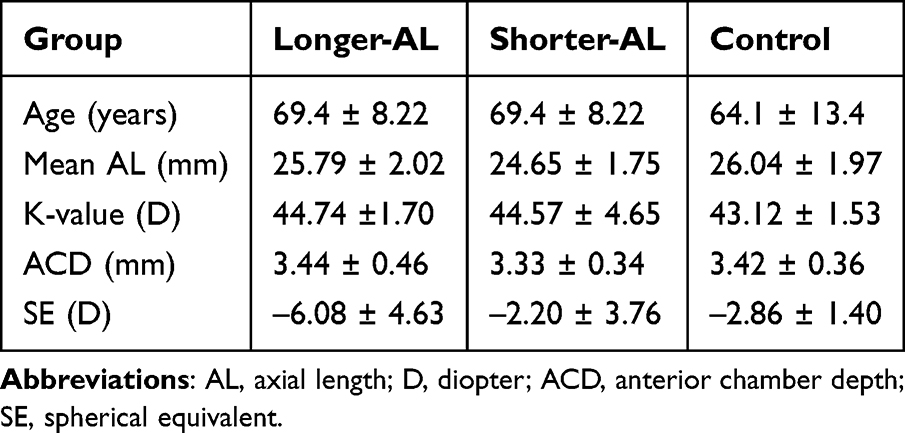 |
Table 1 Baseline Ocular Characteristics (Mean ± Standard Deviation) by Group |
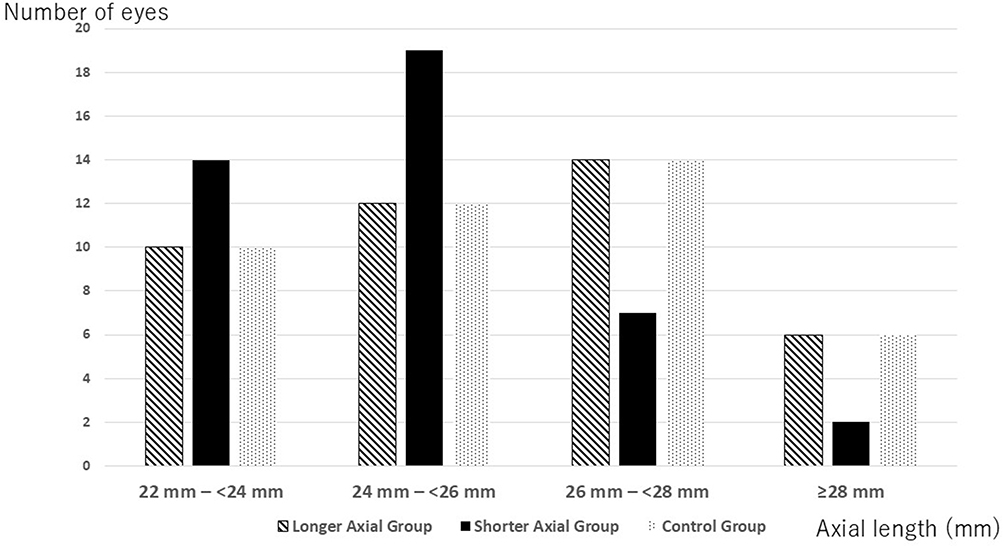 |
Figure 1 Distribution of axial length (AL) in longer-AL, shorter-AL, and control groups. |
The predicted postoperative refractions were as follows: BU formula: −3.04 ± 1.21 D (longer-AL group) and −0.73 ± 1.17 D (shorter-AL group); SRK/T formula: −2.84 ± 1.10 D (longer-AL group) and −0.65 ± 1.02 D (shorter-AL group). The actual postoperative subjective spherical equivalents (SEs) were −3.26 ± 1.49 D in the longer-AL group and −0.71 ± 1.26 D in the shorter-AL group (Table 2). The postoperative refractive errors were as follows: BU formula: −0.20 ± 0.63 D (longer-AL group) and 0.02 ± 0.50 D (shorter-AL group); SRK/T formula: −0.41 ± 0.84 D (longer-AL group) and −0.05 ± 0.53 D (shorter-AL group). For both formulas, the longer-AL group exhibited a significantly greater myopic deviation (p = 0.009 and 0.02, respectively; Figure 2).
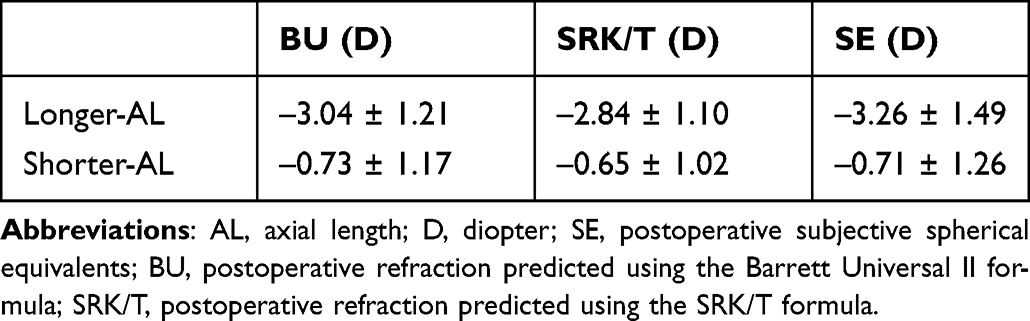 |
Table 2 Predicted vs. Postoperative SE and Refractive Error (Mean ± Standard Deviation) |
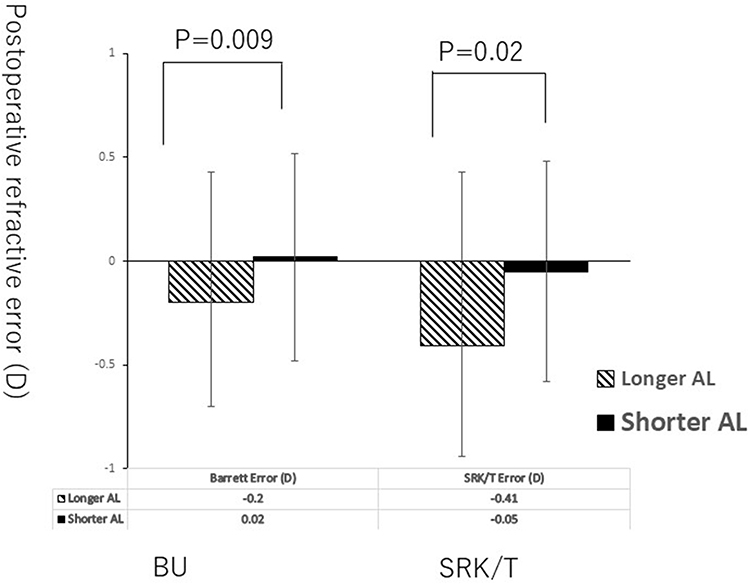 |
Figure 2 Comparison of postoperative refractive errors between longer-AL and shorter-AL eyes. Abbreviations: AL, Axial Length; BU, Barrett Universal II formula. |
We further investigated this issue by dividing the 42 cases into two subgroups according to whether the longer-AL eye had an axial length of ≥26 mm (over26 group, 23 pairs) or <26 mm (under26 group, 19 pairs).
In the over26 group, the postoperative refractive error calculated using the Barrett formula was -0.29 ± 0.43 D in longer-AL eyes and 0.05 ± 0.15 D in shorter-AL eyes (p = 0.005). Using the SRK/T formula, the corresponding values were −0.47 ± 0.95 D and −0.04 ± 0.41 D, respectively (p = 0.05). In both formulas, longer-AL eyes demonstrated a significantly greater myopic shift.
Furthermore, in the under26 group, the postoperative refractive error calculated using the Barrett formula was −0.18 ± 0.52 D in longer-AL eyes and 0.17 ± 0.43 D in shorter-AL eyes (p = 0.06). Using the SRK/T formula, the corresponding values were −0.24 ± 0.49 D and 0.21 ± 0.38 D, respectively (p < 0.001), again demonstrating a myopic shift in longer-AL eyes.
The absolute refractive errors were 0.51 D in the longer-AL group and 0.37 D in the shorter-AL group when using the BU formula, and 0.64 D and 0.39 D, respectively, when using the SRK/T formula. No statistically significant differences were observed in absolute error between the two groups (p = 0.89 and 0.69, respectively; Figure 3).
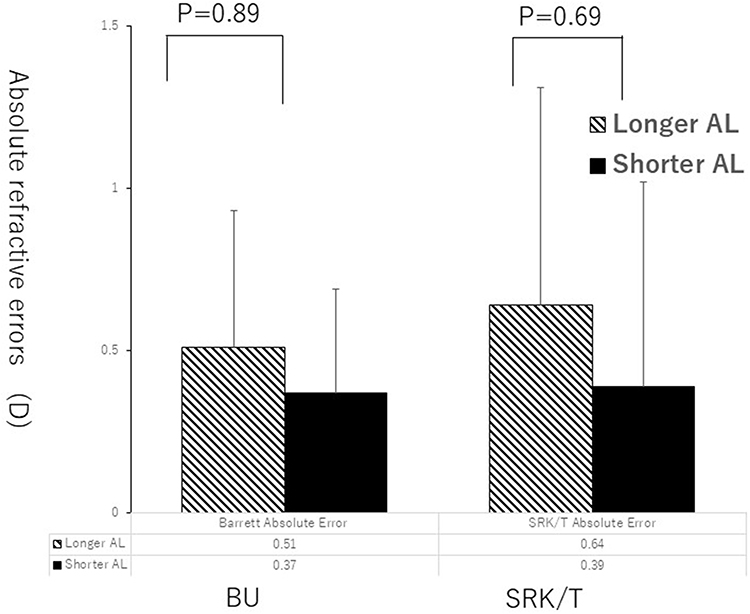 |
Figure 3 Comparison of absolute refractive errors between longer-AL and shorter-AL eyes. Abbreviations: AL, Axial Length; BU, Barrett Universal II formula. |
In contrast, when comparing the postoperative refractive errors between the longer-AL group and control group, the BU formula yielded −0.20 ± 0.63 D for the longer-AL group and 0.07 ± 0.28 D for the control group. Using the SRK/T formula, the values were −0.41 ± 0.84 D and 0.13 ± 0.29 D, respectively. In both formulas, the longer-AL group demonstrated significantly greater myopic deviation than the control group (p = 0.02 and 0.009, respectively; Figure 4).
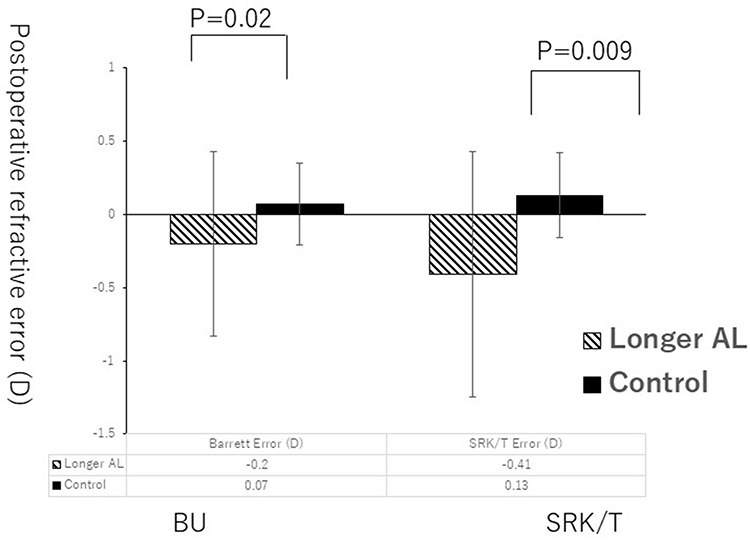 |
Figure 4 Comparison of postoperative refractive error between longer-AL and control eyes. Abbreviations: AL, Axial Length; BU, Barrett Universal II formula. |
Multivariate regression analysis demonstrated that both axial length (β = −2.12, p < 0.001) and interocular axial length difference (β = −1.18, p < 0.001) were independently associated with postoperative refractive error. Keratometry was also significantly associated with refractive error (β = −1.05, p = 0.045), whereas anterior chamber depth and age and the binary variable indicating longer-AL eyes (β = −0.18, p = 0.094) were not significant predictors (Table 3).
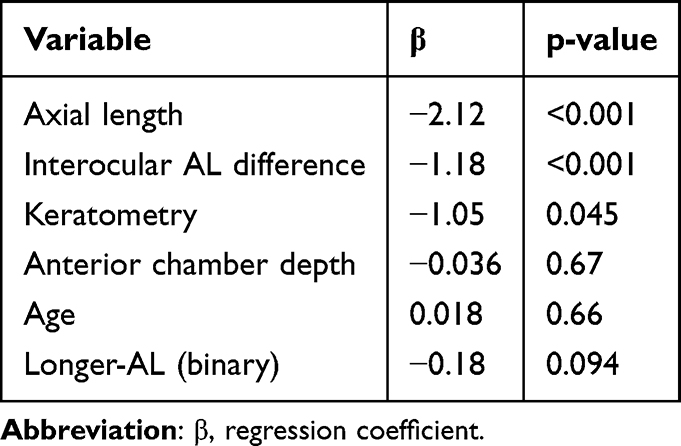 |
Table 3 Multivariate Regression Analysis of Factors Associated with Postoperative Refractive Error |
Discussion
The present study suggests that interocular axial length asymmetry is associated with increased postoperative refractive prediction error. The longer eye is more likely to exhibit a greater myopic postoperative refractive error than the shorter eye and AL-matched eyes without interocular asymmetry. Importantly, multivariate regression analysis demonstrated that interocular axial length difference remained a significant predictor of postoperative refractive error even after adjusting for axial length and other covariates.
Although axial length showed the strongest association, interocular asymmetry emerged as a clinically relevant factor, highlighting the importance of considering bilateral ocular geometry when predicting refractive outcomes.
The BU formula generally performs well across a broad range of ALs; however, its accuracy may decrease in extremely long or short eyes or in eyes with atypical ocular proportions.4–6
In recent years, newer-generation intraocular lens power calculation formulas, such as the Kane formula7 and Hill-RBF8 method, have demonstrated improved refractive accuracy across a wide range of axial lengths, including relatively short and long eyes. However, to our knowledge, no previous studies have specifically investigated intra-individual interocular differences in postoperative refractive error in cases with axial length asymmetry. Therefore, the present study addresses a clinically relevant yet underexplored aspect of refractive predictability.
Accordingly, in the present study, we focused on eyes exhibiting an interocular AL difference and compared the refractive prediction errors between eyes with longer- and shorter-ALs within the same patient, as well as between eyes from patients without an interocular AL discrepancy. The threshold was selected based on clinical relevance and previous studies. In eyes with a normal axial length, a 1-mm difference in axial length generally corresponds to approximately 3 D of refractive difference, and relatively small interocular refractive differences are generally considered less likely to cause clinically significant binocular disturbance or aniseikonia.
Therefore, a cutoff value of 0.5 mm was considered clinically meaningful. In addition, smaller differences may fall within the range of measurement variability.
Previous studies reported conflicting tendencies in refractive error prediction for long eyes when using the BU formula. Iijima et al observed a mean error of 0.04 ± 0.42 D in eyes with an average AL of 24.05 mm, suggesting a slight hyperopic shift,7 and other reports have similarly described hyperopic outcomes in long eyes.9,10 In contrast, several studies have identified AL as a significant factor associated with refractive prediction errors using various formulae, indicating that longer eyes may be more prone to myopic shifts.11
In our study, the longer eye consistently showed myopic shift, whereas the shorter eye demonstrated minimal deviation from the predicted refraction. This pattern aligns with previous reports suggesting that overcompensation in lens factor optimization in the BU formula or inaccuracies in effective lens position estimation in eyes with a long AL may result in mild myopic bias.12 In contrast, although the purpose of this study was to investigate the pattern of postoperative refractive prediction errors in eyes with an interocular AL difference, focusing solely on the findings shown in Figure 2, that is, the longer-AL group exhibited greater refractive error than the shorter-AL group, may merely reflect the well-known phenomenon that long eyes generally have lower refractive prediction accuracy. To characterize the unique features of eyes more accurately with an interocular AL discrepancy, we extracted an additional control group composed of eyes without an interocular difference in AL, but with an AL distribution identical to that of the longer-AL group, and compared these eyes with those in the longer-AL group. Interestingly, even when eyes with longer-ALs were compared to an age- and AL-matched control group without interocular asymmetry, they demonstrated a significantly greater myopic prediction error.
Importantly, this association appears to be independent of absolute axial length, although the underlying mechanisms remain unclear. One possible explanation is that asymmetry in axial length may reflect subtle interocular differences in other biometric parameters, such as effective lens position (ELP), anterior chamber depth, or corneal curvature.
However, several limitations should be considered. First, the retrospective design introduces potential selection bias. Second,sample number was relatively small and the follow-up period was limited to 1 month, and longer-term refractive stability was not evaluated. Nevertheless, previous studies, including a systematic review and clinical studies, have reported that postoperative refraction generally stabilizes within the first postoperative month, with minimal changes after the early postoperative period. Therefore, the use of 1-month postoperative data in the present study appears clinically reasonable.13–16 Third, the use of different IOL models may have influenced refractive outcomes and represents a limitation. Fourth, a formal power analysis was not performed due to the retrospective design, which is acknowledged as a limitation. Finally, as only the Barrett Universal II and SRK/T formulas were used, the generalizability of the findings to newer formulas such as the Kane formula may be limited.
Additionally, although multivariable analysis was performed, residual confounding cannot be completely excluded. The inclusion of eyes with overlapping axial length ranges between groups may also have influenced the results.
Therefore, the findings of this study should be interpreted as demonstrating an association rather than a causal relationship. Further prospective studies with larger sample sizes and longer follow-up are warranted to confirm these findings.
Despite these limitations, this study highlights a clinically relevant concept: interocular axial length asymmetry may be an additional factor to consider when predicting refractive outcomes following cataract surgery.
Conclusion
Eyes with interocular AL differences ≥0.5 mm are at a higher risk of myopic postoperative refractive error in the longer eye. Awareness of this tendency is important for optimizing IOL power selection and improving postoperative refractive outcomes and patient satisfaction.
These findings suggest that interocular asymmetry should be considered as an additional factor when predicting postoperative refractive outcomes.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Melles RB, Holladay JT, Chang WJ. Accuracy of intraocular lens calculation formulas. Ophthalmology. 2018;125:169–8. doi:10.1016/j.ophtha.2017.08.027
2. Cooke DL, Cooke TL. Comparison of 9 intraocular lens power calculation formulas. J Cataract Refract Surg. 2016;42:1157–1164. doi:10.1016/j.jcrs.2016.06.029
3. Kane JX, Van Heerden A, Atik A, Petsoglou C. Intraocular lens power formula accuracy: comparison of 7 formulas. J Cataract Refract Surg. 2016;42:1490–1500. doi:10.1016/j.jcrs.2016.07.021
4. Mo E, Chen Z, Feng K, Yang F, Li J, Zhao YE. Accuracy of seven modern online IOL formulas in eyes with axial lengths longer than 30 mm. J Refract Surg. 2023;39:705–710. doi:10.3928/1081597X-20230831-03
5. Ma S, Li C, Sun J, et al. Comparative analysis of eighteen IOL power calculation formulas using a modified formula performance index across diverse biometric parameters. Am J Ophthalmol. 2025;273:221–230. doi:10.1016/j.ajo.2025.02.035
6. Mori Y, Minami K, Tokuda S, Lee J, Miyata K. Effect of the ratio of axial length to keratometry on SRK/T intraocular lens power calculations for eyes with long axial lengths. Sci Rep. 2019;9:19515. doi:10.1038/s41598-019-56116-4
7. Darcy K, Gunn D, Tavassoli S, Sparrow J, Kane JX. Assessment of the accuracy of new and updated intraocular lens power calculation formulas in 10 930 eyes from the UK National Health Service. J Cataract Refract Surg. 2020;46:2–7. doi:10.1016/j.jcrs.2019.08.014
8. Wan KH, Lam TCH, MCY Y, Chan TCY. Accuracy and precision of intraocular lens calculations using the New Hill-RBF Version 2.0 in eyes with high axial myopia. Am J Ophthalmol. 2019;205:66–73. doi:10.1016/j.ajo.2019.04.019
9. Iijima K, Kamiya K, Iida Y, Shoji N. Comparison of predictability using Barrett Universal II and SRK/T formulas according to keratometry. J Ophthalmol. 2020;2020:7625725. doi:10.1155/2020/7625725
10. Rong X, He W, Zhu Q, Qian D, Lu Y, Zhu X. Intraocular lens power calculation in eyes with extreme myopia: comparison of Barrett Universal II, Haigis, and Olsen formulas. J Cataract Refract Surg. 2019;45:732–737. doi:10.1016/j.jcrs.2018.12.025
11. Bernardes J, Raimundo M, Lobo C, Murta JN. A comparison of intraocular lens power calculation formulas in high myopia. J Refract Surg. 2021;37:207–211. doi:10.3928/1081597X-20201123-01
12. Choi A, Kwon H, Jeon S. Accuracy of theoretical IOL formulas for Panoptix intraocular lens according to axial length. Sci Rep. 2021;11:7346. doi:10.1038/s41598-021-86604-5
13. Ishida H, Mita T, Shibuya E, et al. Comparison of anterior chamber depth and refractive changes after cataract surgery among three types of monofocal intraocular lenses. Jpn J Cataract Refract Surg. 2020;32:58–62.
14. Charlesworth E, Alderson AJ, de Juan V, Elliott DB. When is refraction stable following routine cataract surgery? A systematic review and meta-analysis. Ophthalmic Physiol Opt. 2020;40:531–539. doi:10.1111/opo.12719
15. Khan AM, Waldner DM, Luong M, Sanders E, Crichton ACS, Ford BA. Stabilization of refractive error and associated factors following small incision phacoemulsification cataract surgery. BMC Ophthalmol. 2022;22(1):13. doi:10.1186/s12886-021-02221-w
16. Ostri C, Holfort SK, Fich MS, Riise P. Automated refraction is stable 1 week after uncomplicated cataract surgery. Acta Ophthalmol. 2018;96:149–153. doi:10.1111/aos.13545
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.