Back to Journals » Clinical Ophthalmology » Volume 19
Internal Limiting Membrane Flap Enhances Macular Hole Closure Rates in Highly Myopic Eyes: A Case-Control Study
Authors Poh SSJ ![]() , Tsai ASH, Chou HD
, Tsai ASH, Chou HD ![]() , Chee ML, Wang CT, Ting DSW
, Chee ML, Wang CT, Ting DSW ![]() , Lai CC, Lee SY
, Lai CC, Lee SY
Received 16 January 2025
Accepted for publication 28 May 2025
Published 8 August 2025 Volume 2025:19 Pages 2615—2624
DOI https://doi.org/10.2147/OPTH.S517929
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Stanley SJ Poh,1,2 Andrew SH Tsai,1,2 Hung-Da Chou,3,4 Miao Li Chee,5 Chung-Ting Wang,3 Daniel SW Ting,1,2,5 Chi-Chun Lai,3,4 Shu Yen Lee1
1Singapore National Eye Centre, Singapore; 2Ophthalmology and Visual Sciences Academic Clinical Program, Duke-NUS Medical School, Singapore; 3Department of Ophthalmology, Chang Gung Memorial Hospital, Linkou Main Branch, Taoyuan, Taiwan; 4College of Medicine, Chang Gung University, Taoyuan, Taiwan; 5Singapore Eye Research Institute, Singapore
Correspondence: Shu Yen Lee, Surgical Retina Department, Singapore National Eye Centre, 11 Third Hospital Avenue, 168751, Singapore, Tel + 65-65757281, Email [email protected]
Purpose: To compare the anatomical and functional outcomes of macular hole (MH) surgery in high myopia (HM) versus non-HM eyes.
Patient and Methods: This is a retrospective case-control study of patients who underwent MH repair between 2018 and 2022. HM was defined by axial length (AL) ≥ 26 mm. MH size, macular curvature and foveoschisis were graded. Surgical technique was divided into internal limiting membrane (ILM) peel or flap. Post-operative best corrected visual acuity (BCVA) and anatomical outcomes including hole closure, restoration of outer retinal layers, presence of foveal gliosis or foveal detachment were assessed at post-operative one, three, six and twelve months.
Results: Thirty-four HM eyes were matched 1:1 to 34 out of 201 non-HM eyes with using gender, age, MH size and concurrent phacoemulsification as covariates. Mean AL in the HM group was 28.46 ± 2.01 mm, ranging from 26.03 to 32.83 mm. MH size was 366± 183 μm and 386± 199 μm in HM and non-HM groups (p=0.667). BCVA and restoration of outer retinal layers were comparable between groups at all time points. Initial hole closure rate was comparable, with 29 (85.3%) in HM group vs 30 (88.2%) in non-HM eyes, p=0.720. One eye in the HM group re-opened 10 months post-operatively. Proportion of eyes with non-closure was higher in those who underwent ILM peel vs flap [7/34 (20.5%) vs 0/34 (0%), p=0.022]. Smaller MH was associated with better closure rate (OR 0.99, 95% CI 0.99– 1.00). AL and macular curvature were not associated with hole closure (OR 0.91, 95% CI 0.72– 1.15; OR 1.01, 95% CI 0.99– 1.02 respectively). Larger MH was associated with poorer final BCVA (β=0.010, 95% CI 0.007– 0.014).
Conclusion: Anatomical success was comparable between HM and non-HM eyes. Higher surgical success was associated with smaller MH size and ILM flap, but not influenced by AL, macular curvature or foveoschisis.
Keywords: macular hole, internal limiting membrane peel, internal limiting membrane flap, high myopia
Introduction
Surgical repair of macular holes (MH) in high myopia (HM) eyes is typically associated with lower surgical success when compared to non-HM eyes.1–4 The pathogenesis of MH in HM is complex and multifactorial, involving not only tangential traction but also anteroposterior traction resulting from axial elongation and the development of retinoschisis and posterior staphyloma.5,6 Furthermore, HM eyes are at increased risk of macular atrophy and myopic choroidal neovascularization, both of which contribute to a poorer visual prognosis.7
The conventional surgical approach for MH repair involved pars plana vitrectomy, internal limiting membrane (ILM) peeling and gas tamponade, achieving success rates ranging from 60% to 90% in HM eyes.1–4 One study reported a 100% closure rate in a small sample of 24 myopic MH cases by using ILM peeling along with platelet concentrate and sulfur hexafluoride, though anatomical success was measured biomicroscopically rather than by optical coherence tomography (OCT).8 In eyes with extremely long axial length (AL) of >30 mm, anatomical closure rates can be as low as 0%.4 The ILM peel aids in the complete removal of the cortical vitreous which releases traction. However, it may not be sufficient to address the unique anatomical challenges of HM eyes, particularly the additional tension caused by posterior staphyloma.
Since the introduction of ILM flap technique, outcomes in MH repair in HM eyes have improved, with closure rates reported between 88% and 100%, even in cases of extreme myopia.9–13 The ILM flap acts as a scaffold, promoting glial cell proliferation, which enhances hole closure.10,11 A meta-analyses reported closure rates between 91.8% and 97.1% with this technique, along with visual acuity (VA) improvements between 66.2% and 77.3%.14 However, while the closure rate has significantly improved, the presence of ILM flap may induce fibrosis over time, potentially limiting long-term visual recovery.15 One study suggests that conventional ILM peeling may instead result in better functional outcomes for large MH.16
Multiple retrospective studies including meta-analysis have evaluated outcomes in HM eyes, but there is limited literature directly comparing outcomes between HM and non-HM eyes in a case-control fashion.17 To address this gap, we conducted a case-control comparative study to assess and compare the anatomical functional outcomes of MH repair in HM versus non-HM eyes, utilizing standard surgical techniques of both ILM peeling or ILM flap. We also aim to investigate the association of posterior staphyloma and foveoschisis with surgical success.
Materials and Methods
This is a retrospective, multi-surgeon, case-control study of patients who underwent full-thickness MH repair consecutively between 2018 and 2022 in Singapore National Eye Centre (SNEC). Cases that had ocular biometry data for on axial length (AL) were included. HM is defined by AL of ≥26.0mm. Although some studies adopt higher cutoffs of ≥26.5mm, the ≥26.0mm threshold is widely accepted in clinical practice and was chosen to ensure adequate case inclusion, given the rarity of MH formation in HM eyes.7,18 Refractive errors was not included in the HM definition, as the study specically focused on the effect of axial myopia on hole closure. Cases of retinal detachment, secondary or recurrent MH, retinal pathologies such as previous retinal detachment, choroidal neovascularization or macular atrophy were excluded. Surgical techniques other than ILM peeling or ILM flap were also excluded. The control group consists of 201 consecutive MH surgery in non-HM eyes and was matched 1:1 using covariates age, gender, MH size, and whether combined cataract surgery was performed. This study was conducted according to the tenets of Declaration of Helsinki and was granted approval by SingHealth Centralized Institutional Review Board, which governs research conducted at SNEC, a member institution under SingHealth. Informed consent was waived due to the retrospective nature of the study, and all patient data were anonymized to ensure confidentiality.
Baseline characteristics of patients including age, gender, medical or ocular history were recorded. All patients underwent pre-operative ophthalmic examination that included best corrected visual acuity (BCVA) and axial length (AL) measurement. Diagnosis of MH was confirmed using OCT (Heidelberg Engineering, Heidelberg, Germany), and the MH size was determined by the minimum linear distance between the hole edges that is parallel to the retinal pigment epithelium (RPE). Associated features such as perihole fluid, subretinal fluid and foveoschisis were recorded. Macular curvature was graded using an OCT-based measurement technique previously described.19 The OCT image is first scaled to 1:1 pixel, and a best fit circle was drawn to approximate the macular curvature. Curvature (mm−¹) is defined as the reciprocal of the radius of the best-fit circle.
Surgical repair of MH was performed using pars plana vitrectomy, followed by either ILM peeling or flap creation, and subsequent gas tamponade. MembraneBlue-Dual (DORC International, Zuidland, Netherlands) was used intraoperatively to enhance ILM visualization. The choice between ILM peeling or flap techniques was determined at the surgeon’s discretion. In the ILM peeling group, standard complete ILM removal was performed, whereas in the ILM flap group, an inverted ILM flap technique was performed in majority of cases. Gas tamponade was achieved using air, sulfur hexafluoride (SF6), hexafluoroethane (C2F6) or octafluoropropane (C3F8) according to case requirements. Phakic eyes were considered for combined phacoemulsification and intraocular lens implant at the time of vitrectomy.
Examination findings and OCT at post-operative months 1, 3, 6 and 12 were reviewed. BCVA based on refraction was recorded if available, otherwise, the pinhole VA of that visit was recorded. In terms of anatomical outcomes, complete hole closure was defined as approximation of the inner edges and no exposure of the RPE on the OCT. Some of these cases may have residual interruption of the inner or outer retinal layers. The restoration of outer retinal layer in the external limiting membrane (ELM), ellipsoid zone (EZ), and interdigitation zone (IZ) were measured. Presence of foveal gliosis or foveal detachment was also recorded.
All statistical analysis were performed using Stata (Version 15.0, StataCorp, College Station, Texas) and R programming (Version 4.3.2). Propensity score was estimated using covariates which include age, gender, concurrent cataract surgery and MH size. Based on the estimated propensity scores, 1:1 nearest neighbor matching was applied to match the controls to the cases. VA, initially recorded in Snellen, was converted to logMAR for analysis. Comparison of baseline demographic, systemic and ocular characteristics between HM vs non-HM eyes were performed using chi-squared tests and independent T-tests for categorical and continuous variables, respectively. Linear mixed effect models were applied to evaluate the changes in BCVA between HM and non-HM eyes over time, and the association of various risk factors with VA. Logistic regression analyses were applied to examine the association of risk factors with hole closure. All reported P values were two-sided, and statistical significance was set at P < 0.05.
Results
Table 1 presents the baseline characteristics comparing HM eyes with non-HM eyes. Thirty-four HM eyes were matched 1:1 to 34 out of 201 non-HM eyes using gender, age, MH size and concurrent phacoemulsification covariates. AL was significantly longer in the HM group (28.46 ± 2.01 mm) compared to the non-HM group (23.73 ± 1.12 mm, p<0.001). Similarly, the presence of foveoschisis and macular curvature was significantly higher in the HM group (p=0.015 and p<0.001, respectively). The pre-operative VA was comparable between the two groups (0.84 ± 0.38 and 0.85 ± 0.30 logMAR, respectively, p=0.882). The use of surgical techniques of either ILM peeling or ILM flap was equally distributed in both groups.
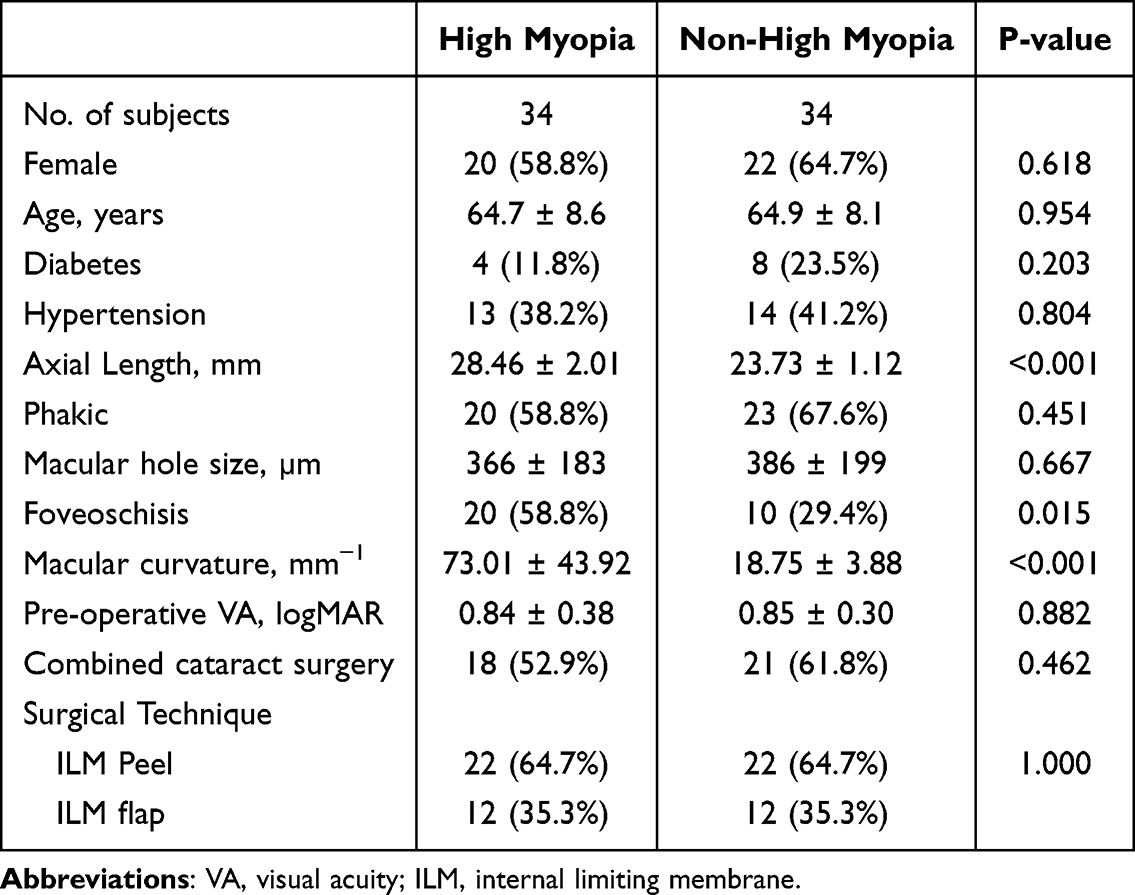 |
Table 1 Baseline Characteristics of Study Population |
Table 2 shows the post-operative outcomes of MH repair between HM and non-HM eyes. Primary hole closure had comparable results, with rates of 85.3% and 88.2%, respectively (p=0.720). One eye (2.9%) in HM group had hole re-opening at 10 months post-operatively, while no reopening was observed in the non-highly myopic group (p=0.314). All eyes with ILM flap achieved 100% closure rate compared to 79.5% closure rate in ILM peel group (p=0.022). Both groups experienced BCVA improvement over time (Table 2 and Figure 1), but there were no statistically significant differences in BCVA at any postoperative time point, with the overall change in VA at 12 months showing 0.48 ± 0.40 logMAR for highly myopic and 0.42 ± 0.27 logMAR for non-highly myopic eyes (p=0.449). For eyes achieving complete hole closure, BCVA improvements followed a similar trend, with no significant differences between groups at any interval, including the final 12-month assessment. In the subgroup analysis of eyes with ILM peel and complete hole closure, as well as in the pseudophakic subgroup with complete hole closure, both groups demonstrated comparable BCVA outcomes, with no significant differences in VA change by month 12.
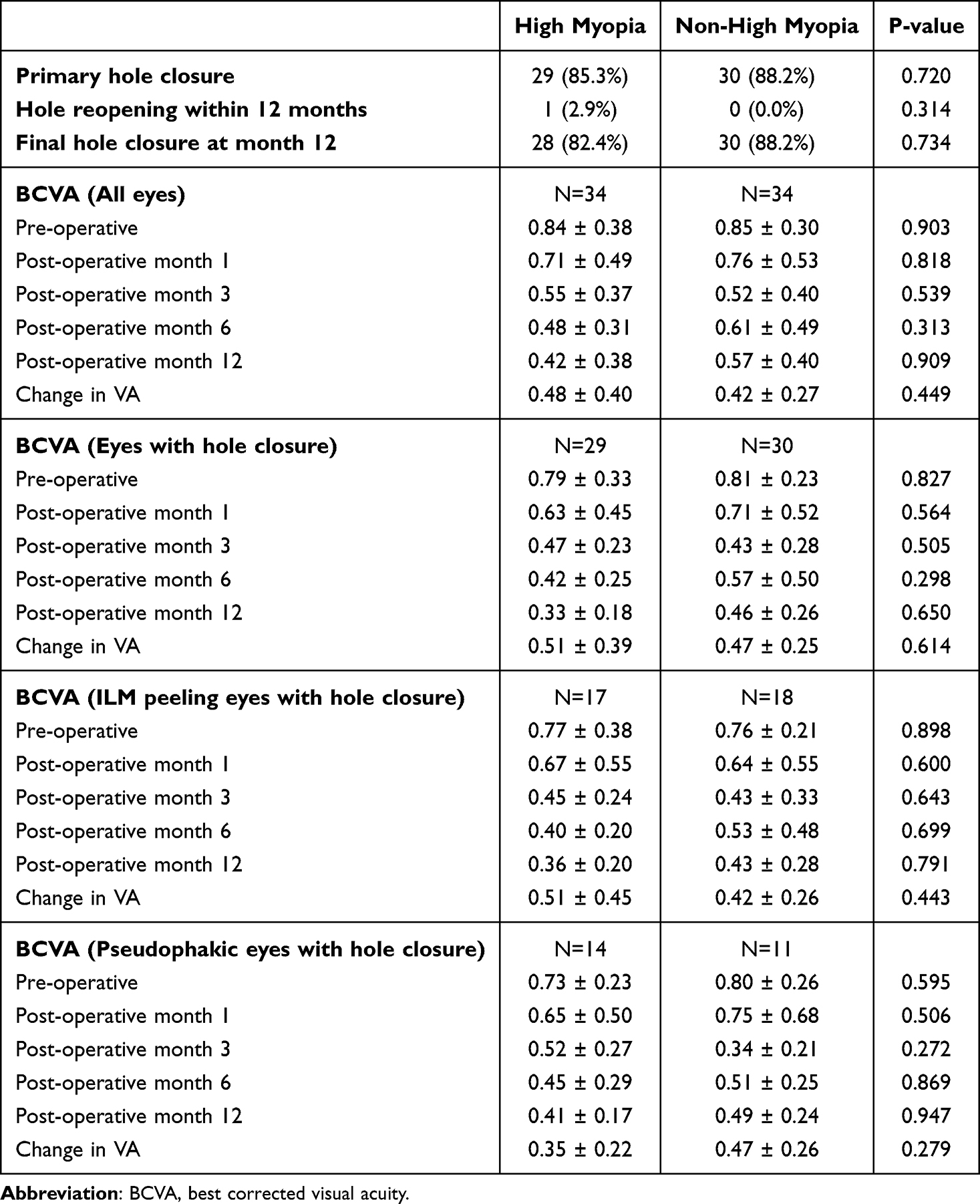 |
Table 2 Post-Operative Anatomical and Functional Outcomes Between Highly Myopic and Non-Highly Myopic Eyes |
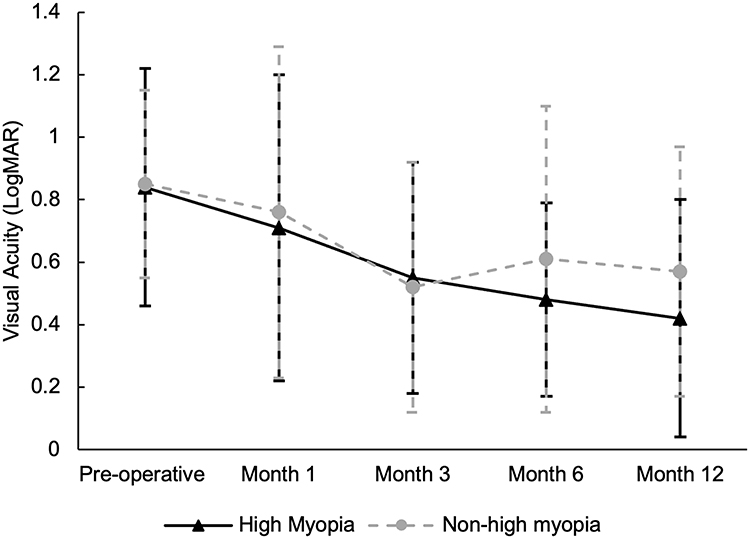 |
Figure 1 Post-operative functional recovery in visual acuity between highly myopic eyes (n=34) and non-highly myopic eyes (n=34). |
Figure 2 shows the comparison of outer retinal layer recovery of eyes with complete hole closure between groups. ELM restoration was the most common and occurs the earliest. This is followed by EZ and IZ restoration in both groups. There was no significant difference in the individual outer retinal layer restoration between HM and non-HM eyes at all time points.
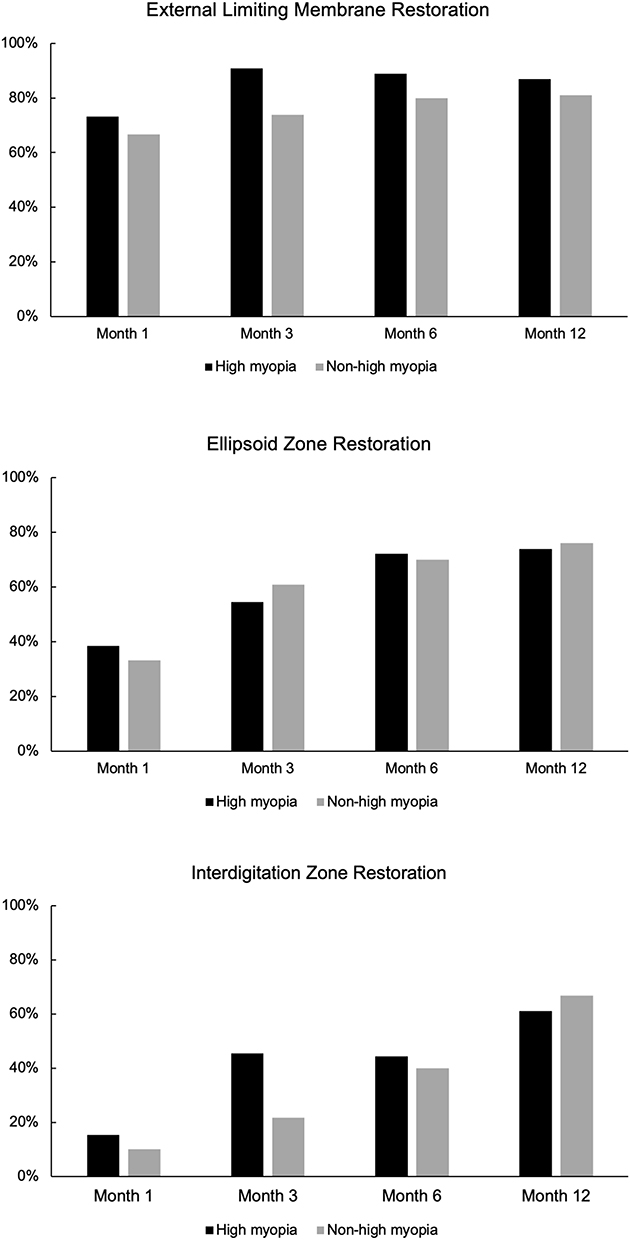 |
Figure 2 Comparison of the restoration of outer retina layers in eyes with hole closure between highly myopic and non-highly myopic eyes. |
The univariate analysis in Table 3 identified smaller MH size as a significant factor associated with hole closure in the overall cohort (349.8 ± 173.4 µm vs 545.2 ± 215.4 µm, p=0.003) as well in the HM subgroup (327.8 ± 154.5 µm vs 585.6 ± 193.5 µm, p=0.002). In non-HM subgroup, the absence of foveoschisis was significantly associated with higher closure rates (p=0.033). Use of the ILM flap technique was significantly associated with hole closure in the overall cohort (p=0.017) but this association did not reach statistical significance within the HM (p=0.074) or non-HM (p=0.116) subgroups.
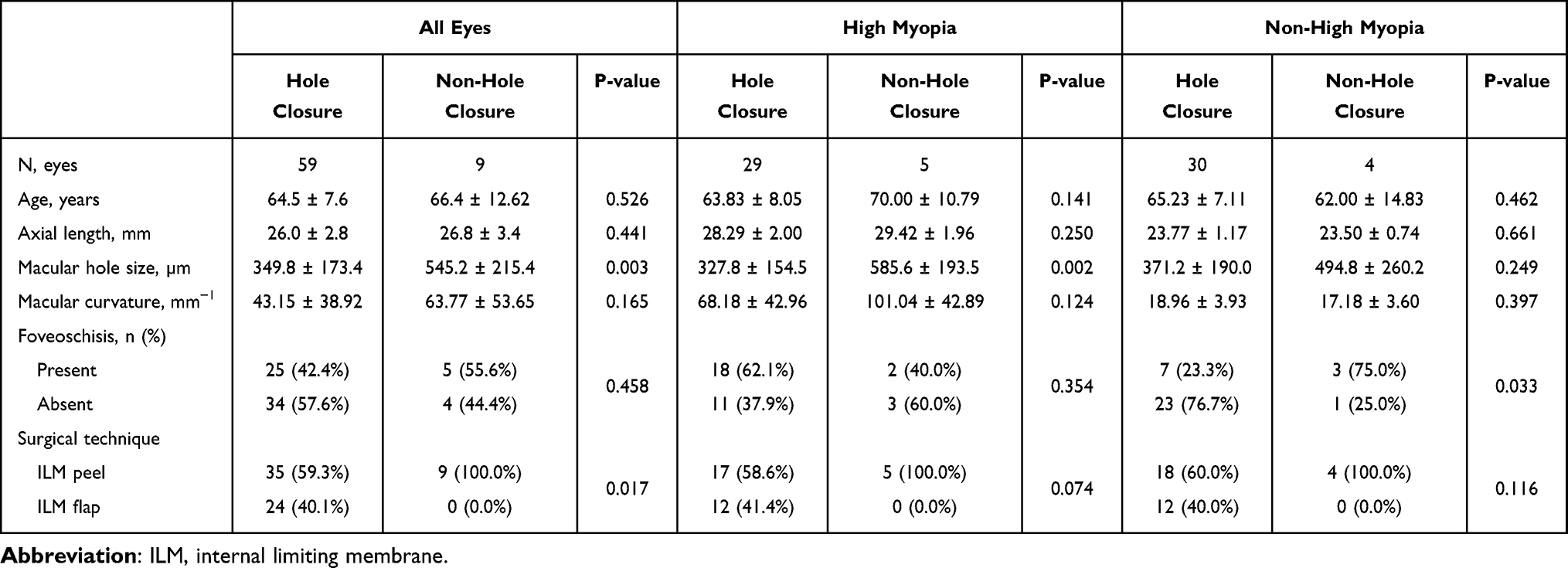 |
Table 3 Univariate Analysis of Clinical and Surgical Risk Factors Associated with Macular Hole Closure in All Eyes, High Myopia and Non-High Myopia Subgroups |
Linear regression analysis in Table 4, demonstrated that MH size was a significant predictor of final visual acuity at 12 months (β=0.010, 95% CI: 0.007–0.014), with larger holes associated with poorer VA outcomes. Age, AL, and macular curvature showed no significant relationship with VA, suggesting that MH size is the primary factor influencing both anatomical and functional outcomes in MH repair.
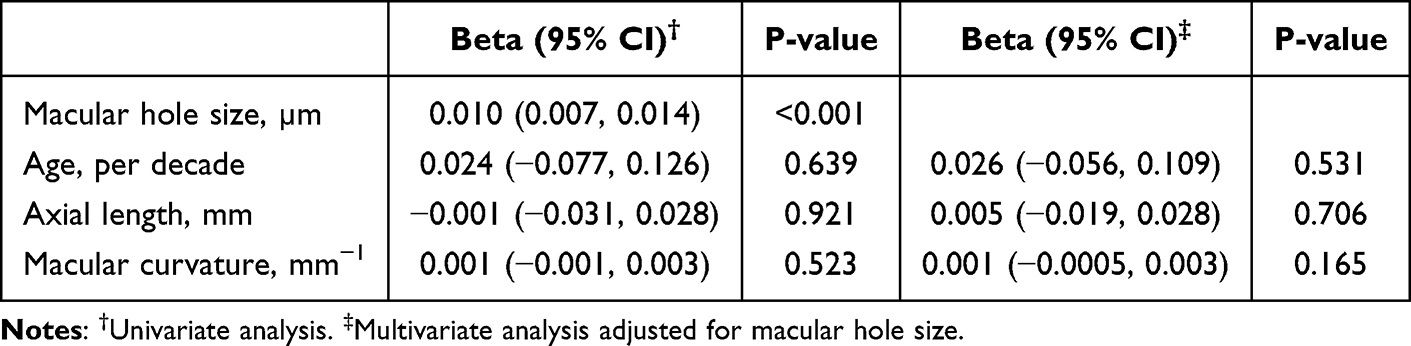 |
Table 4 Linear Regression Analysis of Factors Associated with Final Visual Acuity at 12 months |
Discussion
In this study, we compared post-operative anatomical and functional outcomes of MH repair in HM eyes to non-HM eyes. Primary hole closure rates were comparable between groups (85.3% vs 88.2%), with only one HM eye experiencing hole reopening within 12 months. BCVA at all time points did not differ significantly between groups. Larger MH size was associated with poorer anatomical and functional outcomes, underscoring its role as a critical determinant of surgical success. In addition, the use of ILM flap was associated with significantly higher hole closure rates compared to standard ILM peeling, across all eyes.
Historically, HM eyes have been associated with poorer surgical outcomes due to anatomical challenges such as posterior staphyloma, retinal thinning, and increased tractional forces.1–4 However, our findings support growing evidence that with modern surgical approaches, such as ILM peeling or flap-assisted closure, favorable anatomical outcomes can be achieved in HM eyes. In contrast to earlier studies where ILM peeling alone yielded closure rates as low as 62.5% in HM eyes, the introduction of the ILM flap technique has markedly improved success.17 A recent meta-analysis review reported an OR of 4.80 for primary closure using ILM flap versus ILM peeling.20 The technique is especially beneficial for complex cases such as large holes or those associated with macular detachment.21 Another meta-analyses focusing on HM eyes further support the effectiveness of ILM flap technique, reporting closure rates between 91.6% and 96.2%.14 Some studies had also reported its effectiveness in hole closure in eyes with extreme HM.22,23 Mechanistically, the flap may serve as a scaffold for Müller cell proliferation and gliosis, with the release of neurotrophic and basic fibroblast growth factors facilitating tissue remodeling and hole closure.24
Despite the anatomical benefits, the functional superiority of ILM flap over peeling remains debatable.15,16,25 Excessive gliosis at the fovea may hinder complete outer retinal recovery, thereby limiting visual gains.14 In our study, overall VA improvement did not differ significantly between HM and non-HM groups. Significant proportion of eyes underwent ILM peel in both groups, and subgroup analysis of eyes undergoing ILM peeling (Table 2) revealed no significant difference in VA improvement between HM and non-HM eyes. The VA improvement may be somewhat limited by incomplete restoration of outer retina layers despite successful hole closure. Figure 3 highlights this by contrasting the full reconstitution of the outer retina in a non-HM eye with persistent outer retinal disruption in an HM eye. We also observed a sequential pattern of outer retinal recovery, with the ELM being restored earliest, typically by 1 month postoperatively, followed by the EZ and IZ (Figure 2). This sequence is consistent with prior literature indicating that ELM recovery, a surrogate for Müller cell process restoration, is essential for subsequent EZ reconstitution.26,27 While our sample may be underpowered to detect differences in outer retinal recovery, the results suggest that HM eyes can achieve meaningful structural restoration despite axial elongation and chorioretinal thinning. In addition, achieving primary hole closure should still be the primary aim and is especially crucial in HM eyes, as reoperation can be difficult due to anatomical complexities.28 Persistent non-hole closure poses a risk of hole enlargement resulting in larger scotoma or even retinal detachment.
 |
Figure 3 (A–D) illustrate a non-highly myopic eye with axial length of 25.05mm. (A) pre-operative minimal hole diameter of 252 µm and visual acuity of 0.4 logMAR. (B) 1 month after surgery (internal limiting membrane peel) demonstrating incomplete hole closure with defects of the outer retinal layer. (C and D) illustrate gradual reconstitution of the external limiting membrane, ellipsoid zone and interdigitation zone at 6 and 12 months, with final visual acuity of 0.2 logMAR. (E–H) illustrate a highly myopic eye with axial length of 31.29 mm. (E) minimal hole diameter of 411 µm, pre-operative visual acuity of 1.0 logMAR. (F), 1 month after surgery (internal limiting membrane flap) demonstrating complete hole closure, however outer retinal layers are not fully reconstituted. (G and H) illustrate the progress at 6 months and 12 months showing incomplete reconstitution of outer retinal layer with final visual acuity of 0.8 logMAR. |
Although high axial myopia, characterized by increased AL, has traditionally been associated with poorer surgical outcomes due to factors such as increased traction and posterior staphyloma, we did not observe a significant effect of AL on closure rates. The high closure rates in HM eyes likely reflect the mitigating effect of the ILM flap technique. We also note that not all HM eyes exhibited increased macular curvature despite the longer AL. We hypothesize that differences in macular curvature, rather than AL, may be more relevant in determining surgical outcomes. Within the HM subgroup, eyes that achieved successful closure tended to have flatter macula, although this trend did not reach statistical significance. Given the limited imaging field of the 6×6 mm OCT scan, we could not definitively determine whether the increased macular curvature represented true outpouching, therefore we avoided the term posterior staphyloma. Consistent with previous literature, smaller MH size remained a significant factor associated with successful anatomical and visual outcomes, particularly in the HM subgroup.29 This association was not observed in non-HM eyes.
Our study has several limitations. First, swept-source OCT imaging was not utilized in this retrospective cohort, which could have provided valuable insights in characterizing and quantification of posterior staphyloma.5 While our sample size may have been insufficient to detect subtle associations between macular curvature and surgical outcomes, the observed high closure rates and comparable visual outcomes between HM and HM eyes are clinically meaningful and provide important real-world evidence. MH formation in HM remains an uncommon complication, and even with five years of consecutive data from a national tertiary center, the number of cases was inherently limited. Future multicenter study with larger cohorts is important to elucidate the influence of posterior staphyloma and foveoschisis on surgical outcomes. We also found no significant difference in functional outcomes between groups based on BCVA. While BCVA is a useful and convenient parameter for assessing functional outcomes, it only represents foveal function. In conditions like MH where the fovea is compromised, parafoveal function becomes increasingly important. More comprehensive assessments using microperimetry to assess parafoveal and perifoveal retinal sensitivity could be considered in future studies.30
Conclusion
MH surgery in HM eyes performed using current techniques of ILM peeling or flap, was able to achieve anatomical and functional outcomes comparable to those in non-HM eyes. These findings suggest AL alone may not be a critical determinant of surgical success. Instead, MH size remains a key prognostic factor, with larger holes associated with lower rates of anatomical closure and poorer BCVA. The ILM flap technique is associated with a significantly higher rate of hole closure compared to ILM peeling and should be considered more routinely in HM eyes to increase the likelihood of achieving anatomical success.
Acknowledgments
This study was presented at the Euretina Congress in September 2024 and the Asia-Pacific Vitreo-Retina Society in November 2024.
Funding
The publication of this study was supported by the SingHealth Fund - Singapore National Eye Centre (SHF-SNEC).
Disclosure
Professor Daniel Ting reports grants from National Medical Research Council, Singapore, National Medical Research Council, Singapore, Duke-NUS Medical School, Duke-NUS Medical School, Duke-NUS Medical School, Agency for Science, Technology and Research, Singapore, Agency for Science, Technology and Research, Singapore. In addition, Professor Daniel Ting has pending patents to SG Non-Provisional titled “Deep learning system for diabetic retinopathy, glaucoma, and age- related macular degeneration” (Application number 10201706186V) and “A computer-implemented method for training an image classifier using weakly annotated training data” (Application number 10201901083Y). All authors declare no other proprietary or commercial interests in any materials mentioned in this article.
References
1. Sulkes DJ, Smiddy WE, Flynn HW, Feuer W. Outcomes of macular hole surgery in severely myopic eyes: a case-control study. Am J Ophthalmol. 2000;130(3):335–339. doi:10.1016/s0002-9394(00)00489-x
2. Sc P, Rh L, Jt T, Rn S. Macular hole surgery in high myopia. Ophthalmology. 2001;108(2). doi:10.1016/s0161-6420(00)00532-7
3. Kwok AKH, Lai TYY. Internal limiting membrane removal in macular hole surgery for severely myopic eyes: a case-control study. Br J Ophthalmol. 2003;87(7):885–889. doi:10.1136/bjo.87.7.885
4. Suda K, Hangai M, Yoshimura N. Axial length and outcomes of macular hole surgery assessed by spectral-domain optical coherence tomography. Am J Ophthalmol. 2011;151(1):118–127.e1. doi:10.1016/j.ajo.2010.07.007
5. Ohno-Matsui K, Jonas JB. Posterior staphyloma in pathologic myopia. Prog Retin Eye Res. 2019;70:99–109. doi:10.1016/j.preteyeres.2018.12.001
6. Jo Y, Ikuno Y, Nishida K. Retinoschisis: a predictive factor in vitrectomy for macular holes without retinal detachment in highly myopic eyes. Br J Ophthalmol. 2012;96(2):197–200. doi:10.1136/bjo.2011.203232
7. Ruiz-Medrano J, Montero JA, Flores-Moreno I, Arias L, García-Layana A, Ruiz-Moreno JM. Myopic maculopathy: current status and proposal for a new classification and grading system (ATN). Prog Retin Eye Res. 2019;69:80–115. doi:10.1016/j.preteyeres.2018.10.005
8. García-Arumí J, Martinez V, Puig J, Corcostegui B. The role of vitreoretinal surgery in the management of myopic macular hole without retinal detachment. Retina Phila Pa. 2001;21(4). doi:10.1097/00006982-200108000-00006
9. Mete M, Alfano A, Guerriero M, et al. Inverted internal limiting membrane flap technique versus complete internal limiting membrane removal in myopic macular hole surgery: a comparative study. Retina Phila Pa. 2017;37(10):1923–1930. doi:10.1097/IAE.0000000000001446
10. Kuriyama S, Hayashi H, Jingami Y, Kuramoto N, Akita J, Matsumoto M. Efficacy of inverted internal limiting membrane flap technique for the treatment of macular hole in high myopia. Am J Ophthalmol. 2013;156(1):125–131.e1. doi:10.1016/j.ajo.2013.02.014
11. Michalewska Z, Michalewski J, Dulczewska-Cichecka K, Nawrocki J. Inverted internal limiting membrane flap technique for surgical repair of myopic macular holes. Retina Phila Pa. 2014;34(4):664–669. doi:10.1097/IAE.0000000000000042
12. Rizzo S, Tartaro R, Barca F, Caporossi T, Bacherini D, Giansanti F. Internal limiting membrane peeling versus inverted flap technique for treatment of full-thickness macular holes: a comparative study in a large series of patients. Retina Phila Pa. 2018;38(1):S73–S78. doi:10.1097/IAE.0000000000001985
13. Oleñik A, Rios J, Mateo C. Inverted internal limiting membrane flap technique for macular holes in high myopia with axial length ≥30 mm. Retina Phila Pa. 2016;36(9):1688–1693. doi:10.1097/IAE.0000000000001010
14. Chatziralli I, Machairoudia G, Kazantzis D, Theodossiadis G, Theodossiadis P. Inverted internal limiting membrane flap technique for myopic macular hole: a meta-analysis. Surv Ophthalmol. 2021;66(5):771–780. doi:10.1016/j.survophthal.2021.02.010
15. Shin MK, Park KH, Park SW, Byon IS, Lee JE. Perfluoro-n-octane-assisted single-layered inverted internal limiting membrane flap technique for macular hole surgery. Retina Phila Pa. 2014;34(9):1905–1910. doi:10.1097/IAE.0000000000000339
16. Zhang K, Yang X, Qi B, Wu X, Wang X, Liu W. Internal limiting membrane peeling or inverted flap technique combined with air tamponade in the treatment of macular holes in high myopia. Ophthalmic Res. 2023;66(1):561–570. doi:10.1159/000529387
17. Wu TT, Kung YH. Comparison of anatomical and visual outcomes of macular hole surgery in patients with high myopia vs. non-high myopia: a case-control study using optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2012;250(3):327–331. doi:10.1007/s00417-011-1821-7
18. Flores-Moreno I, Puertas M, Almazán-Alonso E, et al. Pathologic myopia and severe pathologic myopia: correlation with axial length. Graefes Arch Clin Exp Ophthalmol. 2022;260(1):133–140. doi:10.1007/s00417-021-05372-0
19. Rahimy E, Beardsley RM, Gomez J, Hung C, Sarraf D. Grading of posterior staphyloma with spectral-domain optical coherence tomography and correlation with macular disease. Can J Ophthalmol J Can Ophtalmol. 2013;48(6):539–545. doi:10.1016/j.jcjo.2013.07.006
20. Tzoumas N, McNally TW, Teh BL, et al. Internal limiting membrane flaps in macular hole surgery. Ophthalmol Retina. 2025:S2468653025000557. doi:10.1016/j.oret.2025.02.003
21. Re M, Dc S, L I, My F, Marques-Neves C. Complete ILM peeling versus inverted flap technique for macular hole surgery: a meta-analysis. Ophthalmic Surg Lasers Imaging Retina. 2020;51(3). doi:10.3928/23258160-20200228-08
22. Wu TT, Kung YH, Chang CY, Chang SP. Surgical outcomes in eyes with extremely high myopia for macular hole without retinal detachment. Retina Phila Pa. 2018;38(10):2051–2055. doi:10.1097/IAE.0000000000001806
23. Wu TT, Hou TY, Peng KL, Kung YH. Inverted flap technique versus internal limiting membrane insertion for macular hole in eyes with extremely high myopia. BMC Ophthalmol. 2024;24(1):286. doi:10.1186/s12886-024-03566-8
24. Shiode Y, Morizane Y, Matoba R, et al. The role of inverted internal limiting membrane flap in macular hole closure. Investig Opthalmology Vis Sci. 2017;58(11):4847. doi:10.1167/iovs.17-21756
25. Chou HD, Liu L, Wang CT, et al. Single-layer inverted internal limiting membrane flap versus conventional peel for small- or medium-sized full-thickness macular holes. Am J Ophthalmol. 2022;235:111–119. doi:10.1016/j.ajo.2021.08.016
26. Iwasaki M, Ando R, Aoki S, Miyamoto H. Restoration process of the outer retinal layers after surgical macular hole closure. Retina Phila Pa. 2022;42(2):313–320. doi:10.1097/IAE.0000000000003323
27. Wakabayashi T, Fujiwara M, Sakaguchi H, Kusaka S, Oshima Y. Foveal microstructure and visual acuity in surgically closed macular holes: spectral-domain optical coherence tomographic analysis. Ophthalmology. 2010;117(9):1815–1824. doi:10.1016/j.ophtha.2010.01.017
28. De Giacinto C, Pastore MR, Cirigliano G, Tognetto D. Macular hole in myopic eyes: a narrative review of the current surgical techniques. J Ophthalmol. 2019;2019:3230695. doi:10.1155/2019/3230695
29. Steel DH, Donachie PHJ, Aylward GW, Laidlaw DA, Williamson TH, Yorston D. Factors affecting anatomical and visual outcome after macular hole surgery: findings from a large prospective UK cohort. Eye. 2021;35(1):316–325. doi:10.1038/s41433-020-0844-x
30. Donati S, Valle PD, Premi E, Mazzola M, Presti LL, Azzolini C. Lamellar macular holes: the role of microperimetry in functional assessment. J Ophthalmol. 2019;2019:9035837. doi:10.1155/2019/9035837
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.