Back to Journals » Psychology Research and Behavior Management » Volume 15
Internalizing Behavior Problems Among the Left-Behind Children of the Hui Nationality in Rural China: A Cross-Sectional Study
Authors Yu X, Wang LL, Liu MM, Li QL, Dai XY, Li LG
Received 10 November 2021
Accepted for publication 15 March 2022
Published 12 April 2022 Volume 2022:15 Pages 887—902
DOI https://doi.org/10.2147/PRBM.S347639
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Xue Yu,1,* Ling-Ling Wang,2,* Miao-Miao Liu,3 Qiu-Li Li,4 Xiu-Ying Dai,4 Lin-Gui Li5
1Department of Psychiatry, Beijing First Hospital of Integrated Traditional Chinese and Western Medicine, Beijing, People’s Republic of China; 2Clinical Psychiatry 16, Luoyang Fifth People’s Hospital-Fifth Affiliated Hospital of Henan University of Science and Technology, Luoyang, Henan Province, People’s Republic of China; 3Mental Health Education Center, Yinchuan University of Energy, Yongning, Ningxia Hui Autonomous Region, People’s Republic of China; 4Mental Health Education Consulting Center, College of Clinic Medicine, Ningxia Medical University, Yinchuan, Ningxia Hui Autonomous Region, People’s Republic of China; 5Department of Epidemiology, School of Public Health and Management, Ningxia Medical University, Yinchuan, Ningxia Hui Autonomous Region, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xue Yu, Department of Psychiatry Beijing First Hospital of Integrated Traditional Chinese and Western Medicine, No. 13 Jintai Road, Chaoyang District, Beijing, 100026, People’s Republic of China, Tel +86-137-1862-8959, Email [email protected]
Background: The internalizing behavior problems (IBPs) of left-behind children (LBC) due to parental migration are a widespread public health concern in China. A previous study showed that the detection rate of behavioral problems in the Hui was far higher than in the LBC of the Han nationality. However, to date, limited research has focused on IBPs in Chinese LBC of the Hui nationality. The aims of this present study are to explore the prevalence of IBPs and the influencing factors among the Hui LBC in the rural areas of China.
Methods: A cross-sectional study was conducted among school students from the southern rural areas in Ningxia, China (2012– 2013). The caregivers or parents assessed IBPs using Achenbach’s Child Behavior Checklist for parents. The children completed the Egma Minnen av Bardndosnauppforstran, Junior Eysenck Personality Questionnaire and Piers–Harris Children’s Self-concept Scale. Data on 383 Hui LBC aged 6– 16 y were included in this study. Multivariate logistic regression analysis was used to examine the relationships between the independent variables and children’s internalizing behaviors.
Results: Among the Hui population, the prevalence of IBPs in LBC and non-left-behind children (non-LBC) was 21.67% (83 of 383) and 18.18% (104 of 572), respectively, with no significant difference between these two groups (χ2 = 1.77 and P = 0.18). However, among males of the Hui population, the prevalence of IBPs in LBC was 22.16%, which is significantly higher than in non-LBC (14.07%; χ2 = 5.07; and P = 0.02). By controlling for gender and age, the multivariate logistic regression analysis showed that a mother highly favoring the subject (odds ratio [OR] = 2.70), average levels of neuroticism (OR = 9.01), and high levels of neuroticism (OR = 8.44) were risk factors for IBPs in Hui LBC.
Conclusion: Our findings suggest that IBPs among male LBC of the Hui nationality in rural China were positively related to parental migration. Positive measures should be taken to prevent IBPs of male LBC of the Hui nationality in rural China in terms of personality development and parental childrearing patterns.
Keywords: Hui nationality, left-behind children, internalizing behavior problems, rural areas
Introduction
Children’s behavioral problems can be divided into externalizing and internalizing behavior disorders.1 Internalizing behavior problems (IBPs) refer to a group of behavior problems, including withdrawal, anxiety, depression, and somatic complaints, that have a tendency to cause internal distress.2 This study focuses on childhood IBPs, which are a major risk factor for later internalizing disorders, including mood and anxiety disorders.2 In addition, previous studies have shown that IBPs are associated with a higher risk of physical symptoms, such as infectious diseases, respiratory diseases, health problems associated with risk behaviors, and weight problems, in children aged 8–20 y.3,4 Importantly, this can cause serious functional impairments later in life,5 resulting in an inability to work properly in young adulthood.6
In recent decades, with the continuous development of China’s industrialization and urbanization, millions of migrant workers have moved from rural areas to cities to improve the circumstances of their families and children. However, due to the restrictions of domicile control and urban public resources, these migrant workers need to leave their children in their hometown to attend school. Therefore, a special population of left-behind children (LBC) has been created. LBC have been defined as children <16 y old who stay in their hometown and are taken care of by their grandparents, relatives, neighbors, one parent, or siblings or take care of themselves for more than six months each year while one or both of their parents migrate to an urban area for work.7 According to the data from the ministry of civil affairs of China, there were about 6.436 million rural LBC in China at the end of 2020.8 Children and adolescents are at a critical period of psychological development, and a long-term separation from their parents will have a lasting negative impact on their psychological and behavioral health,9–11 which makes them prone to IBPs, such as anxiety, depression, and withdrawal.12 Previous studies have suggested that IBPs are the most common mental health problem among adolescents, with a prevalence rate of 31.9% for anxiety disorders and 14.3% for mood disorders.13 If not corrected, these problems will seriously affect the healthy development of children and adolescents.
The Ningxia Hui Autonomous Region is located in Northwest China, with a population of 6.3 million people. The main ethnic groups in Ningxia are the Hui and Han nationalities. The Hui population accounts for approximately one-third of the total population of the autonomous region and one-fifth of the total population of the whole country. The Hui population in the southern mountainous region of Ningxia accounts for more than 60% of the population. Xiji and Haiyuan, two national-level poverty-stricken counties in the southern mountainous region, are the gathering places of the Hui population and have severe water shortages, barren land, closed transportation, backward economies, and a high rate of labor export. Zhao et al14 reported that in the rural areas of Guyuan, China, the mental health of LBC was worse than non-left-behind children (non-LBC). Feng et al15 reported that the detection rate of behavioral problems in LBC was far greater in the Hui population (31.25%) than in the Han population (17.84%). The analysis showed that the potential reasons may be that most of the Hui population live in remote rural areas with a backward economy, resulting in some Hui parents retaining more traditional ideas and unscientific parenting behaviors. In addition, some families may have more children, which results in the children being unable to receive a good education. Previous studies have shown that children’s psychological behavioral problems are related to a variety of factors, including the child’s personality traits16 and self-concept,17–19 parenting behaviors,20,21 and family environmental factors,10,18 and trauma.22 Du et al23 showed that family structure and environment were closely related to children’s behavioral development and LBC, belonging to a particular family structure, experience more emotional24 and social behavioral problems.25 Existing results showed a sizable adverse effect of the exposure to parental migration on the health and educational outcomes of children.26 A previous study reported that parental migration had a negative impact on IBPs in children.27 Some researchers have shown that changes in the family structure in early childhood,28 poor family communication, and decreased positive maternal attention29 are statistically associated higher rates of IBPs in children.
This research is part of “twelfth five-year” National Science and Technology for Rural Areas Support Program (2012BAJ18B07-2), and we conducted an 8-week group psychological intervention on hui left-behind children with behavior problems selected from the baseline survey. Five years later, from 2018 to 2019, these children were followed up. The results showed that although the contact information was left at that time, some left behind children still did not get in touch, some left behind children repeatedly went to hospital because of suffering from Anxiety, Depression and Schizophrenia, et al, and some dropped out of school for depression and Schizophrenia. Nearly 10 years have passed and under our active appeal, local government have formulated many policies in favor of the left behind children of Hui nationality, however, because these left behind Hui children are located in the backward rural mountainous areas in Northwest China, their economy is backward and the available educational resources are relatively backward, their mental health have not been significantly improved. Last but not least, up to now, there are few research reports on the IBPs of Chinese Hui left behind children. There is still a lack of research with large sample sizes that could reveal the actual background of IBPs in this population.
The present study addresses the research gap by employing logistic regression analysis to examine the internalizing behaviors of the Hui LBC in the context of the Chinese Hui culture.
Given unscientific parenting behaviors and the high detection rate of behavioral problems in LBC of the Hui population, this study were designed to investigate the prevalence of IBPs among the LBC of the Hui nationality, to evaluate the potential influence of children’s individual characteristics and self-concept and the family environment on children’s mental health and to discuss the relationship between the multilevel risk factors and the incidence of IBPs in children, and to examine the IBPs of the LBC of the Hui nationality in the context of their unique culture. In addition, this study may provide a theoretical basis for more appropriate intervention measures and related ethnic policies for the LBC of the Hui nationality.
Methods
Participants
This research is a school-based cross-sectional study of LBC in the rural areas of the Ningxia Hui Autonomous Region spanning December 2012 to September 2013. It is part of the national science and technology program’s “integration and demonstration research on key technologies for the nutrition and health of rural children and mental patients” in the “12th Five Year Plan” for the rural areas. Subjects were selected using the multistage random cluster sampling method. First, two representative counties, Xiji and Haiyuan County, were selected in the southern mountainous area of the Ningxia Hui Autonomous Region. Second, all towns were coded according to a random digit in the target county, and five towns were randomly selected, namely Xinglong, Hongyao, Xinying, Xi’an, and Shutai townships. Third, all primary schools and junior middle schools in the five selected towns were separately coded. Given that the number of students in primary schools is lower than the number in junior middle schools, six primary schools and five junior middle schools were randomly selected. Finally, one class from each grade (1–6) was randomly selected from each of the six primary schools, and one class in each grade (7–9) was randomly selected from the five junior middle schools, resulting in a total of 51 classes being included in the study.
A total of 2000 students were recruited, and 1905 valid responses were received, with a response rate of 95.25%, of which 955 (50.13%) were children of the Hui nationality who were enrolled as the subjects for this study. These students were divided into the LBC group (n = 383) and the non-LBC group (n = 572). The inclusion criteria for the LBC group were: 1. staying in a rural area for more than half a year while one or both parents work outside of the area; 2. being taken care of by grandparents, relatives, neighbors, one parent, or siblings or looking after themselves; and 3. aged 6–16 y. The exclusion criteria were: 1. one or both parents working outside of the rural area for <6 months or 2. having a serious physical or mental illness.
Measures
Sociodemographic Characteristics
All the surveyed students were asked to fill out questionnaires about their socio-demographic characteristics, including their gender, age, nationality, academic performance, caregivers (including their educational level), and parents (including their educational level and occupation); the frequency of their contact with their parents; and the frequency of their contact with their teachers.
Internalizing Behavior Problems
Achenbach’s Child Behavior Checklist (CBCL) was developed by Achenbach, PhD, American Psychology and was initially published in 19761 and revised for the first time in 1983.30 There are three versions including the parent report version, teacher report version, and self-assessment of older children, of which the parent version has been the most widely tested and is the basis of the scale. This scale is applicable to children aged 4–16 y and has been widely used worldwide. China has also introduced and standardized the scale and formulated national and Hunan norms, and the Chinese translation has adequate psychometric properties.31,32 In this study, the parent report version included 113 items to identify the children’s behavioral problems, and it was mainly used to assess the types of behaviors exhibited by the children over the preceding six months by instructing parents or caregivers who were familiar with the children to report on the their behavioral problems on a three-point Likert scale (0 = not true, 1 = somewhat true or sometimes true, and 2 = very true or often true). Male and female students each had eight to nine specific syndromes, including schizoid, depressed, uncommunicative, obsessive-compulsive, somatic complaints, social withdrawal, hyperactivity, aggressive, and delinquent behavior. Through a principal component analysis of the above factors, two dimensions, namely IBPs and externalizing behavior problems, were obtained. We only calculated raw scores for the IBPs and their specific syndromes, which were used to compare with scores of the sample norm. The higher the score, the more obvious the behavior problem. Because the measured syndromes differed by age and gender groups according to the sample norm, we calculated and compared the syndrome scores separately. Internalizing problems focus on children’s emotional disturbances, including schizoid or depressed, social-withdrawal, and somatic complaints. If the child’s raw scores were above the upper threshold of the normal sample in at least one syndrome, they were considered to have behavioral disorders.32 The IBP score was calculated by adding the corresponding syndrome scores, in which repeated items were not cumulatively scored.
Parenting Style
The parenting style was measured by Egna Minnen av Barndoms Uppfostran (Chinese version) revised by Yue.33 Cultural differences between Chinese individuals and Western individuals are considered in the revised version, which consists of 66 items. There were 58 items relating to paternal rearing style, covering a total of six syndromes, including emotional warmth and understanding, punishment and strictness, over-interference, favoring subjects, refusal and denial, and over-protection, and 57 items relating to maternal rearing style, with a total of five syndromes, including emotional warmth and understanding, over-interference and over-protection, refusal and denial, punishment and strictness, and favoring subjects. The reliability of homogeneity of each subscale was 0.46–0.88, the split and half reliability was 0.50–0.91, the retest reliability was 0.67–0.89, and Cronbach’s alpha was 0.921. This scale has been used by many researchers who obtained good reliability and validity. The scale is suitable for all children, including children in single-parent families and those who are an only child, and allows for these situations by providing the option “unsuitable” in the answer sheet. Each item is scored on the following scale: never = 1, occasionally = 2, often = 3, always = 4, and unsuitable = 0. The scores were graded based on the sample norm mean ± standard deviation. If the factor score was less than the mean score minus the standard deviation, it was considered a low score and if it was greater than the mean score plus the standard deviation, it was considered a high score. All other scores were considered average scores.
Children’s Personality
Personality was assessed using the Junior Eysenck personality questionnaire, which was revised by Gong et al.34 This version has 88 true–false items for evaluating four subscales including extroversion–introversion (E), neuroticism (N), psychoticism (P), and lie (L), and part of the scale is reverse scored. We calculated the raw scores of each subscale and converted them into standard T points: standard T < 38.5 was a typical low score, 38.5–43.3 was a score that tended toward being low, 43.3–56.7 was an average score, 56.7–61.5 was a score that tended toward being high, and >61.5 was a typical high score. The Cronbach’s alpha was 0.70 for the total scale and 0.76, 0.76, 0.88, and 0.77 for E, P, N, and L, respectively.
Children’s Self-Concept
Children’s self-concept was measured using the Piers–Harris Children’s Self-concept Scale (PHCSS), which was introduced and revised by Su et al,33,35 with good reliability and validity. It is composed of 80 items, including 6 subscales of behavior, intelligence and school status, physical appearance and attributes, anxiety, popularity, and happiness and satisfaction. The scores for the answers are yes = 1 and no = 0, and some of the questions are reverse scored. The factor score was determined according to the mean score ± standard deviation, with scores that were less than the mean score minus the standard deviation being considered low scores, scores greater than the mean score plus the standard deviation being considered high scores, and the remaining scores being considered average. The higher the total score or the score of a factor, the stronger the self-concept or self-concept in that aspect. For example, a high behavior score indicates that the child is behaving appropriately, and a high anxiety score indicates that the child is in a good mood and not anxious. The half-reliability of the PHCSS scale was 0.82, and the Cronbach’s alpha was 0.858, which means that it is suitable for the measurement of children’s self-concept in China.
Procedures
We obtained approval and support from the local education bureau and the leaders of the investigated schools. The head teacher issued informed consent for the investigation to the WeChat parents’ group. Written informed consent, signed by the participants and their parents/guardians, was brought back to the school, and the head teacher then gave these to the researchers. After distributing the questionnaire to the students in the class, we asked the participants to complete the questionnaire within the prescribed time (60–80 min), and we checked and collected the questionnaires immediately. For grade one to grade three students, the investigator read each item to the subjects in neutral, non-suggestive language, asked them if they understood, and then asked for their answer. A CBCL was sent home with each student and given to the caregiver to fill out, after communication between the head teacher and the parents, and they were returned within three days. For students who were missing, or in cases where students’ responses were incomplete, a household supplementary survey was conducted. A total of 122 LBC of the Hui nationality were interviewed using the household survey. All the investigators received training in advance.
Statistical Analyses
SPSS 19.0 software for Windows was used for data analysis. The chi-squared test was used to compare the differences in enumeration data variables between the LBC and non-LBC groups, the independent sample t-test was used to compare the difference in measurement data between the two groups, and binary logistic regression was employed to analyze the risk factors of IBPs in the LBC of the Hui nationality. The value of p was used to assess the probability of each test, and α = 0.05 was used as the test standard.
Results
Sample Description
As seen in Table 1, a total of 955 Hui children were investigated, of which 383 were LBC (50.65% male), with children aged 6–11 y accounting for 29.77% (Mage = 12.86 ± 2.77 y), and 572 were non-LBC (46.98% male), with children aged 6–11 y accounting for 31.64% (Mage = 12.62 ± 2.49 y). There was no significant difference in the demographic characteristics between the LBC and non-LBC groups (see Table 1).
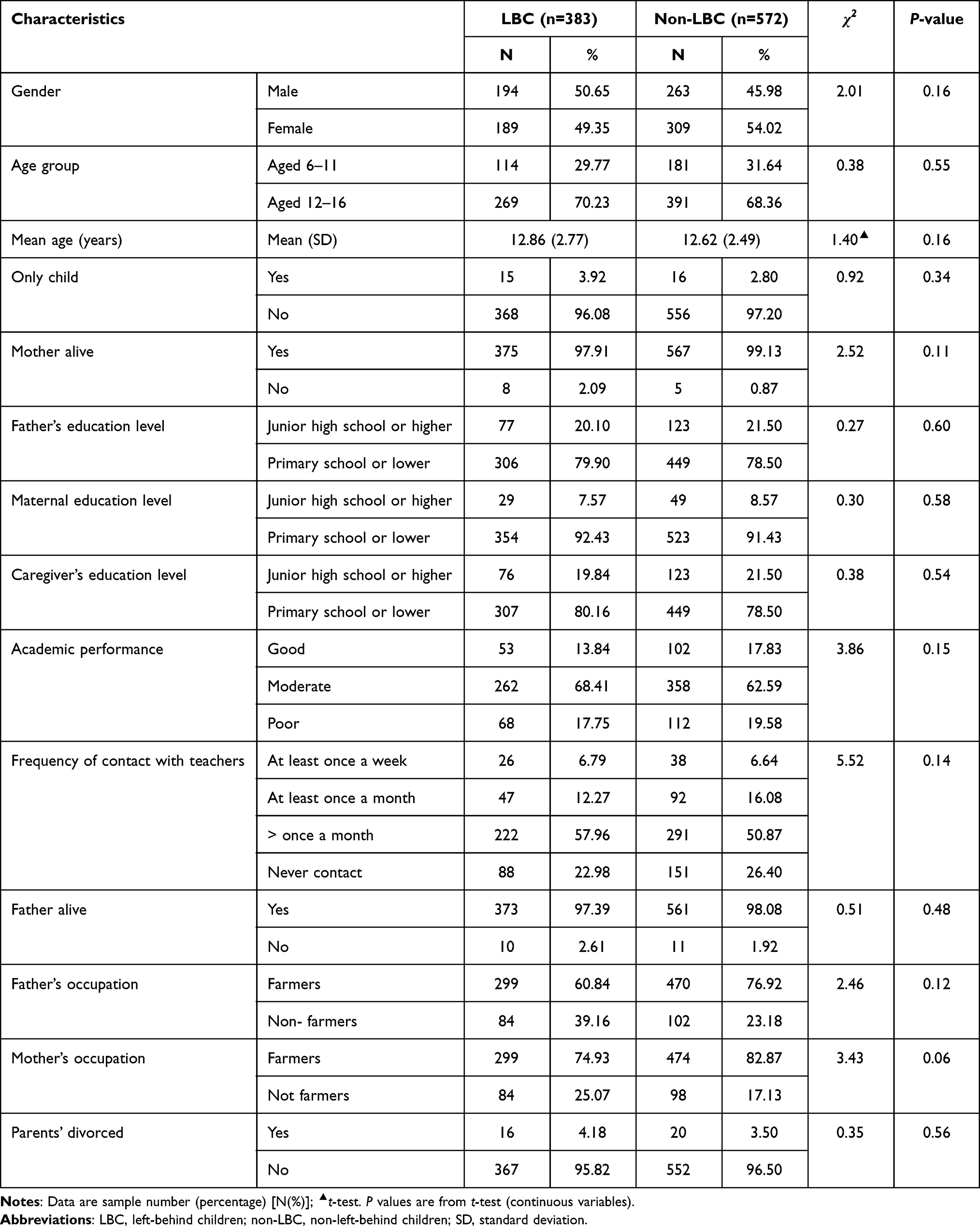 |
Table 1 The Demographic Characteristics Between Hui Nationality LBC and Non-LBC (N=955) |
The Prevalence of IBPs in Hui Children
Table 2 shows that the overall prevalence of IBPs in the 955 children of the Hui nationality was 19.58% (187 of 955), with a prevalence of 21.67% (83 of 383) in the LBC group and 18.18% (104 of 572) in the non-LBC group, but the difference was not significant (χ2 = 1.77, P = 0.18). However, the prevalence of IBPs among males in the LBC group (22.16%) was significantly higher than in the non-LBC group (14.07%; χ2 = 5.07, P = 0.02).
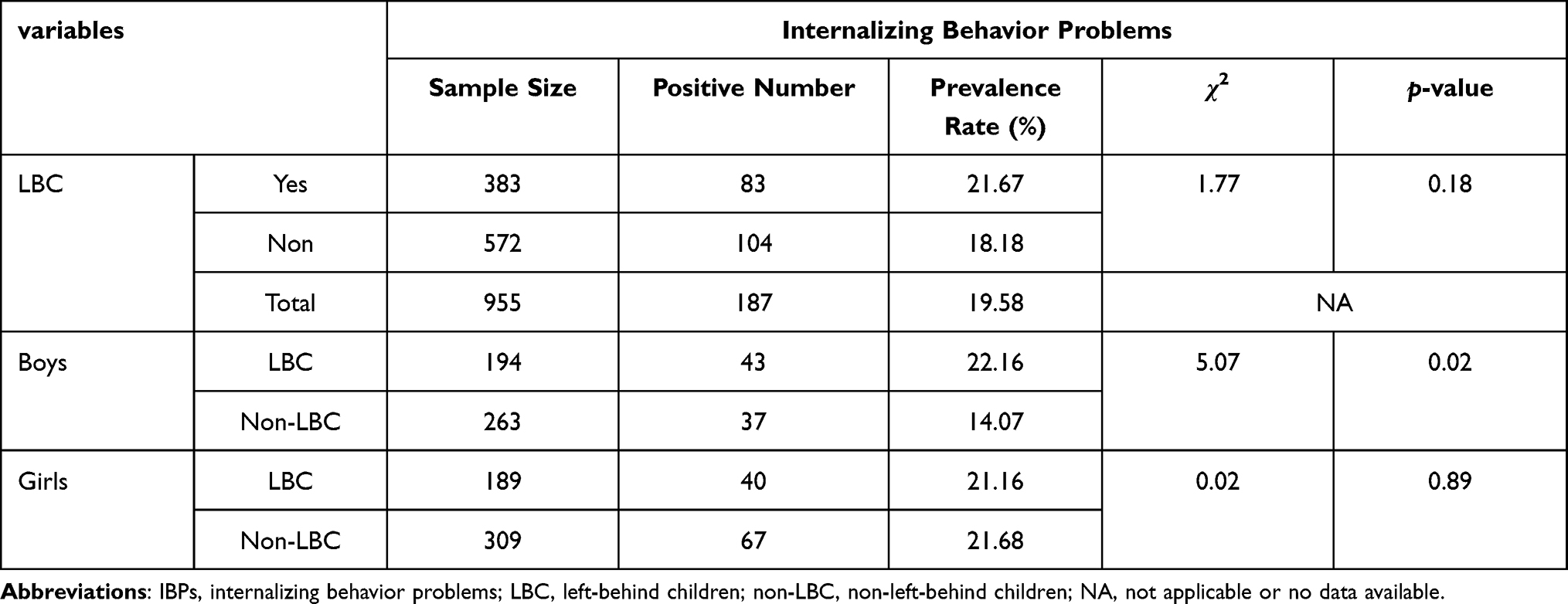 |
Table 2 Prevalence of IBPs Among Different Categories of Hui Nationality Children (N=955) |
Prevalence of IBPs and Specific Syndromes in Hui Children
As illustrated in Table 3, there was no significant difference in the prevalence of IBPs and specific syndromes in children aged 6–11 y between the LBC and non-LBC groups (P > 0.05), but, in children aged 12–16 y, there were significant differences in the prevalence of somatic complaints, uncommunicative, obsessive-compulsive, and internalizing behavior between the LBC and non-LBC groups (P < 0.05). In girls aged 12–16 y, there was no significant difference in the prevalence of internalizing behavior and specific syndromes between the LBC and non-LBC groups (P ≥ 0.05).
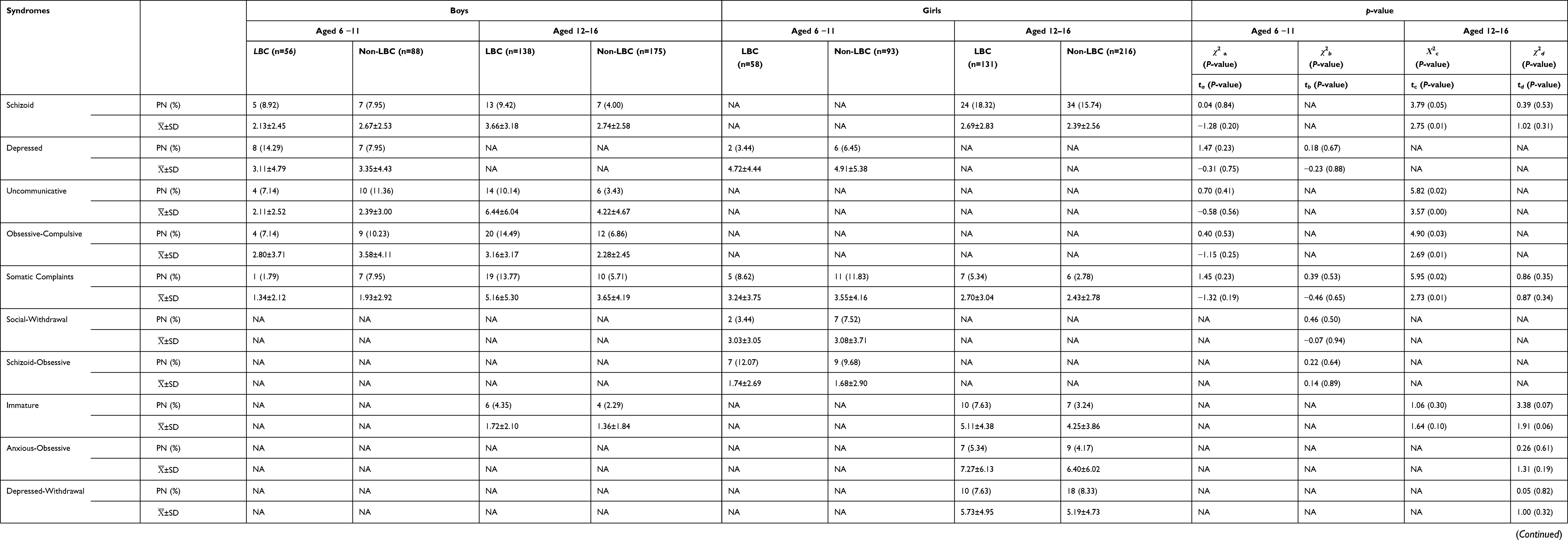 |
Table 3 Prevalence and Scores of IBPs and Specific Syndromes in Hui Nationality Children (N=955) |
Total Scores for IBPs and Specific Syndromes for Hui Children
As shown in Table 3, in children aged 6–11 y, there was no statistically significant difference in the total scores for IBPs and specific syndromes between the LBC and non-LBC groups (P > 0.05). However, in males aged 12–16 y, the scores for schizoid, somatic complaints, uncommunicative, obsessive-compulsive, and IBPs were higher in the LBC than in the non-LBC group (P < 0.05). However, in females aged 12–16 y, there was no significant difference in the total scores for IBPs and specific syndromes between the LBC and non-LBC group (P > 0.05).
Univariate Analysis Results
First, a chi-squared test was performed on the categorical variables that affected the incidence of IBPs, and it was found that no factors were related to the incidence of IBPs in the LBC of the Hui nationality (P > 0.05; see Table 4).
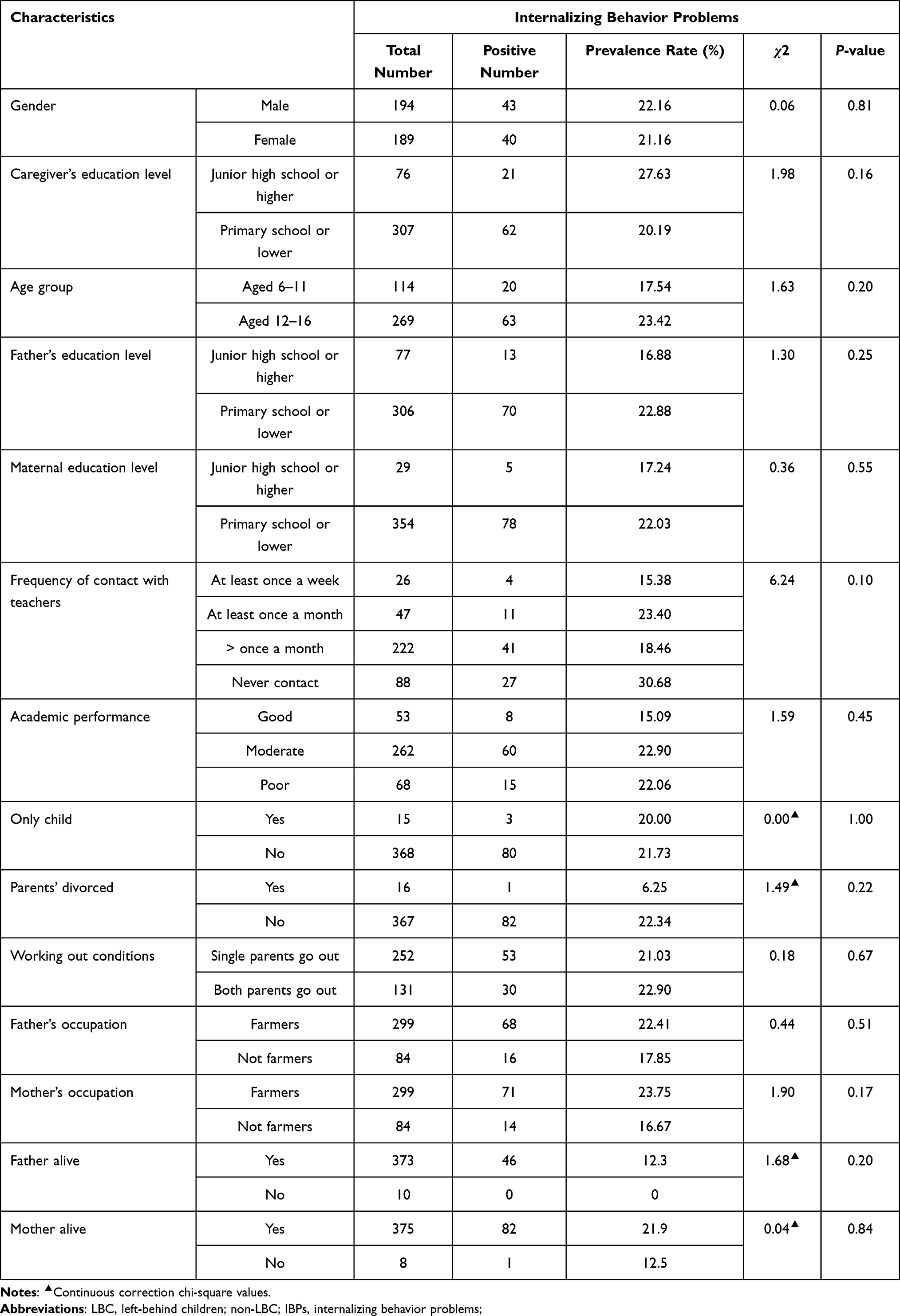 |
Table 4 Univariate Analysis of the Influence of General Demographic Data on IBPs of Hui Nationality LBC (N=383) |
Second, an independent sample t-test was conducted on the measurement data, and the results showed that behavior, anxiety, popularity, happiness and satisfaction, total score of self-concept, father’s punishment and strictness, the father favoring the subject, mother’s refusal and denial, mother’s punishment and strictness, the mother favoring the subject, E, and N were correlated with the incidence of IBPs in Hui LBC (see Table 5).
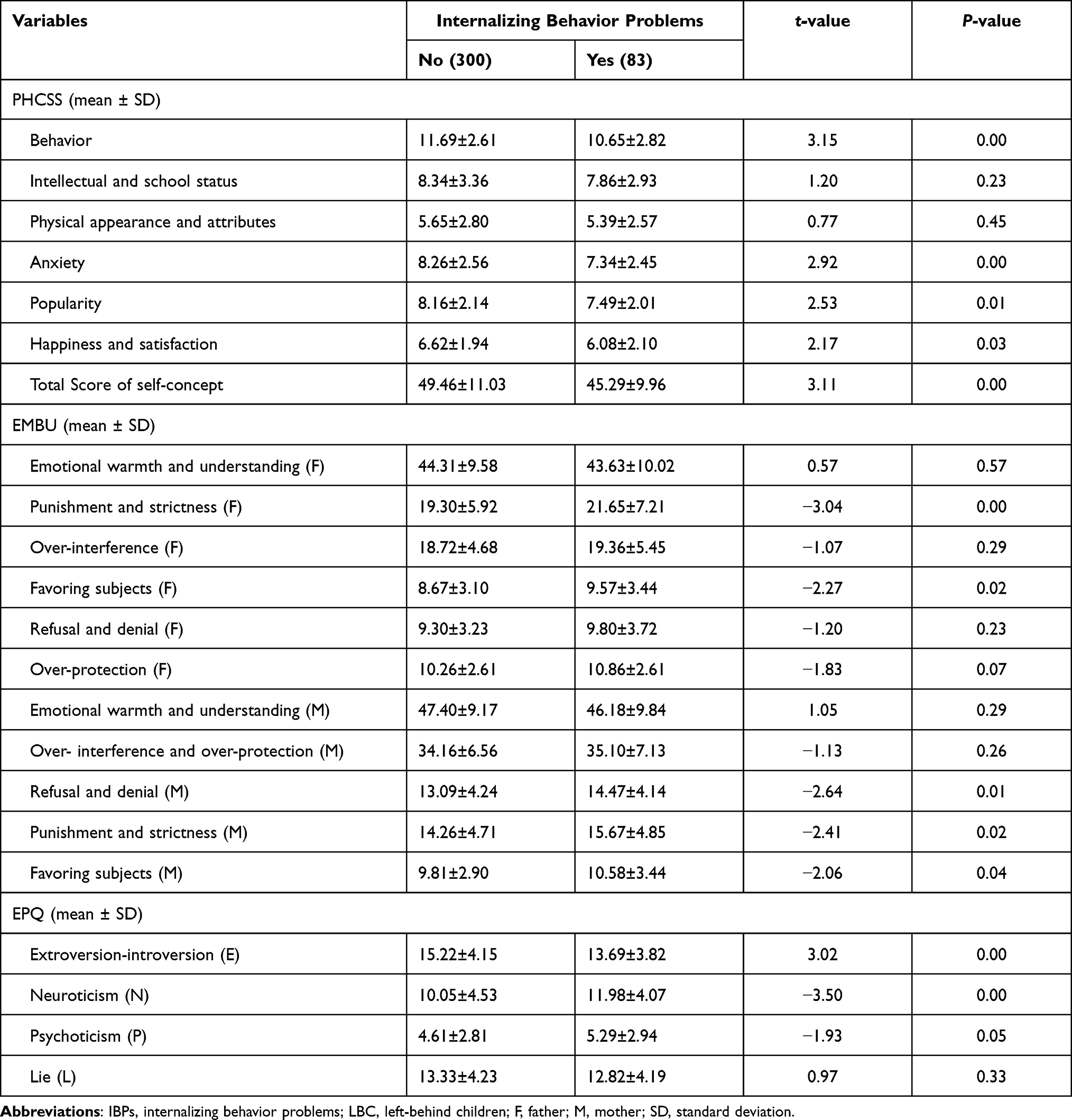 |
Table 5 Univariate Analysis of the Influence of Measurement Data on IBPs of Hui Nationality LBC (N=383) |
Multivariate Non-Conditional Logistic Regression Analysis Results
The total score for IBPs in the LBC of the Hui nationality was taken as the dependent variable (negative = 0 and positive = 1), and 12 factors with statistical significance in the univariate analysis including behavior, anxiety, popularity, happiness and satisfaction, total self-concept score, father’s punishment and strictness, the father favoring the subject, mother’s refusal and denial, mother’s punishment and strictness, the mother favoring the subject, E, and N were taken as the independent variables. The multivariate non-conditional logistic regression analysis, using forward conditions, the standard of alpha = 0.05, and exclusion criteria = 0.10, showed that the mother favoring the subject (odds ratio [OR] = 2.70), average levels of neuroticism (OR = 9.01), and high levels of neuroticism (OR = 8.44) were risk factors for IBPs in Hui LBC (see Table 6).
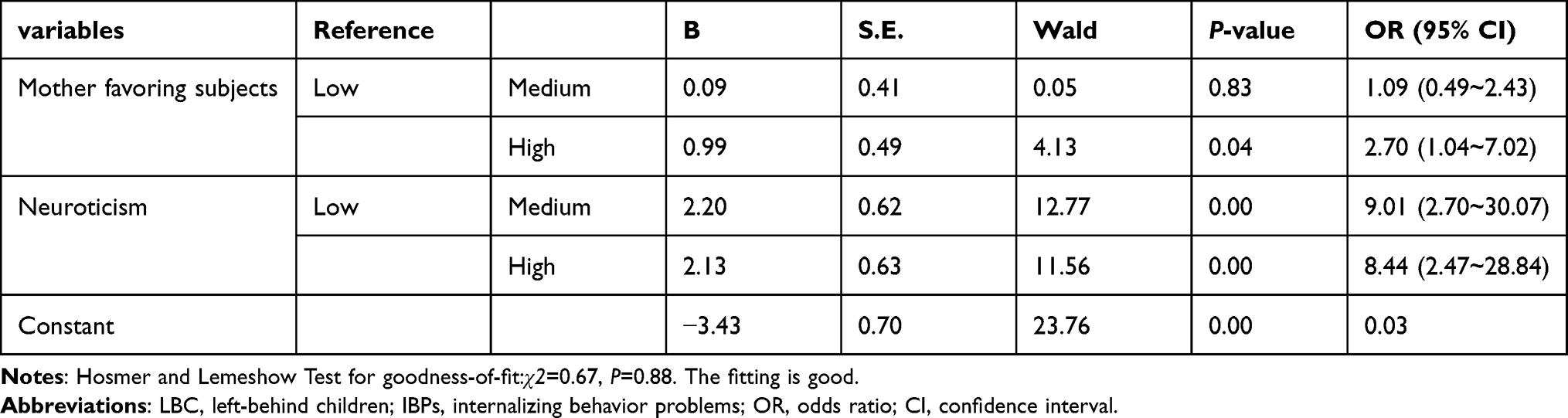 |
Table 6 Results of Multivariate Logistic Regression Analysis Predicting IBPs of Hui Nationality LBC (N=383) |
Discussion
This research showed that 187 out of 955 Hui children had IBPs, with a prevalence of 19.58%. Of the 383 Hui LBC, 83 had IBPs, with a prevalence of 21.67%. A total of 104 out of 572 Hui non-LBC had IBPs, with a prevalence of 18.18%. The prevalence of IBPs was not significantly different between the LBC and non-LBC groups. However, our findings showed that in Hui males, the prevalence of IBPs was higher in the LBC than the non-LBC group. In terms of IBPs, in our study, the prevalence in the LBC group was 21.67%, which is significantly higher than the prevalence of 6.3% in school-aged children in the rural areas of Harbin reported by Wu et al36 and higher than the prevalence of 15.19% in LBC reported by Hu et al.37 Our results showed that there was no significant difference in the prevalence of IBPs between males and females in the LBC group, which is not consistent with previous research results in which the incidence was higher in girls than in boys.6,38 We believe that this could be related to differences in ethnic and cultural background and social development.
Our findings showed that among Hui LBC aged 6–11 y, the three CBCL-specific syndromes with the highest prevalence in male subjects were IBPs (17.86%), depression (14.29%), and schizoid (8.92%) and in female subjects were IBPs (17.24%), schizoid obsessive (12.07%), and somatic complaints (8.62%). However, no significant difference was found in prevalence of specific syndromes and IBPs between Hui children aged 6–11 y in the LBC and non-LBC groups, which is not consistent with the findings reported by Liu et al.39
Among Hui LBC aged 12–16 y, the three CBCL-specific syndromes with the highest prevalence in the male subjects were IBPs (23.91%), obsessive-compulsive (14.49%), and somatic complaints (13.77%), and the four CBCL-specific syndromes with the highest prevalence in the female subjects were IBPs (22.90%), schizoid (18.32%), depressed-withdrawal (7.63%), and immaturity (7.63%). This study showed that with increasing age, the prevalence of IBPs among male Hui LBC increased, while the prevalence in female Hui LBC remained constant.
Our study results indicated that younger Hui LBC are less likely to have IBPs. The reason maybe that at this age, while they are in primary school, they have a simple and peaceful psychology with relatively few behavioral problems, and, because they are far away from their parents, they learn and master certain interpersonal skills. However, when children reach middle school and enter adolescence, they enter a stage of psychological rebellion.
Our findings showed that male Hui LBC aged 12–16 y scored higher on schizoid, somatic complaints, uncommunicative, obsessive-compulsive, and IBP scales than male Hui non-LBC, indicating that age of male Hui LBC were related to the behavioral problems, which is consistent with results reported by Xu.40 The reason for this may be related to boys’ physiological characteristics, personality traits, and family educational environments. After entering junior high school, because parents and teachers pay too much attention to children’s academic performance, the learning pressure increases, which may have an impact on the child’s psyche. In addition, due to parents’ migrant work, as the children get older, the lack of parental care and discipline causes an increase in their psychological needs, which is consistent with the increasing trend of emotional and behavioral problems as children enter adolescence.41
The results of the univariate analysis showed that children’s gender, caregivers’ educational level, parents’ educational level, parents’ marital status, frequency of contact with teachers, and parents’ work situation did not seem to affect the IBPs of Hui LBC, which is inconsistent with the existing research.42,43 One possible reason is that the subjects of this study are Hui LBC residing in poor mountainous areas that are influenced by the Hui national culture, which may have a certain regulatory effect on IBPs, or it may be related to the small sample size of this study. These results suggest that they may play an indirect role by influencing the development of a child’s personality and self-concept, but the exact mechanism of this is unknown, and the underlying associations deserve further study. However, this research shows that behavior, anxiety, popularity, happiness and satisfaction, total score of self-concept, father’s punishment and strictness, the father favoring the subject, mother’s refusal and denial, mother’s punishment and strictness, the mother favoring the subject, E, and N are related to the IBPs of Hui LBC.
The multivariate logistic regression analysis showed that the more the mothers preferred the subjects, the more neurotic the children were (above average score), which is an independent risk factor for IBPs in Hui LBC but is not completely consistent with the independent factors influencing the overall incidence of behavioral problems in the Hui LBC in our study.44
The results of this study suggest that negative parenting styles, such as mothers favoring the subjects greatly, are positively related to IBPs in Hui LBC. The more unstable the children’s emotions are,45 the more likely they are to have IBPs dominated by anxiety and depression. The analysis suggests that an overindulgence of a child by their mothers may lead to the child’s lack of self-restraint and independence, thus causing their behavior to deviate from the norm.46 Family is not only an important carrier of culture but also the first learning environment that a child is exposed to. In addition, studies of intergenerational psychiatry demonstrate the negative effects of parental exposure to trauma on psychiatric outcomes in the next generation.47 Parenting style is considered to be a specific educational medium through which Chinese culture and social values are passed on to children. As a result of the impact that traditional Chinese culture and the modern education system have on parents, a hierarchy still exists between parents and children in most Chinese families. Hui culture is an ethnic culture formed on the basis of Islamic culture and traditional Chinese culture. Mosque, market, and the Hui community are interlinked and interdependent and constitute the three important cornerstones of Hui life, ie, worship, commerce, and residence.48 In families with plenty of time and a strong religious atmosphere, most Muslim young people can enrich their understanding of their religion through religious activities that are consciously guided by their parents’ words and deeds because religious parents are more likely to manifest their religious values and beliefs through their daily interactions with their children.49 This culture subtly influences Hui children through family and social education, in which they may no longer adhere to their own views in the face of conflicts with others but unconsciously compromise. With the deepening of China’s reform and opening up, the construction of the market economy, and the influx of a large amount of labor into the cities, the pattern of mosque, market, and Hui community has been destroyed,50 which affects the family educational model and the belief system of the Hui children, resulting in confusion, anxiety, and depression.51
Our study had several limitations. First, due to the limitations of the conditions, a single sample population was selected, involving only five township schools in two project demonstration counties, which limits the generalizability of the study results and affects the external validity of this study. Second, we collected information from caregivers or parents about children’s behavioral problems, which could lead to bias. Third, the scores of the nationwide norm sample used in this study were collected through an epidemiology survey in 1992, which could have led to limitations when it was used to assess children’s behavioral problems in the current study, as China has undergone dramatic development over the past decades. Third, when getting into middle school, children and adolescents in a stage of psychological rebellion are prone to undergo the IBPs-related adversity and trauma, which were not evaluated in our study. Finally, the research object of this paper is mainly LBC in school and does not consider other children who have dropped out of school. In addition, this study is a cross-sectional survey conducted from 2012 to 2013, and it is impossible to obtain detailed information about the complete development process and the overall trends of IBPs over time in Hui LBC. Almost 10 years have passed, and, under the intervention of some government policies, IBPs and their influencing factors on the Hui LBC in rural China may have changed. However, their mental health status is still not optimistic, and, to date, there is no other relevant research paper on this topic, which is a further limitation of this paper. Therefore, to provide more compelling evidence concerning the factors influencing IBPs in Chinese LBC of the Hui nationality, a longitudinal prospective study is recommended to explore the mechanism of how these risk factors lead to IBPs at an individual and group level.
Conclusion
In summary, this study showed that the incidence of IBPs in Hui males was higher in the LBC than in the non-LBC group. The findings suggested that IBPs among male Hui LBC in rural China are related to parental migration. Mothers showing a strong preference for the subjects and medium and high levels of neuroticism in the subjects are independent risk factors for the occurrence of IBPs in Hui LBC. Positive measures should be taken to prevent IBPs in male Hui LBC in the rural areas of China, and it is important to consider personality development and parental rearing patterns.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Beijing First Hospital of Integrated Traditional Chinese and Western Medicine. This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participant’s guardians.
Funding
This research was financially supported by grants from the “twelfth five-year” National Science and Technology for Rural Areas Support Program (2012BAJ18B07-2).
Disclosure
Xue Yu and Ling-Ling Wang are co-first authors for this study. The authors declare that they have no conflicts of interest in this work.
References
1. Achenbach TM. The child behavior profile: I. Boys aged 6–11. J Consult Clin Psychol. 1978;46(3):478–488. doi:10.1037/0022-006X.46.3.478
2. Cosgrove VE, Rhee SH, Gelhorn HL, et al. Structure and etiology of co-occurring internalizing and externalizing disorders in adolescents. J Abnorm Child Psychol. 2011;39(1):109–123. doi:10.1007/s10802-010-9444-8
3. Biebl SJ, Dilalla LF, Davis EK, Lynch KA, Shinn SO. Longitudinal associations among peer victimization and physical and mental health problems. J Pediatr Psychol. 2011;36(8):868–877. doi:10.1093/jpepsy/jsr025
4. Nelson TD, Smith TR, Duppong Hurley K, Epstein MH, Thompson RW, Tonniges TF. Association between psychopathology and physical health problems among youth in residential treatment. J Emot Behav Disord. 2012;21(2):150–160. doi:10.1177/1063426612450187
5. Dekker MC, Ferdinand RF, Van Lang NDJ, Bongers IL, Van Der Ende J, Verhulst FC. Developmental trajectories of depressive symptoms from early childhood to late adolescence: gender differences and adult outcome. J Child Psychol Psychiatry. 2007;48:657–666. doi:10.1111/j.1469-7610.2007.01742.x
6. Narusyte J, Ropponen A, Alexanderson K, Svedberg P. Internalizing and externalizing problems in childhood and adolescence as predictors of work incapacity in young adulthood. Soc Psychiatry Psychiatr Epidemiol. 2017;52(9):1159–1168. doi:10.1007/s00127-017-1409-6
7. Duan CR, Zhou FL. Study on the situation of left behind children in China. Population Res. 2005. 29 (1):29-36.
8. The ministry of civil affairs of China. Available from: http://lyzx.mca.gov.cn:8280/consult/showQuestion.jsp?MZ=7910978776.
9. Zheng TG, Wang SM, Zhou SH, et al. Analysis of intervention effect on left-children students from different guardian. Chin J School Health. 2010;31(12):1459–1460.
10. Bush NR, Wakschlag LS, LeWinn KZ, et al. Family environment, neurodevelopmental risk, and the Environmental Influences on Child Health Outcomes (ECHO) initiative: looking back and moving forward. Front Psychiatry. 2020;19(11):547. doi:10.3389/fpsyt.2020.00547
11. Zhao C, Wang F, Li L, Zhou X, Hesketh T. Long-term impacts of parental migration on Chinese children’s psychosocial well-being: mitigating and exacerbating factors. Soc Psychiatry Psychiatr Epidemiol. 2017;52(6):669–677. doi:10.1007/s00127-017-1386-9
12. Paus T, Keshavan M, Giedd JN. Why do many psychiatric disorders emerge during adolescence? Nat Rev Neurosci. 2008;9(12):947–957. doi:10.1038/nrn2513
13. Merikangas KR, He JP, Burstein M, et al. Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2010;49(10):980–989. doi:10.1016/j.jaac.2010.05.017
14. Zhao MM, Li H, Li J, et al. Studying on the influence of migrant parents on mental health of their left-behind children in rural China. Chin HealthService Manage. 2012;29(1):60–63.
15. Feng YT, Hu CZ, Li QL, Liu MM, Yu X, Dai XY. Detectable rate and correlative factors of behavior problems among Hui nationality left-behindchildren in rural district of Ningxia. Chin J Behavioral Med Brain Sci. 2013;22(2):157–159.
16. Van Heel M, Bijttebier P, Colpin H, et al. Investigating the interplay between adolescent personality, parental control, and externalizing problem behavior across adolescence. J Res Pers. 2019;81:176–186. doi:10.1016/j.jrp.2019.06.005
17. Wang X, Ling L, Su H, Cheng J, Jin L, Yh S. Self-concept of left-behind children in China: a systematic review of the literature. Child Care Health Dev. 2015;41(3):346–355. doi:10.1111/cch.12172
18. Ybrandt H. The relation between self-concept and social functioning in adolescence. J Adolesc. 2008;31(1):1–16. doi:10.1016/j.adolescence.2007.03.004
19. Shen JQ, Wu HJ, Chen HW. Research on correlations between aggressive behavior and rearing pattern, family environment and self-concept. Chin J Behavioral Med Sci. 2006;15(8):744–745.
20. Burlaka V. Externalizing behaviors of Ukrainian children: the role of parenting. Child Abuse Negl. 2016;54:23–32. doi:10.1016/j.chiabu.2015.12.013
21. Park S, Dotterer AM. Longitudinal associations of family stressors, fathers’ warmth, and Korean children’s externalizing behaviors. J Fam Psychol. 2018;32(8):1036–1045. doi:10.1037/fam0000486
22. Posner J, Eilenberg J, Friedman JH, Fullilove MJ. Quality and use of trauma histories obtained from psychiatric outpatients: a ten-year follow-up. Psychiatr Serv. 2008;59(3):318–321. doi:10.1176/ps.2008.59.3.318
23. Du YS, Tang HQ, Bao YJ, Wang YW, Zheng WZ. Behavior problems of children in special families. Chin Ment Health J. 2002;16(1):41–43.
24. Wang -Y-Y, Xiao L, Rao -W-W, et al. The prevalence of depressive symptoms in ‘left-behind children’in China: a meta-analysis of comparative studies and epidemiological surveys. J Affect Disord. 2019;244:209–216. doi:10.1016/j.jad.2018.09.066
25. Tang W, Wang G, Hu T, et al. Mental health and psychosocial problems among Chinese left-behind children: a cross-sectional comparative study. J Affect Disord. 2018;241:133–141. doi:10.1016/j.jad.2018.08.017
26. Meng X, Yamauchi C. Children of migrants: the cumulative impact of parental migration on children’s education and health outcomes in China. Demography. 2017;54(5):1677–1714. doi:10.1007/s13524-017-0613-z
27. Zhao J, Li Q, Wang L, Lin L, Zhang W. Latent profile analysis of left-behind adolescents’ psychosocial adaptation in rural China. J Youth Adolesc. 2019;48(6):1146–1160. doi:10.1007/s10964-019-00989-1
28. Womack SR, Taraban L, Shaw DS, Wilson MN, Dishion TJ. Family turbulence and child internalizing and externalizing behaviors: moderation of effects by race. Child Dev. 2019;90(6):e729–e744. doi:10.1111/cdev.13103
29. Burlaka V, Wu Q, Wu S, Churakova I. Internalizing and externalizing behaviors among Ukrainian children: the role of family communication and maternal coping. J Child Fam Stud. 2019;28(5):1283–1293. doi:10.1007/s10826-019-01377-w
30. Achenbach TM, Edelbrock CS. Manual for the Child Behavior Checklist and Revised Child Behavior Profile. Vermont: University of Vermont, Department of Psychiatry; 1983.
31. Su LY, Li XR, Wan GB, Yang ZW, Luo XR. Hunan norm of Achenbach child behavior checklist. Chin J Clinical Psychol. 1996;4(1):24-28+64.
32. Xin RE, Tang HQ. Investigate on 24013 city children’s behavioral problems in 26 units of 22 provinces. Shanghai Arch Psychiatr. 1992;new4(1):47–55.
33. Yue DM, Li MG, Jin KH, Ding BK. Parenting styles: a preliminary revision of EMBU and its application in neurotic patients. Chin Ment Health J. 1993;3:
34. Gong YX. Revised Eysenck Personality Questionnaire Handbook. Changsha: Hunan Medical college; 1986:2.
35. Su LY, Luo XR, Zhang GS, Xie GR, Liu YZ. Norms of the piers-harris children’ s self-concept scale of Chinese urban children. Chin Ment Health J. 2002;16(1):31–34.
36. Wu LJ, Liu AS, Tao YC, Zhang LP, Wu K, Chen L. An epidemiological survey of behavioral problems among school-aged children in Harbin. Chin J School Health. 2002;23(6):488–489.
37. Hu H, Gao J, Jiang H, et al. A comparative study of behavior problems among left-behind children, migrant children and local children. Int J Environ Res Public Health. 2018;15(4):655. doi:10.3390/ijerph15040655
38. Jamnik MR, DiLalla LF. Health outcomes associated with internalizing problems in early childhood and adolescence. Front Psychol. 2019;10:60. doi:10.3389/fpsyg.2019.00060
39. Liu SM, Wang RZ, Wang YH, et al. epidemiological investigation of behavioral problems and the relevant factors in children aged 6~11 years in Shandong province. J Psychiatry. 2018;31(4):272–275.
40. Xu WM, Tang JL, Wu D, Xu XY, Yang L. Research on present situation of behavior disorders of left-behind children in the countryside of Anhui province. J Appl Clin Pediatr. 2007;22(11):852–853.
41. Wang XL, Li PF, Peng Y, Li K. Emotional and behavioral problems of children-adolescents aged 4–18 in Changsha. Chin Ment Health J. 2012;26(10):775–779.
42. Zhao XX, Chen JQ, Feng YN, Jin YC, Liu CF, Yu PY. Investigation on behavioral problems and influencing factors among primary school students in rural areas of Shandong province. Chin J Child Health Care. 2015;23(5):522–525.
43. Zhou YM, Qi YJ, Zhang ZX, He F, Zheng Y. Analysis of incidence and influencing factors of psychological behavior problems of left-behind children aged 4–6 in rural areas. J Clin Psychiatry. 2019;29(3):157–160.
44. Yu X, Dai XY, Li QL, et al. Psychological behavior problems and influencing factors in rural Muslim left-behind children. Chin J Public Health. 2014;30(7):857–860.
45. Zhang WY, Tan YY, Wu JD, Tang ZH. Behavioral problems and personality characteristics of some left-behind children in Guangxi. South China Prev Med. 2009;35(5):
46. Wang XZ, Zheng Z, Tang YH, Yang HY, Wang JW. Study on the relationship between behavior problems and personality and parenting style of childrenaged 10 ~ 11 years. Chin J Behavioral Med Sci. 2006;15(12):1114–1116.
47. Duarte CS, Monk C, Weissman MM, Posner J. Intergenerational psychiatry: a new look at a powerful perspective. World Psychiatry. 2020;19(2):175–176. doi:10.1002/wps.20733
48. Ji FT. The fundamental characteristics of Hui culture. Northwest Ethnic Studies. 2018;1:96–103.
49. Bornstein MH, Putnick DL, Lansford JE, et al. ‘Mixed blessings’: parental religiousness, parenting, and child adjustment in global perspective. J Child Psychol Psychiatry. 2017;58(8):880–892. doi:10.1111/jcpp.12705
50. Li JL, Ma CQ. Family education and the formation of Hui culture concept. J Northwest Unive. 1997;27(3):118–121.
51. Wang J. Research on the relationship between cultural alienation, cultural identity, acculturation pressure and coping style of Hui adolescents. Southwest Unive. 2012:8.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.