Back to Journals » Clinical Ophthalmology » Volume 15
Intermediate Uveitis Etiology, Complications, Treatment, and Outcomes in a Colombian Uveitis Referral Center
Authors Rojas-Carabali W ![]() , Reyes-Guanes J
, Reyes-Guanes J ![]() , Villabona-Martinez V, Fonseca-Mora MA, de-la-Torre A
, Villabona-Martinez V, Fonseca-Mora MA, de-la-Torre A ![]()
Received 2 March 2021
Accepted for publication 14 April 2021
Published 21 June 2021 Volume 2021:15 Pages 2597—2605
DOI https://doi.org/10.2147/OPTH.S309193
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
William Rojas-Carabali,1,* Juliana Reyes-Guanes,2,* Valeria Villabona-Martinez,1 Maria Alejandra Fonseca-Mora,1 Alejandra de-la-Torre1
1Neuroscience Research Group “NeURos”, Escuela de Medicina y Ciencias de la Salud, Universidad del Rosario, Bogotá, Colombia; 2Escuela Barraquer Research Group, Escuela Superior de Oftalmología del Instituto Barraquer de América, Bogotá, Colombia
*These authors contributed equally to this work
Correspondence: Alejandra de-la-Torre
Neuroscience Research Group “NeURos”, Escuela de Medicina y Ciencias de la Salud, Universidad del Rosario, Carrera 24 # 63C - 69, Bogotá, Colombia
Tel +57 3102482196
Email [email protected]
Purpose: To analyze the etiology, clinical characteristics, complications, treatments, and outcomes of patients with intermediate uveitis examined in a uveitis referral center in Bogotá, Colombia.
Patients and Methods: We conducted a retrospective descriptive study. We reviewed systematically the clinical records of patients attending a uveitis referral center in Bogotá, Colombia from 2013 to 2020. Data analysis included demographics, etiology, clinical characteristics, treatment modalities, best-corrected visual acuity, and complications. For categorical variables, absolute and relative frequencies were used while for continuous variables mean and standard deviations were calculated.
Results: We identified 18 patients with intermediate uveitis. The mean age at disease onset was 19.4 years. There was no sex predominance. Two-thirds of the patients presented bilateral involvement. The mean initial best-corrected visual acuity was 0.19 LogMAR. The most common etiology was idiopathic followed by undetermined, tuberculosis, multiple sclerosis, and juvenile idiopathic arthritis. The most common characteristics were insidious onset, chronic course, and persistent duration. The complications found were macular edema, optic disk edema, cataract, epiretinal membrane, among others. Corticosteroids and immunosuppressive therapy were the most common treatments. Mean follow-up time was 24.4 months, and the mean final best-corrected visual acuity was 0.12 LogMAR.
Conclusion: This is the first study describing intermediate uveitis features in South America. In our context, intermediate uveitis is infrequent. Polyautoimmunity and familial autoimmunity phenomena were found in some patients. These may require a multidisciplinary approach. Ophthalmologists should promptly diagnose, treat, and refer patients with this disease to avoid common complications. Further studies are required to determine the disease relation with polyautoimmunity.
Keywords: ocular inflammatory diseases, uveitis, epidemiology, etiology, Colombia
Introduction
Intermediate uveitis (IU) refers to the inflammation, generally bilateral, of the anterior vitreous, ciliary body, and peripheral retina.1,2 Etiology is usually idiopathic, but it has been as well associated with autoimmune and infectious systemic diseases.3,4 Several studies suggest that IU represents the second most common localization of uveitis in childhood and the least common in adults.2,5 Prognosis is usually good, but it can be associated with complications.6,7 Therefore, early diagnosis and prompt treatment are necessary. Nevertheless, as it is an uncommon disease and has multiple etiologies, it does not have a specific treatment that can be generalized for all cases.8
IU incidence varies from 1.5 to 2.08/100,000 inhabitants per year and its prevalence from 4.0 to 5.6/100,000 inhabitants.9,10 Despite the studies that have been carried out, epidemiological data remain very limited, especially in Latin America.11–13 In Colombia, studies in adult population (2006)13 and pediatric population (2015)12 have been carried out, but only addressing general uveitis.
Consequently, this study aims to describe the demographics and clinical characteristics, treatment, and outcomes from a group of patients diagnosed with IU who attended a uveitis referral center in Bogotá, Colombia from 2013 to 2020. This allows us to increase our knowledge of the disease and improve its diagnostic and therapeutic approach.
Patients and Methods
Design: We conducted a retrospective, observational, descriptive, cross-sectional study in patients with IU presented at a uveitis referral center in Bogotá, Colombia.
Population: We reviewed 435 clinical records of patients with uveitis diagnosis from 2013 to 2020. Inclusion criteria were 1) patients diagnosed with IU, 2) patients who attended the uveitis referral center, 3) patients evaluated from 2013 to 2020. Exclusion criteria were 1) medical records of patients with incomplete information. Eighteen clinical records of patients with IU were recovered, and after applying inclusion and exclusion criteria all of them were included.
Patient approach: All patients were examined by a specialist in uveitis and treated in a multidisciplinary setting.
All patients with suspected IU received detailed eye examinations, physical examinations, and laboratory workup for infectious or non-infectious etiologies were order: complete blood count, erythrocyte sedimentation rate, C-reactive protein (CRP), urine analysis, VDRL, FTA-ABS, Mantoux test, and chest radiography. Based on specific clinical findings, antibodies profile, specific infectious tests, and imagenological assessment were asked.
Brain magnetic resonance imaging (B-MRI) was ordered when patients referred neurological symptoms and chest computerized tomography (C-CT) was ordered when tuberculosis or sarcoidosis were suspected based on radiography or laboratory results.
During follow-up fluorescein angiography was ordered to all patients. Optical Coherence Tomography (OCT) was asked when macular edema was suspected. Ocular ultrasonography was ordered when posterior pole details were unable to be examined due to ocular media opacities.
If necessary, the patients were referred to the appropriate specialists (neurologist, rheumatologist or infectious disease specialist) for systemic evaluation based on results of testing.
Patients were classified by anatomical location, onset, course, and duration of the disease according to the Standardization of Uveitis Nomenclature (SUN) Working Group System.1 We defined etiology as undetermined when patients had not complete workup in order to rule out systemic or infectious etiologies.
Data collection and statistical analysis: We elaborated and validated a database in Microsoft Excel (Microsoft Corp., Redmond, WA, USA). Variables included in the database were: demographics, etiology, clinical characteristics, treatment modalities, best-corrected visual acuity (BCVA), and complications. Univariate analysis was performed, using absolute and relative frequencies for categorical variables and mean and standard deviations for continuous variables.
Results
The prevalence of IU in our center was 4.13%. The mean age at first consultation with the uveitis specialist was 21.2 ± 15.9 years-old, with a 50% female prevalence. Patients presented a mean of 1.2 ± 1.9 autoimmune diseases in their family history and a mean of 0.38 ± 0.84 personal autoimmune diseases. More detailed information is given in Table 1.
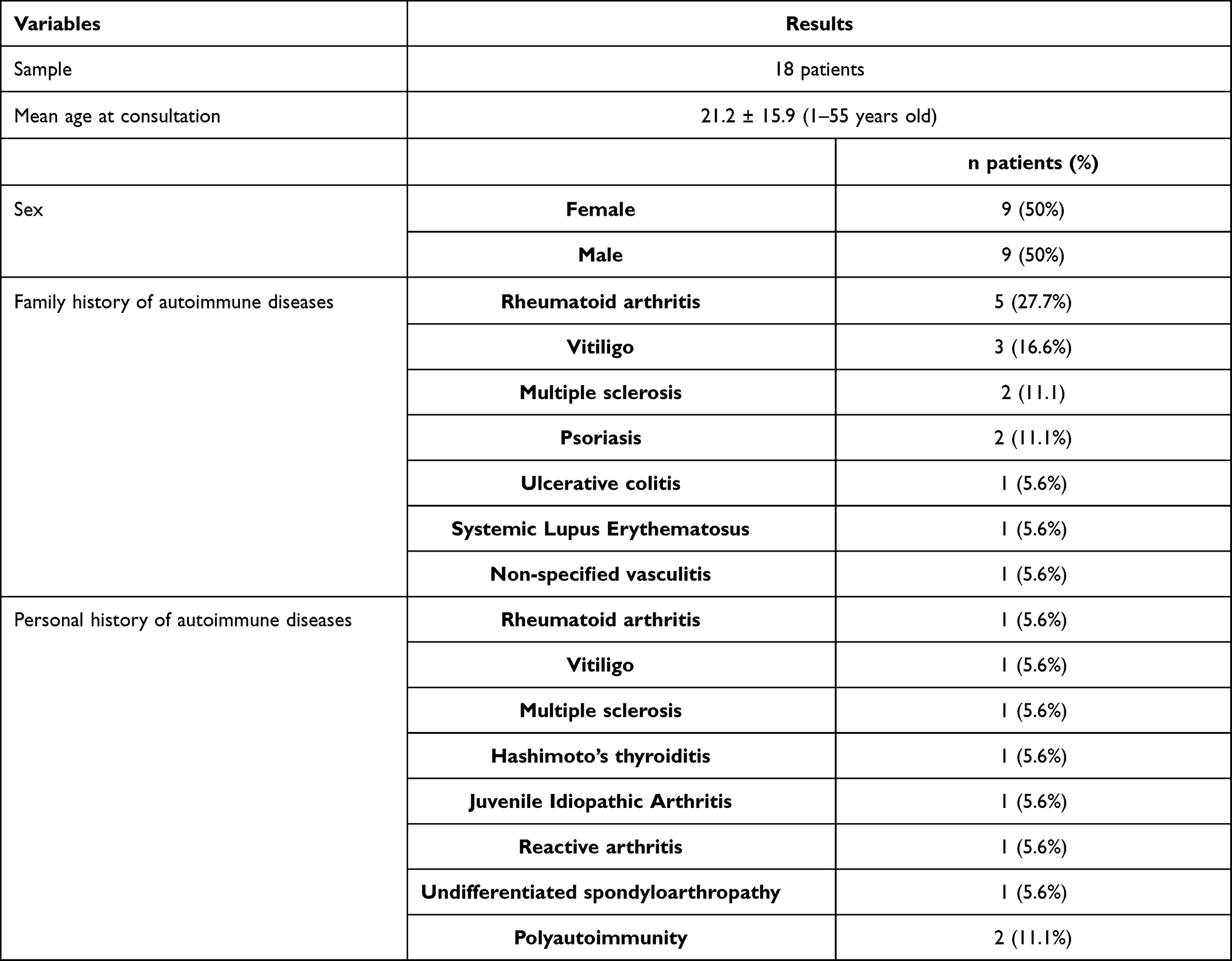 |
Table 1 Patients Demographic Description |
In the first consultation, two-thirds of the patients presented bilateral involvement, being the right eye the most affected. Mean age at disease onset was 19.4 ± 17.1 years-old. The most common onset was insidious, followed by undetermined and sudden. The mean BCVA was 0.19 ± 0.19 in LogMAR. Anterior chamber cells were found in 6/18 (33.3%) patients, vitritis was found in 13/18 (72.2%) patients and none of them presented flare. Snowballs and snowbanks were found in 14/18 (77.7%) and 8/18 (44.4%) patients, respectively. The mean intraocular pressure was 14 ± 2.3 mmHg. Eight patients presented posterior vitreous detachment. Other ocular inflammation signs found were vasculitis, retinitis, papillitis, optic neuritis, and iris nodules. More detailed information about clinical aspects is found in Table 2.
 |
Table 2 Clinical Characteristics of Patients in the First Consultation |
Abnormal laboratory findings for specific infectious etiologies were positive Mantoux test and positive Interferon-Gamma Release Assays; other findings were leukocytosis, positive CRP, mild increased ACE, positive autoantibodies (AntiTG, AntiPC, AntiTPO, pANCA, cANCA, and ANAs). Abnormal imaging findings were optic neuritis in one of the five B-MRI ordered, a radio-opaque nodule in one chest radiography, and a subcentimeter pulmonary nodule, and a mediastinal lymphadenopathy, each in one of the four C-CT ordered. Additionally, the most common abnormal findings in ocular imaging were peripheral vascular staining and leakage in the fluorescein angiography; macro and micro-cyst changes in the macula, continuous line of hyperreflectivity attached to the inner retinal surface, and macular thickening in the OCT; and dense and motile vitreous opacities in the ocular ultrasonography. More detailed information about paraclinical tests is given in Table 2.
Regarding etiology, 15/18 patients had confirmed etiological diagnoses. The most common cause was idiopathic 11/18 (61.1%), followed by tuberculosis 2/18 (11.1%). One patient had MS and one JIA (5.6%, each). Three patients were classified as undetermined because they are still being studied (16.6%) (Table 3).
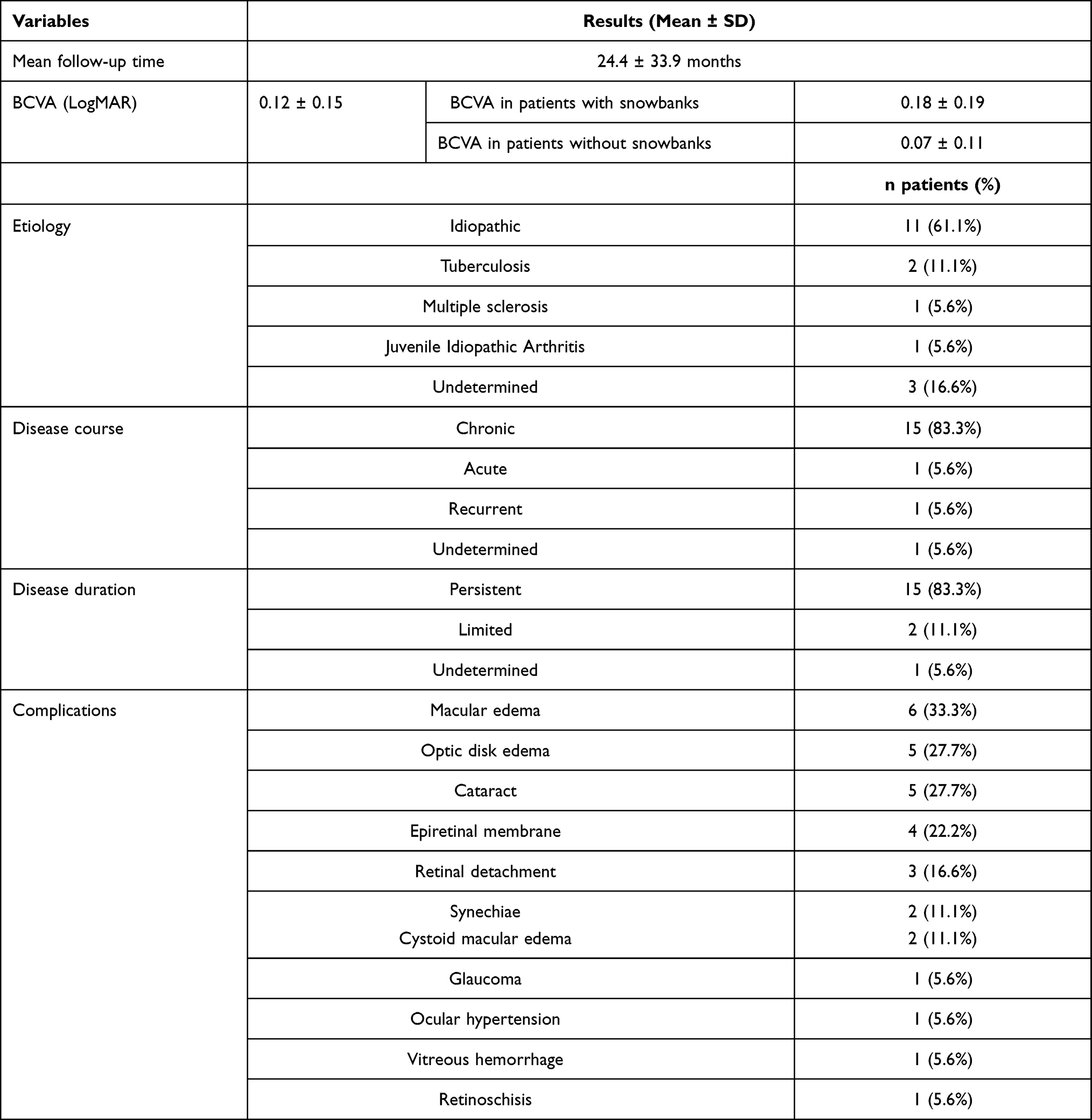 |
Table 3 Follow-Up |
Regarding treatment, fourteen patients received therapy before our consultation, with a mean of 3.1 ± 2.9 medications. Once the patients were evaluated and diagnosed by the uveitis specialist, they were treated relying on the course and etiology of the disease. Three patients were not treated because etiology could not be identified due to lack of follow-up. The two patients with ocular TB received RIPE therapy. The patients with non-infectious etiology were treated with a step-by-step approach, starting with corticosteroids, followed by immunosuppressive agents, and lastly biologic therapy, as needed. Two patients with inactive IU were treated with adjuvants (lubricants and topical NSAIDs). Nine patients with active IU, who were being treated from the remission site, were continued on corticosteroids (topical 3, oral 3, both 3) and corticosteroids were started in three patients (topical 1, oral 1, both 1). Ten patients required additional immunomodulatory therapy with methotrexate, two of them required subcutaneous methotrexate because they presented oral methotrexate intolerance and three were staggered to biologic therapy (Adalimumab 2, Infliximab 1). Two patients required surgical procedures: one photocoagulation and one Ahmed glaucoma valve implantation; none of them required cataract surgery. Finally, the most common adjuvant therapy was topical NSAIDs, followed by lubricants and mydriatics. More detailed information is given in Table 4.
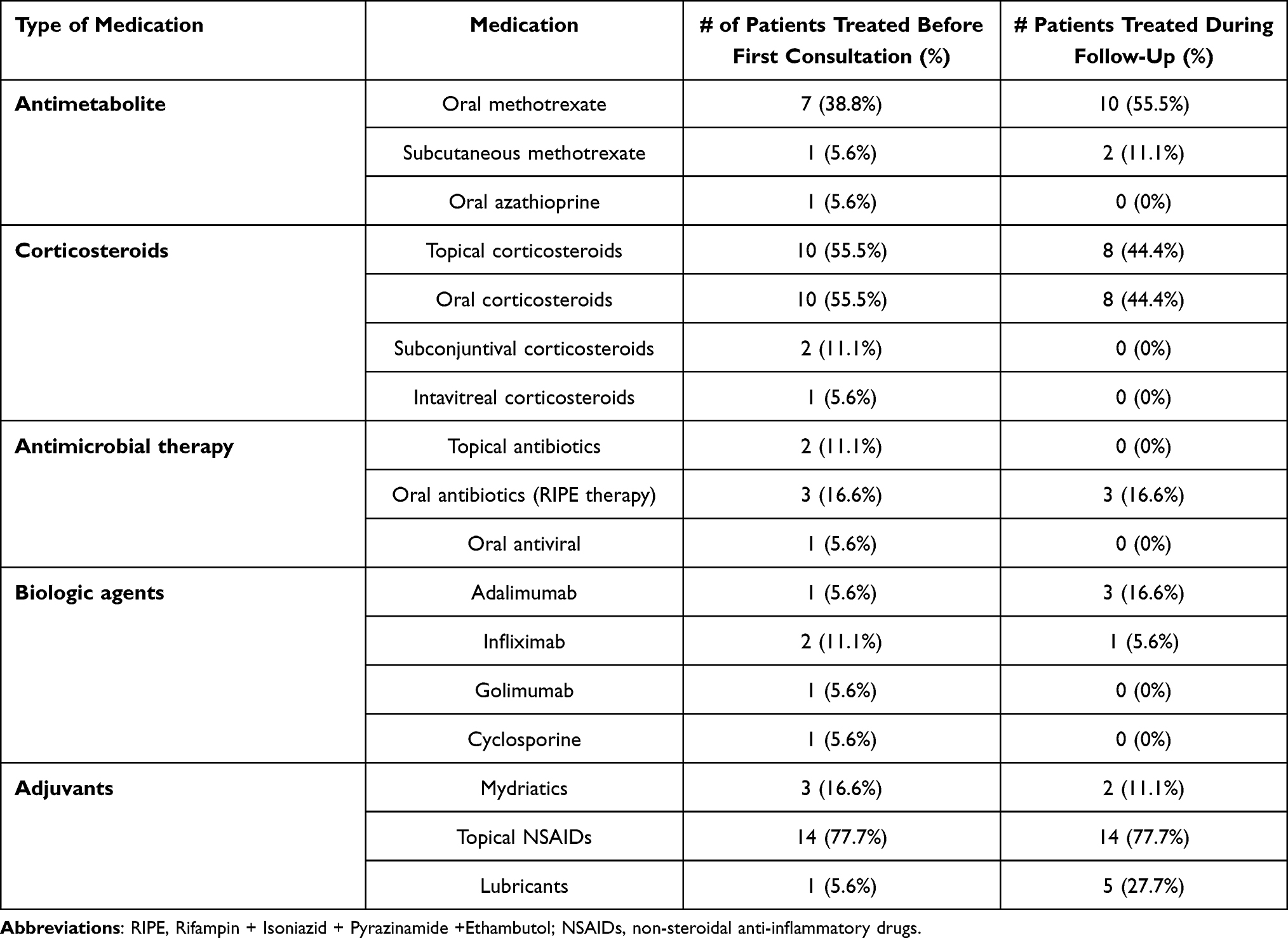 |
Table 4 Treatments Used Before First Consultation and During Follow-Up |
The mean follow-up time was 24.4 ± 33.9 months. The most prevalent course of the disease was chronic, followed by recurrent, undetermined, and acute. The duration was persistent in most of the patients followed by limited and undetermined. Outcomes of patients were studied based on the final BCVA and complications. The mean BCVA in the last visit to our center was 0.12 ± 0.15 in LogMAR. A total of 10/18 patients developed at least one complication. The most common complications were macular edema 6/18 (33.3%), optic disk edema 5/18 (27.8%), cataract 5/18 (27.8%) and epiretinal membrane 4/18 (22.2%). See Table 3 for a full list of complications.
Discussion
Literature has reported IU patterns and complications. Nevertheless, to the best of our knowledge, no characterization, nor IU treatment and management description has been published in Latin America. Here we present the first South American study describing demographics and clinical characteristics, treatment, and outcomes from a group of patients diagnosed with IU.
Globally, IU is the least common type of uveitis reported, representing about 16% of all uveitis anatomical locations.5,12,14 However, in Colombia IU represents 4.3% of all uveitis,13 which coincides with our results. Therefore, global studies have reported samples up to 159 patients, compared to our study which reports a sample of 18 patients.15
Distribution patterns are influenced by demographic, genetic, and environmental factors. IU affects patients in all age groups, from children to adults.2,16 The mean age at disease onset of our patients was 19.4 years, younger than reported in other populations like Grajewski et al17 in Germany and Vidovic-Valentincic et al7 in Slovenia where the average age at onset was 44 years and 31 years, respectively.
Usually, the prevalence of females and males is similar as found in our study.2 However, Paroli et al18,19 and Silpa-Archa et al20 found a slightly greater female prevalence, and Arellanes et al21 found a male predominance in patients with pars planitis.
Although MS has been described as IU’s most commonly associated disease,19 this was not the case in our sample. However, we have to consider that the size of our sample was smaller. Interestingly, we found that ten patients had familial autoimmunity and one of them had uveitis as a familial autoimmune disease. The most common autoimmune disease reported in family history was rheumatoid arthritis, followed by vitiligo and MS. To the best of our knowledge, there are no previous studies analyzing familial autoimmunity in patients with IU.
Despite the most common cause of IU in our patients was idiopathic, and only two patients had a systemic autoimmune disease (MS and JIA), we found a personal background related to seven autoimmune disorders with a mean of 0.38 ± 0.84 diseases. Additionally, we found six patients with positive autoantibodies (AntiTG, AntiPC, AntiTPO, pANCA, cANCA, and ANAs). Given that latent polyautoimmunity is defined as the presence of autoantibodies unrelated to the primary autoimmune disease22 and considering idiopathic uveitis as a primary disease, based on the autoimmune hypothesis,23 the positive autoantibodies could be related to a latent polyautoimmunity phenomenon, as has been shown in a previous study by Malagón et al.24 Nevertheless, it could be an incidental finding, so further studies are necessary to elucidate this issue.
Most of our patients had bilateral involvement, which coincides with previous Colombian and worldwide literature. In a previous study, Lonngi et al12 found that IU was bilateral in 84.8% of cases. In contrast, the study conducted by Dajee et al25 in the United States (USA), which evaluated the characteristics and outcomes of pediatric uveitis cases, found that just 48% of IU cases were bilateral.
In a study conducted in a tertiary referral center in Taiwan among uveitis patients, most patients experienced insidious onset (65.4%) and persistent duration (69.2%).26 In the same way, Silpa-Archa et al20 and Boer et al27 found that chronic was the most common course in their patients. In another study in Chinese patients, chronic course was equal to recurrent course.28 In the last two studies, duration was predominantly persistent. Similarly, we found insidious onset, chronic course, and persistent duration in most of our patients.
Abnormal image results were expected, as abnormal B-MRI corresponded to a patient with MS, and abnormal chest images (radiography and C-CT) corresponded to patients with tuberculosis. Interestingly, Vidovic-Valentincic et al7 found that periphlebitis was strongly associated with systemic disease. In contrast, all of our patients that presented peripheral periphlebitis had an idiopathic or undetermined diagnosis.
Concerning etiology, despite fifteen patients had abnormal laboratory findings, ten of them were not specific for any systemic or infectious etiology (eg leukocytosis or elevated CRP) thus were classified as idiopathic. This was the most common etiology in our study, followed by tuberculosis, MS, and JIA, which coincides with Indian29 and Philippines30 studies’ results; and differs from the results in Europe,17,18 USA,31,32 and Canada,33 where sarcoidosis is the second most common cause. Interestingly, in our region sarcoidosis is infrequent and poorly described.34
Ocular inflammation was our main indication for starting therapy and the lack of improvement for treatment staging. Additionally, complications were treated depending on the case. Contrarily, other studies started treatment only when there was an underlying disease or complications.15 All of the patients in our study required treatment, while other studies reported the use of treatment in 75.8–77.5% of their patients.15,35
In our patients, the most common treatments used were corticosteroids, followed by oral antimetabolites; and the most used adjuvant therapy were topical NSAIDs in cases in which macular edema was present. Similarly, other studies reported systemic corticosteroids to be the most common treatment, followed by oral immunosuppressive therapy.6,15,16,21,35 Refractory cases can require biological therapy,36 in our study it was used in three patients, and one of them had to change the biologic drug once.
Our mean follow-up time was 24.4 ± 33.9 months (2.0 ± 2.8 years). Other studies have shown a follow-up of twice or three times greater, with 64.9 and 59.7 months, and 4.5 years.27,28,37
Regarding visual acuity, studies have described values from 0.1 to 0.3 LogMAR,27,28,31,37 which coincides with our results. Additionally, several ocular findings and complications have been reported as poor prognostic factors for final BCVA in patients with IU. In a recent study, Khairallah et al38 reported that poor BCVA at presentation, vitritis ≥ 3+ cells, and the presence of snowbanks increased the risk of poor final BCVA. Similarly, we found ≥ 3+ vitritis in just one patient and snowbanks in 8 patients; those with snowbanks presented similar BCVA at the initial consultation but had a poorer final BCVA (Tables 2 and 3).
Other studies coincide with our findings regarding complications such as macular edema, optic disc edema, cataract, epiretinal membrane, retinal detachment, synechiae, ocular hypertension, glaucoma, vitreous hemorrhage, and retinoschisis.21,27,28,37,39 Another complication described in the literature, not found in our patients, is band keratopathy.37
Limitations
This is a small sample of patients with IU diagnosis. It may be due to a low prevalence of the disease in our population. Based on the sample size we decided not to apply bivariate or multivariate statistical analysis but we made a comprehensive description of all IU cases which could help to increase the knowledge of this uncommon disease. This study can contribute to develop future research with sample size calculation that allow more complex statistical analysis.
Conclusion
In our context, IU is infrequent, does not present sex predominance, and is more prevalent in young individuals. The most common characteristics were idiopathic etiology, insidious onset, chronic course, and persistent duration. Moreover, it is important to discard infectious and systemic origins and identify polyautoimmunity and familial autoimmunity phenomena, as these may require a multidisciplinary approach. Ophthalmologists should be aware of the disease to adequately diagnose, treat, and refer patients with IU diagnosis to prevent common complications, such as macular edema. Additionally, taking into account patients with snowbanks is important, as they may present a worse visual outcome. Further studies are required to increase our knowledge of the disease and its relationship with polyautoimmunity.
Data Sharing Statement
The datasets used and analyzed during the current study are available by the corresponding author on reasonable request.
Ethics Considerations
This study adheres to the ethical principles for human research established by the Helsinki Declaration, the Belmont Report, and Colombian Resolution 008430 from 1993. The confidentiality of the information has been preserved based on the Habeas data law (Organic Law 1581 of 2012). This study was approved by Universidad del Rosario Ethical Committee (DVO005 1509-CV1398).
Consent for Publication
As it is a risk-free research, researchers are exempt, by the Colombian Resolution 008430 from 1993, from obtaining informed consent.
Acknowledgments
We are thankful to the Universidad del Rosario for financing the publication charges of this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work. No funding was required to carry out this study.
References
1. Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509–516. doi:10.1016/j.ajo.2005.03.057
2. Babu M, Rathinam S. Intermediate uveitis. Indian J Ophthalmol. 2010;58(1):21. doi:10.4103/0301-4738.58469
3. Breeveld J, Rothova A, Kuiper H. Intermediate uveitis and Lyme borreliosis. Br J Ophthalmol. 1992;76(3):181–182. doi:10.1136/bjo.76.3.181
4. Zierhut M, Foster CS. Multiple sclerosis, sarcoidosis and other diseases in patients with pars planitis1. In Wrf B, Manthey KF, Nussenblatt RB, editors. Developments in Ophthalmology. Vol. 23. S. Karger AG; 1991:41–47. doi:10.1159/000429628
5. Tsirouki T, Dastiridou A, Symeonidis C, et al. A focus on the epidemiology of uveitis. Ocul Immunol Inflamm. 2018;26(1):2–16. doi:10.1080/09273948.2016.1196713
6. Kardes E, Sezgin Akcay BI, Bozkurt K, Unlu C, Erdogan G, Akcali G. Clinical characteristics of intermediate uveitis in adult Turkish patients. Int J Ophthalmol. 2015;8(4):759–763. doi:10.3980/j.issn.2222-3959.2015.04.21
7. Vidovic-Valentincic N, Kraut A, Hawlina M, Stunf S, Rothova A. Intermediate uveitis: long-term course and visual outcome. Br J Ophthalmol. 2009;93(4):477–480. doi:10.1136/bjo.2008.149039
8. Pars planitis. Genetic and rare diseases. Available from: https://rarediseases.info.nih.gov/diseases/7339/pars-planitis.
9. Gritz D. Incidence and prevalence of uveitis in Northern California The Northern California Epidemiology of Uveitis Study. Ophthalmology. 2004;111(3):491–500. doi:10.1016/j.ophtha.2003.06.014
10. Miserocchi E, Fogliato G, Modorati G, Bandello F. Review on the Worldwide epidemiology of uveitis. Eur J Ophthalmol. 2013;23(5):705–717. doi:10.5301/ejo.5000278
11. Liberman P, Gauro F, Berger O, Urzua CA. Causes of uveitis in a tertiary center in Chile: a cross-sectional retrospective review. Ocul Immunol Inflamm. 2015;23(4):339–345. doi:10.3109/09273948.2014.981548
12. Lonngi M, Aguilar MC, Ríos HA, Aristizábal-Duque CH, Rodríguez FJ, De-la-torre A. Pediatric uveitis: experience in Colombia. Ocul Immunol Inflamm. 2016;24(4):410–414. doi:10.3109/09273948.2016.1160129
13. De-la-torre A, López-Castillo CA, Rueda JC, Mantilla RD, Gómez-Marín JE, Anaya J-M. Clinical patterns of uveitis in two ophthalmology centres in Bogota, Colombia. Clin Experiment Ophthalmol. 2009;37(5):458–466. doi:10.1111/j.1442-9071.2009.02082.x
14. Chang JH-M, Wakefield D. Uveitis: a global perspective. Ocul Immunol Inflamm. 2002;10(4):263–279. doi:10.1076/ocii.10.4.263.15592
15. Ness T, Boehringer D, Heinzelmann S. Intermediate uveitis: pattern of etiology, complications, treatment and outcome in a tertiary academic center. Orphanet J Rare Dis. 2017;12(1):81. doi:10.1186/s13023-017-0638-9
16. Engelmann K, Neß T, Greiner K, Hudde T. Uveitis intermedia im Kindesalter. Klin Monatsblätter Für Augenheilkd. 2007;224(6):462–468. doi:10.1055/s-2007-963303
17. Grajewski RS, Caramoy A, Frank KF, et al. Spectrum of Uveitis in A German Tertiary Center: review of 474 consecutive patients. Ocul Immunol Inflamm. 2015;23(4):346–352. doi:10.3109/09273948.2014.1002567
18. Paroli MP, Spinucci G, Liverani M, Monte R, Pezzi PP. Uveitis in childhood: an Italian Clinical and Epidemiological Study. Ocul Immunol Inflamm. 2009;17(4):238–242. doi:10.1080/09273940802702561
19. Paroli MP, Abicca I, Sapia A, Bruschi S, Pezzi PP. Intermediate uveitis: comparison between childhood-onset and adult-onset disease. Eur J Ophthalmol. 2014;24(1):94–100. doi:10.5301/ejo.5000336
20. Silpa-archa S, Noonpradej S, Amphornphruet A. Pattern of uveitis in a Referral Ophthalmology Center in the Central District of Thailand. Ocul Immunol Inflamm. 2015;23(4):320–328. doi:10.3109/09273948.2014.943773
21. Arellanes-García L, Navarro-López LP, Recillas-Gispert C. Pars planitis in the Mexican Mestizo population: ocular findings, treatment, and visual outcome. Ocul Immunol Inflamm. 2003;11(1):53–60. doi:10.1076/ocii.11.1.53.15583
22. Botello A, Herrán M, Salcedo V, Rodríguez Y, Anaya J, Rojas M. Prevalence of latent and overt polyautoimmunity in autoimmune thyroid disease: a systematic review and meta-analysis. Clin Endocrinol (Oxf). 2020;93(4):375–389. doi:10.1111/cen.14304
23. Forrester JV, Kuffova L, Dick AD. Autoimmunity, autoinflammation, and infection in uveitis. Am J Ophthalmol. 2018;189:77–85. doi:10.1016/j.ajo.2018.02.019
24. Malagón C, Del Gomez MP, Mosquera C, et al. Juvenile polyautoimmunity in a rheumatology setting. Autoimmun Rev. 2019;18(4):369–381. doi:10.1016/j.autrev.2018.11.006
25. Dajee K, Rossen J, Bratton M, Whitson J, He Y-G. A 10-year review of pediatric uveitis at a Hispanic-dominated tertiary pediatric ophthalmic clinic. Clin Ophthalmol. 2016;10:1607–1612. doi:10.2147/OPTH.S96323
26. Chen S-C, Chuang C-T, Chu M-Y, Sheu S-J. Patterns and Etiologies of Uveitis at a Tertiary Referral Center in Taiwan. Ocul Immunol Inflamm. 2017;25(sup1):S31–S38. doi:10.1080/09273948.2016.1189577
27. de Boer J, Berendschot TTJM, van der Does P, Rothova A. Long-term follow-up of intermediate uveitis in children. Am J Ophthalmol. 2006;141(4):616–616.e7. doi:10.1016/j.ajo.2005.09.035
28. Chan CKM, Wu ZHY, Luk FOJ, et al. Clinical characteristics of intermediate uveitis in Chinese patients. Ocul Immunol Inflamm. 2013;21(1):71–76. doi:10.3109/09273948.2012.736587
29. Dogra M, Singh R, Agarwal A, et al. Epidemiology of uveitis in a Tertiary-care Referral Institute in North India. Ocul Immunol Inflamm. 2017;25(sup1):S46–S53. doi:10.1080/09273948.2016.1255761
30. Abaño JM, Galvante PR, Siopongco P, Dans K, Lopez J. Review of epidemiology of uveitis in Asia: pattern of uveitis in a Tertiary Hospital in the Philippines. Ocul Immunol Inflamm. 2017;25(sup1):S75–S80. doi:10.1080/09273948.2017.1335755
31. Engelhard S, Patel V, Reddy A. Intermediate uveitis, posterior uveitis, and panuveitis in the Mid-Atlantic USA. Clin Ophthalmol. 2015;1549. doi:10.2147/OPTH.S89428
32. Chan SM, Hudson M, Weis E. Anterior and intermediate uveitis cases referred to a tertiary centre in Alberta. Can J Ophthalmol. 2007;42(6):860–864. doi:10.3129/i07-159
33. Chan SM, Gan KD, Weis E. Characteristics and predictors of recurrence of anterior and intermediate uveitis in a Canadian referral centre. Can J Ophthalmol. 2010;45(2):144–148. doi:10.3129/i10-002
34. Chavarriaga-Restrepo A, López-Amaya JE, Mesa-Navas MA, Velásquez-Franco CJ. Sarcoidosis: muchas caras, una enfermedad. Revisión narrativa de la literatura. Iatreia. 2019;32(3):191–203. doi:10.17533/udea.iatreia.11
35. Mi H, Ho SL, Lim WK, Wong EPY, Teoh SC. Trends in patterns of intermediate uveitis in a Tertiary Institution in Singapore. PLoS One. 2014;9(3):e91533. doi:10.1371/journal.pone.0091533
36. Lai FHP, Liu DTL, Lam DSC. Review of Intermediate Uveitis. Asia Pac J Ophthalmol. 2013;2(6):375–387. doi:10.1097/APO.0b013e3182a2c90b
37. Sancho L, Kramer M, Koriat A, Eiger-Moscovich M, Sharon Y, Amer R. Complications in intermediate uveitis: prevalence, time of onset, and effects on vision in short-term and long-term follow-up. Ocul Immunol Inflamm. 2019;27(3):447–455. doi:10.1080/09273948.2017.1420203
38. Khairallah M, Hmidi K, Attia S, et al. Clinical characteristics of intermediate uveitis in Tunisian patients. Int Ophthalmol. 2010;30(5):531–537. doi:10.1007/s10792-010-9352-5
39. Pichi F, Srivastava SK, Nucci P, Baynes K, Neri P, Lowder CY. Peripheral retinoschisis in intermediate uveitis. Retina. 2017;37(11):2167–2174. doi:10.1097/IAE.0000000000001463
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.