Back to Journals » International Medical Case Reports Journal » Volume 19
Intermittent Oroesophageal Feeding Modulates Post-Hemorrhagic Pharyngeal Inflammation in Dysphagia
Authors An D, Zhang Y, Hou X, Dou Z, Tang ZM, Wen H
Received 13 May 2025
Accepted for publication 18 December 2025
Published 13 January 2026 Volume 2026:19 538664
DOI https://doi.org/10.2147/IMCRJ.S538664
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Delian An,1,* Yaowen Zhang,1,* Xingyue Hou,1 Zulin Dou,1 Zhi-Ming Tang,2 Hongmei Wen1
1Department of Rehabilitation Medicine, The Third Affiliated Hospital Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Rehabilitation Medicine, The First People’s Hospital of Foshan, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongmei Wen, Department of Rehabilitation Medicine, The Third Affiliated Hospital Sun Yat-sen University, 600 Tianhe Road, Guangzhou, Guangdong Province, 510630, People’s Republic of China, Email [email protected] Zhi-Ming Tang, Department of Rehabilitation Medicine, The First People’s Hospital of Foshan, 600 Tianhe Road, Guangzhou, Guangdong, 510630, People’s Republic of China, Tel/Fax +86 20 85256013, Email [email protected]
Abstract: Dysphagia may be caused by stroke, cranial trauma, head and neck tumor surgery, and neurodegeneration. The overall prevalence of dysphagia in China is 38.7%, which can lead to aspiration pneumonia and malnutrition, increasing mortality rates and prolonging hospitalization. As an independent predictor of death, post-stroke dysphagia mortality ranges from 29% to 37%. Indwelling nasogastric tube feeding is widely used for dysphagic patients, but complications include mucosal bleeding, tumefaction, pneumonia, and acid regurgitation. Intermittent nasogastric tubes are an alternative option, though rarely reported. This paper describes a stroke patient with dysphagia and tracheotomy who received intermittent oroesophageal tube feeding. Notably, epiglottis tumefaction caused by the indwelling nasogastric tube disappeared after switching to intermittent oroesophageal tube feeding, with concurrent improvements in nutritional indicators, gastrointestinal tolerance, and swallowing function. To avoid side effects of indwelling nasogastric tubes in dysphagic patients, intermittent oroesophageal tube feeding deserves clinical consideration.
Plain Language Summary: A 34-year-old male with post-cerebral hemorrhage quadriplegia developed persistent dysphagia and pharyngeal edema after six months of indwelling nasogastric tube feeding. Serial fiberoptic bronchoscopy demonstrated progressive epiglottic and left piriform sinus swelling correlating with prolonged tube placement. Transition to intermittent oroesophageal feeding (Ch14 tube, 6 times/day protocol) led to complete resolution of mucosal edema within 12 days, documented through three endoscopic examinations. Nutritional status improved with 2160 kcal/day enteral nutrition (35 kcal/kg/day), accompanied by 5% weight gain. Successful tracheostomy decannulation occurred on February 24, 2020, with stable vital signs post-extubation. Key clinical insights include the association between indwelling tube duration and pharyngeal inflammation severity, the therapeutic role of feeding interval adjustment in mucosal recovery, and the value of serial endoscopic monitoring when videofluoroscopic swallowing studies are unavailable. This protocol demonstrates effective dysphagia management in post-neurosurgical rehabilitation settings.
Keywords: intermittent oroesophageal tube feeding, nutrition, stroke, dysphagia, epiglottis tumefaction
Background
Dysphagia affects approximately 23–80% of stroke patients, manifesting as coughing, choking, aspiration, penetration, food residue, and reflux.1,2 This condition significantly increases the risk of pneumonia, malnutrition, and dehydration, thereby impeding medical recovery and diminishing quality of life.2
Nasogastric tube feeding represents the standard nutritional intervention for patients with severe dysphagia. While this approach effectively prevents malnutrition by enabling direct food delivery to the stomach,3 prolonged nasogastric tube placement carries substantial complications. These include xerostomia, mycteroxerosis, pharyngeal discomfort, and mucosal erosion resulting from chronic compression.4–6 More concerning, evidence suggests that indwelling nasogastric tubes may contribute to swallowing muscle atrophy and cardia achalasia, potentially exacerbating the risk of reflux, aspiration, and pneumonia.7,8 Alternative feeding approaches such as percutaneous endoscopic gastrostomy (PEG) can mitigate certain nasogastric tube-associated complications.7,9 However, PEG adoption remains limited in Chinese healthcare settings due to cultural concerns regarding invasiveness and complications including infection and gastric hemorrhage.
This clinical knowledge gap necessitates exploration of alternative feeding strategies for dysphagic stroke patients, particularly those with tracheostomy. We propose that intermittent oroesophageal tube feeding may represent a viable alternative that minimizes the complications associated with continuous nasogastric intubation while accommodating cultural preferences against permanent gastrostomy placement.
Case Presentation
A 34-year-old man was referred to the Department of Rehabilitation on February 9, 2020, because of dysphagia, dyslogia (impairment of speech due to mental disorder), and quadriplegia lasting 6 months. According to his medical history, he lost consciousness on July 14, 2019, and computed tomography confirmed cerebral hemorrhage (Figure 1). He underwent emergency decompressive craniectomy and hematoma evacuation on the same day and tracheotomy on July 18, 2019, because of pneumonia and mechanical ventilation. When transferred to our department, he had stable vital signs, clear consciousness (Glasgow Coma Scale (GSC) total score: E4VTM6), and cognitive impairment. He could turn over but could not sit, stand, or walk alone. He had a metal tracheal cannula without a cuff and could say 2 or 3 words when the tube was blocked. He was fed via an indwelling nasogastric tube, but had suffered a weight loss of 10 kg within the previous 6 months.
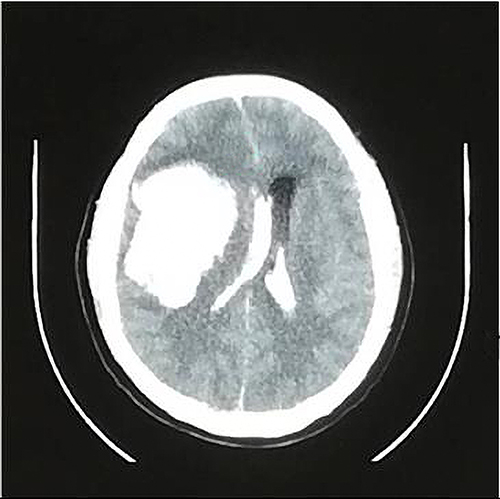 |
Figure 1 Position and volume of hemorrhage on computed tomography. |
The patient was unable to complete the physical examination. His body temperature was 36.7–37.1 °C, oxygen saturation was 92%–98%, and blood pressure was 117–142/72-102 mmHg. His respiratory rate ranged from 18–33 times per minute. His weight, height, and body mass index (BMI) were 67.8 kg, 177 cm, and 21.6, respectively. His scores on the Functional Oral Intake Scale (FOIS) and Nutritional Risk Screening 2002 (NRS 2002) were 1 and 5, respectively, and his Barthel index, Braden Scale for Predicting Pressure Sore Risk (Braden scale), and Morse Fall Scale scores were 0, 14, and 60, respectively. The patient had white sticky sputum (approximately 20–50 mL per day).
During the first few days, the patient was fed through an indwelling nasogastric tube. Considering that the patient’s BMI was within the normal range, and rehabilitation training would be conducted daily, we decided to administer 2160 kcal/day of total enteral nutrition (Jiashan, Nestle) based on his body weight (35 kcal/kg/d).10 In addition, the patient received routine treatments, including physical, respiratory, and occupational therapy, sputum excretion, atomization, and pharmacotherapy.
Fiberoptic bronchoscopy on February 13, 2020, showed epiglottis and left arytenoid tumefaction, and the nasogastric tube entering the esophagus through the left piriform sinus (Figure 2Ai and Bi). To resolve this situation, we changed the nasogastric tube from indwelling to intermittent. The changes proceeded smoothly. The patient had no nausea, vomiting, dyspnea (shortness of breath), or other discomfort.
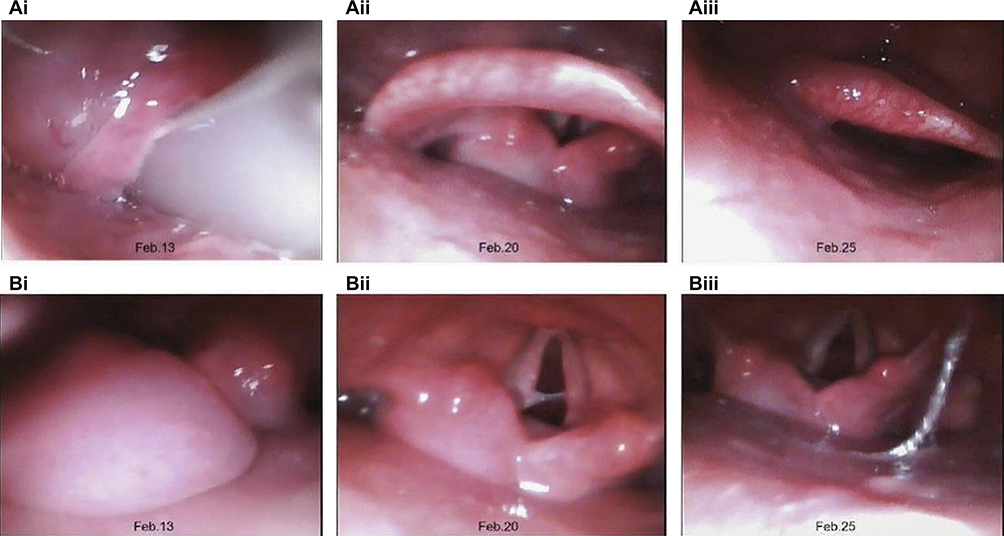 |
Figure 2 Changes in tumefaction of vallecula epiglottica and arytenoid after intermittent oroesophageal tube feeding. (Ai) tumefaction in the epiglottis; (Aii) no tumefaction in the epiglottis; (Aiii) no tumefaction in the epiglottis; (Bi) swollen spoon-shaped cartilage; (Bii) the piriform sinus tumefaction had decreased; (Biii) piriform sinus tumefaction was virtually absent. |
The procedure for intermittent oroesophageal tube feeding was as follows: The nurse assisted the patient in assuming a semi-recumbent position and cleaning the oral cavity. The nurse placed the gastric tube (Ch14, Uerkai, Nutricia Pharmaceutical) into the patient’s mouth and asked the patient to swallow. When the nasogastric tube was advanced to 55–60 cm, correct intragastric placement was inferred by the following clinical signs: the patient reported a transient throat discomfort and a brief gagging sensation as the tube passed the oropharynx; there was no cough reflex or persistent respiratory distress, and oxygen saturation remained stable (SpO2 maintained at 95–100%). Auscultation over the epigastrium during insufflation of 20 mL of air with a syringe produced an immediate, audible “whoosh” sound, further supporting gastric placement. The patient did not exhibit coughing, chest tightness, or signs of respiratory compromise. Food was then injected. After the infusion was complete, the tube was flushed with water and gently withdrawn. The patient was kept in semi-decubitus position for at least 30 min; any stimulating operation (such as suction or expectoration) was avoided. Feedings were given according to the following schedule: 8 am (450 mL), 10 am (300 mL) 12 am (450 mL), 3 pm (300 mL), 6 pm (450 mL), and 8:30 pm (200 mL).
The fiberoptic endoscopic examination of the larynx and pharynx on February 20, 2020, showed no tumefaction in the epiglottis, and the piriform sinus tumefaction had decreased (Figure 2Aii and Bii). On February 24, 2020, the patient was extubated and his breath and vital signs were normal. The fiberoptic bronchoscopy examination of the larynx and pharynx was repeated on February 25, 2020, which showed no tumefaction in the epiglottis, and piriform sinus tumefaction was virtually absent (Figure 2Aiii and Biii). Twelve days after switching to the intermittent nasogastric tube, the patient’s nutritional indicators, gastrointestinal tolerance, and swallowing function improved (Table 1).
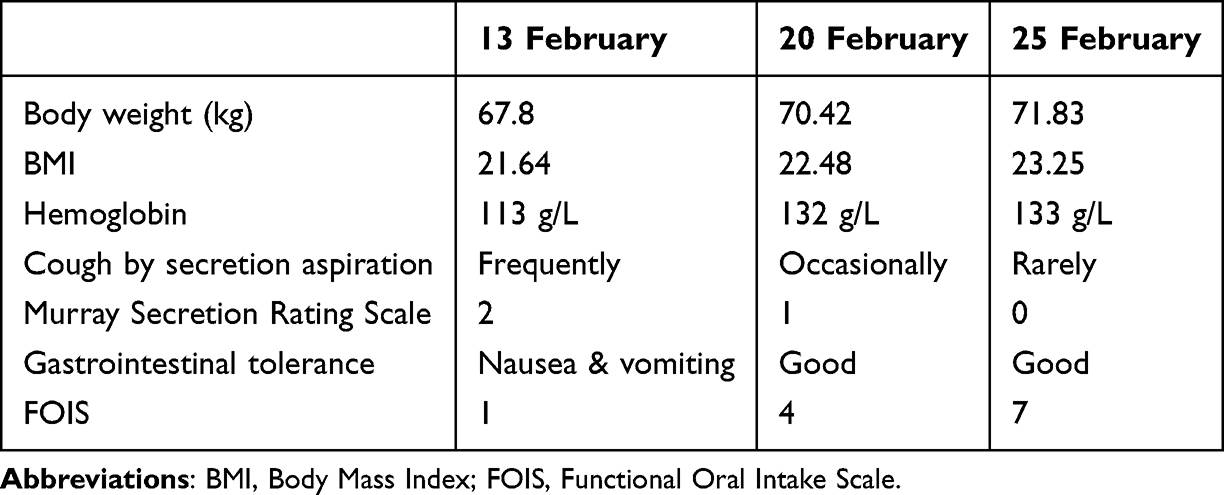 |
Table 1 Patient’s Tumefaction and Clinical Parameters Upon Use of Intermittent Oroesophageal Tube Feeding |
Discussion
The patient in this case had a cerebral hemorrhage with dysphagia, pneumonia, and tracheotomy. The nasogastric tube was initially used as routine clinical nutrition support. However, fiberoptic bronchoscopy revealed tumefaction of the epiglottis and arytenoids. One week after changing to an intermittent nasogastric tube, the tumefaction had begun to shrink and virtually disappeared after 2 weeks. In addition, nutritional indicators improved, and pharyngeal secretions decreased. The tracheal cannula was removed and the patient was able to eat completely by mouth. No obvious complications were noted.
When the patient was transferred to our department, an indwelling nasogastric tube was used as the conventional method for supplying nutrition. However, computed tomography of the neck and fiberoptic bronchoscopy revealed tumefaction of the epiglottis and left arytenoid. Considering his medical history and examinations, these signs were suspected to be common adverse effects of an indwelling nasogastric tube. Tumefaction may have been due to the direct compression of the nasogastric tube, mucous membrane irritation, increased secretions, and reflux.11 The indwelling nasogastric tube limits the lifting of the larynx, thus affecting swallowing movement and airway protection.12 Repeated irritation of the mucous membrane leads to increased secretions. In addition, because of the nasogastric tube, newly generated secretions are not easily cleaned away completely removed.
The incidence of pneumonia associated with indwelling nasogastric tubes has been reported to be as high as 31.25%.8 The normal peristaltic function of the esophagus helps to clear the contents of the stomach that reflux into the esophagus. However, the indwelling nasogastric tube weakens or disappears the esophageal peristalsis, the ability to clear the esophagus lessens, the risk of reflux becomes significantly higher, and acid reflux irritates the pharynx and causes tumefaction.13 At the same time, gastrointestinal peristalsis may slow down, and gastrointestinal intolerance complications such as indigestion, bloating, and reflux may occur.14
Outcome And Follow-up
Previous studies have reported that intermittent oro-esophageal feeding improves nutrition and outcomes. In 2017, Zeng et al reported that intermittent oroesophageal tube feeding can improve the swallowing function of patients; however, the clinical sample size was insufficient.15 Nakajima reported that patients can independently insert an intermittent nasogastric tube, which can significantly reduce the length of hospital stay and make patients more comfortable and involved in treatment.16 However, there are no direct reports of intermittent oroesophageal tube feeding eliminating tumefaction.
In the present case, tumefaction disappeared rapidly after the change from indwelling to intermittent oroesophageal tube feeding, and the nutrition index and clinical outcome improved significantly with no adverse outcomes. A plausible reason for this is the relief of pressure on the pharynx and arytenoids. In addition, because the intermittent tube is removed, there is less irritation to the pharynx, and secretions can be cleared more easily. In addition, with no tube in the pharynx, the risk of reflux is reduced and therefore gastric acid irritation in the throat as well. Intermittent oroesophageal tube feeding also eliminated the limited lifting of the larynx, which is imposed by the indwelling tube, thus improving swallowing function and airway protection.17 In addition, feeding with an intermittent oroesophageal tube is more convenient for patients undergoing rehabilitation training, especially for swallowing and respiratory training.18 These effects are concomitant with the disappearance of tumefaction, improvement of gastrointestinal tolerance after changing the feeding method, and amelioration of swallowing function, nutritional status, and clinical outcomes.
Implications
When tube feeding is not tolerated and PEG is not the alternative for cultural reason, intermittent orafaringeal tube feeding can be an opportunity. Intermittent catheterization feeding provides a novel alternative for clinical nutritional support, significantly reducing complications associated with traditional indwelling nasogastric tubes. It alleviates patients’ sense of being critically ill, increases social interaction, and promotes improved swallowing function.
Limitations
As a single case report, the findings of this study cannot be generalized. Furthermore, the absence of a control group makes it difficult to establish a definitive causal relationship between the intervention and the positive outcome. Nonetheless, this case highlights a promising clinical observation that warrants further investigation through larger, controlled trials to validate the efficacy of this feeding strategy.
Ethics Statement
Ethical approval and institutional approval were obtained from the third affiliated hospital of Sun Yat-sen university.
Patient Consent for Publication
Written informed consent was obtained directly from the patient(s) for the publication of this case report, including all clinical details and images. The patient(s) was informed about the purpose of publication and has read the manuscript before giving consent.
Funding
This work was supported by Guangdong Provincial Nurses Association 2024 Research Project (gdshsxh2024zd03).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Souza JT, Ribeiro PW, de Paiva SAR, et al. Dysphagia and tube feeding after stroke are associated with poorer functional and mortality outcomes. Clin Nutr. 2020;39(9):2786–6. doi:10.1016/j.clnu.2019.11.042
2. De Cock E, Batens K, Hemelsoet D, Boon P, Oostra K, De Herdt V. Dysphagia, dysarthria and aphasia following a first acute ischaemic stroke: incidence and associated factors. Eur J Neurol. 2020;27(10):2014–2021. doi:10.1111/ene.14385
3. Chang W-K, Huang -H-H, Lin -H-H, Tsai C-L. Percutaneous endoscopic gastrostomy versus nasogastric tube feeding: oropharyngeal dysphagia increases risk for pneumonia requiring hospital admission. Nutrients. 2019;11(12):2969. doi:10.3390/nu11122969
4. Qureshi AZ, Jenkins RM, Thornhill TH. Percutaneous endoscopic gastrostomy versus nasogastric tube feeding during neurorehabilitation. Ifs, ands, or buts. Neurosci J. 2016;21(1):69–71. doi:10.17712/nsj.2016.1.20150013
5. Jaafar MH, Mahadeva S, Tan KM, et al. Long‐Term Nasogastric Versus Percutaneous Endoscopic Gastrostomy Tube Feeding in Older Asians With Dysphagia: a Pragmatic Study. Nutr Clin Pract. 2019;34(2):280–289. doi:10.1002/ncp.10195
6. Juan W, Zhen H, Yan-Ying F, et al. A comparative study of two tube feeding methods in patients with dysphagia after stroke: a randomized controlled trial. J Stroke Cerebrovasc Dis. 2020;29(3):104602. doi:10.1016/j.jstrokecerebrovasdis.2019.104602
7. Chime C, Baiomi A, Kumar K, Patel H, Dev A, Makker J. Endoscopic repair of gastrocolic and colocutaneous fistulas complicating percutaneous endoscopic gastrostomy tube. Case Rep Gastrointest Med. 2020;2020(1):7262514. doi:10.1155/2020/7262514
8. Jianqin S, Zulin D. Chinese expert consensus on food and nutrition management for dysphagia (2019 version). Asia Pacific J Clin Nutr. 2020;29(2):434–444.
9. Ichimaru S. Methods of enteral nutrition administration in critically ill patients: continuous, cyclic, intermittent, and bolus feeding. Nutr Clin Pract. 2018;33(6):790–795. doi:10.1002/ncp.10105
10. Hindley K, Fenton C, McIntosh J. A systematic review of enteral feeding by nasogastric tube in young people with eating disorders. J Eating Disorders. 2021;9:1–13. doi:10.1186/s40337-021-00445-1
11. Wang T, Tai J, Hu R, et al. Impacts of long-term nasogastric tube feeding and tracheostomy on pharyngeal and laryngeal structure in ABI patients: an FEES study. Eur J Med Res. 2025;30(1):109. doi:10.1186/s40001-025-02375-z
12. Kwak H-J, Kim L, Ryu B-J, et al. Influence of nasogastric tubes on swallowing in stroke patients: measuring hyoid bone movement with ultrasonography. Ann Rehabil Med. 2018;42(4):551–559. doi:10.5535/arm.2018.42.4.551
13. Hiestand M, Jalil AA, Castell DO. Manometric subtypes of ineffective esophageal motility. Clin Transl Gastroenterol. 2017;8(3):e78. doi:10.1038/ctg.2017.4
14. Wesselink E, Koekkoek KW, Looijen M, van Blokland DA, Witkamp RF, van Zanten AR. Associations of hyperosmolar medications administered via nasogastric or nasoduodenal tubes and feeding adequacy, food intolerance and gastrointestinal complications amongst critically ill patients: a retrospective study. Clin Nutr ESPEN. 2018;25:78–86. doi:10.1016/j.clnesp.2018.04.001
15. Zeng H, Zhao W, Wu J, et al. Effect of intermittent oro-esophageal tube feeding in bulbar palsy after ischemic stroke: a randomized controlled study. Stroke. 2024;55:1142–1150. doi:10.1161/STROKEAHA.123.046122
16. Wu C, Zhu X, Zhou X, et al. Intermittent tube feeding for stroke patients with dysphagia: a meta-analysis and systematic review. Ann Palliat Med. 2021;10(7):7406415–7407415. doi:10.21037/apm-21-736
17. Ajmani GS, Nocon CC, Brockstein BE, et al. Association of a proactive swallowing rehabilitation program with feeding tube placement in patients treated for pharyngeal cancer. JAMA Otolaryngol Head Neck Surg. 2018;144(6):483–488. doi:10.1001/jamaoto.2018.0278
18. Braun RG, Arata J, Gonzalez-Fernandez M. Dysphagia and enteral feeding after stroke in the rehabilitation setting. Phys Med Rehabil Clin. 2024;35(2):433–443. doi:10.1016/j.pmr.2023.07.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.