Back to Journals » Psychology Research and Behavior Management » Volume 19
Internet and Smart Devices Usage and Mental Health in Chinese Older Adults with Chronic Diseases: The Mediating Role of Social Isolation
Received 12 September 2025
Accepted for publication 22 January 2026
Published 28 January 2026 Volume 2026:19 567161
DOI https://doi.org/10.2147/PRBM.S567161
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Gabriela Topa
Huijie Zhu,1,2 Guodong Zhou3
1College of Humanities and Social Development, Nanjing Agricultural University, Nanjing, Jiangsu, 210095, People’s Republic of China; 2Center for Social Research, Nanjing Agricultural University, Nanjing, Jiangsu, 210095, People’s Republic of China; 3The Academy of Science, Nanjing Agricultural University, Nanjing, Jiangsu, 210095, People’s Republic of China
Correspondence: Guodong Zhou, The Academy of Science, Nanjing Agricultural University, Nanjing, Jiangsu, 210095, People’s Republic of China, Email [email protected]
Background: The internet and digital devices are becoming increasingly involved in the lives of older adults with chronic diseases in China. Our research aims to explore the association between the use of the Internet and smart devices and the mental health of older adults with chronic diseases, and to investigate possible mediating mechanisms.
Methods: Data were obtained from 7150 older adults with chronic diseases in mainland China. The obtained data were analyzed using path analysis, and structural equation models were adopted to explore the impact of the use of the Internet and smart devices on their mental health, and to examine whether social isolation plays a mediating role.
Results: There is an association between usage of internet and smart devices and mental health in older adults with chronic diseases. Internet access and healthcare are positively correlated with mental health, and are also associated with lower levels of social alienation and social exclusion. Social isolation plays an important mediating role in the use of the internet and smart devices as well as in mental health of older adults with chronic diseases.
Conclusion: The research on the relationship between the internet and digital devices and mental health, as well as the mediating effect of social isolation, expands the application of Disengagement Theory in the digital age. Although the use of the internet and digital devices can help reduce social isolation and improve mental health, not all smart devices contribute to reducing social isolation.The use of certain intelligent devices, such as sleep monitoring devices, may be associated with risk factors for social participation and mental health. It is important to distinguish the roles of the different types of functional devices. Therefore, more attention should be given to the positive role of digital technology in healthcare for older adults.
Keywords: internet use, smart devices, mental health, older adults with chronic diseases, social isolation
Introduction
The mental health of older adults is emerging as a pressing global public health concern. The global burden of mental disorder among older adults has increased since 1990 and its prevalence is projected to continue increasing through 2050.1 Epidemiological data indicate that one in three individuals aged 65–84years has experienced a mental disorder within the past year, and one in four currently lives with a diagnosable mental disorder.2 Among the multifaceted factors linked to older adults’ mental health, the experience of chronic illness warrants particular scholarly attention.3 Chronic diseases have been shown to markedly elevate depression scores in older populations,4 and they exhibit strong associations with poor mental health outcomes5 and elevated risks of developing mental illnesses.6 Chronic diseases, also known as noncommunicable diseases (NCDs), were recognized as a major challenge for sustainable development in The 2030 Agenda for Sustainable Development. Chronic diseases killed at least 43 million people in 2021,7 which is equivalent to 75% of non-pandemic-related deaths globally.8 One study estimated that, between 2006 and 2015, 23 low- and middle-income countries would collectively lose about US$84 billion in economic output due to the negative effects of heart disease, stroke, and diabetes.9 Chronic diseases impose a significant burden on national health expenditures and personal health management. For most older people, living with chronic diseases has become a norm. Older adults are vulnerable to the risk factors contributing to chronic diseases,10 especially in low- and middle-income countries. In recent years, the incidence of chronic diseases has been continuously increasing, and there has been an increased prevalence of chronic disease in younger patients,11 which also leads to the continuous expansion of the population of older adults with chronic diseases. The prevalence of having at least one chronic disease was 41.8% for adults, 65% among people aged 65–74, and 79.6% among those aged 75 and above in 2011.12 More than 80% of older adults in China have at least one chronic disease.13
Chronic diseases are difficult to achieve rapid cure through medication or other medical interventions; thus, older adults ofen have to live with chronic conditions,which can exert a significant negative impact on their mental health.14 Chronic diseases are closely associated with mental health disorders, such as depression15 and anxiety16 in older adults.6 The number of chronic diseases is significantly related to the depressive symptoms of older adults in China,17 Comorbidity has a greater impact on the mental health of older adults.In the context of the digital society, there is a clear correlation between older adults’ usage of the Internet and smart devices and their mental health outcomes.A large number of researches indicate that the use of the internet18 and smart devices19 is an important factor in improving the mental health of older adults. Smart devices that have been confirmed to improve the mental health of older adults include smart phones,20 wearable devices,21 and contactless sleep monitoring.22 Some studies have suggested that the use of the internet and digital devices may have a negative impact on mental health.23 Specifically, problematic mobile phone use has been linked to diminished perceived social support and subsequent adverse mental health consequences.24 Maladaptive usage patterns may foster the development of digital dependence, a behavioral pattern that exerts a deleterious influence on psychological well-being.25
In recent years, China has vigorously promoted the Digital China strategy and continuously advanced the process of digital construction; however, the problem of digital divide remains prominent.26 Older adults are at a disadvantage in the process of digital society construction,27 and there are significant disparities in their usage of the Internet and smart devices,28 which in turn affect their health.29 Variables associated with both Internet/smart device usage and mental health primarily include social interaction-related factors, healthy lifestyle factors, and socioeconomic factors, such as social activities,30 and cultural capital.31 Digital engagement constitutes a key factor enabling the internet and digital devices to enhance the mental health of older adults by boosting self-efficacy and social integration. For older adults with chronic diseases, restricted social interactions resulting from limited mobility or physical disabilities make digital participation an important avenue for engaging in social activities.
Existing studies have explored the association between the use of internet and smart device and the mental health of older adults with chronic diseases. However, insufficient attention has been paid to the underlying internal mechanisms, and the mediating effect of social isolation has not been clearly described. Therefore, this study analyzed the relationship between the use of the internet and smart devices and mental health using the survey data from the China Longitudinal Ageing Social Survey 2023 (CLASS2023) and attempted to verify the mediating role of social isolation.
Theoretical Model and Hypotheses
Social Cognitive Theory
Social Cognitive Theory (SCT) provides a robust analytical framework forexamining the relationship between internet and smart device use and mental health outcomes. As a foundational psychological theory, SCT fouses on the dynamic interplay between individual behavior, motivational processes, and environmental contexts32. Bandura proposed the triadic reciprocality model, positing that human functioning is shaped by three mutually influential factors: behavioral, environmental, and personal characteristics.33.The interaction among behavior, personal factors, and environment is dynamic and bidirectional, rather than a simple causal relationship.34
In this study, internet and smart device use is conceptualized as a behavioral factor, social isolation as an environmental factor, and mental health as a personal outcome. This conceptualization gives rise to a proposed analytical pathway: internet and smart device use may exert an impact on individual mental health through the mediating role of social isolation. It is important to note that this pathway does not preclude potential interaction effects from alternative pathways. However, given the cross-sectional nature of the data employed in this study, the primary objective is to verify the existence of this proposed pathway rather than to exhaustively test all possible interactive influences. The complete analytical framework is illustrated in Figure 1.
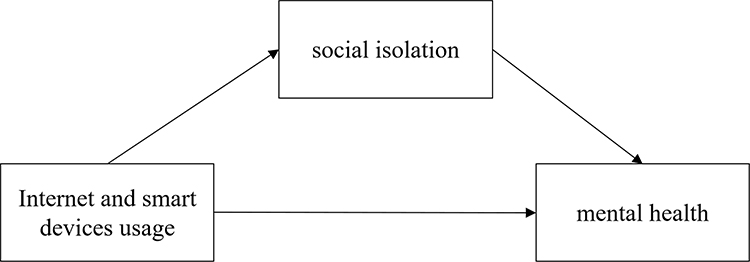 |
Figure 1 Conceptual framework. |
Digital Divide and Mental Health of the Older Adults
The advent of the digitalization age has given rise to the digital divide.35 This divide stems from disparities in the accessibility (availability) and utilization (adoption) of the Internet across different social groups.36 With the acceleration of technological iteration, the Internet has become a pivotal medium for social interaction. However, older adults generally exhibit limited capacity to adapt to new technologies, rendering them prone to information disadvantage37 and increasing their risk of social exclusion.38 Not all older adults are in a disadvantaged position in the information society. Similar to younger adults, older individuals with digital advantages can reap the health dividends brought about by the digital era. Internet use serves as a bridge connecting older adults with chronic diseases to abundant online resources and the digitized modern society, which can exert a positive impact on their mental health. Empirical research has confirmed that Internet access and usage are positively associated with the mental health of older adults with chronic diseases.39 On one hand, internet access and usage can enhance social participation, thereby improving mental health;40 on the other hand, it can promote physical health through e-health services, which in turn further improves mental health.41 Accordingly, we propose the first hypothesis.
H1. Older adults with chronic diseases who have access to the internet exhibit a higher level of mental health compared to their counterparts without internet access.
Smart devices may also be associated with the mental health of older adults with chronic diseases. Thus, these individuals have heightened health management needs.42 Smart devices with health monitoring functions may have a positive impact on physical and mental health.43 Research has shown that smart home health technology can promote the mental health of older people.44 Accordingly, we propose the next hypothesis.
H2. Older people with chronic diseases who use smart devices exhibit a higher level of mental health than those who do not.
Disengagement Theory and the Mediating Effect of Social Isolation
According to Disengagement Theory, with the decline in physical function and retirement, older people will gradually withdraw their social roles, free themselves from the social expectations related to productivity and competitiveness, transition to secondary social roles, and voluntarily maintain distance from society.45 Disengagement Theory has often been criticized by proponents OF Active Theory46 for its perceived lack of respect for the values of older adults. In fact, the widely documented prevalence of loneliness and social isolation in later life47 provides a realistic basis of Disengagement Theory. Social isolation and loneliness are common among older adults,48 affecting one in four individuals in this group.49 The risk of social isolation and loneliness increases in older adults facing aging and disease.50 When older adults leave productive jobs, the social support derived from occupational ties gradually diminishes, making them more reliant on geographic and kinship-based relationships. Unfortunately, as age increases, older adults’ social networks tend to shrink, and their access to social support decreases accordingly. Thus, social isolation is a risk factor for subjective wellbeing51 and mental illness.52
Maintaining a certain level of social participation is crucial for sustaining active health in old age.53 Media functionalism posits that mass media plays a connecting role54 and can build connections between individuals and their social networks,55 thereby improving mental health. In an information society, networks and smart devices can serve as tools for maintaining and rebuilding connections with social networks, thereby providing social support to older adults. Using the internet and smart devices can reduce social isolation.56 Therefore, social isolation may serve as a mediating variable in the relationship between internet and smart device use and mental health. Accordingly, we propose the third hypothesis.
H3. The use of Internet and smart devices improves the mental health of older adults by reducing their social isolation.
The mediating effect of social isolation is an exploratory hypothesis. Whether this effect exists and to what extent it operates require verification through mediation analysis.
Methods
Data Collection
Data for this study were defined from a sample of older adults drawn from the CLASS2023. The CLASS2023 is a stratified, multistage probability sampling survey covering 28 provincial areas in China, conducted by the Renmin University of China. In the sampling procedure, county-level regions (including counties, county-level cities, and municipal districts) were first identified as Primary Sampling Units (PSUs). Subsequently, villages or neighborhood committees within these PSUs were selected as Secondary Sampling Units (SSUs). A systematic sampling method was employed to recruit survey participants from each selected SSU, with a standardized target of completing 25 valid questionnaires per SSU.57 In total, 11,670 adults aged 60 years and above were interviewed.For the purposes of the present study, the sample was further restricted to older adults with chronic diseases to align with the core research focus.
Sample Description
Older adults with chronic diseases were operationalized as individuals aged 60 years or older who self-reported having at least one of 23 predefined chronic conditions. Chronic diseases commonly refer to 23 kinds of diseases such as hypertension, heart disease, diabetes or elevated blood glucose, cerebrovascular disease, kidney disease, liver disease, and cancer/malignant tumors.older adults with chronic mental illnesses were excluded from the final sample for two methodologically critical reasons: (1) data quality concerns—individuals with chronic mental illnesses may face challenges in completing structured surveys, potentially introducing response bias; and (2) avoidance of endogeneity issues—pre-existing chronic mental illnesses could confound the assessment of mental health outcomes, making it difficult to disentangle the causal pathways of interest. After excluding participants with missing values for core variables, a final sample of 7,150 older adults was retained for analysis. The sociodemographic characteristics of the participants are presented in Table 1.
 |
Table 1 Participants’ Descriptive Statistics (N=7150) |
Measurement
Dependent Variables
Mental health was assessed using an abbreviated 9-item Center for Epidemiological Studies Depression Scale (CES-D9, chinese version), which is reliable and valid for detecting depressive symptoms among Chinese older adults.58 The scale includes three questions on positive emotions and six questions on negative emotions such as “Have you been in a good mood?” “Have you had a good life?” “Have you been sad?” Responses to the questions were rated on a three-point scale, from 1(low) to 3(high). The total score was calculated by adding up the scores of 9 questions.59 Mental Health Index (MHI) was obtained by adding positive and negative emotions in a positive direction, with values ranging from 9 to 27, and higher scores indicating better mental health status.
Independent Variables
The independent variables include the use of networks and smart devices, involving four distinct indicators. Internet usage was measured using two variables: internet access and internet healthcare. Smart device usage was measured using two variables: smart bracelet and intelligent sleep monitor. All four variables are related to the usage of internet and smart devices.
The Mediating Variable
The mediating variable was social isolation, measured through 8-item scale, such as “I feel excluded because of my age.” The Cronbach’s alpha of the scale was 0.671 which falls below the conventional threshold of 0.7 for acceptable internal consistency in established scales.0.7 is a value typically considered indicative of “acceptable internal consistency” for established scales. However, this lower alpha was deemed reasonable and interpretable in the context of the present study, as exploratory scales often exhibit slightly reduced reliability during initial application.60 This decision was further supported by existing literature, which notes that alpha values between 0.6 and 0.7 may still be acceptable for exploratory research focused on preliminary associations rather than definitive measurement.61 A factor analysis was conducted on the scale. The Kaiser-Meyer-Olkin measure of sampling adequacy was 0.773, which was suitable for factor analysis. Finally, two common factors were extracted, social alienation and social exclusion, with a cumulative variance contribution rate of 52.66%.
Control Variables
There were eight control variables. Gender, marital status, and household registration type were dummy variables converted to male, married, and agricultural hukou (agricultural registered permanent residence). Educational level was converted to years of education, based on years of schooling and highest education level. Multimorbidity was the number of chronic diseases suffered, and income was converted to Ln (income last year+1).
Statistical Analyses
To examine the mediating role of social isolation in the relationship between internet and smart device use (independent variable, IV) and mental health (dependent variable, DV) among older adults, this study employed path analysis and structural equation modeling—two widely used statistical techniques for testing mediation effects.62 Path analysis prioritizes the interpretation of hypothesized relationships between variables rather than causal discovery,63 and was implemented in three sequential steps to verify the mediating effect of social isolation (mediator, M): Step 1: Test the direct association between the IV (internet and smart device use) and the DV (mental health index); Step 2: Test the direct association between the mediator (social isolation) and the DV (mental health index); Step 3: Test the direct association between the IV (internet and smart device use) and the mediator (social isolation).Only when all three above mentioned associations were statistically significant could social isolation be confirmed as a mediator in the relationship between internet and smart device use and mental health.
Structural Equation Modeling (SEM). SEM is a multivariate statistical approach that analyzes relationships between variables based on their covariance matrix, offering advantages in handling complex latent constructs and testing multiple pathways simultaneously. In this study, SEM was further used to validate the mediating effect of social isolation, complementing the results of path analysis and enhancing the robustness of the mediation inference.
Descriptive statistics (eg, frequencies, means, and standard deviations for sociodemographic variables and key constructs) and general linear regression (conducted as a preliminary analysis to screen covariates) were performed using SPSS 24.0. Path analysis was also implemented in SPSS 24.0, while SEM was executed via AMOS 26.0 to explicitly model the mediating pathway: internet and smart device use→social isolation→mental health. Prior to formal analyses, key model assumptions were verified, including the normality of continuous variables and the absence of severe multicollinearity, to ensure the validity of statistical inferences.
Results
Participants’ Mental Health Status and Their Usage of the Internet and Digital Devices
Table 2 showed a descriptive analysis of the mental health status of older adults with chronic diseases. The average MHI of older adults with chronic diseases is 20.21. There were significant differences in MHIs between registered urban and rural residences, sex, and age.
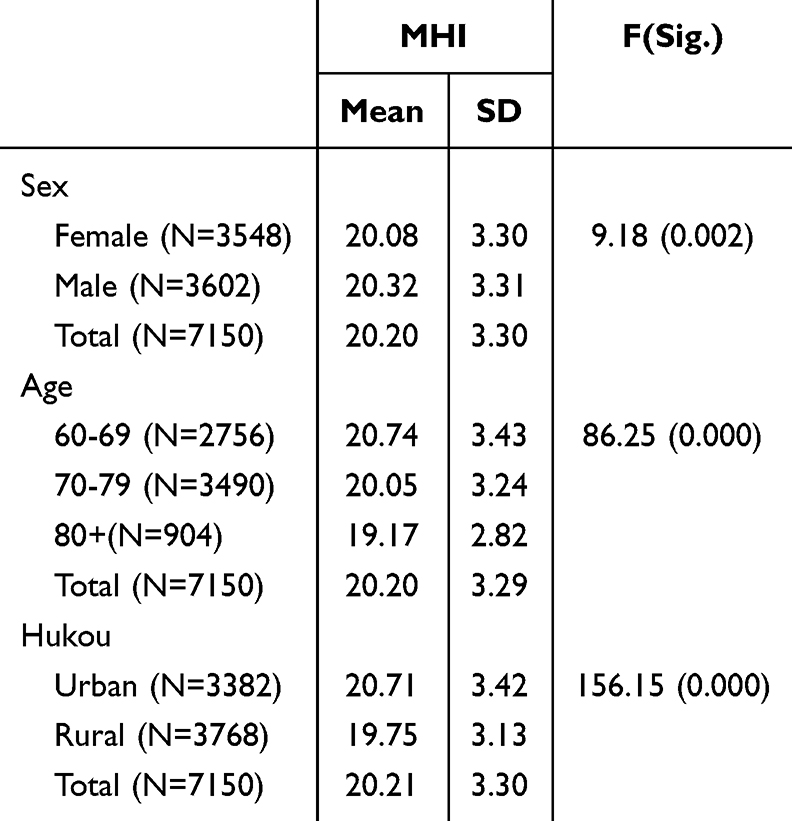 |
Table 2 Mental Health Status of Older Adults |
Regarding the use of the internet and digital devices, 69.8% of the families had internet access, 3.3% of older adults used internet healthcare services, 11.1% had smart bracelets, and 3.3% had intelligent sleep monitors. It is found that there were differences in Internet access and smart device use among respondents of different ages and registered residence in Table 3. The ratio of network access and smart device use among urban respondents was significantly better than that of rural respondents; the older the age, the lower the ratio of internet access and smart device usage.Gender differences of Internet access and smart device use were not found.
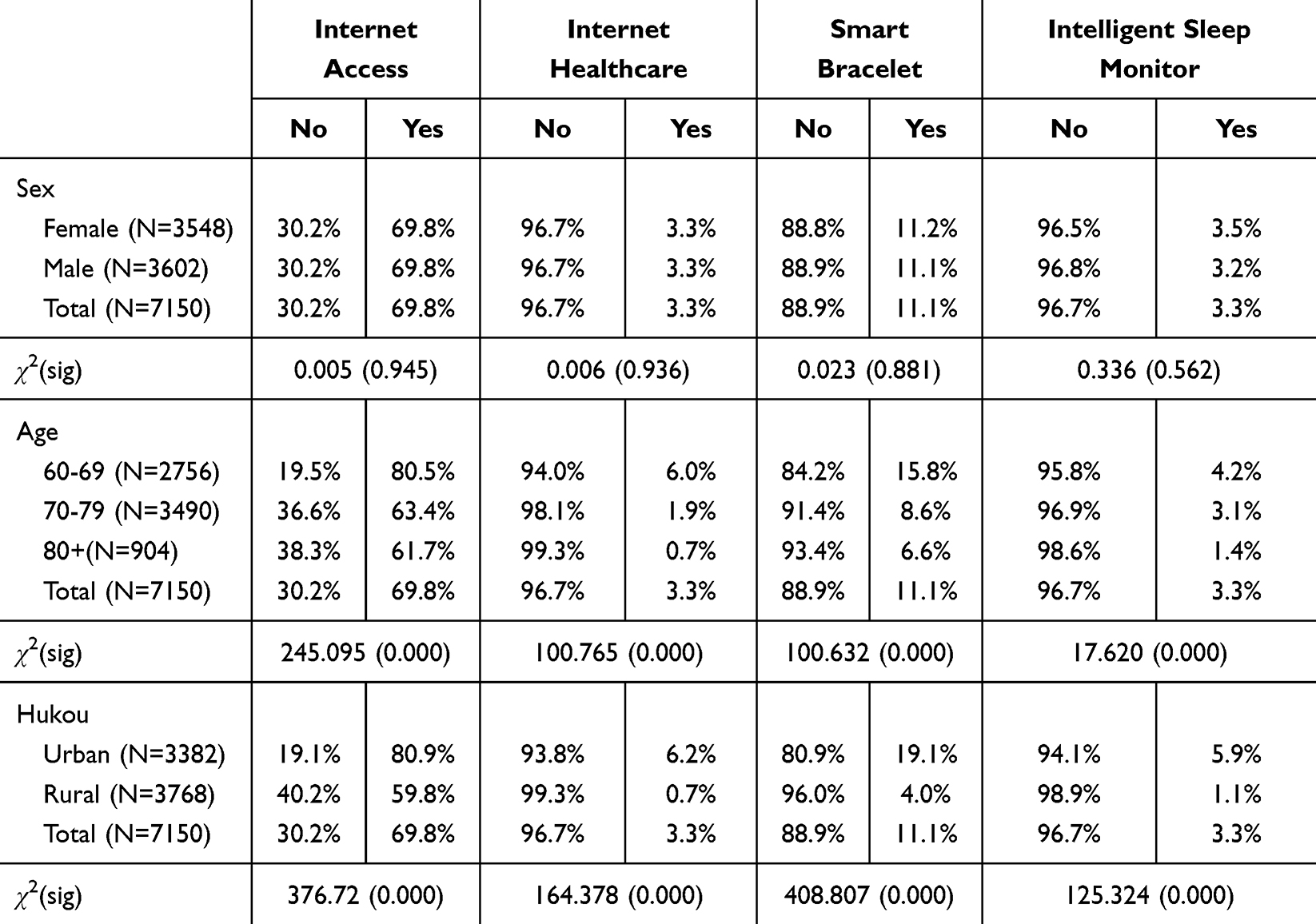 |
Table 3 The Usage of the Internet and Digital Devices of Older Adult |
The Association Between Mental Health Status and Usage of Internet and Digital Devices
Before exploring the causal relationships, the correlations between the variables were tested as shown in Table 4. There was a significant correlation between the MHI and the use of networks and smart devices. Social isolation was significantly negatively correlated with MHI. There was also a significant correlation between the variables related to internet and smart device usage.
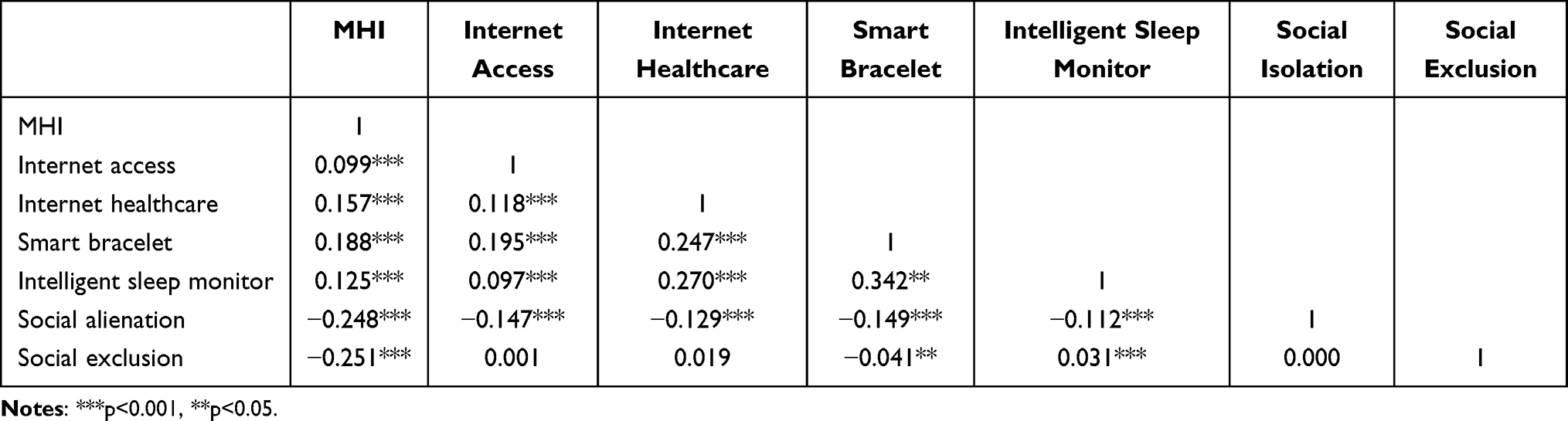 |
Table 4 Results of Pearson’s Correlations Test |
After verifying the correlation between variables, general linear regression analysis was performed with MHI as the dependent variable. Three models were established in Table 5. Model 1 included only control variables, Model 2 included only core independent and mediator variables, and Model 3 was a full model with all independent variables. The adjusted r-squared values for Models 1, 2, and 3 were 0.072, 0.157, and 0.194, respectively. Thus, the explanatory power of the independent variables in the models is acceptable.
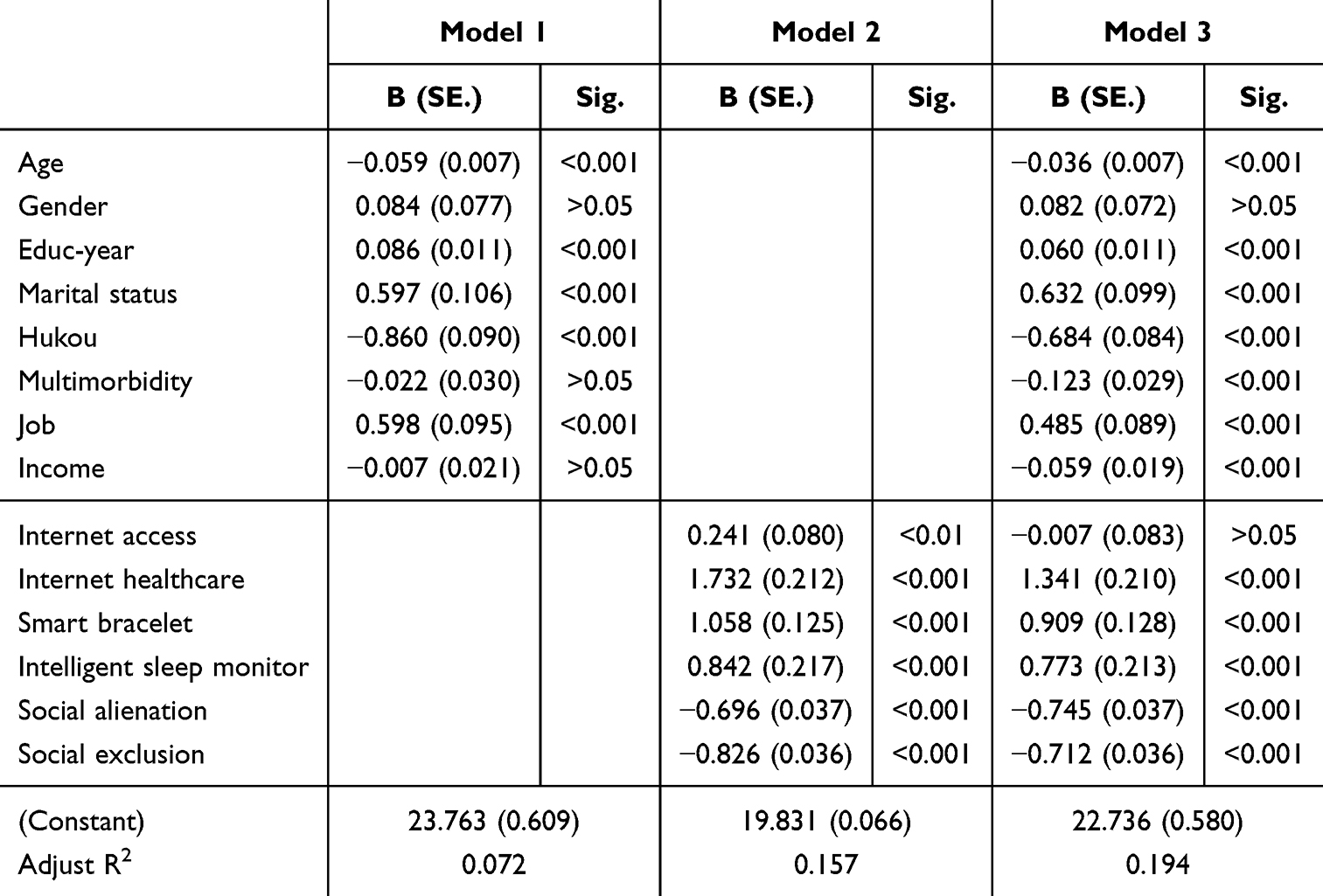 |
Table 5 Linear Regression of MHI in Older Adults with Chronic Disease |
In Model 2, all variables had a significant positive impact on MHI. The use of the internet and smart devices had a positive impact on the mental health of older adults with chronic diseases. Further, both indicators of social isolation lowered participants’ mental health levels. In Model 3, after adding the control variables, the significance of most variables did not change, except for internet access. This analysis validates Hypotheses 1 and 2.
Mediating Role of Social Isolation
A path analysis was used to test the mediating effects of social isolation. The models in Table 6 verify the impact of internet use, smart device use, and social isolation on the MHI of older adults with chronic diseases. If the impact of internet and smart device use on social isolation can be confirmed, the mediating effect of social isolation can be verified. As there are two dimensions of social isolation, regression analysis was conducted on the two factors separately. Models 4 and 6 use the two common factors of social isolation as dependent variables, and internet and smart device use as independent variables, which do not include control variables. Models 5 and 7 include the control variables. The results of the models are shown in Table 6.
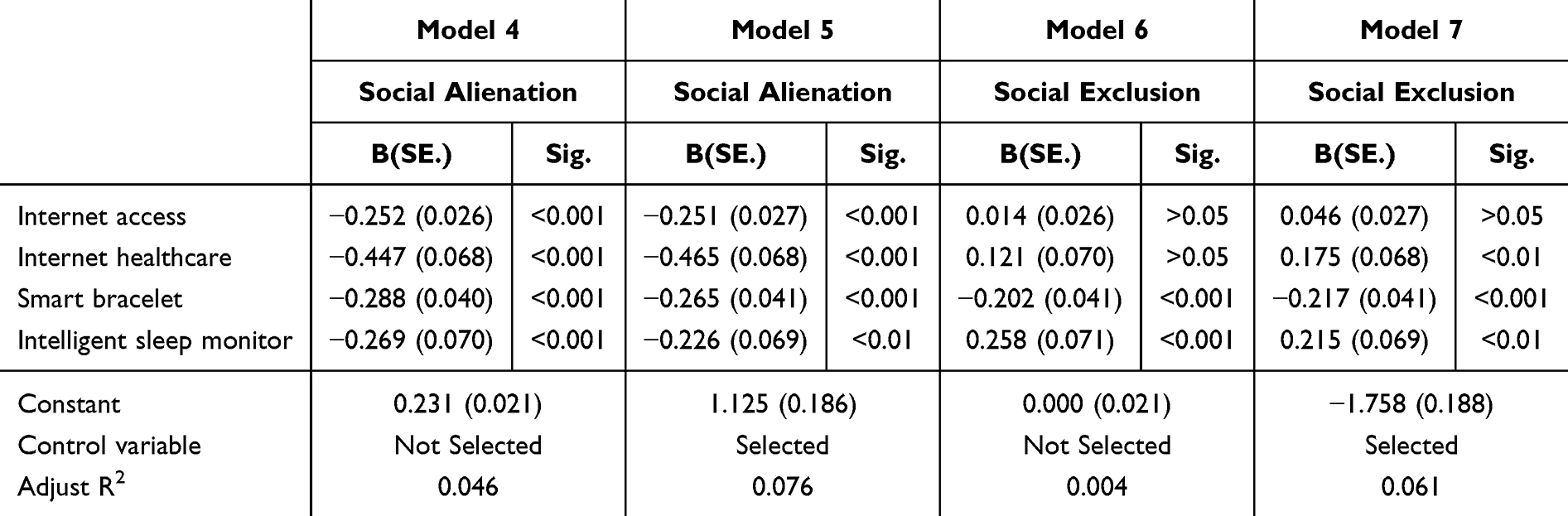 |
Table 6 Linear Regression of Social Isolation |
In Models 4 and 5, the use of the internet and smart devices has been shown to have a significant negative impact on social isolation, indicating that the internet and smart devices can reduce social isolation. In Models 6 and 7, only smart device use had a significant impact on high social exclusion. Contrary to this hypothesis, intelligent sleep monitors increase rather than decrease social exclusion, indicating that smart devices may have both inhibitory and promoting effects on social isolation.
Structural equation modeling was conducted to test the mediating effect of social isolation on the relationship between internet and smart device usage and mental health. The chi-square value of the default model was 3.465 (p=0.325), the root mean square error of approximation (RMSEA) was 0.005, the comparative fit index (CFI) was 0.999, and the Tucker-Lewis index (TLI) was 0.999. These indicators showed that the mediation model met the requirements of SEM and that the mediation effect model was valid and effective.
Figure 2 shows the results of the structural equation model, presenting the impact path of social isolation as a mediating effect. On the one hand, the usage of internet and digital devices reduces the social alienation of older adults with chronic diseases, thereby improving their mental health situation. On the other hand, smart device use is associated with social exclusion, which further affects mental health.
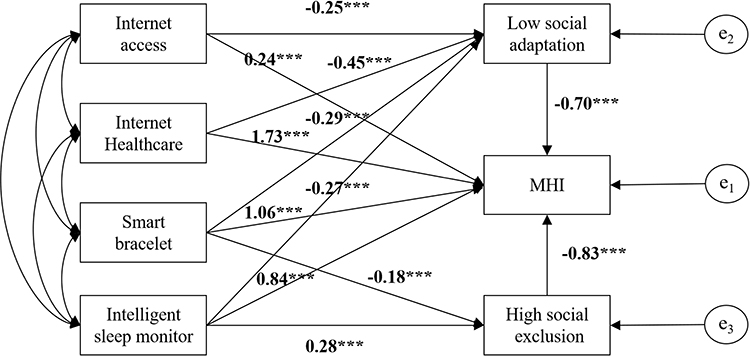 |
Figure 2 Testing the mediating effects of social isolation. Notes: ***p<0.001. |
The variable effects of the SEM models are shown in Table 7. Internet access, Internet medicine, smart bracelets and smart sleep monitors have indirect effects on the mental health of the older adults with chronic diseases, in which social alienation plays a mediating role. However, contrary to research hypothesis 3, it is found that the mediating effect of using smart sleep monitors is negative. Using an intelligent sleep monitor can suppress low-level social adaptation, but can increase social exclusion; therefore, it is necessary to pay attention to the effects of different categories of smart devices.
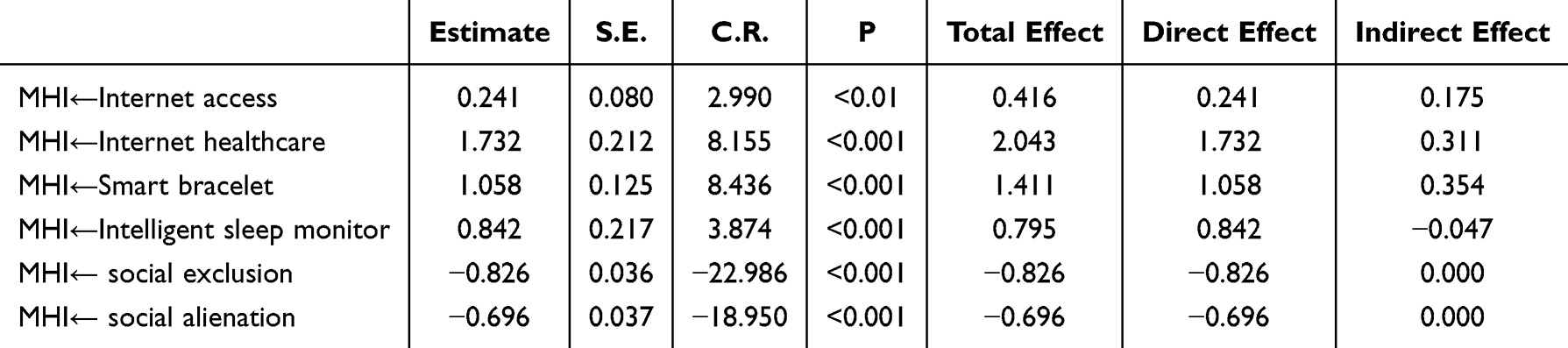 |
Table 7 Variable Effects in the SEM Model |
Discussion
Given that social isolation is a public health issue,64 the potential role of internet-connected intelligent devices should not be overlooked. Pior research has found relationships between the use of the internet and smart devices, social isolation,65 and mental health.66 Our research found that the use of the Internet and smart devices is related to the mental health of older adults with chronic diseases, in which social isolation plays a mediating role. Social connections and adaptation are important pathways from internet use to older adults’ health.67 The internet and intelligent devices have an important impact on social interaction and mental health in the digital age as well as in older people. The older adult population with chronic diseases is a vulnerable group in the digital divide68 and faces higher risks to both physical and mental health. Use of the internet and smart devices is a behavioral factor that reduces social isolation and mental health problems caused by social disengagement.
By 2025, the internet penetration rate in China will reach 79.7%, with the proportions of smart home devices and personal wearable devices accessing the internet at 21.4% and 28.6%, respectively.69 Although older people are the most common group in digital poverty,70 a considerable proportion of older adults with chronic diseases have to use the internet or smart devices. Thus, there is a class gap in digital use among older adults. People from the lower-middle class have disadvantages in digital and smart device usage, resulting in digital inequality.71 Older people with lower incomes do not have the ability to pay for internet access and smart devices, nor do they have the ability and motivation to use them. The inequality in digital usage between urban and rural areas was particularly evident. The level of digital infrastructure in cities is relatively high,72 and many older adults have a high level of education and payment ability to use the internet and digital devices. However, in rural areas, the lack of sound digital infrastructure leads to reduced use of digital devices among older adults. The digital divide between urban and rural areas53 may lead to more pronounced psychological health inequality in countries, and digital inequality caused by socioeconomic factors has given rise to new health inequalities73 that require government and societal intervention.
Although the use of the internet and smart devices has a positive impact on the mental health of older people with chronic diseases, not all smart devices contribute to reducing social isolation, such as intelligent sleep monitoring, which increases social isolation. This may be because older adults with chronic diseases who experience sleep problems are more likely to purchase and use intelligent sleep monitors,while sleep problems may lead to a decrease in social participation, which is detrimental to mental health.74 Studies have indicated that digital lifestyles have potential benefits and harms for health.75 It cannot be ruled out that the usage behavior of certain intelligent devices may be associated with risk factors for social participation and mental health of older adults. It is necessary to distinguish the roles of different smart devices and suppress their impact on social isolation.Therefore, more attention should be given to the positive role of digital technology in healthcare. The probability of older adults suffering from chronic diseases is high globally, and many suffer from more than one chronic disease.76 With the digitization of society, an increasing amount of medical resources will exist in digital form, and chronic disease management will increasingly require the internet and smart devices;77 however, we must remain vigilant about this. The internet and digital devices can indeed improve health levels, but at the same time they may also confine older adults to small circles, forming an information cocoon.78 It is necessary to fully utilize the internet and smart devices to conduct health management, reduce social isolation, and improve the well-being of older adults. However, it is necessary to increase the regulation of the internet and smart devices to prevent negative effects.
Limitation
This study explored the associations between internet and smart device use, social isolation, and mental health among older adults with chronic diseases, and proposed a potential mediating pathway. Despite its contributions, several limitations should be acknowledged: First, the study only identifies correlational relationships rather than causal ones. Given that the analysis relies on cross-sectional data from the CLASS2023, it is impossible to establish the directionality of the observed associations. Second, the reliability of the social isolation scale used in this study was suboptimal. Although existing literature supports the acceptability of such reliability levels for exploratory research, the lower Cronbach’s alpha (below 0.7) increases the risk of measurement bias. This bias may attenuate the strength of the observed associations between social isolation and other key variables, potentially leading to underestimation of the true mediating effect. Third, the sample sizes for the subgroups using Internet healthcare and smart sleep monitors were insufficient, which compromises the credibility of the analyses examining the relationships involving these variables. To address these limitations, future research should adopt longitudinal tracking designs to collect panel data, which would facilitate the establishment of causal inferences. Additionally, developing or validating a more reliable social isolation scale tailored to the Chinese older adults—particularly those with chronic conditions—would help reduce measurement error and improve the robustness of subsequent analyses.
Conclusion
Based on data from 7150 Chinese older adults with chronic diseases, this study demonstrates that internet and digital device use is significantly associated with mental health, with social isolation playing an important mediating role. The use of the internet may help reduce social isolation and improve the mental health of older people with chronic diseases, while the use of smart bracelets helps reduce social exclusion and improve mental health. The results suggest that the use of Internet and digital devices can help older adults integrate into their social networks, thereby reducing the risks associated with social withdrawal.Notably, not all smart devices contribute to reducing social isolation. The use of sleep monitoring devices, were found to increase social exclusion, which may be associated with risk factors for social participation and mental health.These results highlight the need for a nuanced understanding of the heterogeneous effects of different digital devices on older adults’ mental health and social well-being.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Review Committee of the college of humanities and social development, Nanjing agricultural University (202509001).
Acknowledgment
Thank the Institute of Gerontology of Renmin University of China for providing CLASS, which data can be accessed at http://www.class.ruc.edu.cn.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Fundamental Research Funds for the Central Universities of Nanjing Agricultural University (Grant No.SKYD2025021).
Disclosure
The authors declare that there are no competing interests.
References
1. Wang Y, Qin C, Chen H, Liang W, Liu M, Liu J. Global, regional, and national burden of major depressive disorders in adults aged 60 years and older from 1990 to 2021, with projections of prevalence to 2050: analyses from the Global Burden of Disease Study 2021. J Affective Disorders. 2025;374:486–14. doi:10.1016/j.jad.2025.01.086
2. Andreas S, Schulz H, Volkert J, et al. Prevalence of mental disorders in elderly people: the European MentDis_ICF65+ study. Br J Psychiatry. 2017;210(2):125–131. doi:10.1192/bjp.bp.115.180463
3. Bertolazzi A, Quaglia V, Bongelli R. Barriers and facilitators to health technology adoption by older adults with chronic diseases: an integrative systematic review. BMC Public Health. 2024;24(1):506. doi:10.1186/s12889-024-18036-5
4. Li D, Su M, Guo X, Liu B, Zhang T. The association between chronic disease and depression in middle-aged and elderly people: the moderating effect of health insurance and health service quality. Front Public Health. 2023;11:935969. doi:10.3389/fpubh.2023.935969
5. Wang S, Li B, Ungvari GS, et al. Poor mental health status and its associations with demographic characteristics and chronic diseases in Chinese elderly. Social Psychiatry Psychiatric Epidemiol. 2016;51(10):1449–1455. doi:10.1007/s00127-016-1271-y
6. Huang Y, Loux T, Huang X, Feng X. Xiaoke Feng.The relationship between chronic diseases and mental health: a cross-sectional study. Mental Health Prev. 2023;32:200307. doi:10.1016/j.mhp.2023.200307
7. Global Health Estimates. Deaths by Cause, Age, Sex, by Country and by Region, 2000–2021. Geneva: World Health Organization; 2024.
8. World Health Organization. Tackling NCDs: best buys and other recommended interventions for the prevention and.
9. Beaglehole R, Ebrahim S, Reddy S, Voûte J, Leeder S. Steve Leeder.Prevention of chronic diseases: a call to action. Lancet. 2007;370(9605):2152–2157. doi:10.1016/S0140-6736(07)61700-0
10. World Health Organization. Assessing national capacity for the prevention and control of noncommunicable diseases: report on 2023 global survey. Geneva: World Health Organization. 2025.
11. Lim LL, Jones S, Cikomola JC, et al. Understanding the drivers and consequences of early-onset type 2 diabetes. Lancet. 2025;405(10497):2327–2340. doi:10.1016/S0140-6736(25)01012-8
12. Van Oostrom SH, Gijsen R, Stirbu I, et al. Time Trends in Prevalence of Chronic Diseases and Multimorbidity Not Only due to Aging: data from General Practices and Health Surveys. PLoS One. 2016;11(8):e0160264. doi:10.1371/journal.pone.0160264
13. Su B, Li D, Xie J, et al. Chronic disease in China: geographic and socioeconomic determinants among persons aged 60 and older. J Am Med Directors Assoc. 2023;24(2):206–212.e5. doi:10.1016/j.jamda.2022.10.002
14. Shang X, Peng W, Hill E, Szoeke C, Mingguang H, Lei Z. Incidence of Medication-Treated Depression and Anxiety Associated with Long-Term Cancer, Cardiovascular Disease, Diabetes and Osteoarthritis in Community-dwelling Women and Men. EClinicalMedicine. 2019;30(15):23–32. doi:10.1016/j.eclinm.2019.08.010
15. Ma Y, Xiang Q, Yan C, et al. Relationship between chronic diseases and depression: the mediating effect of pain. BMC Psychiatry. 2021;21(1):436. doi:10.1186/s12888-021-03428-3
16. Scott AJ, Correa AB, Bisby MA, et al. Depression and anxiety trajectories in chronic disease: a systematic review and meta-analysis. Psychother Psychosomat. 2023;92(4):227–242. doi:10.1159/000533263
17. Ni Z, Zhu X, Tian K, Chen Q, Yang Y, Xie S. Depressive symptoms of older adults with chronic diseases: the mediating roles of activities of daily living and economic burden of diseases. Front Psychol. 2024;15:1387677. doi:10.3389/fpsyg.2024.1387677
18. Lam SSM, Jivraj S, Scholes S. Scholes S.Exploring the Relationship Between Internet Use and Mental Health Among Older Adults in England: longitudinal Observational Study. J Med Internet Res. 2020;22(7):e15683. doi:10.2196/15683
19. Wei Y, Guo X. Impact of smart device use on objective and subjective health of older adults: findings from four provinces in China. Front Public Health. 2023;11:1118207. doi:10.3389/fpubh.2023.1118207
20. Sixsmith A, Cosco TD. Technology, aging, and mental health: opportunities and challenges. Aging Mental Health. 2024;28(4):i–iii. doi:10.1080/13607863.2024.2320132
21. Camacho E, Cohen A, Torous J. Assessment of Mental Health Services Available Through Smartphone Apps. JAMA Network Open. 2022;5(12):e2248784. doi:10.1001/jamanetworkopen.2022.48784
22. Babu M, Lautman Z, Lin X, Sobota MHB, Snyder MP. Wearable Devices: implications for Precision Medicine and the Future of Health Care. Annu Rev Med. 2024;75:401–415. doi:10.1146/annurev-med-052422-020437
23. Hofer M, Hargittai E. Hofer Matthias,Hargittai Eszter: online social engagement, depression, and anxiety among older adults. New Med Soc. 2024;26(1):113–130. doi:10.1177/14614448211054377
24. Ding L, Li Z, Jiang H, et al. Mobile phone problem use and depressive symptoms: the mediating role of social support and attitude to aging among Chinese older adults. BMC Psychiatry. 2024;24(1):135. doi:10.1186/s12888-024-05565-x
25. Mohamed SAAK, Shaban M. Mostafa Shaban.Digital Dependence in Aging: nomophobia as the New Mental Health Threat for Older Adults. J Emerg Nurs. 2025;51(3):371–378. doi:10.1016/j.jen.2025.02.001
26. Li Y, Liu C, Sun J, et al. The digital divide and cognitive disparities among older adults: community-based cohort study in China. J Med Internet Res. 2024;26:e59684. doi:10.2196/59684
27. Schütz N, Saner H, Botros A, et al. Contactless sleep monitoring for early detection of health deteriorations in community-dwelling older adults: exploratory study. JMIR mHealth and uHealth. 2021;9(6):e24666. doi:10.2196/24666
28. Huxhold O, Hees E, Webster NJ. Towards bridging the grey digital divide: changes in internet access and its predictors from 2002 to 2014 in Germany. Eur J Ageing. 2020;17(3):271–280. doi:10.1007/s10433-020-00552-z
29. Van Boekel LC, Peek STM, Luijkx KG. Diversity in older adults’ use of the internet: identifying subgroups through latent class analysis. J Med Internet Res. 2017;19(5):e180. doi:10.2196/jmir.6853
30. Zhu H, Li Z, Lin W. The heterogeneous impact of internet use on older people’s mental health: an instrumental variable quantize regression analysis. Int Journal of Public Health. 2023;68:1605664. doi:10.3389/ijph.2023.1605664
31. Zhao Y, Zhang T, Dasgupta RK, et al. Narrowing the age’ based digital divide: developing digital capability through social activities. Information Systems J. 2023;33(2):268–298. doi:10.1111/isj.12400
32. Schunk DH, DiBenedetto MK. Motivation and social cognitive theory. Contemp Educ Psychol. 2020;60:101832. doi:10.1016/j.cedpsych.2019.101832
33. Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice Hall; 1986.
34. Bandura A. Social Cognitive Theory: An Agentic Perspective on Human Nature. New Jersey: Wiley & Sons; 2023.
35. Cui Y, He Y, Xu X, et al. Cultural capital, the digital divide, and the health of older adults: a moderated mediation effect test. BMC Public Health. 2024;24(1). doi:10.1186/s12889-024-17831-4
36. National Telecommunications and Information Administration (NTIA). Falling Through the Net: Defining the Digital Divide. 1999.
37. Fabiola R, Fazio M. Measuring the Digital Divide.IAOS 2002. Official Statistics New Economy. 2002.
38. Chee SY. Age-related digital disparities, functional limitations, and social isolation: unraveling the grey digital divide between baby boomers and the silent generation in senior living facilities. Aging Mental Health. 2024;28(4):621–632. doi:10.1080/13607863.2023.2233454
39. Tsatsou P. Vulnerable people’s digital inclusion: intersectionality patterns and associated lessons. Inform Comm Soc. 2021;2021(1):1–20. doi:10.1080/1369118X.2021.1873402
40. Peyroteo M, Ferreira IA, Elvas LB, Ferreira JC, Lapão LV. Remote monitoring systems for patients with chronic diseases in primary health care: systematic review. JMIR mHealth and uHealth. 2021;9(12):e28285. doi:10.2196/28285
41. Yang HL, Zhang S, Cheng SM, Tang LL. A study on the impact of Internet use on depression among Chinese older people under the perspective of social participation. BMC Geriatr. 2022;22(1):701. doi:10.1186/s12877-022-03359-y
42. Timakum T, Xie Q, Song M. Analysis of E-mental health research: mapping the relationship between information technology and mental healthcare. BMC Psychiatry. 2022;22(1):57. doi:10.1186/s12888-022-03713-9
43. Reynolds III CF, Jeste DV, Sachdev PS, Blazer DG. Mental health care for older adults: recent advances and new directions in clinical practice and research. World Psychiatry. 2022;21(3):336–363. doi:10.1002/wps.20996
44. Hickey BA, Chalmers T, Newton P, et al. Smart Devices and Wearable Technologies to Detect and Monitor Mental Health Conditions and Stress: a Systematic Review. Sensors. 2021;21(10):3461. doi:10.3390/s21103461
45. Tian YJ, Felber NA, Pageau F, Schwab DR, Wangmo T. Benefits and barriers associated with the use of smart home health technologies in the care of older persons: a systematic review. BMC Geriatr. 2024;24(1):152. doi:10.1186/s12877-024-04702-1
46. Cumming E, Henry W. Growing Old: The Process of Disengagement. New York: Basic Books; 1961.
47. Havighurst RJ. Successful aging. Gerontologist. 1961;1(1):8–13. doi:10.1093/geront/1.1.8
48. Mann F, Wang J, Pearce E, et al. Loneliness and the onset of new mental health problems in the general population. Soc Psychiatry Psychiatr Epidemiol. 2022;57(11):2161–2178. doi:10.1007/s00127-022-02261-7
49. Hajek A, Volkmar A, König HH. Prevalence and correlates of loneliness and social isolation in the oldest old: a systematic review, meta-analysis and meta-regression. Soc Psychiatry Psychiatr Epidemiol. 2025;60(5):993–1015. doi:10.1007/s00127-023-02602-0
50. Kotwal AA, Cenzer IS, Waite LJ, et al. The epidemiology of social isolation and loneliness among older adults during the last years of life. J Am Geriatr Soc. 2021;69(11):1–11. doi:10.1111/jgs.17366
51. Zhang D. Pain and the risk of social isolation and loneliness in older Chinese adults: do gender, age, and education make a difference? Soc sci med. 2024;363:117486. doi:10.1016/j.socscimed.2024.117486
52. Nguyen ND, Lin Z. Social Isolation and Subjective Well-Being Among Older Adults: a Longitudinal Examination by Race/Ethnicity and Gender. J Gerontol B Psychol Sci Soc Sci. 2025;80(6):gbaf066. doi:10.1093/geronb/gbaf066
53. Huijie Z, Haojun J, Zhiping Z, et al. Association between residential environment and emotional wellbeing among older adults in China: the mediating effect of health lifestyle. Front Public Health. 2024;12:1338079. doi:10.3389/fpubh.2024.1338079
54. Jenkins GT, Janich N, Wu S, et al. Social isolation and mental health: evidence from adults with serious mental illness. Psychiatric Rehab J. 2023;46(2):148–155. doi:10.1037/prj0000554
55. Harold LD. The structure and function of communication in society. In: The Communication of Ideas. New York: The Institute for Religious and Social Studies; 1948.
56. Meier A, Reinecke L. Computer-mediated communication, social media, and mental health: a conceptual and empirical meta-review. Commun Res. 2021;48(8):1182–1209. doi:10.1177/0093650220958224
57. Wu Y. The influence mechanisms of living environment on the physical and mental health of Chinese older adults: a cross-sectional exploration based on CLASS 2023. Scitific Report. 2025;15(1):42313. doi:10.1038/s41598-025-26254-z
58. Sen K, Prybutok G, Prybutok V. The use of digital technology for social wellbeing reduces social isolation in older adults: a systematic review. SSM Population Health. 2021;17:101020. doi:10.1016/j.ssmph.2021.101020
59. Zhou D, Zhan Q, Li L. The impact of self-employment on mental health of the younger elderly in China. BMC Geriatr. 2023;2023(23):280. doi:10.1186/s12877-023-03948-5
60. Nunnally JC. Psychometric Theory (2nd Ed.). New York: McGraw-Hill; 1978.
61. Taber Keith S. The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res Sci Educ. 2018;48(6):1273–1296. doi:10.1007/s11165-016-9602-2
62. Kite ME, Whitley Jr BE. Principles of Research in Behavioral Science.
63. Duncan OD. Path Analysis: sociological Examples. Am J Sociol. 1966;72(1):1–16. doi:10.1086/224256
64. Blazer D. Social isolation and loneliness in older adults—a mental health/public health challenge. JAMA psychiatry. 2020;77(10):990–991. doi:10.1001/jamapsychiatry.2020.1054
65. Stockwell S, Stubbs B, Jackson SE, et al. Internet use, social isolation and loneliness in older adults. Ageing Soc. 2021;41(12):2723–2746. doi:10.1089/cpb.2007.0010
66. Chai Y, Xian G, Wang M, et al. Aging wisely: the impact of Internet use on older adults’ mental health. J Affective Disorders. 2024;364:139–145. doi:10.1016/j.jad.2024.08.076
67. Junfeng J, Lisha L. Does Internet use improve the physical and mental health of older adults in China? A study based on the digital divide theory. Geriatric Nurs. 2024;59:526–534. doi:10.1016/j.gerinurse.2024.08.009
68. Frydman JL, Gelfman LP, Goldstein NE, et al. The digital divide: do older adults with serious illness access telemedicine? J Gen Intern Med. 2022;37(4):984–986. doi:10.1007/s11606-021-06629-4
69. China internet network information center. The 56th statistical report on China’s internet development. Available from: https://www.cnnic.net.cn/n4/2025/0721/c88-11328.html.
70. Beneito-Montagut R, Rosales A. Fernández-Ardèvol M.Emerging Digital Inequalities: a Comparative Study of Older Adults’ Smartphone Use. Social Media + Society. 2022;8(4):1–12. doi:10.1177/20563051221138756
71. Richard H. Digital inequality beyond the digital divide: conceptualizing adverse digital incorporation in the global South. Inf Technol Dev. 2022;28(4):688–704. doi:10.1080/02681102.2022.2068492
72. Rongjun Y, Yuanpeng C. On the tension between rural digital empowerment and digital divide and its resolution. J Nanjing Agric Univ. 2021;5(31–40). doi:10.19714/j.cnki.1671-7465.2021.0070
73. Wu M, Xue Y, Ma C. Ma C.The Association Between the Digital Divide and Health Inequalities Among Older Adults in China: nationally Representative Cross-Sectional Survey. J Med Internet Res. 2025;27:e62645. doi:10.2196/62645
74. Ben Simon E, Walker MP. Sleep loss causes social withdrawal and loneliness. Nat Commun. 2018;9(1):3146. doi:10.1038/s41467-018-05377-0
75. Wang B. A comparative analysis of the impacts of digital lifestyles on the physical, mental, and social health among older internet users. Humanit Soc Sci Commun. 2025;12(1):207. doi:10.1057/s41599-025-04490-y
76. Nicholson K, Liu W, Fitzpatrick D, et al. Prevalence of multimorbidity and polypharmacy among adults and older adults: a systematic review. Lancet Healthy Longevity. 2024;5(4):e287–e296. doi:10.1016/S2666-7568(24)00007-2
77. Kvedar J, Fogel A, Elenko E, et al. Digital medicine’s march on chronic disease. Nat Biotechnol. 2016;34(3):239–246. doi:10.1038/nbt.3495
78. He Y, Liu D, Guo R, Guo S. Information Cocoons on Short Video Platforms and Its Influence on Depression Among the Elderly: a Moderated Mediation Model. Psychol Res Behavi Management. 2023;16:2469–2480. doi:10.2147/PRBM.S415832
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Internet Use Behavior and Adolescent Mental Health: The Mediating Effects of Self-Education Expectations and Parental Support
Du W, Fan Z, Li D, Wu M
Psychology Research and Behavior Management 2024, 17:1163-1176
Published Date: 13 March 2024
Mitigating Social Isolation Among Peritoneal Dialysis Patients: The Impact of Educational Level, Physical Activity, and Familial Support
Cai H, Wu Z, Xu J, Wang T, Li Y, Jiang Y, Xu M
Risk Management and Healthcare Policy 2024, 17:2271-2280
Published Date: 20 September 2024